
Abstract
Study Design
Retrospective, cross-sectional
Objectives
To identify trauma patients with confirmed tears of the transverse atlantal ligament on cervical MRI and measure several parameters of atlanto-axial alignment on cervical CT, including the anterior atlantodens interval, to determine which method is most sensitive in predicting transverse atlantal ligament injury.
Methods
Adult trauma patients who suffered a transverse atlantal ligament tear on cervical MRI were identified retrospectively. The cervical CT and MRI exams for these patients were reviewed for the following: anterior and lateral atlantodens interval widening, lateral C1 mass offset, C1–C2 rotatory subluxation, and transverse atlantal ligament injuries on cervical MRI.
Results
Twenty-six patients were identified with a tear of the transverse atlantal ligament on cervical MRI. Twelve percent of these patients demonstrated an anterior dens interval measuring greater than 2 mm, 26% of patients demonstrated lateral mass offset of C1 on C2 (average offset of 2.4 mm), 18% of patients demonstrated an asymmetry greater than 1 mm between the left and right lateral atlantodens interval, and one patient demonstrated atlanto-axial rotation measuring greater than 20%. Ten patients had an accompanying C1 burst fracture and eight patients had a C2 fracture. One patient demonstrated widening of the atlanto-occipital joint space greater than 2 mm indicative of craniocervical dissociation injury.
Conclusions
An anterior atlantodens interval measuring greater than 2 mm is an unreliable methodology to screen trauma patients for transverse altantal ligament injuries and atlanto-axial instability. Moreover, C1 lateral mass offset, lateral atlantodens asymmetry, and atlanto-axial rotation were all poor predictors of transverse atlantal ligament tears.
Introduction
The transverse atlantal ligament (TAL) is a strong and thick, horizontally oriented ligamentous band that extends posterior to the C2 dens and inserts along the medial C1 tubercles. Anatomically, it is the major component of the cruciform ligament at C1–C2, along with the relatively weak superior and inferior longitudinal bands, and helps lock the dens in close apposition to the anterior arch of C1.1-3 Between the dens and TAL, a small synovial capsule exists that—along with the smooth, anterior fibrocartilaginous surface of the TAL—facilitates rotatory movement between C1 and C2. The TAL is considered one of the most important ligaments in the body. 4 Biomechanical research studies of the TAL have demonstrated the vital role of this strong, relatively inelastic ligament as the primary stabilizer of the atlanto-axial joint and the primary preventer of anterior subluxation of C1 on C2. 5
Radiologically, TAL injuries are traditionally inferred by widening of the anterior atlantodens interval (ADI) greater than 2 mm on cervical spine CT and plain film, and multiple large research studies have established normative values for the anterior ADI in pediatric and adult patients.6-10 Moreover, the neurosurgical literature has suggested a combined C1 lateral mass offset (LMO) greater than 6.9 mm in the setting of a C1 vertebral fracture (“Rule of Spence”) predicts TAL injury, however, this criteria has more recently been challenged.11-14
Clinically, TAL integrity plays a crucial role in the management of C1 ring fractures. Dickman et. al. asserts that TAL disruption in the setting of a C1 fracture necessitates prompt C1–C2 fusion since conservative, external bracing will not correct the insufficient TAL. 15 In addition, he developed a widely accepted classification scheme that divides TAL injuries into whether the injury occurs mid-substance (unstable and treated operatively with fusion) vs laterally with an associated C1 tubercle fracture (stable and treated conservatively with external bracing). 16
Given the widespread availability and utilization of cervical MRI to directly inspect the TAL and crucial importance of TAL integrity in neurosurgical management, we wanted to evaluate and measure several parameters of atlanto-axial alignment on cervical CT in the setting of established TAL injuries on follow-up cervical MRI. We hypothesize that anterior ADI widening greater than 2 mm on cervical CT is an unreliable methodology to evaluate for TAL injury and potential atlanto-axial instability.
Materials and Methods
A waiver of informed consent was granted by the IRB chairman to retrospectively evaluate the imaging and clinical findings of adult and pediatric trauma patients (<16 y/o) who suffered a TAL injury on cervical MRI exams. Twenty-six adults and one pediatric patient who presented to the ED between January 2016 and January 2021 with a confirmed TAL injury on cervical MRI were identified retrospectively by a keyword search of cervical spine radiology reports using Nuance mPower software using the keywords “transverse atlantal,” “transverse band,” and “cruciate ligament.” Confirmation of TAL injury were agreed upon in consensus by two CAQ certified neuroradiologists with dedicated experience and prior research in CCJ trauma and the anatomic and imaging appearance of the TAL. Inclusion criteria included all adult trauma patients with confirmed TAL injury on cervical MRI with a preceding cervical CT within 48 h. Exclusion criteria included pediatric patients, and patients without both CT and MRI exams performed within 48 h.
