
Abstract
Study Design
Retrospective Cohort Study.
Objectives
Few previous studies have examined the relationship between preoperative disability and patient outcomes after complex adult spinal deformity surgery. In this study, we hypothesized that patients with worse preoperative disability would be more likely achieve a clinically significant improvement in their symptoms after surgery.
Methods
Demographics, comorbidities, surgical data, and health related survey results were analyzed from a consecutive series of adults (≥18 years old) who underwent spinal deformity correction, instrumentation, and fusion. Patients included had 6 or more levels fused and their surgery performed at single institution between 2015 and 2018 with minimum 2 year follow up.
Results
A total of 108 patients met inclusion criteria. Bivariate analysis demonstrated the following as having a greater probability of reaching minimum clinically important difference (MCID) at 2 years postoperatively: >50th percentile Oswestry Disability Index (ODI) score (ODI >36), cardiac comorbidities, and use of pelvic fixation, pedicle subtraction osteotomy, and transforaminal lumbar interbody fusion. Conversely, baseline Scoliosis research society score (SRS) >50th percentile (SRS ≥62) and use of vertebral column resection (VCR) were significant predictors of not reaching MCID at 2 years. On logistic regression analysis, >50th percentile ODI score (ODI >36) was identified as the only independent predictor of achieving MCID.
Conclusions
Patients with greater disability, independent of other preoperative or surgical factors, are more likely to have clinically significant improvement in their daily functioning after complex deformity surgery. For patients who undergo surgical intervention for severe or progressive deformity, including VCR, MCID might be an ineffective outcome measure.
Keywords
Introduction
Adult spinal deformity (ASD) affects nearly 30% of the general population and 60% of those above age 70.1-3 Adult spinal deformity can lead to significant disability that impacts patient daily function. Health-related quality of life surveys (HRQoL) are an important metric for quantifying the symptoms and the impact that ASD has on a patient’s everyday life. The Oswestry Disability Index (ODI) is a commonly used outcome measure in spine surgery that assesses the degree to which a patient is debilitated from their pathology.4,5 Another commonly used outcome measure is the Scoliosis Research Society (SRS-22) questionnaire which measures a patient’s perception of their quality of life by function, pain, self-image, mental health, and satisfaction/ dissatisfaction domains.6,7 These surveys, in addition to others, provide quantitative metrics of a patient’s clinical disability.
One of the most clinically relevant ways to utilize HRQoL scores is to establish a threshold for achieving a minimum clinically important difference (MCID). Since not all improvements in HRQoL scores reflect meaningful improvements, the MCID allows investigators to determine if clinically significant improvements have occurred.8-11 Previous research has been conducted to determine which preoperative factors will influence a patient’s probability of achieving MCID, including age, gender, pathology, and psychiatric disorders.12-14
In this study, we evaluate the correlation between preoperative HRQoL scores of ASD patients and their ability to achieve MCID after surgery. Our hypothesis is that, since ASD patients with lower baseline HRQoL scores are more debilitated than those with higher scores, they will be more likely to achieve MCID following spinal fusion.
Methods
This was a retrospective review of consecutively collected adult (≥18 years old) patients who underwent complex ASD surgery at a single institution from 2015 to 2018 with minimum 2 year follow up. Complex ASD surgery was defined as a deformity correction and instrumentation procedure with minimum 6 levels fused. Approval was obtained from our Institutional Review Board (IRB approval number AAAR1866) and patient informed consent was not required. Patient demographic data was collected and included gender, Body Mass Index (BMI), American Association of Anesthesiologists (ASA), baseline psychiatric diagnosis (specifically anxiety and depression), anemia, cardiac comorbidities, diabetes, gastrointestinal comorbidities, history of cancer, history of deep vein thrombosis or pulmonary embolism, hypothyroidism, pulmonary comorbidities, osteoporosis, and history of stroke/transient ischemic events. Surgical characteristics were also collected including operative duration, posterior column osteotomy (PCO), pelvic fixation, pedicle subtraction osteotomy (PSO), transforaminal lumbar interbody fusion (TLIF), anterior lumbar interbody fusion (ALIF), oblique lateral interbody fusion (OLIF), vertebral column resection (VCR), postoperative transfusion, operative complication, length of stay (LOS), and readmission within 90 days of surgery. ODI and SRS-22 scores were collected preoperatively, at 1 year, and at 2 years.
