
Abstract
Study Design:
Retrospective cross-sectional study.
Objectives:
To determine if pre-operative albumin and CRP can predict post-operative infections after lumbar surgery.
Methods:
Patients who underwent an anterior lumbar interbody fusion (ALIF), posterior lumbar interbody fusion (PLIF), or lumbar discectomy were identified using a patient record database (PearlDiver) and were included in this retrospective study. Patients were stratified by Charlson Comorbidity Index (CCI) scores and pre-operative albumin and CRP status. Post-operative complications included deep infections and urinary tract infections within 3 months of the surgery and revisions within 1 year of the surgery.
Results:
74,280 patients were included in this study. 21,903 had pre-operative albumin or CRP lab values. 7,191 (33%), 12,183 (56%), and 2,529 (12%) patients underwent an ALIF, PLIF, and a lumbar discectomy, respectively. 16,191 did not have any complication (74%). The most common complication was UTI (16%). Among all patients, hypoalbuminemia was a significant risk factor for deep infection and UTI after ALIF, deep infection, UTI, and surgical revision after PLIF, and deep infection after lumbar discectomy. Elevated CRP was a significant risk factor for deep infection after ALIF, UTI after PLIF, and deep infection after lumbar discectomy in patients with a CCI ≤ 3.
Conclusions:
Pre-operative hypoalbuminemia and elevated CRP were significant risk factors for deep infection, UTI, and/or revision, after ALIF, PLIT, and/or lumbar discectomy. Future studies with a larger population of patients with low albumin and high CRP values are needed to further elaborate on the current findings.
Introduction
The World Health Organization (WHO) has estimated that 4-33% of the world’s population suffers from low-back pain, the most prevalent musculoskeletal condition. 1 The total cost of low-back pain in the United States has been estimated to cost over 100 billion dollars per year with less than 5% of patients accounting for 75% of the total costs. 2 Additionally, a recent study states that the prevalence of elective lumbar fusion surgery increased from 60.4 per 100,000 US adults to 79.8 per 100,000 US adults between 2004 and 2015. 3
Compared to conservative management, instrumentation surgery of the lumbar spine is associated with complication rates as high as 19%. 4 Common post-operative complications of lumbar surgery include pseudarthrosis, hardware failures, radiculopathies, wound infections, and urinary tract infections.4,5 Pre-operative risk factors include obesity, smoking history, diabetes mellitus, chronic obstructive pulmonary disease, osteoporosis, and malnutrition among others.5-7
A widely used marker to assess malnutrition is albumin, which is also a well-studied marker of inflammation and chronic disease.8-10 Previous studies have looked at preoperative values of hypoalbuminemia as markers for postoperative complications in lumbar spine procedures. In elderly Medicare patients receiving posterior lumbar interbody fusion (PLIF), poor nutritional status, as measured by albumin, within 3 months prior to surgery had more major medical complications within 90 days, a higher 1-year mortality rate, and increased infection and wound dehiscence. 11 Another study found that pre-operative hypoalbuminemia was significantly associated with an increased risk of operative mortality, any complication, sepsis, and prolonged length of stay among other complications after surgical decompression of spinal metastases. 12 In a study on adult lumbar deformity surgeries using the National Surgical Quality Improvement Program (NSQIP) database, hypoalbuminemia showed to be a risk factor for mortality, increased length of stay, any complications, and 30-day mortality. 13 On the other hand, a single institution study demonstrated that a low preoperative albumin level may be a risk factor for surgical site infections (SSI) in spine surgeries overall, but it was not seen to be statistically significant. 14 Additionally, a retrospective analysis of patients undergoing PLIF in the NSQIP database did not find low serum albumin to be a significant predictor of postoperative complications. 15 However, another NSQIP database study showed a 4.8% incidence of hypoalbuminemia, which was also predictive of wound dehiscence and SSI. 16 The relationship between hypoalbuminemia and poor outcomes is not fully understood. It is postulated to be related to low nutrition, decrease in vital functions, hyperinflammation. 17 It may also be due to the hypermetabolic state associated with spinal cord injuries, which may be intensified after surgery. 18
Another promising preoperative marker is C-reactive protein (CRP), a recognized marker of inflammation. 19 Elevated postoperative CRP has been extensively studied as a predictive marker for infections and complications,19-22 but the utility of preoperative CRP has not yet been fully explored in spine surgeries. Larger differences between preoperative and postoperative CRP was associated with a higher risk of postoperative complications in lumbar fusion procedures in a single center study. 23 A single center study that included all types of spinal surgery found that preoperative CRP was not shown to be predictive of postoperative SSI. 15
Many of the existing studies investigating the relationship between pre-operative serum albumin or CRP levels and post-operative infections are single institution studies or do not analyze pre-operative serum albumin or CRP as risk factors after specific spine surgeries. Additionally, one challenge large retrospective database studies face is the ability to control for patient co-morbidities, as stratifying patients by their individual medical conditions would significantly reduce the sample size. One comprehensive and reliable metric to control for this is the Charlson Comorbidity Index (CCI) score, a cumulative score predicting 10-year survival factoring in patient age and history of various cardiac, pulmonary, and other comorbidities that is frequently used to stratify patient’s risk pre-operatively. 24 Therefore, this large, retrospective database study aimed to determine if albumin and CRP can be predictors of post-operative infections and revisions after anterior lumbar interbody fusion (ALIF), posterior lumbar interbody fusion (PLIF), or lumbar discectomy in a patient population stratified by CCI score.