CT and MRI exams were performed using the standard departmental protocols. CT images were generated with .625 mm slice thickness and reconstructed using multiplanar bone and soft tissue algorithms (GE medical systems). MRI studies were performed on a 1.5 T magnet with a head and neck coil (Avanto, Siemens). Slice thickness was 3 mm and sagittal T1, T2, and STIR as well as axial T2, and T2 Multi-Echo Data Image Combination sequences were obtained.
TAL injuries were confirmed on T2 and STIR axial and sagittal MRI sequences when there was clear disruption of the normal T2 hypointense ligament and increased T2 signal within the ligament on at least two sequences. The TAL was also considered injured if the ligament was not visible with increased T2 signal present. The location of the TAL injury was recorded as right, left, midline, or bilateral in relation to the C2 dens (Figure 1). In cases of disagreement between neuroradiologists regarding TAL injury, the patient was not included in the data set. Quality of cervical MRI exams was graded at excellent, diagnostic, or non-diagnostic for ligamentous injury. Coronal illustration of the craniocervcial junction from a posterior orientation with cut posterior atlanto-occipital membrane and translucent (pink) tectorial membrane detailing the anatomic location of the transverse (atlantal) ligament inserting on the medial tubercles of C1.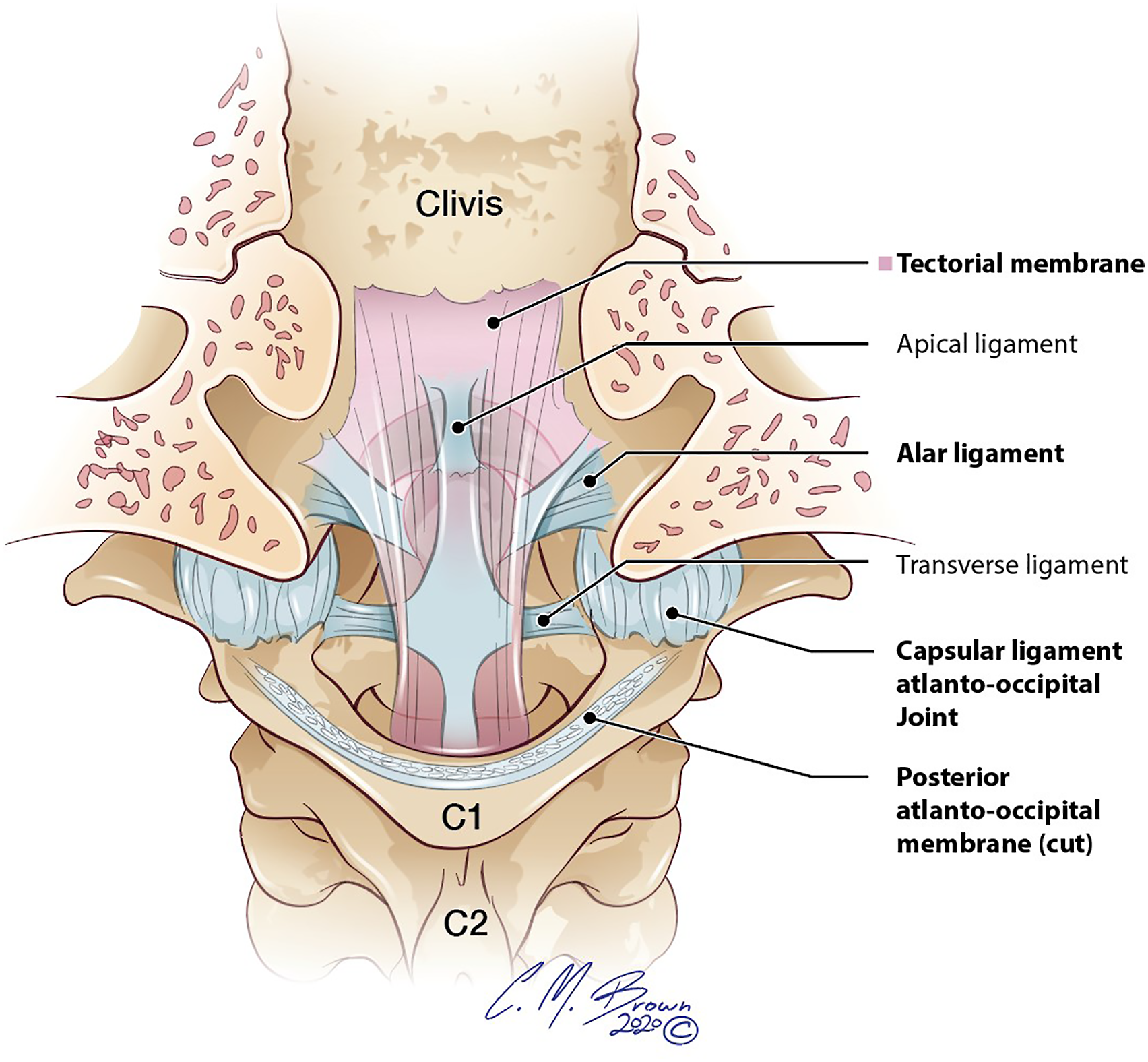
