
Abstract
Study Design
Cross-Sectional Study
Objectives
Socioeconomic status (SES) is a fundamental root of health disparities, however, its effect on surgical outcomes is often difficult to capture in clinical research, especially in spine surgery. Here, we present a large single-center study assessing whether SES is associated with cause-specific surgical outcomes.
Methods
Patients undergoing spine surgery between 2015 and 2019 were assigned income in accordance with the national distribution and divided into quartiles based on the ZIP code-level median household income. We performed univariate, chi-square, and Analysis of Variance (ANOVA) analysis assessing the independent association of SES, quantified by household income, to operative outcomes, and multiple metrics of opioid consumption.
Results
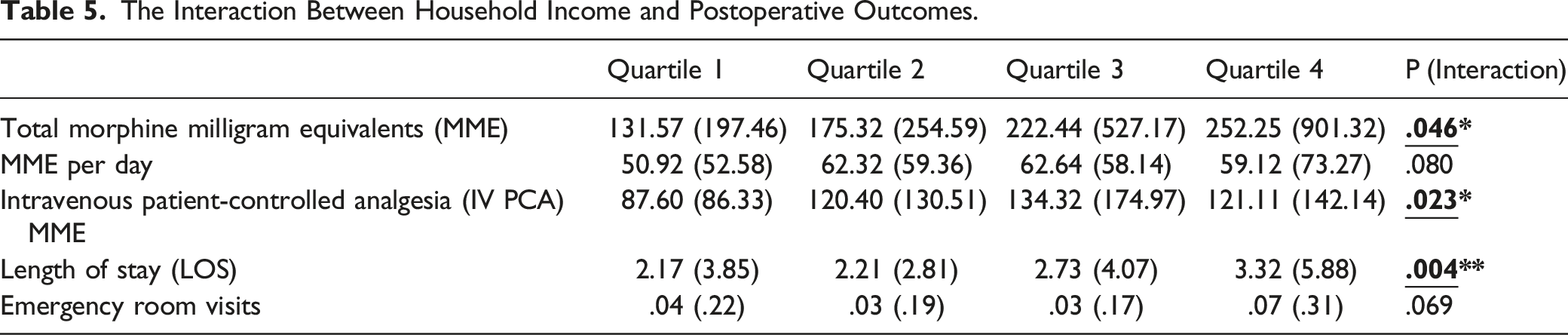
1199 patients were enrolled, and 1138 patients were included in the analysis. Low household income was associated with the greatest rates of 3-month opioid script renewal (OR:1.65, 95% CI:1.14-2.40). In addition, low-income was associated with higher rates of perioperative opioid consumption compared to higher income including increased mean total morphine milligram equivalent (MME) 252.25 (SD 901.32) vs 131.57 (SD 197.46) (P < .046), and inpatient IV patient-controlled analgesia (PCA) MME 121.11 (SD 142.14) vs 87.60 (SD 86.33) (P < .023). In addition, household income was independently associated with length of stay (LOS), and emergency room (ER) revisits with low-income patients demonstrating significantly longer postop LOS and increasing postoperative ER visits.
Conclusions
Considering the comparable surgical management provided by the single institution, the associated differences in postoperative outcomes as defined by increased morbidities and opioid consumption can potentially be attributed to health disparities caused by SES.
Introduction
In surgery, the quality of care provided, whether by operative intervention or non-operative treatment, is closely intertwined with social factors related to the socioeconomic status (SES) of a patient. 1 In addition, perioperative outcomes including opioid consumption and length of stay can have significant influence on patient-reported outcomes such as functional status, activities of daily living, quality of life, and overall patient experience. Several reports have previously reported the increased likelihood of physicians prescribing opioids to patients of low SES as a significant problem facing this vulnerable population.2,3 The opioid crisis is one of the greatest health crises in the history of the United States. In 2018 alone, there were 15 000 deaths due to overdoses involving prescription opioids, totaling 32% of all opioid overdose deaths. 4 This crisis has disproportionately affected communities of low SES. 5 Studies have also found differential risk for chronic opioid use based on SES risk factors such as gender, geographical region, race, and household income in the United States.6-9 However, an underlying issue in many of these studies is the lack of a consistent definition for SES.
Socioeconomic status (SES) is a critical issue affecting all disciplines of medicine.10-13 Patients from low SES are at an increased risk for postoperative morbidity and mortality, which directly contributes to healthcare disparities across various medical specialties. 14 The impact of SES on surgical outcomes in the presence of healthcare access in the United States remains unclear. SES is known to be related to other factors, such as insurance status, education, race, ethnicity, sex, and household income. These variables contribute to shape the social determinants of health that underlie disease development, access to healthcare, provider attitude, and patient-reported outcomes. The relationship between SES and clinical outcome of medical treatments has been the subject of various studies over the past decade, and SES-related risks of poor outcome in surgery including 30-day complications, readmission, length of stay, and mortality have been demonstrated previously.15-20 Although this relationship is multifactorial and complex, most studies comparing these two factors have attributed their negative association to differences in accessibility and provision of care, rather than patient or health provider factors.