Methods
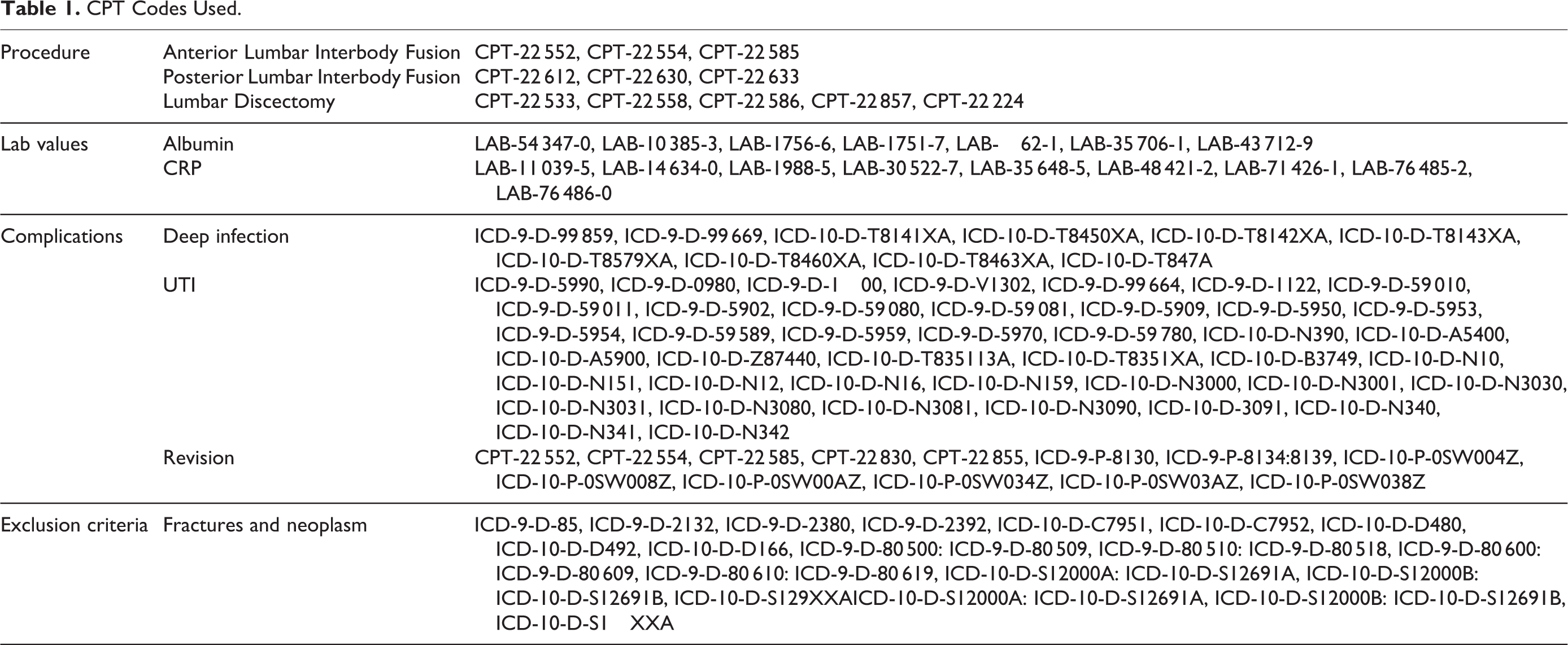
In this retrospective database study, we hypothesized that patients with low pre-operative albumin or elevated pre-operative CRP would have increased post-operative complication rates including deep infection and UTI within 3 months of surgery and surgical revision within 1 year of surgery. Data was extracted using the Humana Insurance database within PearlDiver, which is a large database consisting of over 25 million Health Information Portability and Affordability Act compliant patient records spanning across private and public health insurance policies. All patients undergoing an ALIF, PLIF, or lumbar discectomy with pre-operative labs between January 1, 2007 and March 31, 2016 were selected for the study (Table 1). In accordance to CCI score classification with CCI scores of 1-2 being mild, 3-4 being moderate, and ≥ 5 being severe, patients were stratified into one group consisting of patients with a CCI ≤ 3 and the other with a CCI > 3. 25 Based on their pre-operative lab values, patients were further stratified into either a normal albumin (3.5-5.4 g/dL), low albumin (<3.5 g/dL), normal CRP (<1.0 mg/dL), or high CRP (≥ 1.0 mg/dL) group (Figure 1). In order to maintain patient anonymity, all groups returned by PearlDiver that had 11 or fewer patients did not report the specific number of patients.
CPT Codes Used.
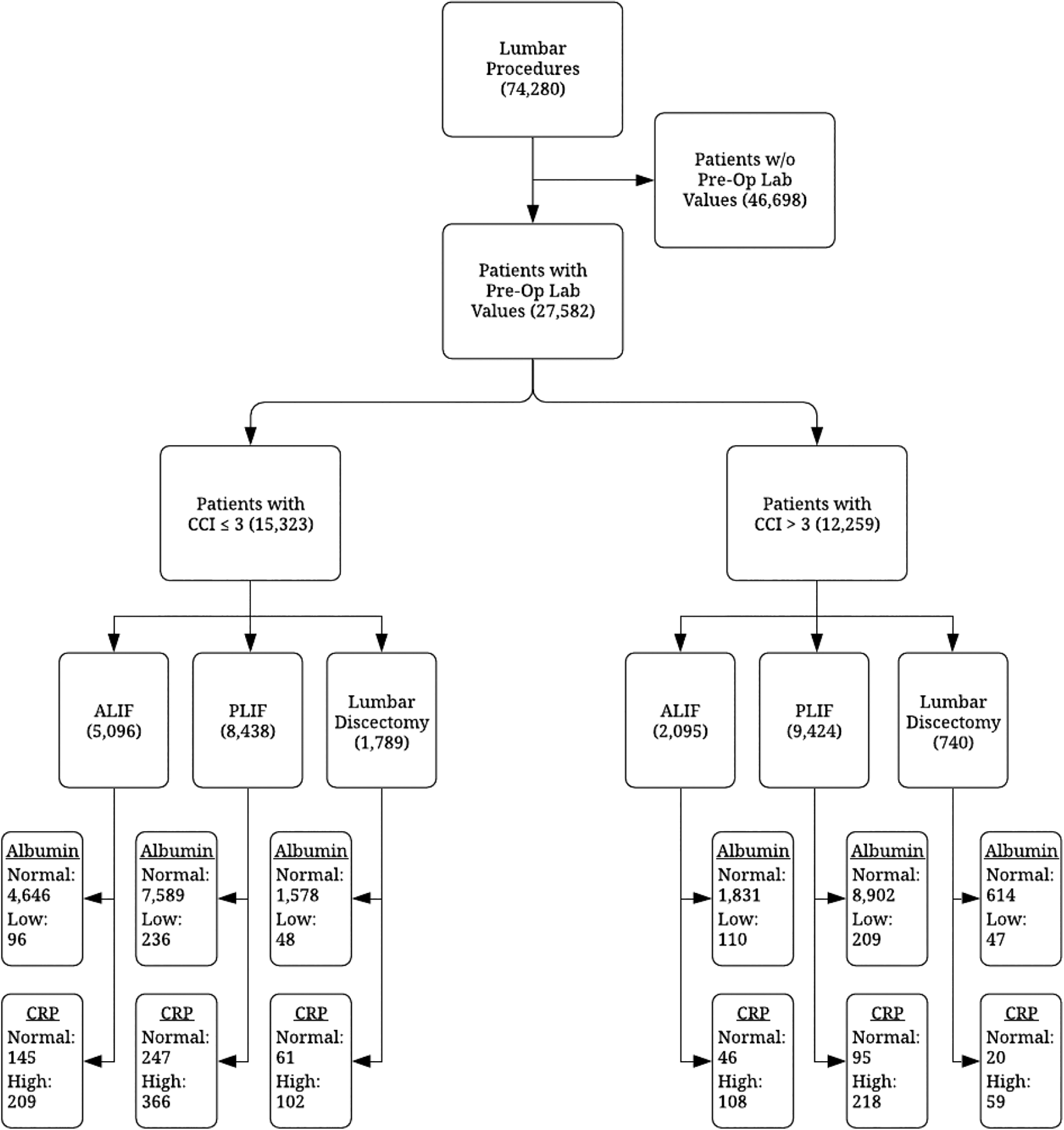
Flow diagram of study design.
