
Abstract
Study design
Retrospective cohort study.
Objectives
To elucidate incidence, risk factor, and clinical effect of bone regrowth after posterior cervical foraminotomy (PCF).
Methods
Ninety-eight patients who underwent PCF for the treatment of cervical radiculopathy and were followed up for >2 years were retrospectively reviewed. Foraminal dimension, sagittal gap at resected area, facet thickness, lamina length, and cervical range of motion (ROM) were measured. Neck pain visual analogue scale (VAS), arm pain VAS, and neck disability index (NDI) were recorded. Radiographic measures were compared between segments with foraminal narrowing of ≥20% at the 2-years follow-up (restenosis segments) and foraminal narrowing of <20% (patent segments).
Results
Sixty-nine patients with 109 segments were included. 73.4% (80/109) of foramens demonstrated foraminal narrowing and decrease of foraminal dimension of ≥20% occurred in 30.3% (30/109). Foraminal dimension at postoperative 2-days was significantly higher in the restenosis segments (P = .047). Furthermore, increase of foraminal dimension was significantly associated with foraminal restenosis of ≥20% (P = .018). Facet thickness was significantly higher in the restenosis segments compared to patent segments at postoperative 2-years follow-up (P = .038). Neck pain VAS was significantly aggravated only in the restenosis group at postoperative 2-years follow-up (P < .001).
Conclusions
Foraminal narrowing commonly occurs after PCF due to bone healing. Bone growth occurs in all directions while medial facet growth contributes more to foraminal restenosis. Greater widening of foramen during PCF is a risk factor for postoperative foramen restenosis. Therefore, amount of bone resection should be kept optimal and excessive resection should be avoided to prevent foramen restenosis.
Keywords
Introduction
Posterior cervical foraminotomy (PCF) is an effective surgical method for the treatment of cervical radiculopathy which revision rate and clinical efficacy are reported to be similar with that of anterior cervical discectomy and fusion (ACDF).1-4 It also can avoid troublesome postoperative complications of ACDF including pseudarthrosis, adjacent segmental disease, loss of motion segments, and postoperative dysphagia.5,6 Furthermore, recent reports have demonstrated that PCF results in shortened hospital stay and reduced blood loss or cost compared to ACDF which makes PCF a widely applied surgical option for cervical radiculopathy.5,7
While many studies have been conducted regarding radiographic outcome of ACDF including fusion, subsidence, and pseudarthrosis, not much have been reported about what happens to the foramens that underwent PCF.8-12 Fractured or resected bone has potential to heal, and it remains unclear whether decompressed foramen would remain patent permanently or restenosis would occur due to regrowth of facet and lamina. 13 It has been reported that interlaminar bone fusion occurs after laminoplasty due to bone healing process although laminoplasty is originally known as a non-fusion, motion preservation technique.14,15 Spontaneous lamina recovery has also been described for lumbar posterior decompression.16,17 There is a possibility that similar, unintended bone healing phenomenon would occur after PCF.