There has been a steady increase in research focusing on the impact of socioeconomic factors on a wide range of different patient-reported outcomes in orthopedic and joint surgery.1,21,22 These recent studies have tried to evaluate the impact of SES on postoperative functional outcomes, such as range of motion, walking ability, complications, and mortality; however, there are limited studies characterizing the impact of SES on hospital length of stay, rate of readmission, emergency room revisits and preoperative opioid consumption. These limited studies that do exist primarily draw their samples from nationwide databases, which often define SES through insurance status or other indirect proxies and limit the capacity to control for patient-specific confounding variables. Insurance status is often used as a proxy for SES, since patient-related factors such as educational level, occupation, and annual income are often difficult to directly obtain from medical records.
The primary objective of this study is to determine the association between SES, reflected by gross annual household income, and primary surgical and patient-reported outcomes after elective spine surgery in an academic medical center. Additionally, we aim to establish whether SES is associated with perioperative opioid consumption, length of stay, and emergency room visits. The results from this study will better inform spine surgeons of SES as a potential significant factor to be considered during preoperative decision-making, as well as increased awareness of established SES-related risk factors in the hopes of alleviating these risk factors and improve surgical outcomes for low SES patients.
Methods
Patient Selection
After obtaining Institutional Review Board approval (IRB #STU-2019-0519), patient data was collected retrospectively by reviewing the electronic medical records of all adult patients who underwent elective spine surgery at our academic medical center and completed follow up with our providers between August 2015 and May 2019. Patients included in our analysis underwent initial consultation between 2015 and 2017 with patient follow-ups ranging from 2016 to 2019. All patients included in our study were 18 or older and underwent cervical, thoracic, or lumbar spinal surgery including discectomy, laminectomy, fusion, foraminotomy, disc replacement, deformity correction, hardware replacement, corpectomy, or combinations thereof. We excluded patients with missing information including patients lost to follow and those who were from out of state due to lack of data on their zip codes and household income.
Socioeconomic Status
In this study, gross annual household income was used as an indicator of SES. Household income is one of the most widely accepted and used methods to quantify SES and has previously been validated to provide an accurate reflection of SES-related health disparities.16,23-25 Income was determined via the median annual household income by ZIP code as provided by the United States Census and divided into 4 categories according to the following percentiles: 100th to 76th (first quartile), 75th to 51st (second quartile), 50th to 26th (third quartile), and 25th to 0 (fourth quartile), as previously done in a study by Hernandez-Meza et al. 16 Patients were assigned income percentiles and quartiles in accordance with the national income distribution. Quartile cutoffs were determined by assessing the interquartile ranges of the reported household incomes of the patients. Berkowitz et al. found that using ZIP code-level median household income or the percent living in poverty was the easiest and most consistent way to monitor SES differences in health outcomes. 23