Bivariate analysis was performed on perioperative variables. Independent risk factors for reaching MCID for ODI questionnaires were identified using multivariate logistic regression. MCID was determined by the established distribution method. The distribution based MCID ensured that the HRQoL changes observed between time periods was the result of true and clinically relevant changes, rather than inter-test variance. The established MCID equation was, as used in prior literature,
Results
Demographics of Patients Included in the Analysis.
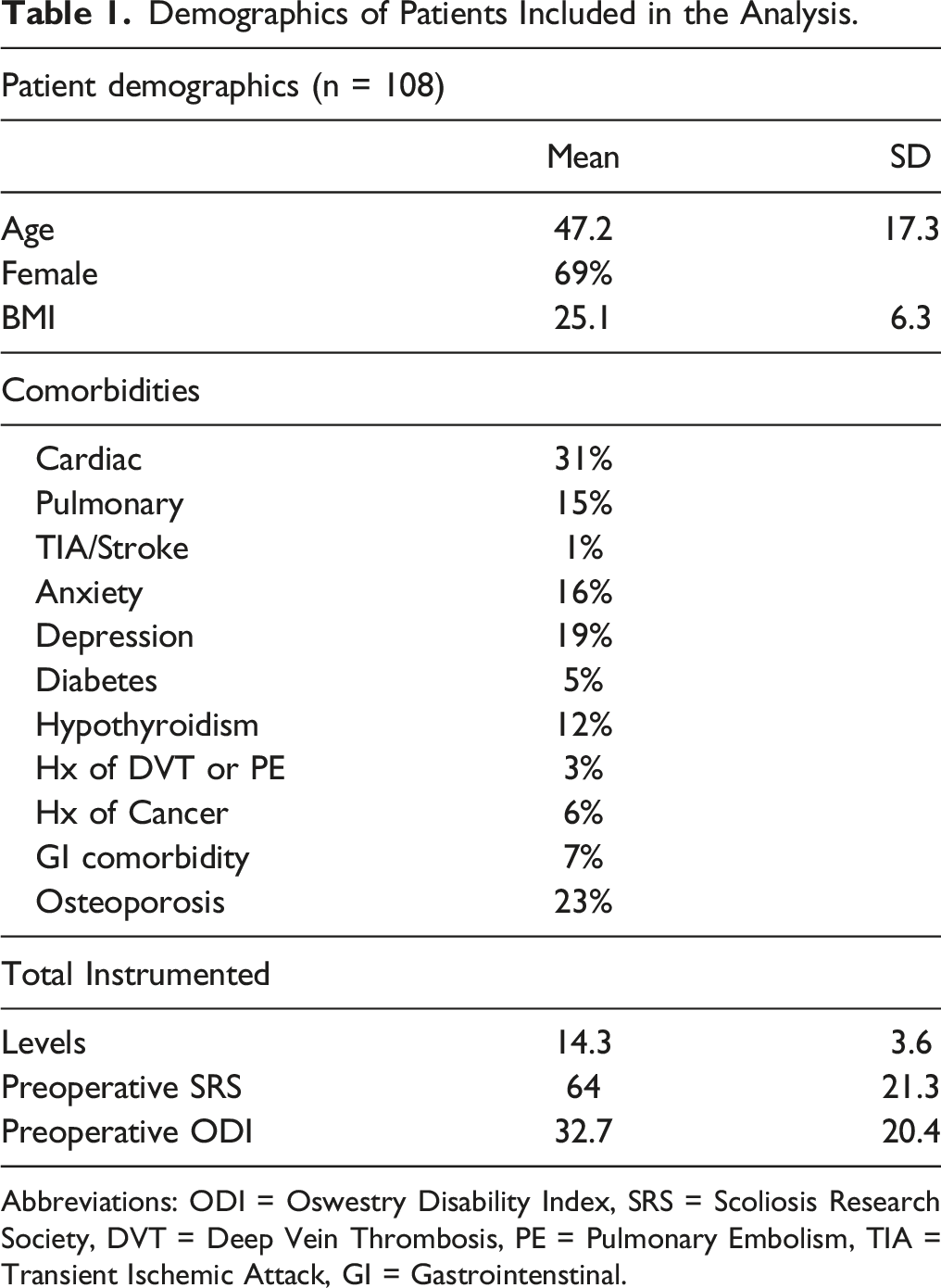
Abbreviations: ODI = Oswestry Disability Index, SRS = Scoliosis Research Society, DVT = Deep Vein Thrombosis, PE = Pulmonary Embolism, TIA = Transient Ischemic Attack, GI = Gastrointenstinal.