While reviewing postoperative CT images of patients who underwent PCF, we frequently observed that previously resected lamina and facet had been spontaneously healed during the follow-up. 11 Since bone growth into the resected foramen is an unintended process after PCF, it might adversely affect clinical outcome or increase chance of radiculopathy recurrence. Whereas, it may have beneficial effect such as decreasing chance of segmental instability after PCF. Therefore, the present study was conducted to (1) describe incidence and pattern of bone healing after PCF; (2) demonstrate how such bone healing or restenosis affects clinical and radiographic outcome; and (3) elucidate factors affecting foraminal restenosis.
Materials and Methods
Study Design and Participants
This retrospective cohort study was approved by the institutional review board (Asan Medical Center Institutional Review Board, S2018-1580-0001). Informed consent was waived due to the retrospective nature of the study. The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cohort studies.
Ninety-eight patients who underwent PCF for the treatment of cervical radiculopathy between March 2014 and December 2018 were retrospectively reviewed. The inclusion criteria were (1) radiculopathy due to foraminal stenosis; (2) who underwent 1-,2-, or 3-level PCF; and (3) who were followed-up for >2 years. Patients who had (1) previous cervical spine operations; or (2) surgery due to infection, trauma, neoplasm, or ossification of the posterior longitudinal ligament were excluded (Figure 1). Patient selection process.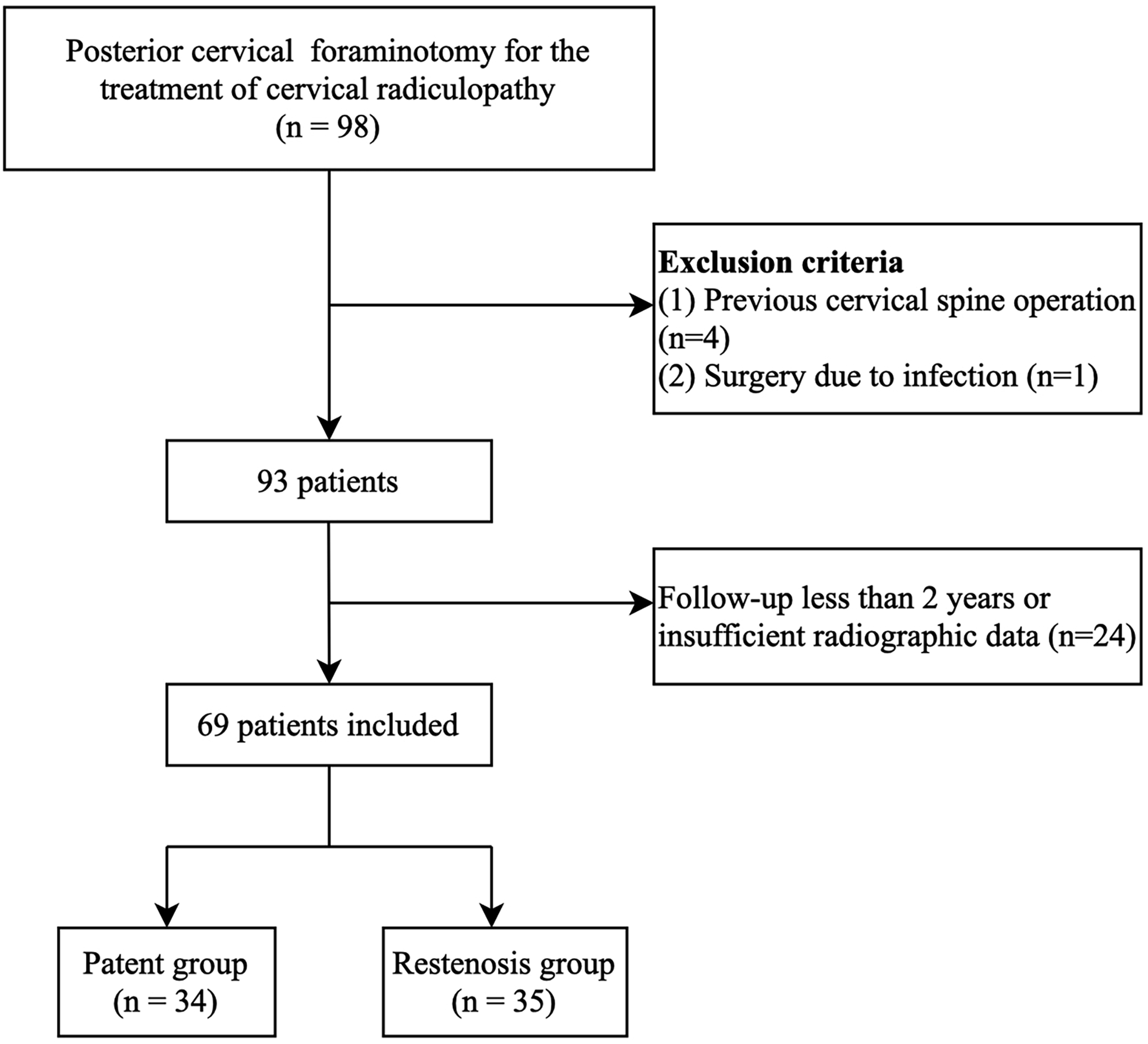
Segments which demonstrated narrowing of foraminal dimension of ≥20% at the 2 years follow-up compared to postoperative 2 days CT were classified as restenosis segments. Segments with no foraminal narrowing or narrowing of <20% at the 2 years follow-up compared to postoperative 2 days CT were defined as patent segments. A cutoff value of 20% was chosen based on the mean value of the foraminal narrowing rate demonstrated in the present study (20.0% ± 16.9%)
Surgical Techniques
After confirming the operative level with lateral fluoroscopy, midline unilateral dissection is performed to expose indicated levels while care is taken not to injure facet joint capsule. Keyhole foraminotomy including partial laminectomy and partial resection of medial facet joint is performed using high-speed burr and Kerrison punch. The extent of laminectomy and facetectomy differs according to the locations of the disc material and foraminal stenosis. However, attention is paid not to resect greater than 50% of the facet to avoid iatrogenic instability.18-20 Adequate decompression is confirmed by visualization of the nerve root and palpation of the foramen by angled curette.