Complication rates for deep infection and urinary tract infection (UTI) within 3 months of surgery and surgical revisions within 1 year of surgery were measured for each group (Table 1). All odds ratios were calculated using the R statistical program through PearlDiver. Chi-square analysis was used to identify the significance of complication rates. 95% confidence intervals (CI) were calculated for all risk ratios by using an alpha level of P ≤ 0.05.
Results
A total of 74,280 patients were included in this study, of which, 21,903 (30%) had either pre-operative albumin or CRP measured within 3 months of surgery. 7,191 (33%), 12,183 (56%) and 2,529 (12%) patients had undergone an ALIF, PLIF, and lumbar discectomy, respectively. Furthermore, 3% (n = 746) of all patients with pre-operative albumin measured had low albumin and 5% (n = 1062) of all patients with pre-operative CRP had elevated CRP levels. 56% (n = 15,343) of all patients who underwent surgery had a CCI ≤ 3 and 74% (n = 16,191) of all patients did not have a complication (Tables 2 and 3). Patients with a CCI ≤ 3 were significantly less likely to have any post-operative complication compared to patients with a CCI > 3 (23.1% vs. 33.0%, respectively; P < 0.001).
Demographic Data for Patients With Pre-Operative Albumin.
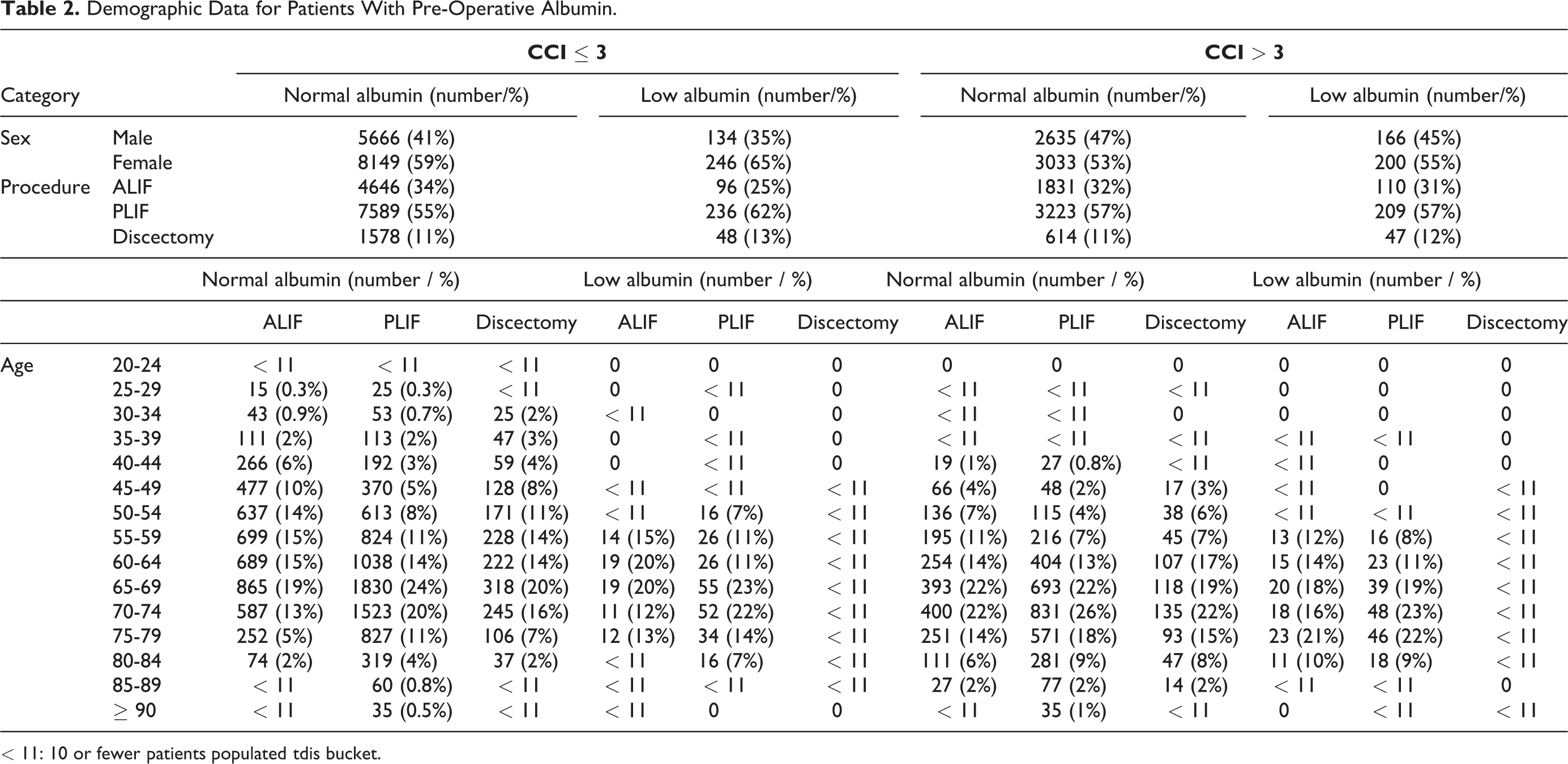
< 11: 10 or fewer patients populated tdis bucket.