Baseline Characteristics
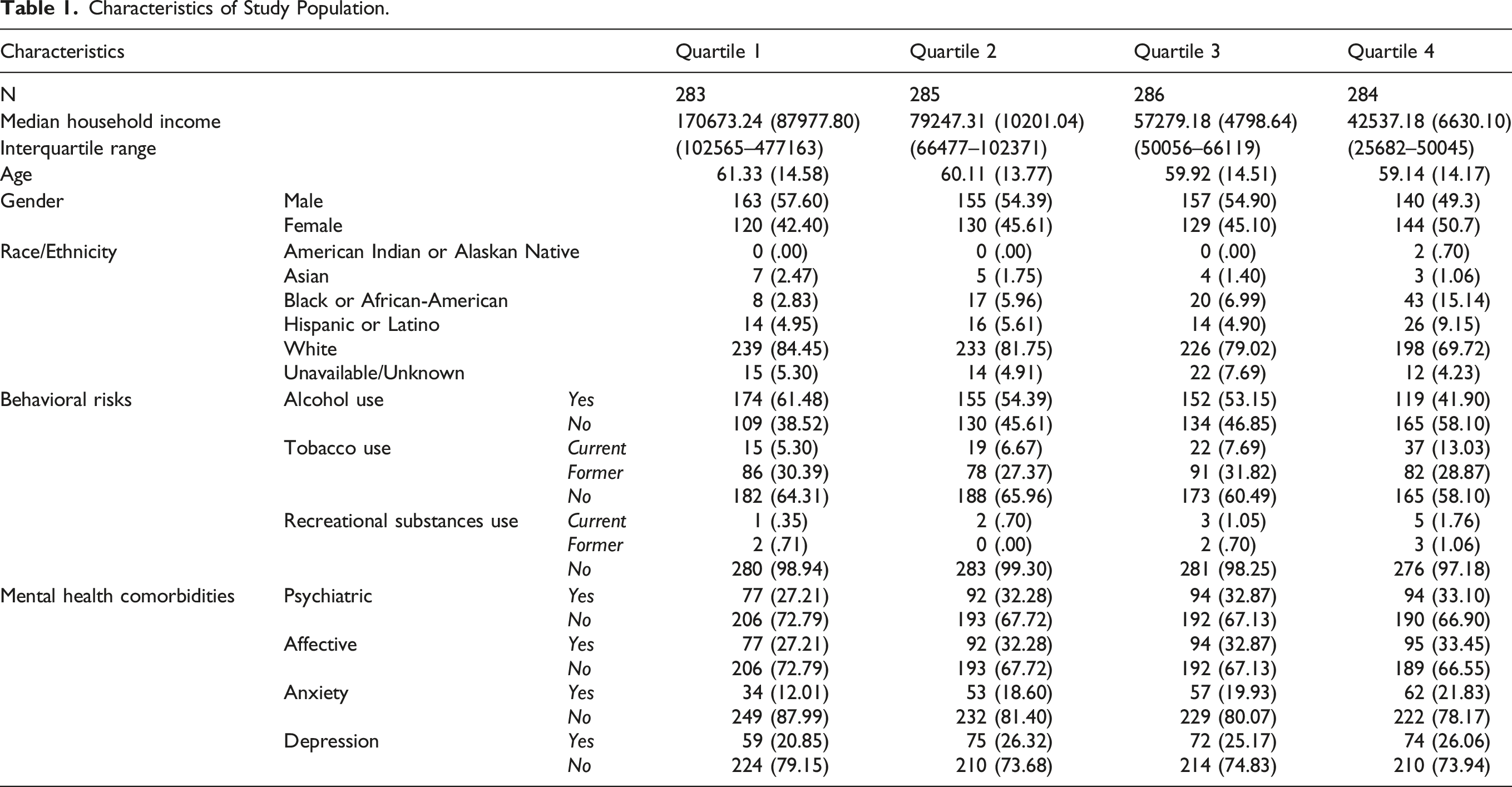
Preoperative factors including patient demographics (age, gender, race, and median household income), social history (alcohol use, smoking status, and recreational drug use), psychiatric history (depression, anxiety, obsessive compulsive disorder, and post-traumatic stress disorder), and preoperative opioid and benzodiazepine use were collected. Median household income was divided into 4 groups: Quartile 1 corresponded to the highest income patients (Median: 170673.24, Range: 102565–477163), Quartile 2 (Median: 79247.31, Range: 66477–102371), Quartile 3 (Median:57279.18, Range: 50060–66119) while quartile 4 was the lowest income patients (Median: 42537.18, Range: 25682–50045). Race was categorized into American Indian or Alaska Native, Asian, Black/African-American, Hispanic or Latino, White/Caucasian, and Unavailable/Unknown. Current smoking status, alcohol use, and recreational drug use were each classified into current, former, and no use.
Regarding surgical categories, patients were divided into 7 surgical management categories according to level of spine segment and number of segments affected during surgery as has been previously described: 26 Anterior Cervical, Anterior Cervical/Posterior Cervical, Lumbar Long, Lumbar Short, Lumbar Short/Anterior Cervical, Posterior cervical and Pure Thoracic. A surgery involving 3 segments or less was considered short segment, while 4 segments or more was considered long segment. In addition, the number of patients who had a fusion was recorded per income group. We compared the 7 surgical management categories between the 4 income distributions and examined the association between household income and surgical characteristics.
Endpoints
The primary objective of interest was association between household income and perioperative opioid consumption. Preoperative baseline opioid use for each patient was divided into 3 categories: Controlled Substance Act (CSA) Schedule II (hydrocodone, oxycodone, morphine, hydromorphone, fentanyl), CSA Schedule III or IV (Tylenol-codeine, tramadol), and none. The division of preoperative baseline opioid users into separate groups was done to better characterize patients by the potency and addictive potential of the medication they were on at the before the time of surgery. Total inpatient opioid use was collected from Epidural and intravenous (IV) pain-controlled analgesia (PCA) routes, and then converted into morphine milligram equivalents (MME) to standardize the opioid consumption. Opioid intake preoperatively, intra-operatively, or while the patient was in the post-anesthesia care unit was not included. The total MME was then divided by length of stay (LOS) to calculate an average opioid consumption per hospital day. 26
Secondary endpoints for this study focused on the association between household income and LOS, emergency room (ER) visits, hospital readmission and opioid script renewal. Opioid script renewal included renewal within 3 months and 12 months after surgery to assess narcotic prescriptions in the subacute and chronic postoperative period. Number of ER visits were counted only if the visit was within 6 weeks of procedure. In addition, the relationship between household income and patient baseline characteristics was assessed.