Variables and Outcome Measures
Patient reported outcome measures including neck pain visual analogue scale (VAS), arm pain VAS, and neck disability index (NDI) were recorded preoperatively and at postoperative 3 months and 2 years.
CT was taken preoperatively for operative planning, 2 days after the operation for the detection of immediate complication and determine adequate decompression, and 2 years after the operation for the evaluation of delayed complications. Foraminal dimension was measured at each follow-up period using area measuring function of PACS software (PetaVision for Clinics, 3.1, Asan Medical Center, Seoul, Korea) in a sagittal image showing the inner margin of pedicles of the superior and inferior vertebrae (Figure 2A). Postoperative foraminal dimension was measured respecting the margin of remaining inferior articular process (Figure 2B). Sagittal gap, facet thickness, and lamina length of the index side were also measured in postoperative 2 days and 2 years CT to evaluate bone growth pattern. Facet thickness was measured by the length between medial and lateral margin of remained facet in the axial CT image targeting the middle of bone resection part (Figure 2C). Lamina length was measured as a remained lamina length after resection in the same axial CT image (Figure 2C). Sagittal gap between the remained superior articular process of inferior vertebra and inferior articular process of superior vertebra was also measured in the same sagittal image (Figure 2D). Dynamic cervical radiographs were taken preoperatively and at each postoperative follow-up period. Segmental range of motion (ROM) was measured as a change in the angle between the upper and the lower end plate of the respective disc on dynamic radiographs. Global cervical ROM was measured as the change in the angle between the lower margin of C2 and lower margin of C7 on dynamic radiographs.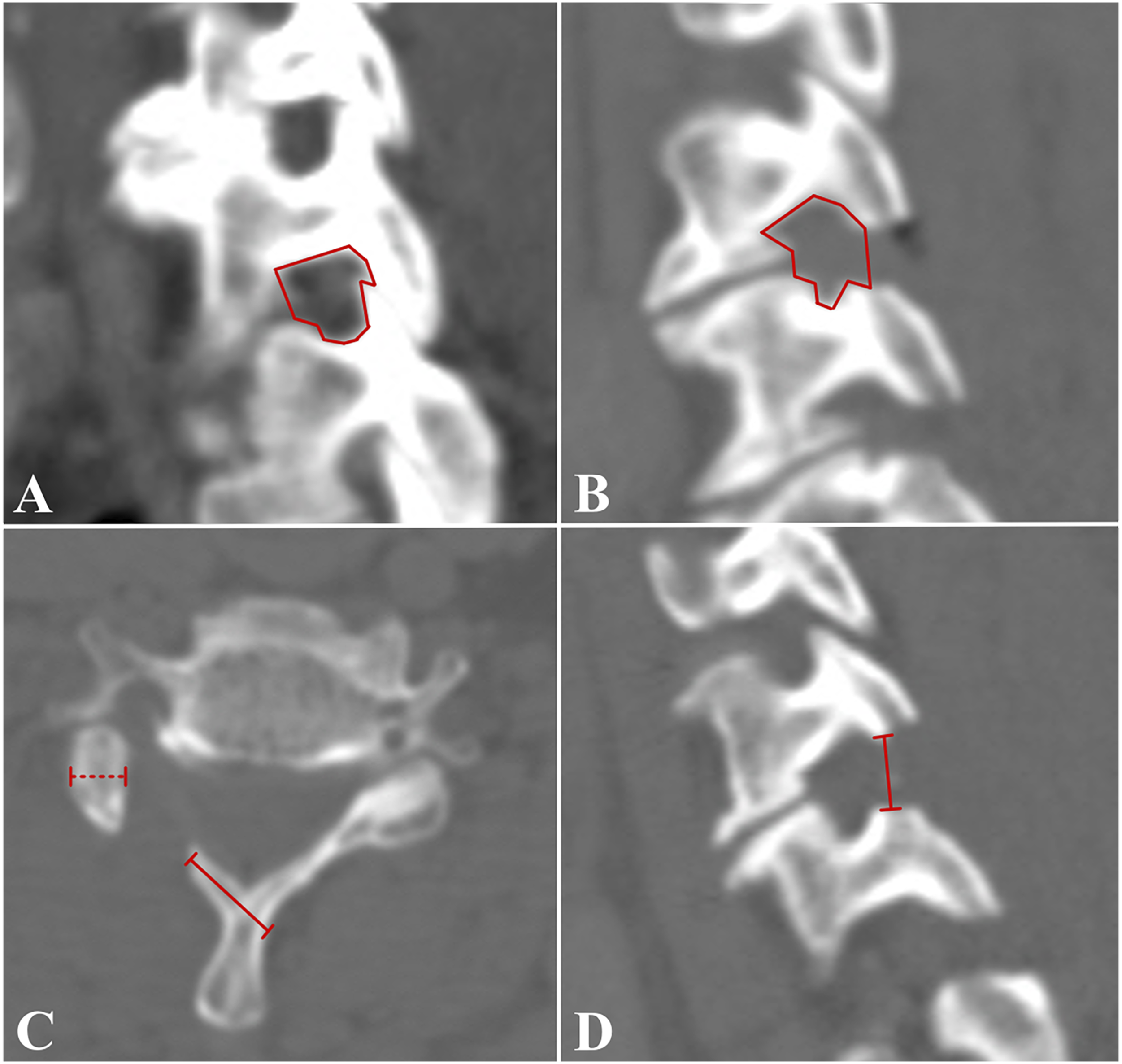
Statistical Analysis
All statistical analyses were performed using SPSS software (version 22.0; SPSS, inc., Chicago, IL). The level of significance was set at P < .05. Comparison between restenosis segments and patent segments and also between restenosis group and patent group was performed using independent t-test and chi-square test. Parameters at different time periods were compared using a paired t-test. We conducted logistic regression analysis to identify risk factors for foraminal restenosis. Two orthopedic surgeons performed radiographic measurements. The intraclass correlation coefficient (ICC) was used to define interobserver reliability. The ICC for interobserver reliability was .881, .832, .795, and .827 for the measurement of foraminal dimension, sagittal gap, facet thickness, and lamina length. The ICC for segmental or global cervical ROM was .833.
Results
Patient Characteristics.
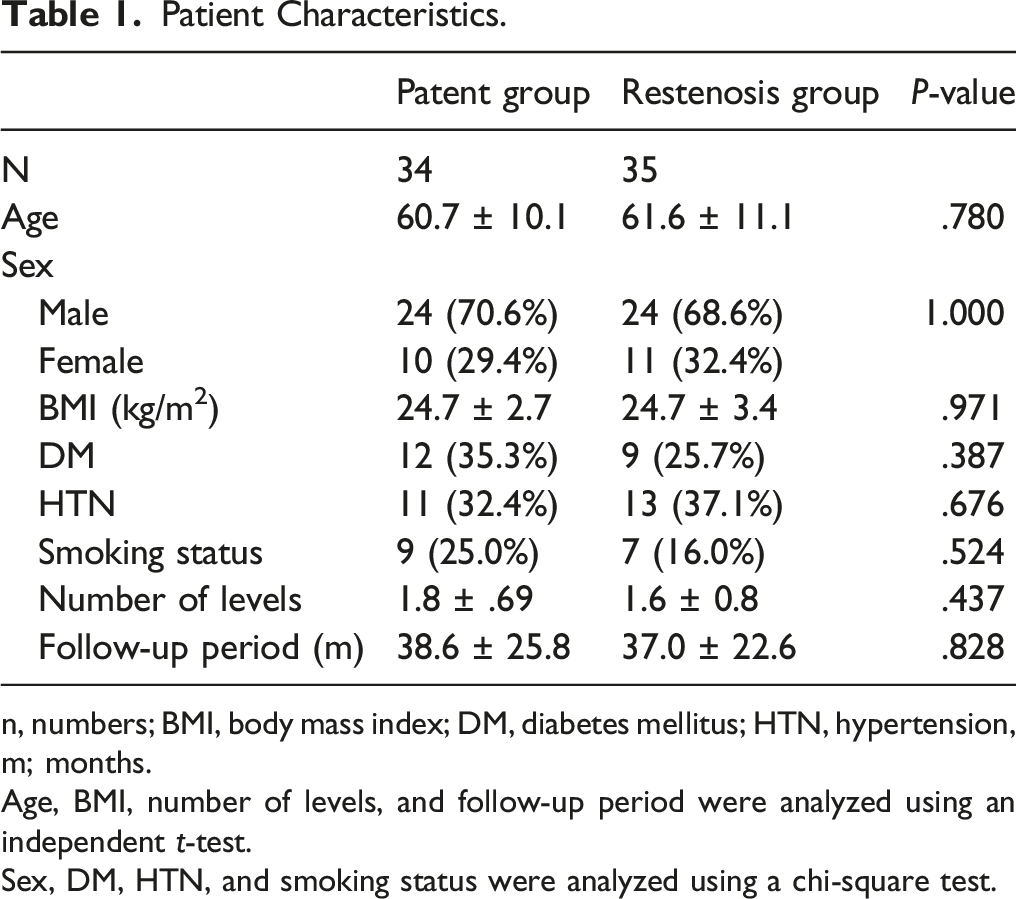
n, numbers; BMI, body mass index; DM, diabetes mellitus; HTN, hypertension, m; months.