Analysis of Preoperative Factors Leading to MCID in ODI Scores at 2 Years.
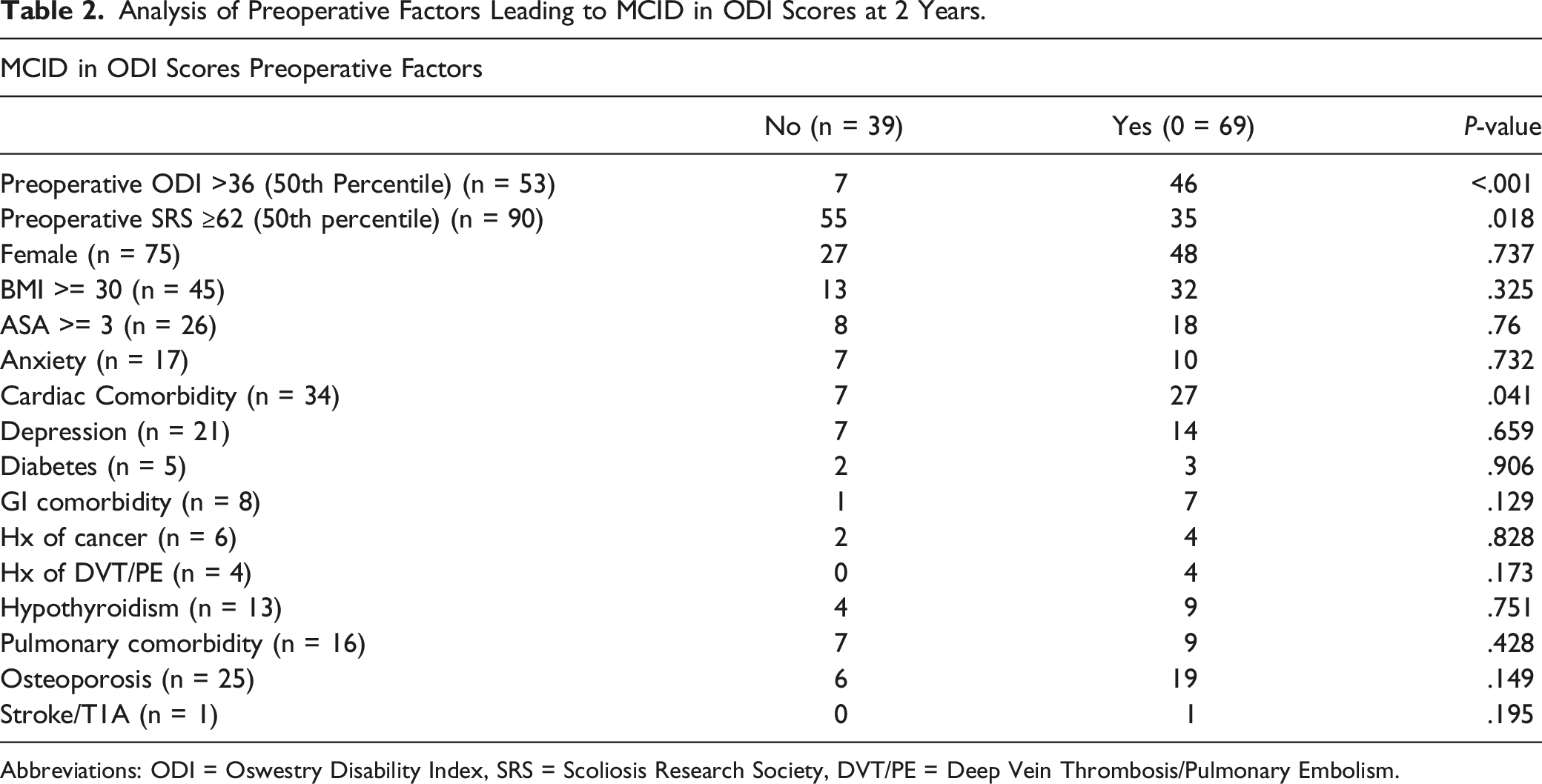
Abbreviations: ODI = Oswestry Disability Index, SRS = Scoliosis Research Society, DVT/PE = Deep Vein Thrombosis/Pulmonary Embolism.