Demographic Data for Patients With Pre-Operative CRP.
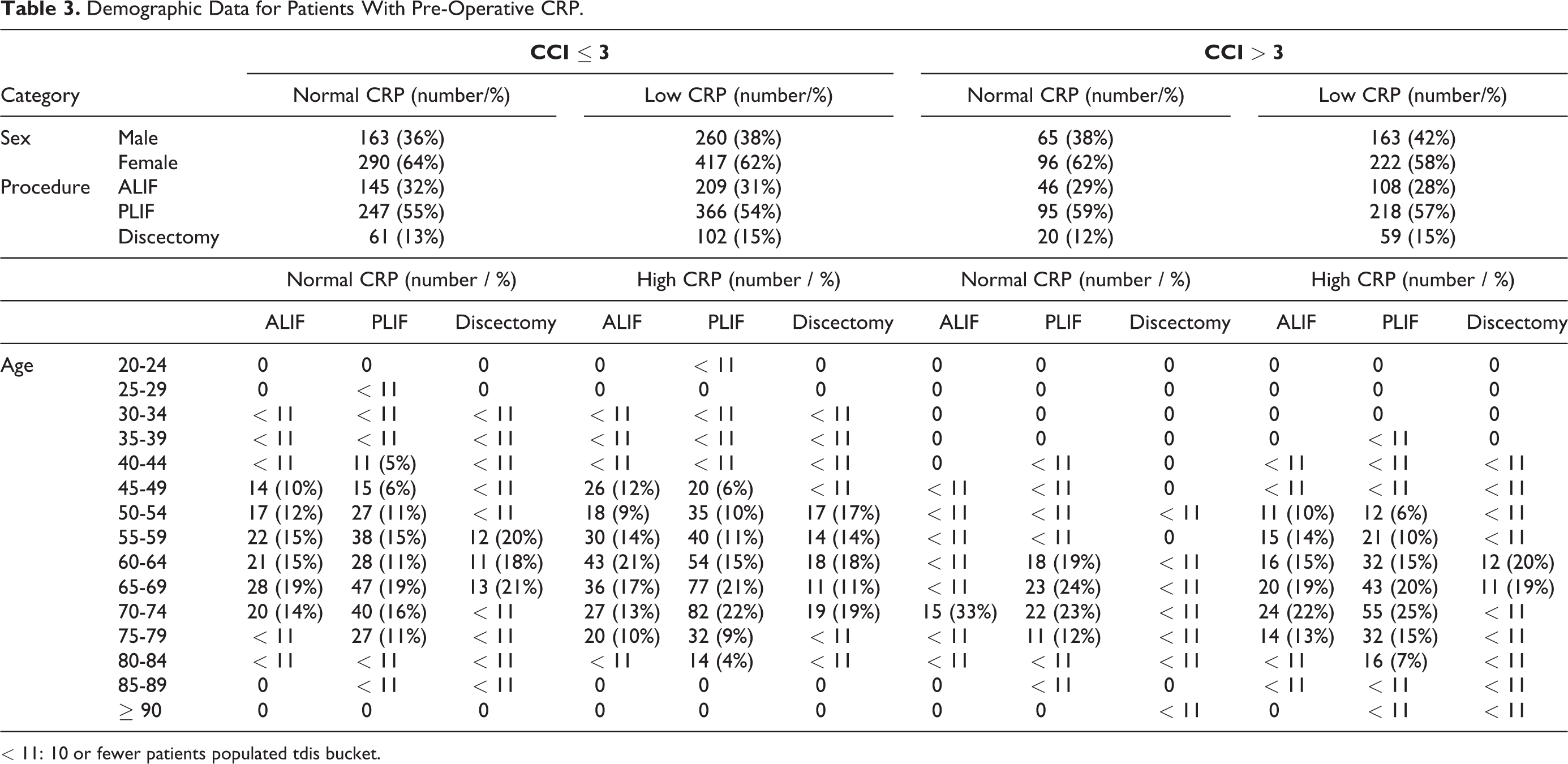
< 11: 10 or fewer patients populated tdis bucket.