Several parameters assessing atlanto-axial alignment were evaluated and measured on the preceding cervical CT exams using sub-millimeter, multiplanar, orthogonal reconstructions, including anterior and lateral ADI, right and left C1 LMO, and atlanto-axial rotation (lineal method) (Figure 2). Concomitant C1–C2 fractures were recorded along with the presence of atlanto-occipital joint space widening. Sagittal CT image (top left) of the atlanto-axial joint demonstrating a normal anterior atlantodens interval (<2 mm) and coronal CT image (top right) demonstrating a symmetric lateral atlantodens interval (red lines) and absence of C1 lateral mass offset (white arrow). Axial T2 MEDIC (bottom left) and T2 weighted MRI images (bottom right) through the C1–C2 level demonstrating the transverse atlantal ligament (red arrows) posterior to the dens and inserting on the medial tubercle of C1. The transverse atlantal ligament is the major stabilizing ligament of the atlanto-axial joint.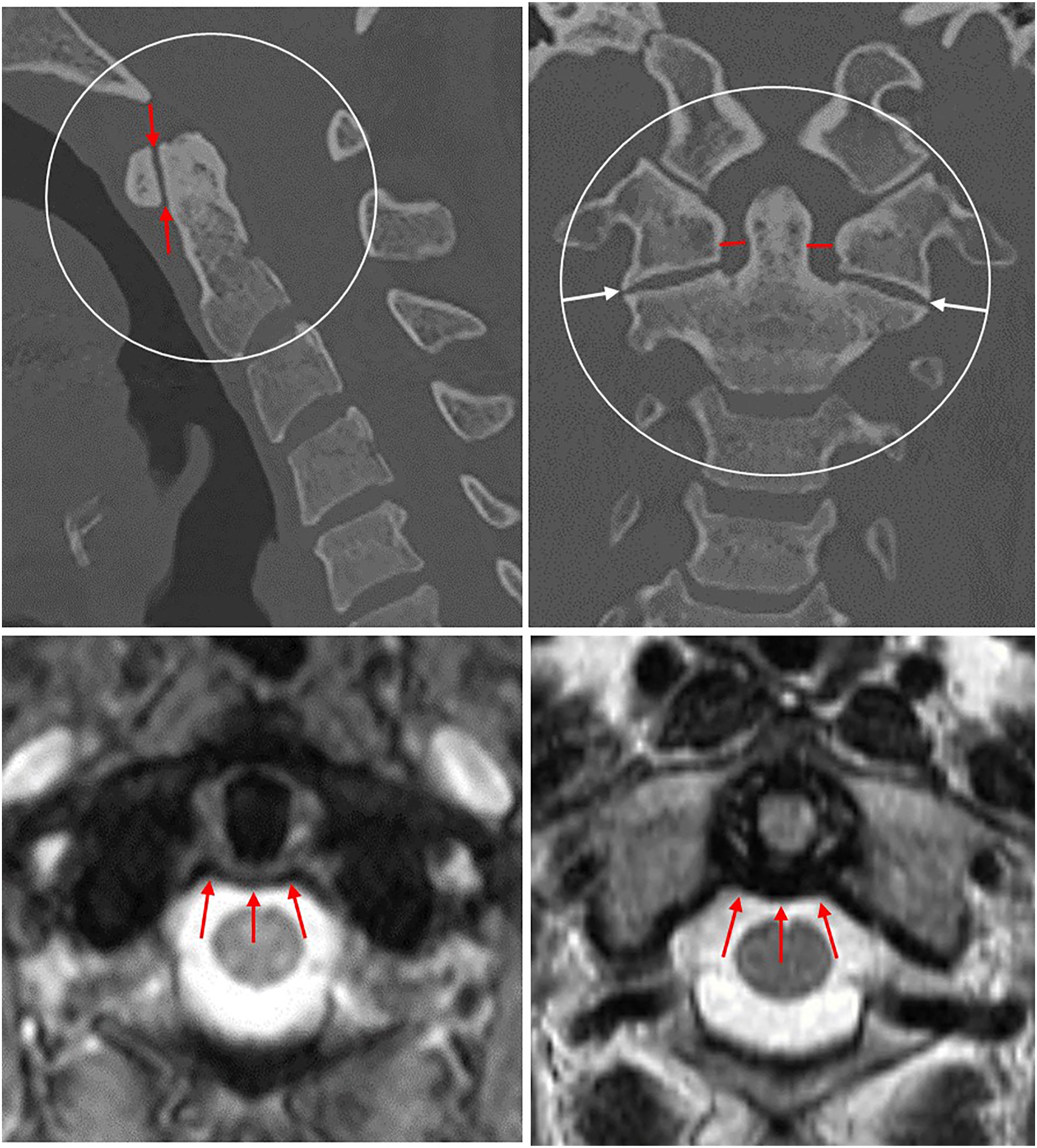
Electronic medical records were also reviewed for the following: (1) age and sex of patient, (2) mechanism of trauma, (3) management (surgery, external fixation, neck collar), and (4) clinical outcome (ambulatory, wheelchair, paretic, etc).