Statistical Analysis
SPSS software (v26 SPSS Inc, Chicago, IL) was used to divide the total sample size into 4 quartiles. 16 Baseline characteristics are presented as counts and percentages (dichotomous variables), means and standard deviations (continuous variables), or medians and interquartile ranges (IQR). Patients were grouped in quartiles in correspondence with the national gross household income distribution. 16 Differences at baseline between income quartiles were tested using Pearson’s chi-square analysis and Analysis of Variance (ANOVA), where appropriate. ANOVA was used to test for interactions between quartiles for each continuous outcome variable. In the case of significant overall interactions (P < .05), a post-hoc least significant difference analysis was performed to analyze differences between individual quartiles. Odds ratios and confidence intervals were calculated for each categorical outcome variable to determine the variables in the derivation sample predictive of household income according to Sheskin, 2004. In income quartile analysis, the highest income quartile (Quartile 1) was designated reference category. Possible predictor variables included: gender, race/ethnicity, behavioral risks, and perioperative characteristics. The postoperative outcomes were also assessed with an ANOVA test for linear, quadratic, and cubic trend. All tests were two-sided, and significance was considered when P-value <.05. Statistical analysis was performed using the IBM SPSS Statistics 20 (IBM Inc, Chicago, IL).
Results
Baseline Characteristics
Characteristics of Study Population.
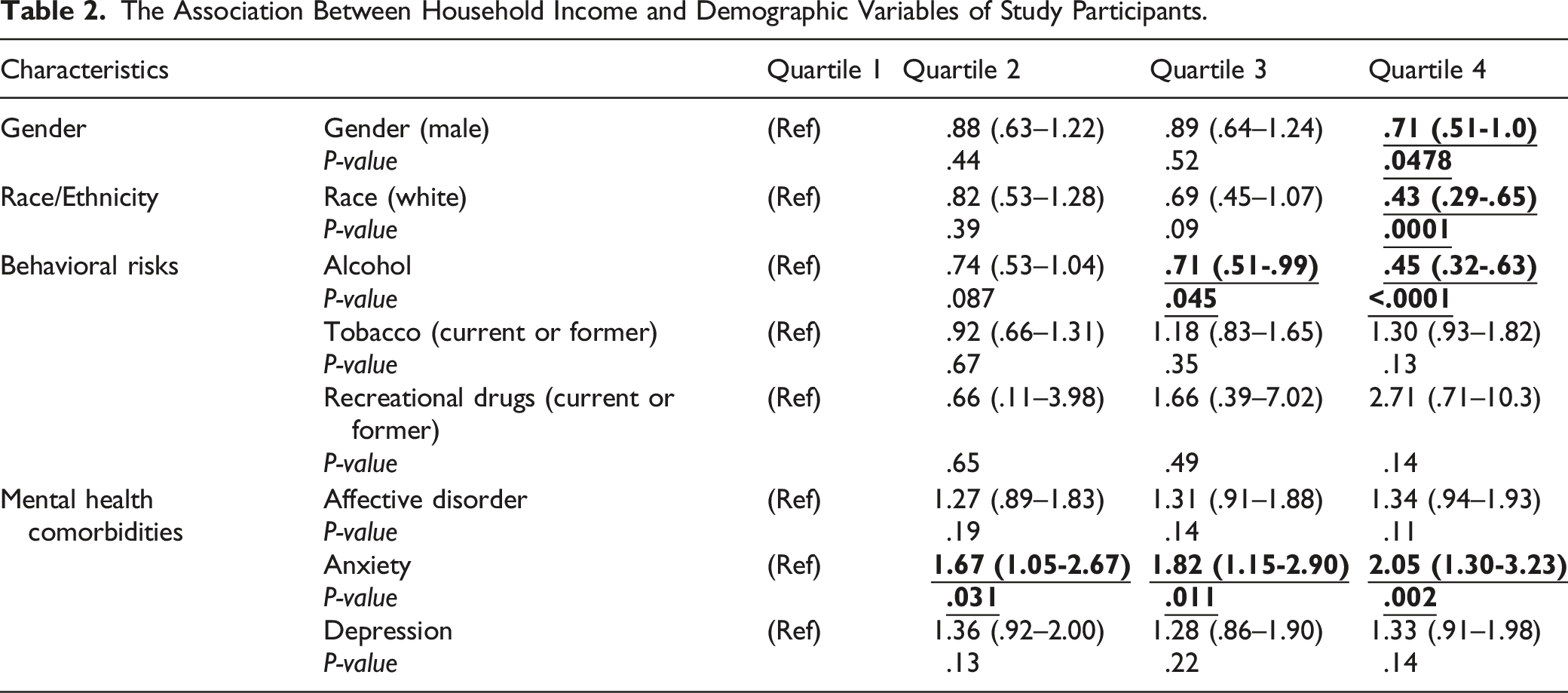
The Association Between Household Income and Demographic Variables of Study Participants.