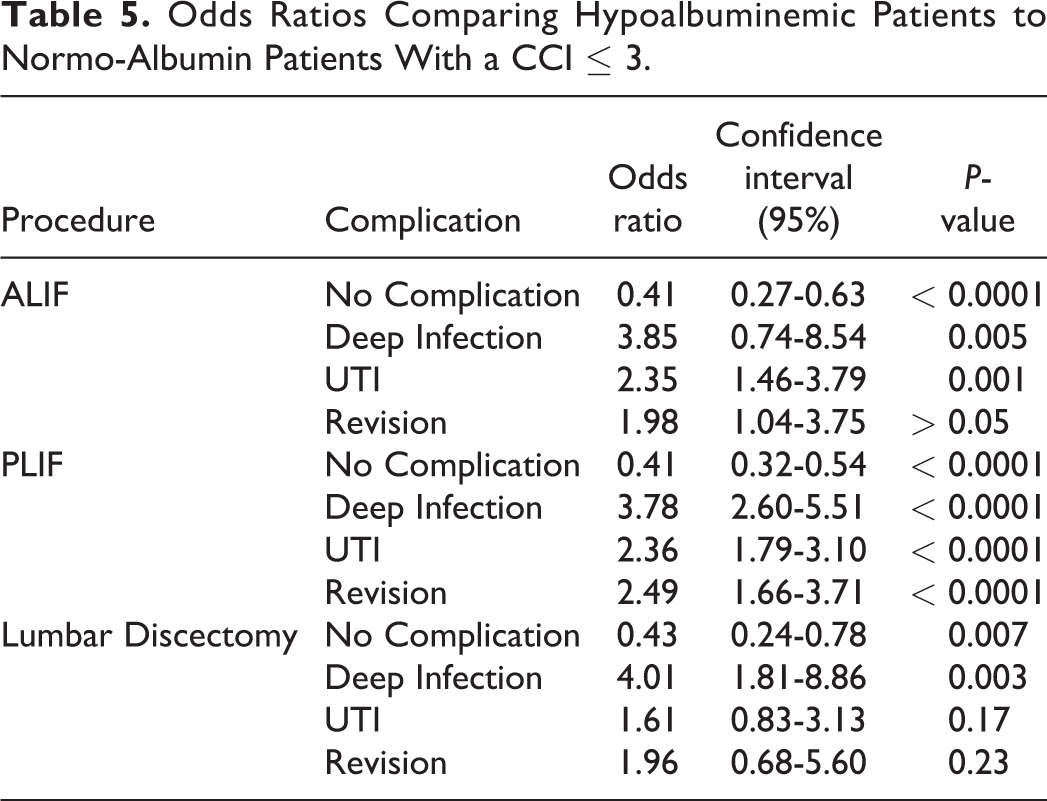
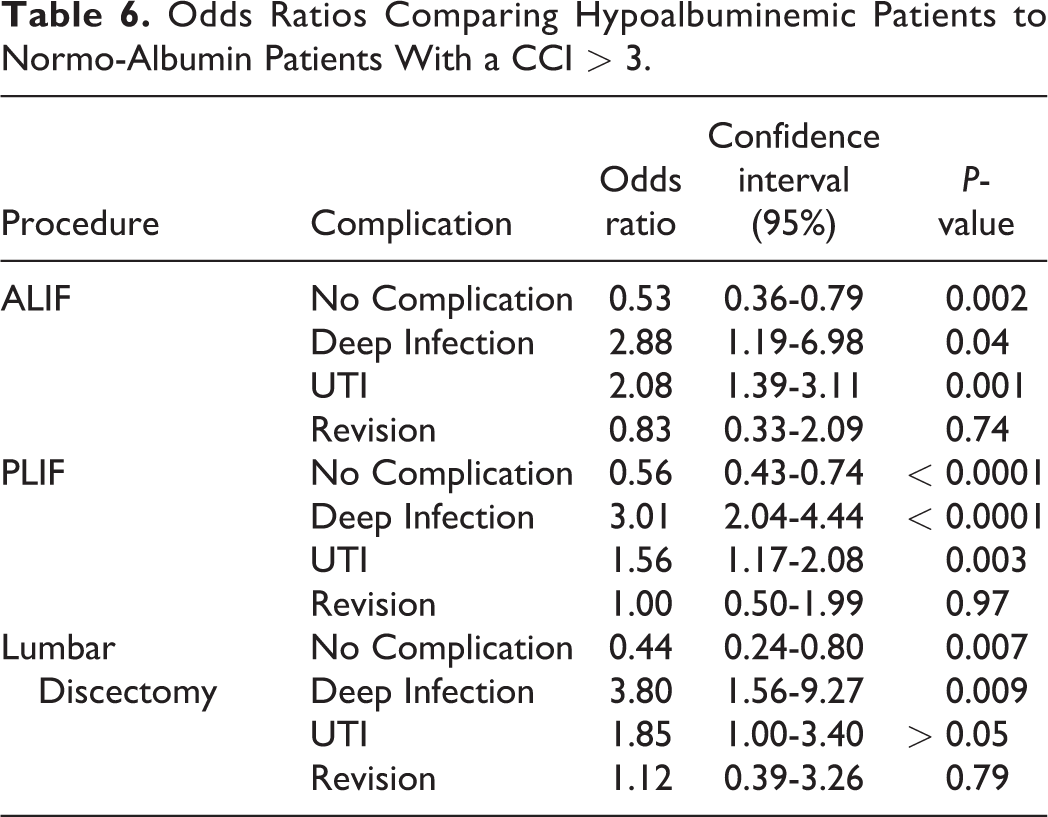
Hypoalbuminemic patients had a UTI complication rate as high as 40% and a deep infection rate as high as 17% in patients with a CCI > 3 who underwent lumbar discectomy and PLIF, respectively (Table 4). In patients with a CCI ≤ 3, hypoalbuminemic patients were at significant risk of having a UTI (OR 3.03, CI 1.39-6.37, P < 0.005) after ALIF and deep surgical site infection (OR 3.85, CI 2.63-5.56, P < 0.0001), UTI (OR 2.38, CI 1.82-3.13, P < 0.0001), and surgical revision (OR 2.44, CI 1.61-3.57, P < 0.0001) after PLIF (Table 5). Similarly, in patients with a CCI > 3, hypoalbuminemia was significant risk factor for UTI (OR 1.92, CI 0.93-3.85, P < 0.05) after ALIF, deep infection (OR 2.94, CI 1.96-4.35, P < 0.0001) and UTI (OR 1.52, CI 1.14-2.04, P < 0.005) after PLIF, and deep infection (OR 3.57, CI 1.25-10.00, P < 0.05) and UTI (OR 1.72, CI 0.89-3.33, P < 0.05) after lumbar discectomy (Table 6).
Complication Rates.