Age, BMI, number of levels, and follow-up period were analyzed using an independent t-test.
Sex, DM, HTN, and smoking status were analyzed using a chi-square test.
Demographic factors did not demonstrate significant difference between the patent group and the restenosis group (Table 1). Two patients (5.7%) in the restenosis group and 2 patients (5.8%) in the patent group underwent revision ACDF during the follow-up. Other complications including infection, neurologic deficit, or dura tear did not occur. No postoperative segmental instability or listhesis developed during the follow-up.
Radiographic Results
Radiographic Measurements.
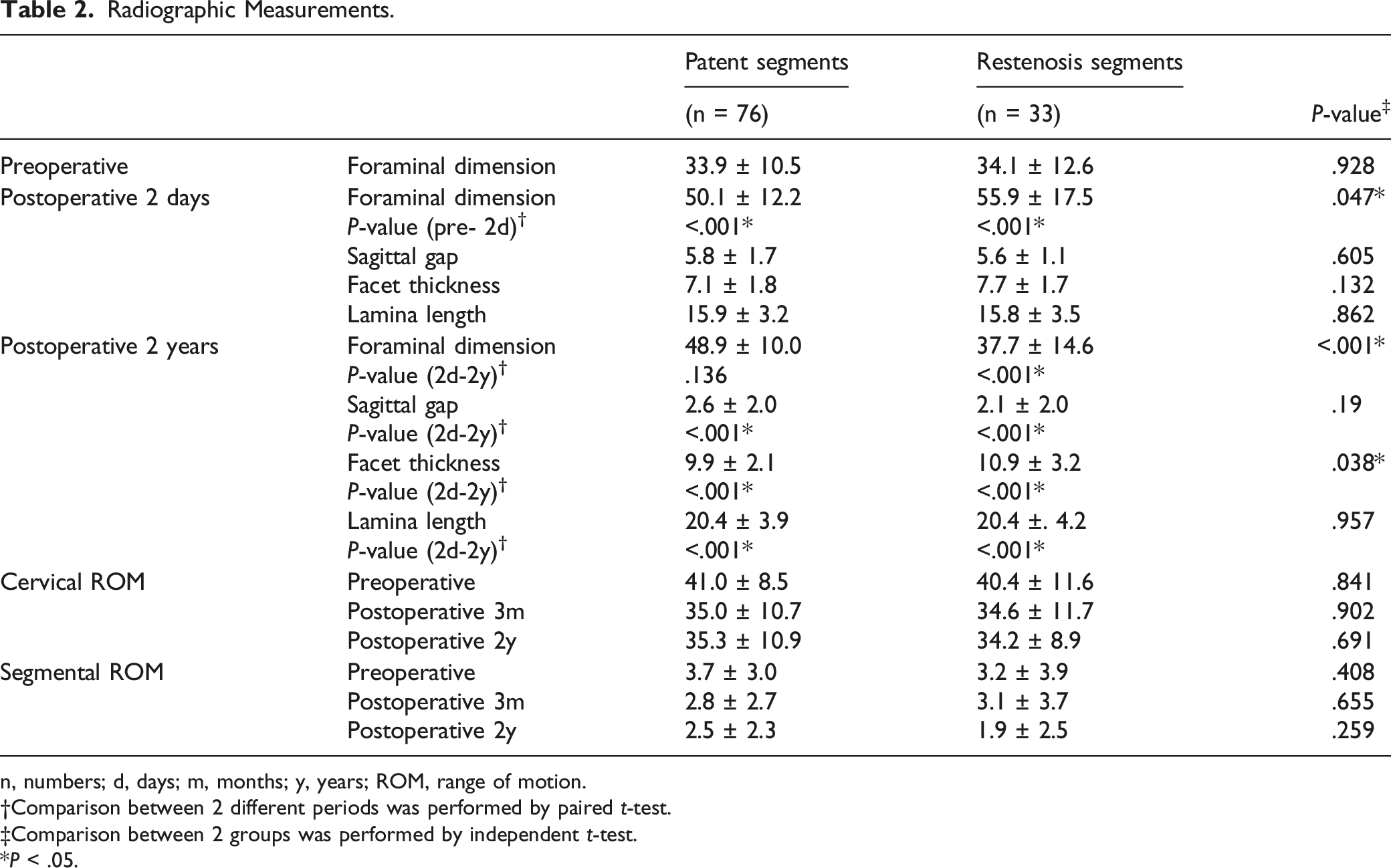
n, numbers; d, days; m, months; y, years; ROM, range of motion.
†Comparison between 2 different periods was performed by paired t-test.
‡Comparison between 2 groups was performed by independent t-test.
*P < .05.