Results
Demographic information and additional imaging findings of patients with tears of the transverse atlantal ligament.
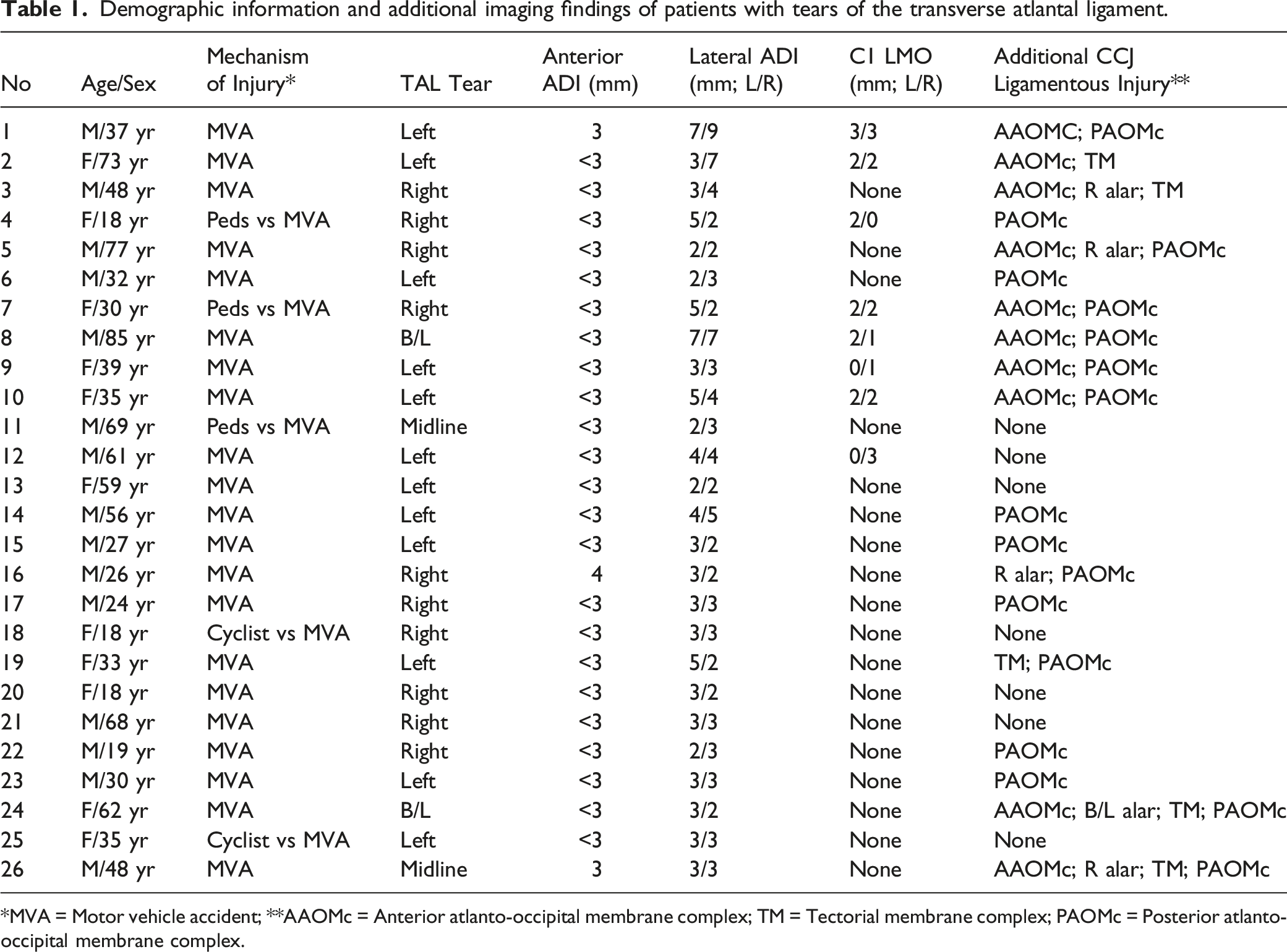
*MVA = Motor vehicle accident; **AAOMc = Anterior atlanto-occipital membrane complex; TM = Tectorial membrane complex; PAOMc = Posterior atlanto-occipital membrane complex.