Analysis of Intra and Postoperative Factors Leading to MCID in ODI Scores at 2 Years.
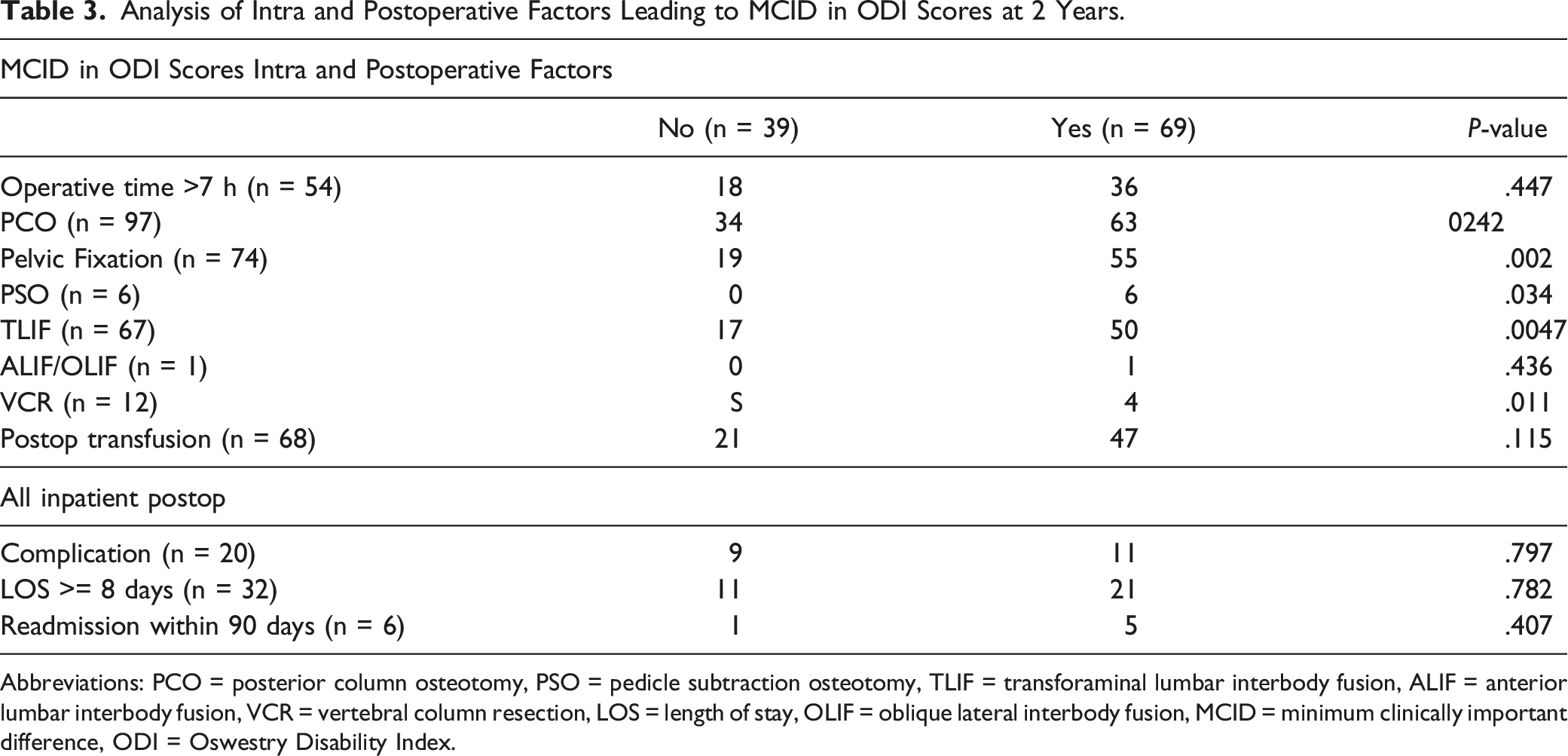
Abbreviations: PCO = posterior column osteotomy, PSO = pedicle subtraction osteotomy, TLIF = transforaminal lumbar interbody fusion, ALIF = anterior lumbar interbody fusion, VCR = vertebral column resection, LOS = length of stay, OLIF = oblique lateral interbody fusion, MCID = minimum clinically important difference, ODI = Oswestry Disability Index.