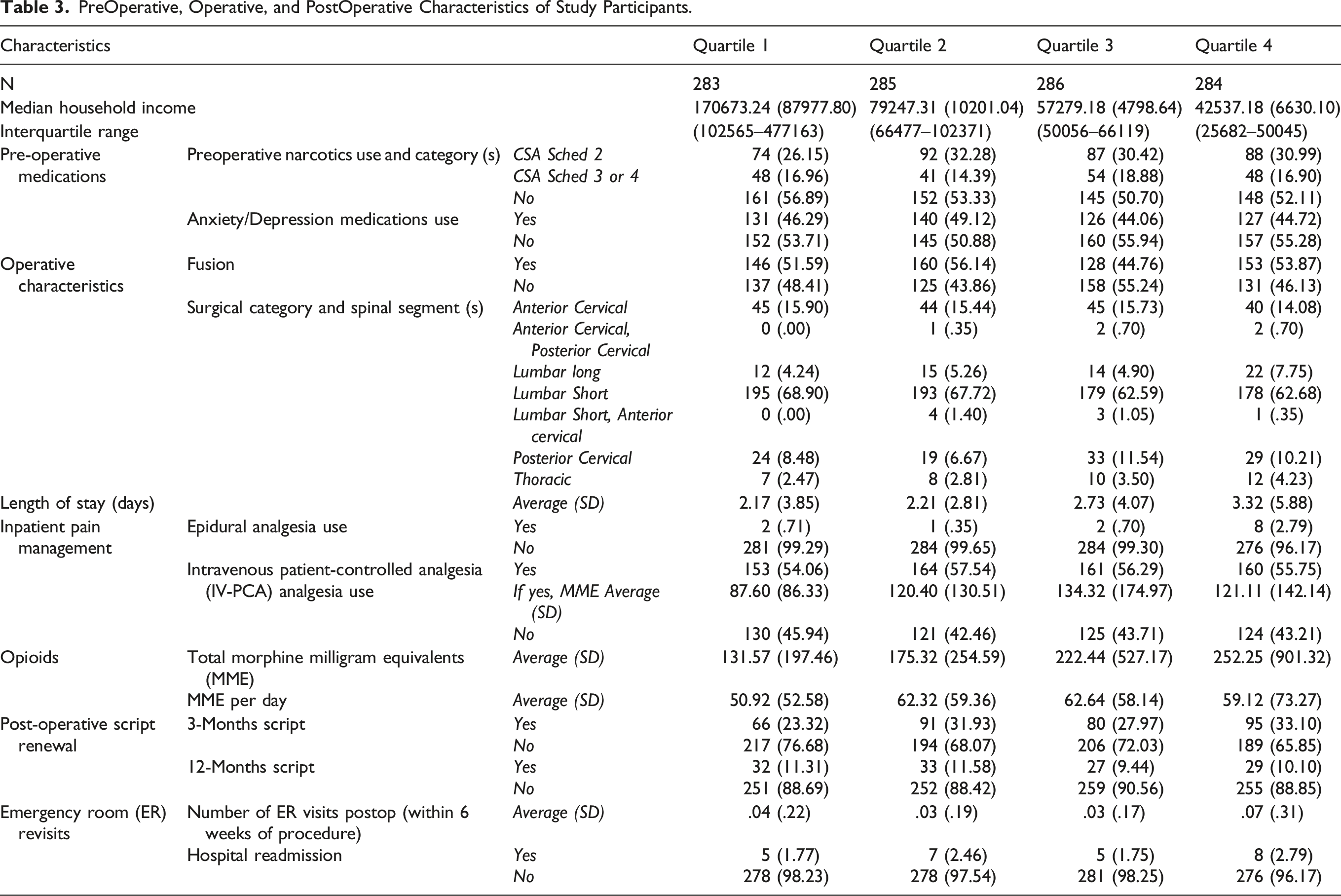
PreOperative, Operative, and PostOperative Characteristics of Study Participants.