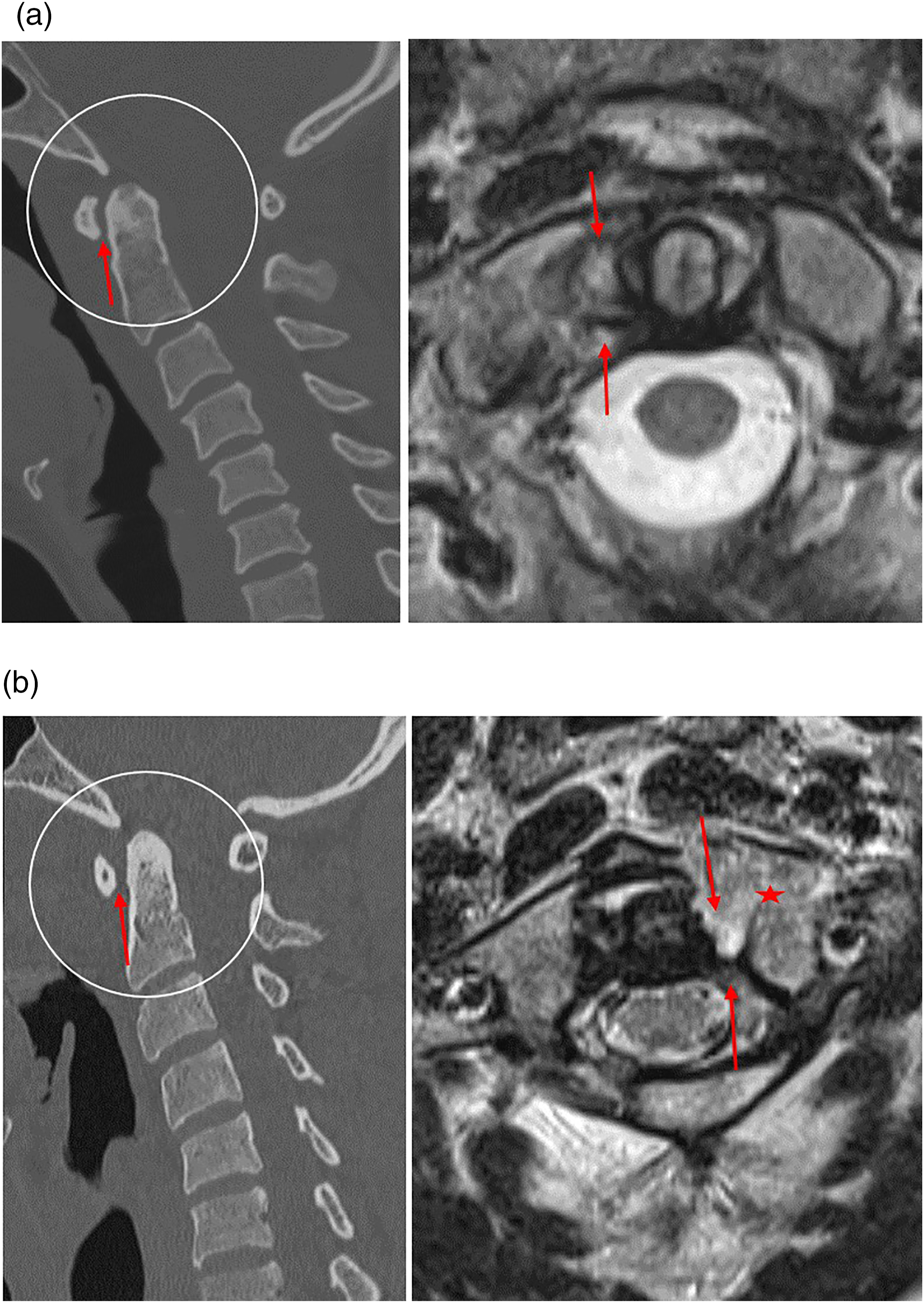
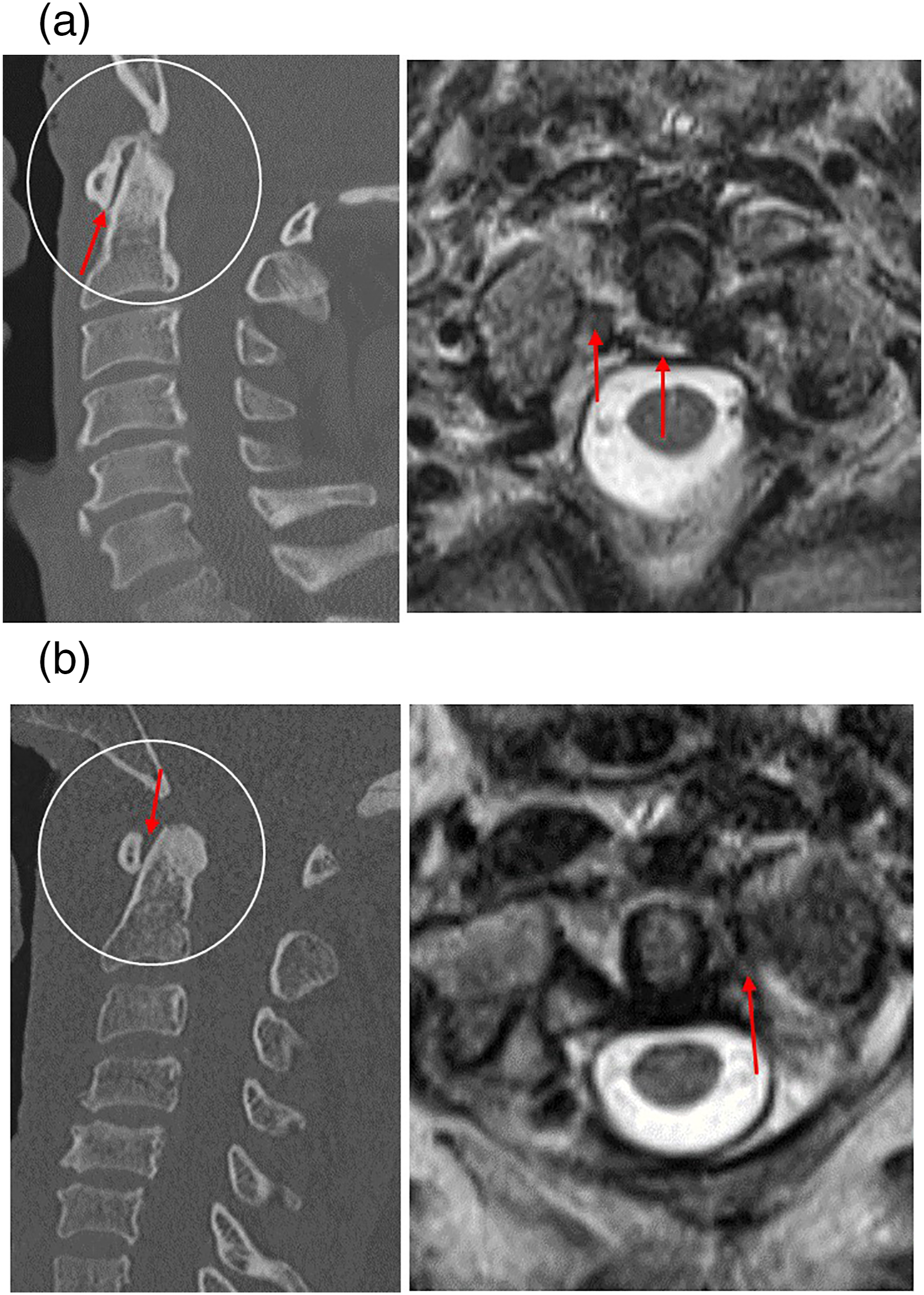
a: Sagittal CT image (left) of a 37-year-old trauma patient status post-motor vehicle accident. The anterior atlantodens interval measures within normal limits at less than 2 mm (red arrow). Corresponding axial T2 weighted MRI (right) through the C1–C2 level in the same patient however demonstrates a full thickness tear in the right transverse atlantal ligament (red arrow). b: Sagittal CT image (left) of a 32-year-old trauma patient status post-motor vehicle accident. The anterior atlantodens interval measures at the upper limits of normal at 2 mm (red arrow). Corresponding axial T2 weighted MRI (right) through the C1–C2 level in the same patient however demonstrates a left posterior arch and lateral mass C1 fracture (red star) and full thickness tear in the left transverse atlantal ligament.
a: Sagittal CT image (left) of a 56-year-old trauma patient struck by a motor vehicle. The anterior atlantodens interval is not widened (red arrow). Moderate atlanto-axial osteoarthritis is also present. Corresponding axial T2 weighted MRI (right) through the C1–C2 level in the same patient however demonstrates a full thickness tear in the central and right transverse atlantal ligament (red arrow). b: Sagittal CT image (left) of a 48-year-old trauma status post-motor vehicle accident. The anterior atlantodens interval measures less than 2 mm along the inferior joint space with slight widening along the superior joint space (red arrows). Moderate atlanto-axial osteoarthritis is present. Corresponding axial T2 weighted MRI (right) through the C1–C2 level in the same patients demonstrates a full thickness tear in the left transverse atlantal ligament (red arrow).
All injuries involved motor vehicles, either primary motor vehicle accidents or bicyclists/pedestrians struck by motor vehicles. Clinical management was variable and depended on concomitant traumatic injuries.