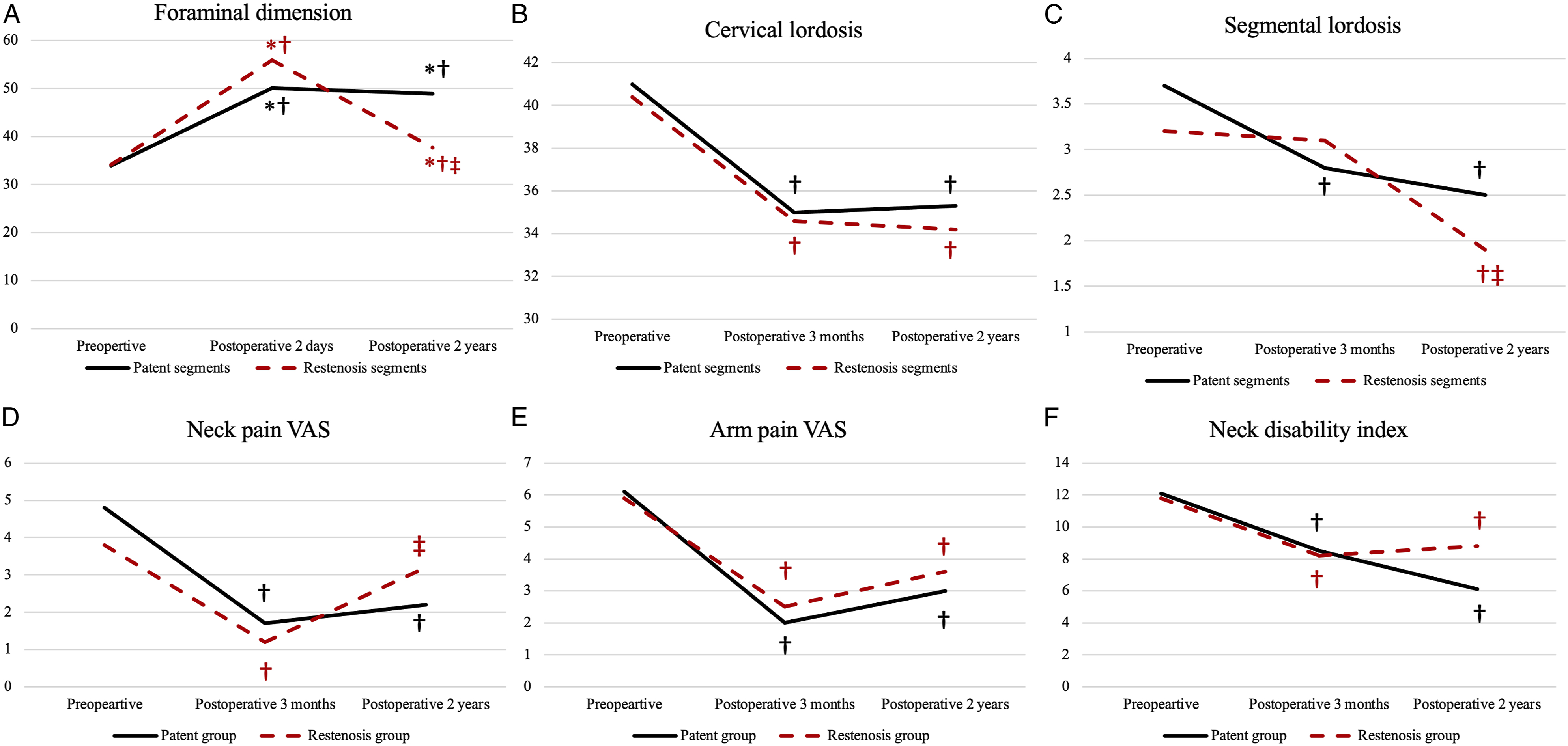
Sagittal gap decreased significantly at the 2 years follow-up compared to postoperative 2 days measurement in both groups (P < .001, .001, respectively). Furthermore, facet thickness (P < .001, <.001, respectively) and lamina length (P < .001, <.001, respectively) also demonstrated significant increase at the 2 years follow-up measurement. Facet thickness was significantly greater in the restenosis segments compared to patent segments at the 2-years follow-up (P = .038), while sagittal gap (P = .190) and lamina length (P = .957) did not significantly differ between the 2 groups (Table 2).
Patient Reported Outcome Measures.
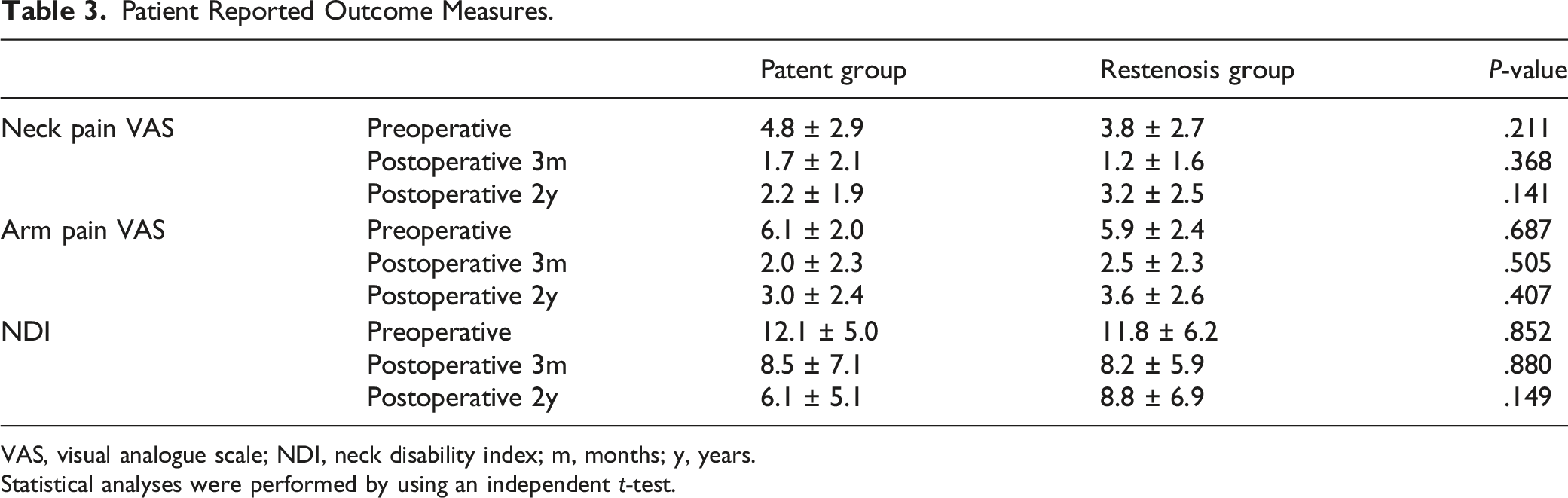
VAS, visual analogue scale; NDI, neck disability index; m, months; y, years.
Statistical analyses were performed by using an independent t-test.
Patient Reported Outcome Measures
Preoperative neck pain VAS, arm pain VAS, and NDI did not significantly differ between the 2 groups (P = .211, P = .687, P = .852, respectively). Neck pain VAS significantly improved after the operation in both groups (P < .001, <.001, respectively). However, neck pain aggravated at the 2 years postoperative period only in the restenosis group (P < .001), while it did not change in the patent group (P = .303). Neck pain at the postoperative 2 years follow-up remained significantly improved compared to preoperative scores in the patent group (P = .001), while it did not demonstrate significant difference in the restenosis group (P = .491). Neck pain VAS at each follow-up point was not significantly different between the 2 groups (Table 3) (Figure 3D).