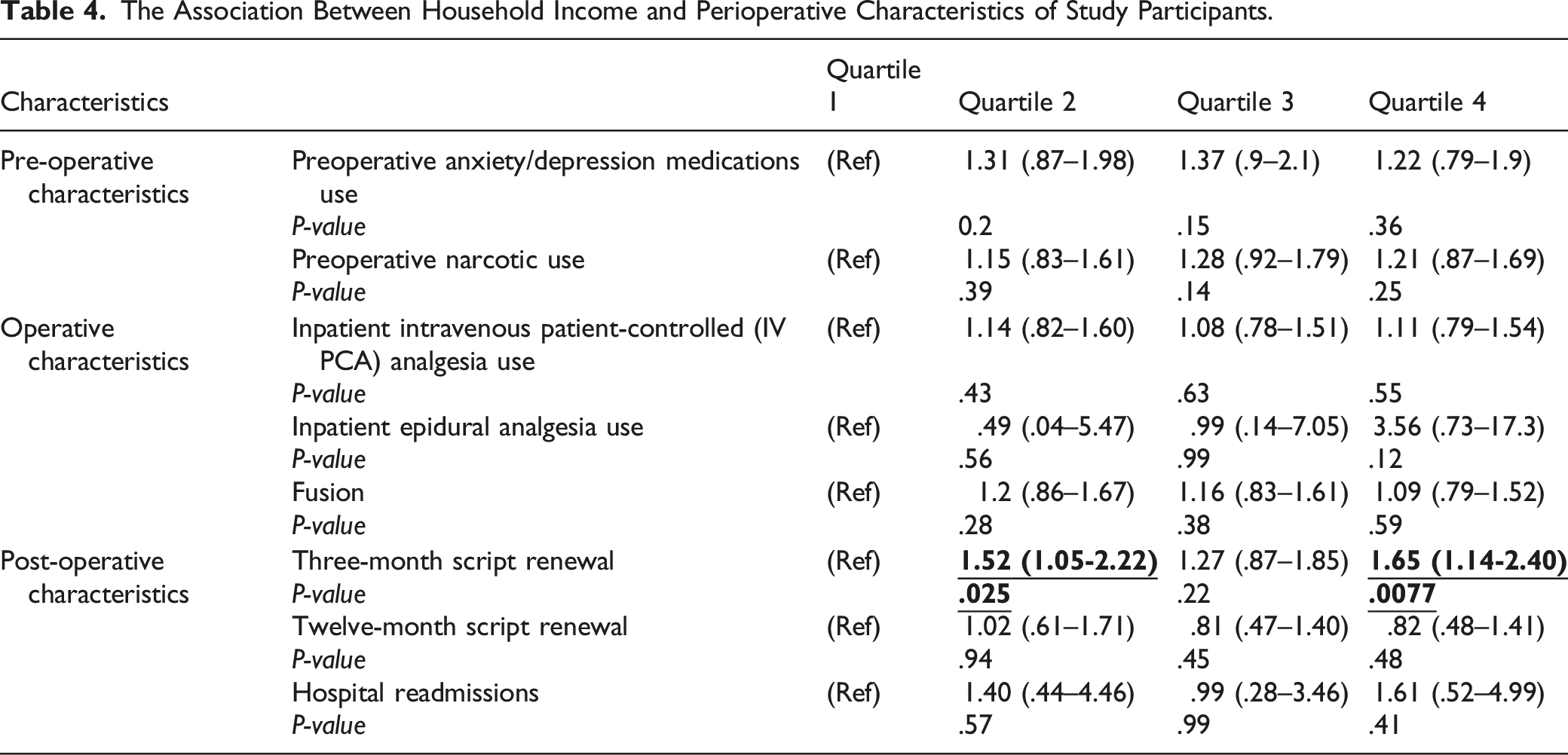
The Association Between Household Income and Perioperative Characteristics of Study Participants.
PostOperative Characteristics
Readmission and ER visits
The Interaction Between Household Income and Postoperative Outcomes.