Discussion
Our study suggests that evaluating for anterior, lateral, and rotatory subluxation of the atlanto-axial joint on trauma cervical CT exams is an unreliable methodology to screen patients for TAL injury and potential atlanto-axial instability. The anterior ADI—which is the most commonly recognized measurement for atlanto-axial instability—was abnormal (greater than or equal to 3 mm) in only 11% of patients with a confirmed TAL injury. In addition, 70% of patients with a TAL injury demonstrated no evidence of anterior, lateral, or rotatory translation when measuring the combined anterior and lateral ADI, LMO at C1, and atlanto-axial rotation.
These research findings conflict with several previous, large, and robust studies which have attempted to define normative values for anterior ADI and atlanto-axial alignment on cervical CT in order to screen patients for cervical instability at C1–C2 and guide clinical management.17-20 Rojas et. al. evaluated 200 patients who underwent cervical CT and found that 95% of non-trauma patients demonstrated an anterior ADI measuring less than 3 mm. 21 Moreover, studies on the clinical management of atlanto-axial instability stress the importance of an anterior ADI measuring less than 3 mm as a primary way to evaluate trauma patients for TAL integrity on CT imaging. Given prior biomechanical studies describing the function of the TAL as the primary stabilizer of the atlanto-axial joint and the sole preventer of anterior subluxation, a “normal” anterior ADI on CT intuitively makes sense as a means to exclude atlanto-axial instability. However, with the increasing availability and utilization of cervical MRI to directly evaluate the integrity of the craniocervical ligaments, the accepted normal alignment of the CCJ and C1–C2 on cervical CT can now be further scrutinized.22,23 This point is especially salient for trauma patients with persistent neck pain and contraindications to undergoing cervical MRI.