Arm pain VAS also significantly improved after the operation in both groups (P < .001, <.001, respectively). Arm pain did not aggravate significantly at the 2 years follow-up in both groups (patent group, P = .060; restenosis group, P = .010) and remained improved compared to the preoperative scores in the 2 groups (patent group, P < .001; restenosis group, P = .004). Arm pain VAS at each follow-up period did not significantly differ between the 2 groups (Table 3) (Figure 3E).
Neck disability index significantly improved after the operation in both groups (patent group, P = .048; restenosis group, P = .008). Neck disability index at the postoperative 2 years was significantly less than the preoperative values in both groups (patent group, P < .001; restenosis group, P = .042). Furthermore, NDI at each follow-up point was not significantly different between the 2 groups (Table 3) (Figure 3F).
Factors Associated With Foramen Restenosis
Results of Logistic Analysis Demonstrating Factors Related to Foraminal Restenosis.
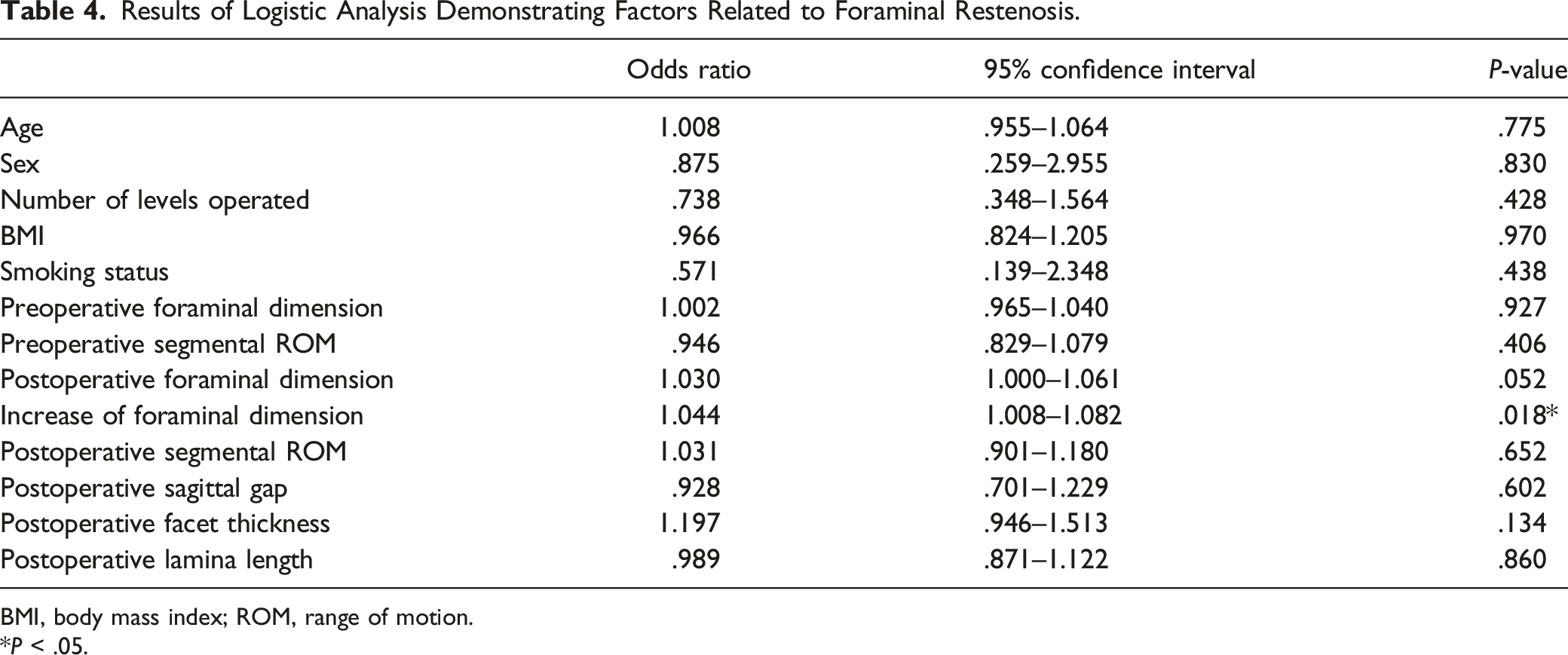
BMI, body mass index; ROM, range of motion.
*P < .05.
Discussions
Posterior cervical foraminotomy has proven to be an effective alternative of ACDF for the treatment of cervical radiculopathy due to its minimal invasiveness, safety, and potential to preserve motion.2,5,21 However, while patient symptoms have been proved to be favorable in long-term after PCF, not much is known regarding radiographic outcome. 19 Mizouchi et al 11 reported that foramen reclosure occurs for patients who underwent concomitant PCF and laminoplasty. However, radiographic fate of decompressed foramens that underwent PCF alone is unknown. Therefore, the present study aimed to demonstrate foramen reclosure after PCF and its clinical implications.
The present study demonstrated that foraminal narrowing occurred in 73.4% of operated segments. Even in segments that were classified as patent segment, 61.8% demonstrated mild narrowing of foramen. Therefore, it seems that narrowing of foramen due to bone regrowth is a common phenomenon after PCF. 11 Furthermore, since sagittal gap, facet thickness, and lamina length at postoperative 2 years demonstrated significant difference compared to postoperative 2 days measurements, the bone regrowth seems to occur in both sagittal and axial directions by growth of inferior articular process, medial facet, and lamina. However, medial facet regrowth would be a factor that contributes more to foraminal narrowing since facet thickness at postoperative 2 years demonstrated significant difference between the 2 groups. Mizouchi et al 11 also demonstrated that medial facet regrowth is a major factor that causes foraminal narrowing after PCF.