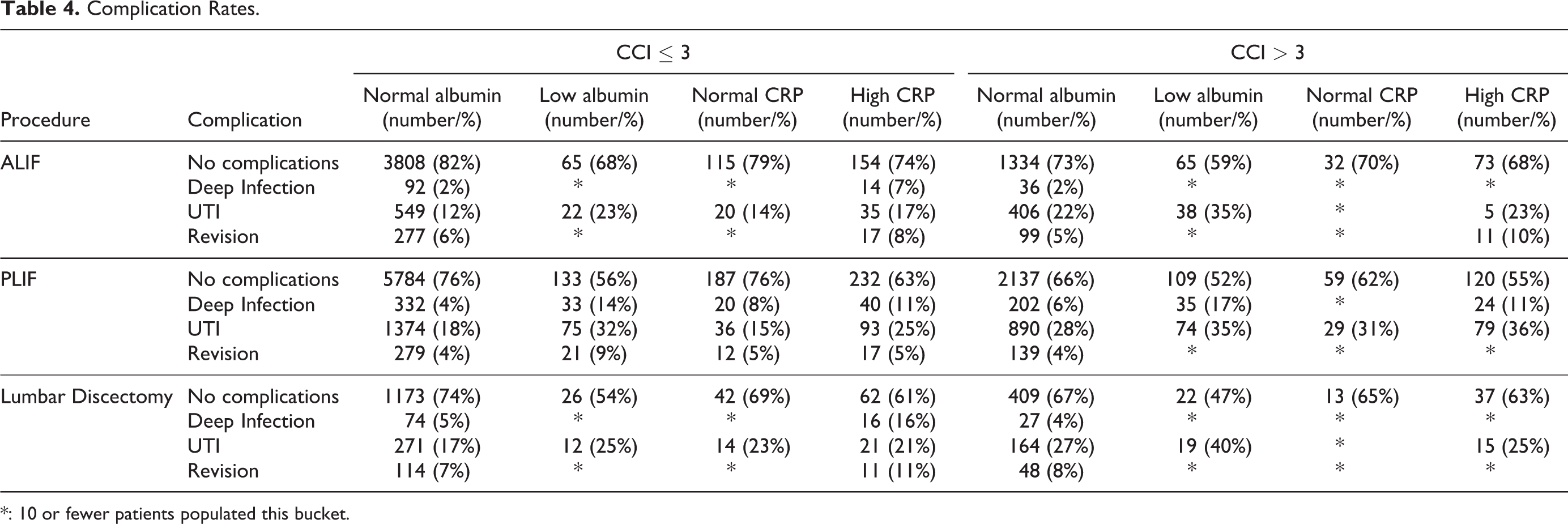
*: 10 or fewer patients populated this bucket.
Odds Ratios Comparing Hypoalbuminemic Patients to Normo-Albumin Patients With a CCI ≤ 3.
Odds Ratios Comparing Hypoalbuminemic Patients to Normo-Albumin Patients With a CCI > 3.
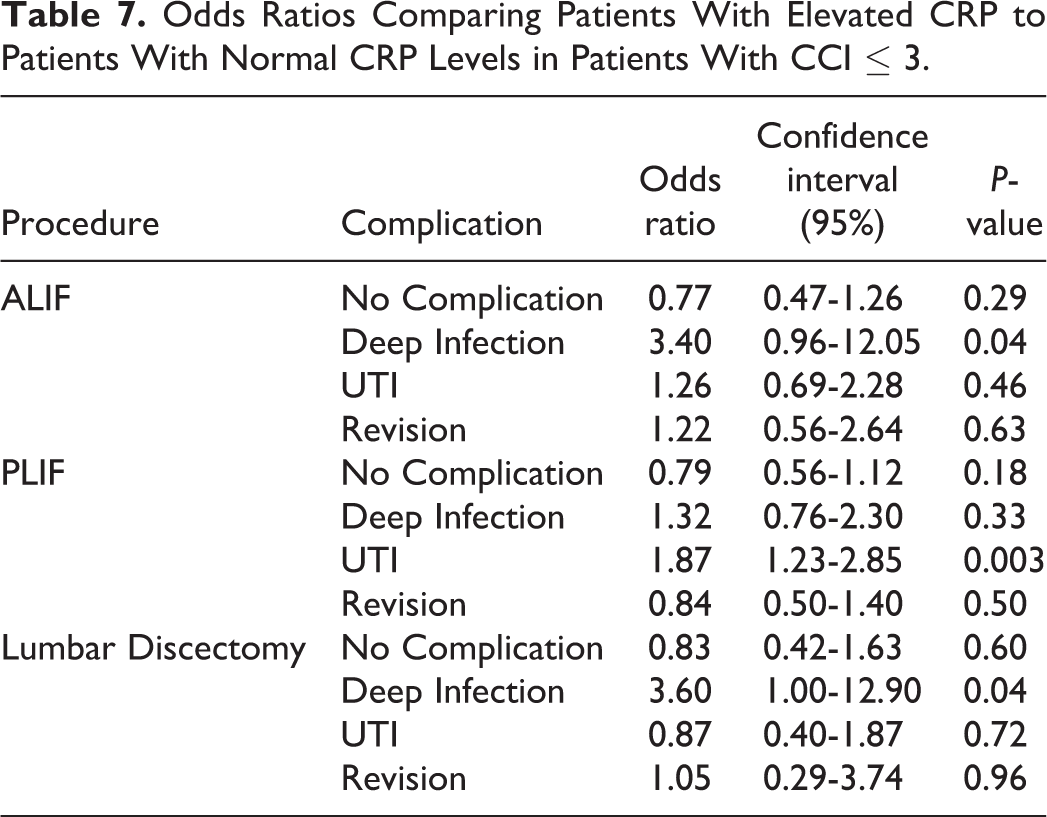
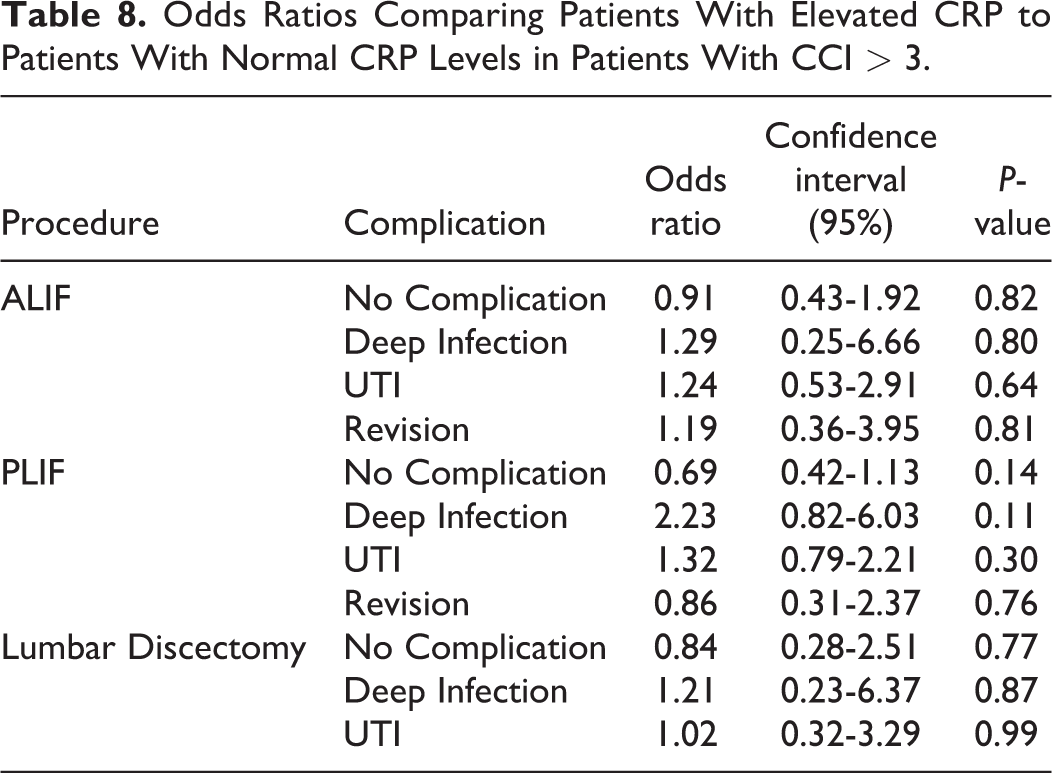
Patients with elevated CRP had UTI complication rates as high as 36% in patients with a CCI > 3 after undergoing PLIF. Deep infection had the second highest complication rate at 11% among patients with an elevated pre-operative CRP after PLIF. The revision rate for patients with elevated pre-operative CRP and a CCI > 3 after ALIF was 10%, the highest of all patient populations. Elevated CRP was a significant risk factor of having deep infection (OR 3.40, CI 0.96-12.05, P < 0.05) after ALIF, UTI (OR 1.85, CI 1.23-2.78, P < 0.005) after PLIF, and deep infection (OR 3.60, CI 1.00-12.90, P < 0.05) after lumbar discectomy in patients with a CCI ≤ 3 (Table 7). Furthermore, patients with a CCI > 3 and elevated pre-operative CRP were less likely to have no post-operative complications after PLIF compared to patients with normal pre-operative CRP but this was not statistically significant likely due to insufficient sample size (Table 8).
Odds Ratios Comparing Patients With Elevated CRP to Patients With Normal CRP Levels in Patients With CCI ≤ 3.
Odds Ratios Comparing Patients With Elevated CRP to Patients With Normal CRP Levels in Patients With CCI > 3.
Discussion
In the current study low pre-operative albumin and elevated pre-operative CRP were statistically significant risk factors for deep surgical site infection, UTI, and/or surgical revision depending on the type of surgery. Generally, hypoalbuminemic patients were approximately 2 to 4 times as likely to have a deep surgical site infection, 1 to 3 times as likely to have a UTI, and almost 3 times as likely to undergo a revision within 1 year of PLIF. Likewise, patients with elevated pre-operative CRP were at similar increased risks for deep surgical site infection and UTI.
Hypoalbuminemia, despite little conflicting evidence, 26 is a reliable marker for assessing patient malnutrition8,9 as well as inflammation and chronic disease. 10 As a result, previous studies have investigated the effects of pre-operative serum albumin levels on operative mortality and morbidity. 27 Specifically within orthopedics, low pre-operative serum albumin levels are associated with greater morbidity, mortality, and length of stay after hip fracture, 28 greater superficial site and deep infection risk after spine surgery29,30 and total joint arthroplasty,29-31 and spine surgery revision. 32