Normative values on cervical CT for lateral ADI, C1 LMO, and atlanto-axial rotation have also been investigated as a potential method to evaluate for TAL integrity and atlanto-axial stability. Wolansky et. al. evaluated 99 non-trauma patients who underwent cervical CT for lateral ADI asymmetry and found the average asymmetry was .99 +/− 1.05 mm with a maximal asymmetry of 5 mm.
24
In addition, Mendenhall et. al. evaluated 540 pediatric non-trauma cervical CT exams and found a mean difference in right and left lateral ADI as .09 +/− 1.23 mm with maximal asymmetry of 4.87 mm.
25
In our 27 patient cohort with TAL injury on cervical MRI, only 14% of patients demonstrated a lateral ADI greater than 2 mm with a maximum lateral ADI of 4 mm in one patient; hence, our findings suggest no measurable difference in lateral ADI between non-trauma patients and those with TAL injuries (Figure 5). Although no known normative values for C1 lateral mass offset have been established on cervical CT, combined C1 LMO greater than 6.9 mm in the setting of a C1 ring fracture—known as the “Rule of Spence”—is still used to help predict TAL injury; however, more recent research studies using cervical MRI have found that this criteria drastically underestimates associated TAL injuries.13,26 Rotatory subluxation of C1 on C2 has demonstrated wide variability in prior studies with rotation measuring up to 70° in otherwise healthy patients.
27
Sagittal CT image (left) of a 42-year-old trauma status post-motor vehicle accident with slight widening of the anterior atlantodens interval measuring 3 mm (red arrow). Corresponding axial T2 weighted MRI (right) through the C1–C2 level in the same patients demonstrates a full thickness tear in the left transverse atlantal ligament (red arrow). Widening of the anterior atlantodens interval on cervical CT was an uncommon finding in patients with a transverse atlantal ligament tear on follow-up MRI.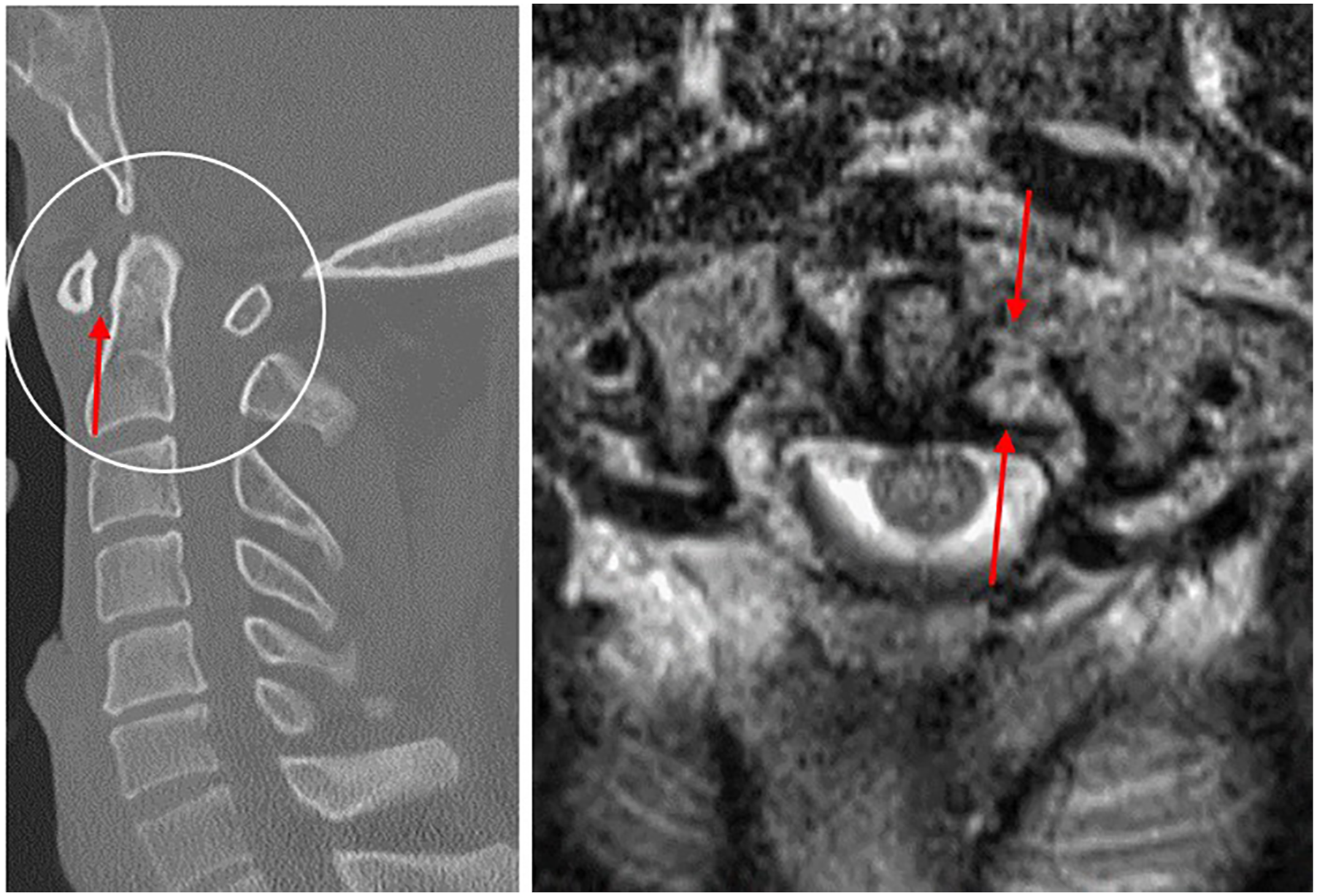
Understanding the role and limitations of cervical CT in determining TAL integrity and atlanto-axial stability is important for several reasons. First, TAL injuries play a determinative role in the management of patients with acute multifocal fractures of the C1 vertebrae—commonly known by their eponym as “Jefferson” fractures. Cervical MRI is commonly performed in these patients to assess the TAL for injuries as research from Dickman et. al. asserts that transverse ligament disruption in the setting of an atlas fracture requires C1–C2 fusion since an external brace will not correct the incompetence of the transverse ligament. 16 Our patient cohort included ten patients with concomitant Jefferson fractures with only one patient demonstrating anterior ADI widening (3 mm), three patients demonstrating lateral ADI asymmetry greater than 2 mm, and five patients demonstrating LMO. Interestingly, none of our patients with LMO would satisfy the “Rule of Spence.” These findings suggest that no one measurement of atlanto-axial alignment on cervical CT in the setting of C1 fracture is reliable in predicting TAL injury. Secondly, the limitations of CT in determining atlanto-axial stability underscores the importance of prompt cervical MRI evaluation of the ligamentous integrity of the CCJ and upper cervical spine in certain high-velocity trauma populations, since the early diagnosis of unstable CCJ injuries and treatment with surgical stabilization has shown to greatly reduce neurologic deterioration and death.28,29