Length of Stay
There was a significant association between length of stay (LOS) and income bracket (P = .004) (Figure 1; Table 5). Post-hoc LSD analysis showed that income was inversely associated with LOS as the lowest income patients (Quartile 4) had an average LOS of 3.32 (SD: 5.88) days compared to 2.17 (SD: 3.85) days average LOS for the highest income patients (Quartile 1) (P = .004). For postoperative outcomes, there was statistically significant linear trend between quartiles present in length of stay (P = .001). The association between household income and postoperative outcomes.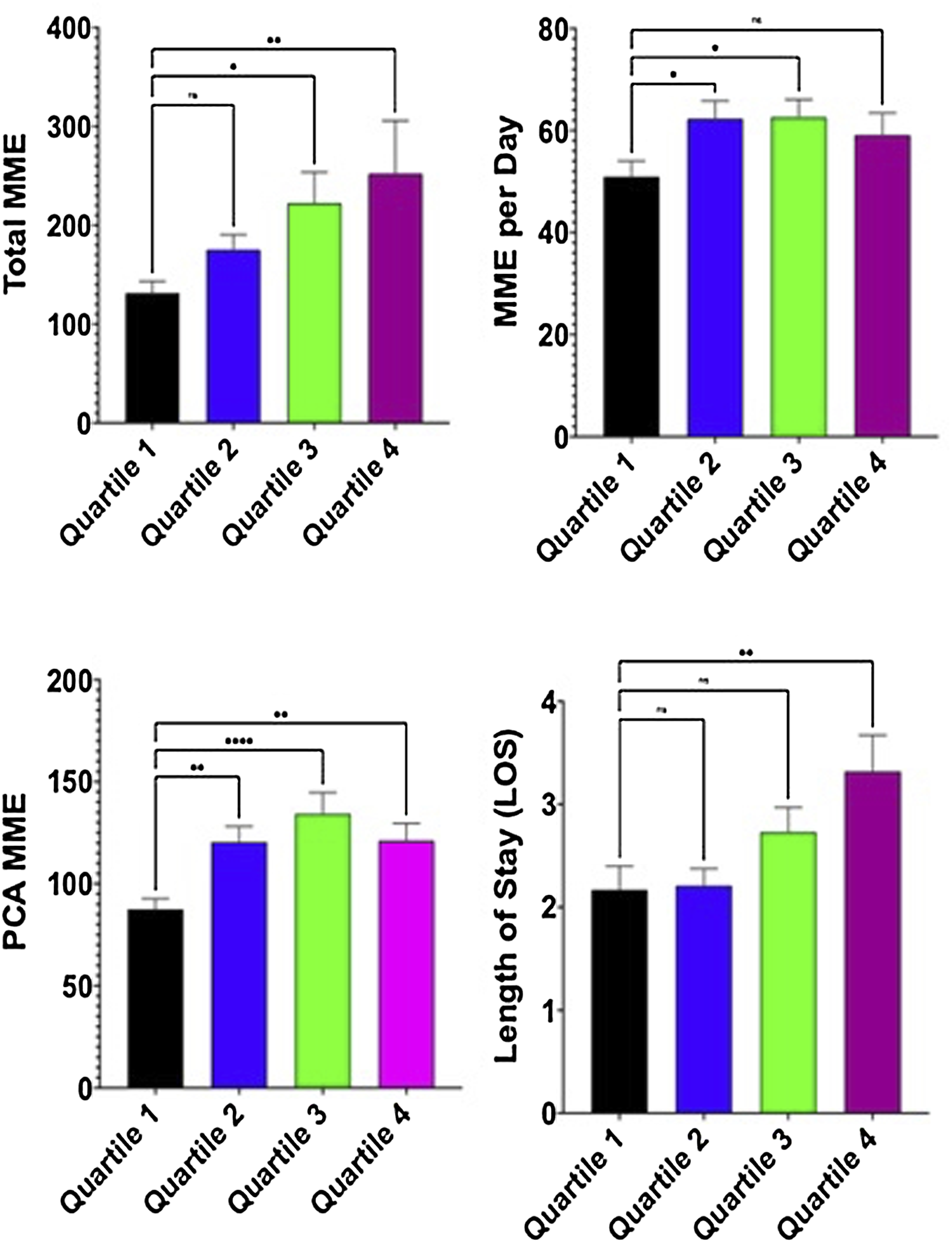
Perioperative Opioid Consumption
In assessing preoperative patient characteristics between groups, the baseline preoperative medications were similar amongst the 4 income brackets (Table 3), and there was no significant association between preoperative narcotic consumption and household income groups (Table 4). Out of our 1199 patients, majority of our patients used IV PCA for inpatient pain management than epidural (638 vs 13), while 548 did not use either (Table 3). The rate of IV-PCA and epidural use was similar between the 4 income groups (Table 4). There was no significant linear trend present in MME used through PCA (P = .33).
Opioid consumption, as measured by total MME, was associated with income (P = .046) (Table 5). The lowest income patients had higher total inpatient MME (252.25 ± 901.32) and higher MME per day 59.12 (SD: 73.27) than the highest income patients who had a total 131.57 (SD: 197.46) MME and 50.92 (SD: 52.58) MME per day (Table 3). Similarly, there was a significant interaction between PCA MME and income (P = .023) (Table 5). Quartile 1 also received less MME via PCA than all other quartiles 87.60 (SD: 86.33), with Quartile 3 receiving the most 134.32 (SD: 174.97) (Table 3). There was statistically significant linear trend between total MME used during the hospitalization (P = .016) and significant quadratic trend in MME consumed per day (P = .043).
In income analysis, patients in the second quartile and fourth quartile had significantly higher number of 3-month opioid script renewal (OR: 1.52, 95% CI: 1.05–2.22; OR: 1.65, 95% CI: 1.14–2.40, respectively) (Table 4). The association lost significance in the third quartile, although a trend remained (OR: 1.27, 95% CI: .87–1.85). There was no significant difference for opioid script renewal at the 12-month mark between comparison groups.