Another interesting finding is that it was not the foramens that underwent less widening that demonstrated restenosis, but the foramens that had greater widening tend to have foraminal restenosis. Furthermore, logistic regression analysis also demonstrated that increase of foraminal dimension is significantly related to foraminal restenosis. Chen et al 16 demonstrated that segmental instability is a factor that accelerates bone regrowth after lumbar decompression. Biomechanical studies also have reported that dilatational mechanical strain is a factor that promotes bone healing.22-24 Increased micromotion due to more bone loss in the restenosis segments might have resulted in accelerated bone growth during the follow-up. However, since postoperative segmental ROM did not demonstrate significant intergroup difference, this suggestion would need further verification. Therefore, although sufficient decompression according to the location and size of the pathology should be performed, additional excessive resection of facet and lamina would not be helpful since it would increase the chance of foramen narrowing in long-term. Many previous reports have suggested that at least 50% of facet joint should be preserved to preserve cervical stability.18,25,26 The result of the present study supports this suggestion in the point that excessive resection would lead to postoperative foraminal narrowing.
Segmental ROM significantly decreased both in the restenosis segments and the patent segments at 2-years follow-up. Cervical ROM also demonstrated significant decrease in both groups. Cho et al
27
also demonstrated that segmental ROM decreases after PCF although some degree of motion is preserved compared to ACDF. Since bone regrowth and foraminal narrowing is a common phenomenon as demonstrated in this study, bone healing at resected foramen could be a factor that causes ROM decrease. Segments that complete fusion have occurred due to bone healing were occasionally observed, which would have negative impact on cervical motion (Figure 4). Furthermore, while previous studies suggest that segmental instability can occur after PCF, the result of present study implies that segmental instability would not be a significant problem after PCF in long-term due to bone healing.25,26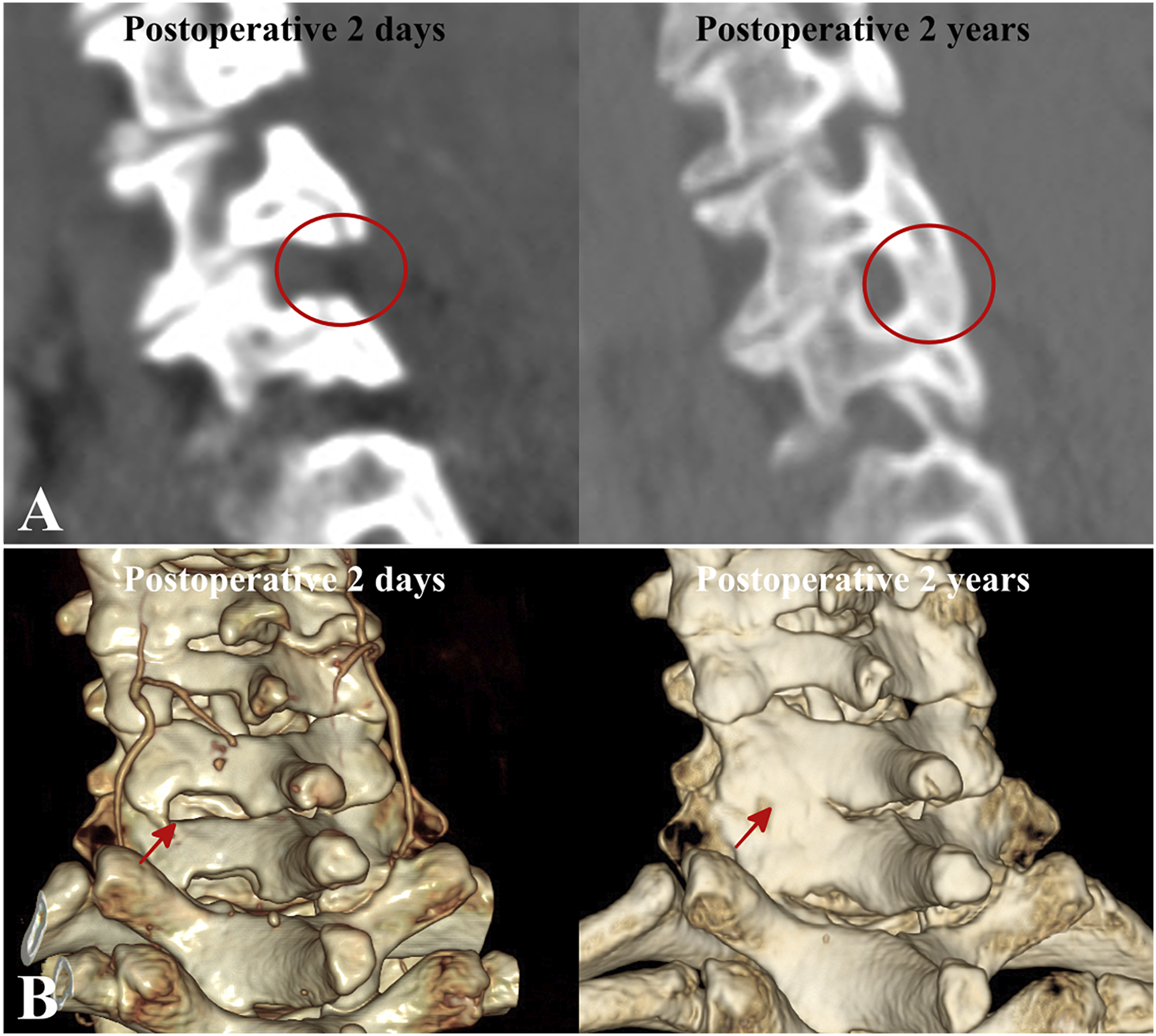
Although arm pain VAS and NDI demonstrated significant improvement at 2-years follow-up compared to preoperative scores both in the patent group and the restenosis group, neck pain VAS demonstrated different trend in the 2 groups. Restenosis group demonstrated significant aggravation of neck pain during the follow-up, and neck pain VAS at the 2-years follow-up was not significantly different from that of preoperative values. Therefore, restenosis of foramens would be a factor that adversely affects clinical outcomes. While arm pain is the main symptom of radiculopathy caused by foraminal stenosis, arm pain did not aggravate even in the restenosis group. 1 Dynamic neural foramen narrowing by segmental motion is closely related to radiculopathy, and recurrence of arm pain might not have occurred due to postoperative decrease in segmental motion despite foraminal restenosis. 28 Furthermore, foraminal dimension at the final follow-up was still greater than the preoperative value in both groups. Therefore, arm pain recurrence due to foramen restenosis would not be of great concern. However, the present study failed to demonstrate significant inter-group differences of patient reported outcome measures between the patent group and the restenosis group and no significant results were demonstrated with arm pain VAS or NDI. This might be due to small sample size at each group which warrants further clarification.