Pre-operative hypoalbuminemia was previously reported as an independent risk factor for post-operative complications including but not limited to UTI, pneumonia, deep and superficial surgical site infections, and sepsis after elective and non-elective anterior or posterior spinal fusion. 33 Lakomkin et al. found that abnormal pre-operative albumin had an odds ratio of 2.52 for major post-operative complications including deep wound infections, organ space infections, and sepsis, among other complications, after posterolateral lumbar fusion and an odds ratio of 2.26 for minor complications, including superficial wound infections, pneumonia, UTI, and wound dehiscence. 15 Looking at surgical site infection specifically, Liu et al. showed that both pre-operative and post-operative hypoalbuminemia were associated with increased risk of infection after posterior lumbar spinal surgery. 34 For anterior lumbar interbody fusions, low albumin had an odds ratio of 5.93 and 5.35 for UTI and sepsis, respectively, in a previously published study. 35 Finally, Bohl et al. calculated an adjusted risk ratio of 2.3 and 2.5 for surgical site infection and UTI, respectively, after posterior lumbar spinal fusions in hypoalbuminemic vs. non-hypoalbuminemic patients. 16 Of the existing literature, only one study did not find pre-operative albumin to be a risk factor for post-operative complications. 36 Additionally, our study reports a greater complication rate for deep infection after ALIF and PLIF compared to the existing literature.37,38 Specifically, study by Mehren et al reported a deep infection rate after ALIF as low as 0.37% in a single center study. 39
Identifying hypoalbuminemic patients and delaying surgery whenever possible not only decreased morbidity and mortality rates on the patient but also leavens the financial burden of hospitalization and increased patient quality of care. One study from 2002 stated that the median total direct cost of hospitalizations per infected patient rose from $6,646 in an uninfected patient to $24,344 in a patient with a surgical site infection. 40 While another study states that the difference in daily total charges was not statistically significant, length of stay for patients who had a surgical site infection rose from 5.64 days to 10.56 days. Additionally, 30-day readmission rates increased from 8.19 to 51.84 readmissions per 100 procedures, resulting in a change in profit due to surgical site infection of $2,268,589. 41
Compared to albumin, CRP was not as strong of a predictor for post-operative complications. While CRP is also an acute phase reactant and therefore a marker for acute and chronic inflammatory states,42,43 CRP was a significant risk factor for only deep infection after anterior lumbar interbody fusion and UTI after posterior lumbar interbody fusion in patients with a CCI ≤ 3. We suspect that this is due to our low power returned for all patients with CRP measured pre-operatively. Previous studies have shown that elevated pre-operative CRP is a risk factor for increased length of stay after elective orthopedic surgery 44 and infection after total hip arthroplasty 45 but another study found that pre-operative CRP levels were not statistically significant risk factors in predicting post-operative complications after total knee arthroplasty. 46 Extensive research on CRP detecting post-operative infection after orthopedic surgery exists19-22,47 but little literature exists investigating pre-operative CRP in lumbar spine surgeries.