Several potential reasons may account for our research findings. As a static exam in patients braced with a cervical neck collar, cervical CT may underestimate the degree of anterior or lateral subluxation at the atlanto-axial joint by the injury being partially reduced by external neck support. Additionally, secondary stabilizers, including the facet capsule, alar ligaments, and surrounding neck musculature may help restore anatomical congruence and play a role in stabilizing the C1–C2 joint in addition to the TAL. This concept is supported by current research studies in the neurosurgical literature that TAL disruption does not inherently lead to C1–C2 instability in the setting of C1 Jefferson fracture.12,14,30,31 Thus, TAL-deficient C1 fractures are now sometimes being treated more conservatively challenging the long-held assertion by Dickman et. al. that TAL disruption in the setting of a C1 fracture necessitates prompt C1–C2 fusion. Finally, poor MRI resolution related to motion artifact or spinal hardware may impair the radiologist’s ability to properly inspect the TAL. In our experience, TAL injuries tend to be over-called on cervical MRI related to the widely acknowledged importance of the TAL in maintaining atlanto-axial alignment and radiologist fear of “missing” a TAL injury.
Our study had several limitations. First, although to our knowledge we collected the largest cohort of TAL injuries on cervical MRI, it is possible we did not capture all patients with a TAL injury on cervical MRI leading to potential selection bias. Secondly, we did not specifically evaluate for other CCJ ligamentous injuries on MRI, such as the alar ligaments or the capsular atlanto-occipital ligaments, which could potentially affect atlanto-axial alignment. However, this was deliberate since we wanted to concentrate solely on the effect of a torn TAL on C1–C2 alignment; thus, we may have been influenced by some degree of confirmation bias. Thirdly, there were variations in MRI exam quality, although all exams were designated as diagnostic in quality for ligamentous injury. Finally, since our analysis was retrospective, the possibility of interpreter error and reinforcement bias is possible. A multi-institutional research study utilizing a larger patient population would be beneficial to further determine the utility of anterior atlantodens interval widening in determining TAL integrity.
Conclusion
The TAL is a vital ligament that serves as the primary stabilizer of the atlanto-axial joint and the sole preventer of anterior subluxation of C1 on C2. TAL integrity is a crucial determining factor in the clinical management of C1 fractures. Based on our research, anterior ADI widening along with lateral ADI asymmetry, C1 LMO, and atlanto-axial rotation are poor predictors of transverse atlantal ligament tears. Our findings underscore the importance of cervical MRI to directly evaluate the TAL in the diagnostic workup and management of patients with acute, high-velocity cervical spine trauma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.