Conversely, two negative predictors for reaching ODI MCID at 2 years were identified. Baseline SRS score >50th percentile (SRS ≥62, ie lesser disability) and use of vertebral column resection (VCR) were significant predictors for not reaching ODI MCID at 2 years (Table 2, Table 3). Of the patients with a baseline SRS >50th percentile, only 39% (n = 35) met ODI MCID at 2 years (P = .018). Of the patients who received a VCR, only 33% (n = 4) met ODI MCID at 2 years (P = .011).
Multivariate Analysis for Independent Variables for MCID.

Abbreviations: MCID = minimum clinically important difference, ODI = Oswestry Disability Index.
Discussion
Worse preoperative HRQoL scores, specifically ODI scores, are associated with a greater probability of reaching MCID following complex spinal fusion. In this study, higher ODI score, or greater disability, was an independent variable predictive of reaching MCID at 2 years after spinal fusion. On the contrary, higher preoperative SRS scores indicative of patients who had less disability and less symptoms, were predictive of not reaching MCID at 2 years. These results replicate the findings of several previous studies, that patients with higher ODI scores preoperatively were more likely to perceive improvement postoperatively.13,19-21 This is the first study focusing specifically on complex ASD defined as minimum 6 level fusion and finding ODI of 36, or 50th percentile, as an independent variable on multivariate analysis. Patients with greater disability, independent of other preoperative or surgical factors, are more likely to have clinically significant improvements in their daily functioning after complex deformity surgery.
The other preoperative or intraoperative factors that significantly influenced the probability of reaching ODI MCID included pelvic fixation (P = .002), PSO (P = .034), TLIF (P = .0047), VCR (P = .011), and cardiac comorbidity (P = .041). With respect to the PSO and VCR, one possible explanation for these findings is that patients who undergo VCR are typically for deformity correction, rather than pain and disability. The age average of patients who underwent VCR in this study was 36 as compared to 47 overall. All 12 patients who underwent VCR had surgery for severe or progressive deformity with adolescent idiopathic scoliosis (AIS) (n = 7) or kyphoscoliosis (n = 5) as their diagnosis. 2 patients had hemivertebra that were resected. For patients undergoing spinal fusion for severe deformity or progressive deformity rather than pain, disability, myelopathy, or radiculopathy, MCID might be an ineffective tool to measure outcomes parameters. Both TLIF and pelvic fixation are widely used in degenerative spine pathology in addition to deformity; the same logic holds that these patients with greater disability from their symptoms would find improvement after surgery. In contrast to our findings, a 2015 paper by Guler et al found that the presence of pelvic fixation had no significant impact on ODI at their 1 year follow-up. 22 For patients undergoing a TLIF, however, our findings are similar to previous literature, for example Perez-Cruet et al who also appreciated significant ODI improvements for patients who underwent a TLIF. 23 No previous studies have demonstrated a correlation between cardiac comorbidities and ODI MCID. Despite the initial significance of these findings, none of these variables were identified on stepwise logistic regression to be independent variables.
The findings of this study are important considering the increasing emphasis placed on patient selection criteria to optimize outcomes. In the case of baseline HRQoL scores, previous studies have investigated HRQoL score as a proxy for mental health and evaluating whether those with worse baseline mental health (ie, worse baseline HRQoL scores) are also worse surgical candidates.12,24-26 This would result in individuals with worse baseline HRQoL scores to be at risk for lower rates of surgical intervention. However, our study has demonstrated that patients with worse baseline ODI scores should actually be operative candidates as they are more likely to benefit from surgical intervention and achieve MCID.
Conclusion
This study demonstrates that patients who are more disabled from their ASD symptoms, specifically at the threshold of 36 or 50th percentile on the ODI score, are more likely to benefit from surgery. On the contrary, patients with high SRS scores, over 62 or the 50th percentile, should be scrutinized prior to surgical intervention as they are less likely to achieve MCID. The exception is likely patients who undergo surgical intervention for severe or progressive deformity without significant disability, where MCID is likely an ineffective outcome parameter. Preoperative ODI score should be used as an additional metric for evaluating and indicating an ASD patient for spine surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.