Our results suggest that perhaps acute or chronic inflammatory states are not the driver of post-operative complications but malnutrition is instead, as both albumin and CRP are markers for inflammatory states but only albumin is used to measure malnutrition. However, regardless of the mechanism by which decreased albumin or elevated CRP confer increased risk for post-operative complications, the odds ratio of pre-operative hypoalbuminemia and elevated CRP is greater than previously documented risk factors. In a single center retrospective study, multivariate logistic regression analysis revealed operation time and American Society of Anesthesiologists (ASA) classification: 3 to be significant risk factors for surgical site infection while operation time, ASA classification: 3, and elevated post-operative CRP after 1 week to be significant risk factors for UTI. 37 However, with exception to ASA classification: 3 which had an odds ratio of 6.0176 and 3.7076 for surgical site infection and UTI, respectively, the odds ratio for operation time 1.0066 and 1.0577 for superficial site infection and UTI, respectively; the odds ratio for elevated CRP after 1 week of surgery was only 1.1336 for UTI.
In the United States, routine pre-operative laboratory is often performed before surgical procedures, as information gathered from such results helps stratify risk and determine intra-operative and post-operative management. Additionally, routine pre-operative laboratory work up has been demonstrated to be a significant cost saving measure in septoplasty, though no literature currently exists within the orthopedic spine surgery space. 48 However, one study by Rodriguez et al 49 have noted that routine pre-operative tests are redundant, as lab results of patients who were indicated to undergo pre-operative laboratory tests per guideline recommendations 50 did not yield unexpected results and consequently did not change anesthetic management. In another study by Onuoha et al, 51 70% of routine pre-operative metabolic panels, a commonly used blood test in the United States that measures serum electrolytes, kidney function, and glucose levels, were collected in patients who were sufficiently healthy according the American Society of Anesthesiology physical status. Nonetheless, while the appropriateness of pre-operative lab work is widely debated, malnutrition is a frequently missed and untreated diagnosis with as many as 2 of every 3 major surgery patients being malnourished. 52 Therefore, orthopedic spine surgeons should consider the possibility of malnourishment in their patients and order appropriate testing to stratify patients’ risk.
While other studies have investigated pre-operative albumin and CRP as risk factors for post-operative complications, most studies are either single institutional studies or utilize the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. Our study provides a unique perspective by being the only study investigating pre-operative albumin and CRP as risk factors for post-operative complications after ALIF, PLIF, and lumbar discectomy using the Pearl Diver database. Using this database provides advantages with the primary one being that Pearl Diver helped facilitate a highly powered study that served to mitigate confounding factors that would otherwise impact other smaller powered studies. Additionally, because Pearl Diver is a national database, we were also able to mitigate regional bias that would otherwise impact single-institutional studies.
Our study was not without limitations. One limitation of using PearlDiver to conduct a retrospective study such as this one is its dependence on ICD-9 and CPT codes, as the accuracy of collected patient information is subject to provider recording, thus serving as a potential source of error. Additionally, due to PearlDiver as well as this study being retrospective in nature, collected patient data is limited to certain demographics and additional information including but not limited to patient outcomes, characteristics, or hospital course could not be obtained; furthermore, controlling for pre-existing conditions is difficult, as doing so would significantly impact the power of our study and therefore impact the primary objective of our study. Information pertaining to intra-operative variables such as operation time, estimated blood loss, and blood transfusion was also absent from this study, which could have otherwise provided additional detail regarding the etiology of various post-operative complications such as infection or surgical revision. Another limitation to Pearl Diver is its inability to report the number of patients for groups in which there were 11 or fewer patients, limiting our ability to report post-operative complication rates or odds ratios. Given the study design and small populations our exclusion criteria did not exclude patients who had a front/back procedure. Power was also a limitation in this study, patients with abnormal CRP and in particular albumin values were low and might have had an impact on the comparison analysis. Lastly, our study did not compare the complication rates between patients who had pre-operative laboratory values compared to those who did not, serving as a potential source of selection bias.
Recent literature has come out investigating how a pre-operative CRP: albumin ratio affects morbidity and mortality. In the study done by Llop-Talaveron et al., a pre-operative CRP: albumin ratio was statistically significant for predicting infection, sepsis, and liver failure. 53 Furthermore, prealbumin has been cited as a serum biomarker of impaired perioperative nutritional status and a risk factor for surgical site infection, UTI, and longer surgery time after spine surgery.15,53-57 In addition to investigating other serum markers for malnutrition, including platelets, INR, absolute lymphocyte count, and hematocrit, special attention should focus on the sensitivity and specificity of these markers in predicting intra-operative and/or post-operative complications including, but not limited to, operative time, bleeding, infection, revision of surgery, MI, DVT, PT, and length of hospitalization.
Conclusion
Using the Humana Insurance database through PearlDiver, we demonstrated that pre-operative hypoalbuminemia is a statistically significant risk factor for deep infection, UTI, and surgery revision while CRP showed a trend but was not a statistically significant risk factor for these complications. For some patient populations, low serum albumin greatly increases risk for post-operative complications, namely deep infections. Given these findings, serum albumin may be a useful test to add pre-operatively to improve patient safety and reduce adverse outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Disclosures outside of submitted work:
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.