The present study involved a patient group who underwent PCF using a mini-open approach. Previous studies comparing open and minimally invasive approaches using tubular retractors demonstrated no significant difference in long-term outcomes between the 2 techniques, including neck and arm pain.19,29,30 While an additional muscle dissection is performed with open PCF, the amount of facet capsule injury and bone resection are similar between the 2 techniques.19,29,30 Therefore, foraminal restenosis is expected to occur regardless of approach, although further verification is needed. Although Dunn et al 2 suggested that minimally invasive PCF could prevent undesired bone growth and fusion, this study did not directly compare open and minimally invasive techniques.
In contrast to PCF, no further osteophyte growth or foraminal narrowing occurs after ACDF.31-33 ACDF eliminates segmental motion, which resists further degeneration and osteophyte enlargement, demonstrating a distinct radiographic course with PCF.31-33 Since PCF is a motion preservation surgery, it carries the potential for further degeneration and foraminal restenosis. 11 Furthermore, the present study’s findings suggest the possibility that foraminal restenosis after PCF might be related to the aggravation of neck pain. Nevertheless, previous studies have proven that PCF and ACDF are equally valuable treatment options for cervical radiculopathy and that long-term neck and arm pain do not differ significantly between them.3,5 Therefore, there is no need to avoid PCF and perform ACDF due to fear of foraminal restenosis after PCF, although further verification is needed to clarify whether distinct radiographic prognosis between the 2 surgical techniques would lead to different clinical outcomes.
The present study suggests a few clinical implications when posterior revision surgery is needed for patients who have undergone PCF. Firstly, covering the posterior surface of facet resulting from the restoration of resected inferior articular process might provide enough thickness for the insertion of lateral mass screws. Secondly, recovery of lamina thickness and length would decrease the possibility of hinge fracture when secondary laminoplasty is needed.
11
Therefore, posterior cervical fusion or laminoplasty need not be precluded due to previous history of PCF, and preoperative CT evaluation would be needed to confirm whether revision surgery could be safely performed (Figure 5).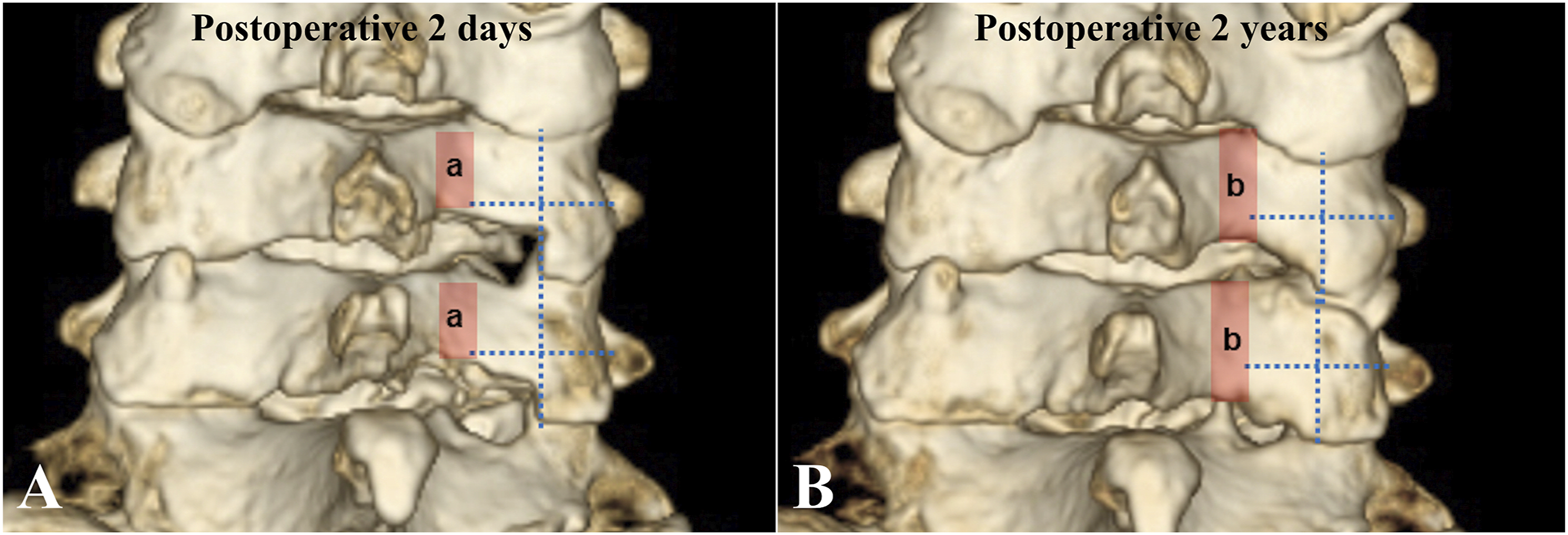
There are a few limitations in this study. Firstly, the measurement in the present study is based on 2-dimensional CT images only. Further evaluation using 3-dimensional volumetric approaches for measurement of bone growth could provide further information. Secondly, as previously mentioned, the study is with relatively small sample size in the patent group and the restenosis group which limits its efficacy to demonstrate statistical significance of patient reported outcome measures. Cervical radiculopathy caused by foraminal stenosis is more directly related to arm pain rather than neck pain, although the result of present study demonstrated significant result only for neck pain. While the present study suggests the possibility that foraminal restenosis after PCF is a factor that could adversely affect patient symptoms, further verification with larger sample size would be needed. Finally, the cutoff value of 20% was selected based on the mean value of foraminal restenosis rate demonstrated in the current study. Since not many studies have described foraminal restenosis phenomenon after PCF, we could not find previous reports that could provide reference point for analysis.
Conclusions
In conclusion, foraminal restenosis commonly occurs after PCF due to bone healing. Bone growth occurs in all directions while medial facet growth contributes more to foraminal restenosis. Greater widening of foramen during PCF is a risk factor for postoperative foramen restenosis. Therefore, amount of bone resection should be kept optimal and excessive resection should be avoided to prevent foraminal restenosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.