Discussion
The primary finding of this study is that SES, reflected by household income, is a significant predictor of surgical outcomes in an overall spine surgery population. Since the negative association between SES and surgical outcomes maintained even as patients’ preoperative narcotics consumption and surgical intervention was comparable amongst the groups, SES should be considered as part of conventional risk estimator in assessing patients preoperatively for worse outcomes. Secondly, this study showed that SES is related to specific short-term postoperative outcomes, as demonstrated by its association with 90-day major complications including opioid consumption, length of stay and hospital emergency room revisits.
Several discrete factors may drive the association of low SES with worse outcomes. First, a patient’s socioeconomic disadvantage is a recognized risk for poor compliance to medications, diet recommendations, and lifestyle restrictions.24,25 Second, apart from patient-specific factors, providers, and their interaction with patients, may also influence the relationship between SES and poor outcomes. Particularly, stereotyping of patients from different cultural or ethnic backgrounds along with communication deficiencies between patient and providers play a critical role in how low SES affects patient care.27-29 In our study, the demographics between income quartiles including the patient’s surgical intervention and preoperative narcotic use were overall homogenous, except for race. Despite the study occurring in a region with a preponderance of Black and Hispanic population, 28 non-Hispanic Caucasian patients made up most of the highest income households while Black and Hispanic patients were disproportionately represented in the lowest income households. Due to the relatively limited number of patients in our cohort, we were unable to stratify the patient population by race and income bracket to separate the effect of economics from race and ethnic categories. Moreover, SES disparities exist even among fully insured patients.12,13
Patient-level determinants that were not analyzed in this study include access to socioeconomic resources including education, food, employment, housing, and social services. All these factors can influence adherence to the plan of care or access to outpatient services, which may be associated with increased opioid consumption, length of stay, ER revisits and hospital readmission. Frequently it is observed that low-income populations due to lack of finances or insurance have delayed initial consultations and late diagnosis leading to increasing pathology upon presentation requiring longer spine surgeries and difficult surgical management exposing more complications.17,30 While our study did not examine delay in diagnosis, future studies could examine time from onset of symptoms to spine surgery presentation and characterize the association between the delayed time in diagnosis and household income.
Differences in outcome after surgery between socioeconomic classes have previously been attributed to disparities in quality and provision of care.13,31-34 However, the equality in access to and provision of care provided by this single-center study setting suggests that patient-related factors that are not adequately captured by the methods we conventionally use to define risk factors, play a dominant causal role in SES-related outcome differences including increased postoperative length of stay and opioid consumption. The analysis of patients within the income brackets treated at a single institution should account for bias linked to the provision of care.
Although opioids are effective as a postoperative analgesic for acute pain, spine surgeons must be acutely attuned to those that are at risk for chronic use. Several studies have revealed that a multitude of factors—the type of surgery, comorbidities of the patient, socioeconomic status (SES), among others—have been associated with adverse prolonged opioid use. However, there is limited data supporting these conclusions in the spine surgery population. Our study helps fill this gap by investigating the relationship of household income with outcomes including perioperative opioid use.
Socioeconomic status is an important consideration when prescribing opioids to spine surgery patients. However, an in-depth understanding of its role in influencing opioid use has yet to be achieved due to varying methodology for determining SES status or due to uncontrolled confounders. 9 Schoenfield et al studied 9991 opioid-naïve spine surgery patients in the Military Health System Data Repository database and found that lower SES was associated with decreased likelihood of discontinuing opioid use postoperatively. 7 In a later study, the group found a similar trend among orthopedic trauma patients in the same database. 6 However, their determinant of SES was the patient’s military rank, which inherently incorporates confounding variables. This finding was further corroborated by Sheth et al. who analyzed 982 joint replacement patients at a single institution, finding that the patients with a worse Area Deprivation Index, determined by home zip code, exhibited increased opioid use. 30 The relationship persisted even after controlling for other common risk factors such preoperative opioid use and other comorbidities. In our study, it was noted that lower income was associated with increase in predisposition to anxiety which may also be a confounding variable for increased PCA use. Together, these results indicate that patients of lower SES are more likely to experience adverse outcomes and exhibit chronic opioid use postoperatively, consistent with our finding that such patients have a longer length of stay, greater inpatient opioid consumption, and higher likelihood of increased opiate script renewal at 3-months postop.
Our study adds to the current body of spine literature by using a zip code-based household income that provides a greater level of specificity to determination of SES; thus, allowing the study of its effect on outcomes. Increased physician awareness of social determinants of health and improvement of communication between patient and provider may help to improve outcomes of low SES surgical patients. 35 Although the association between low SES and worse outcomes is multifactorial and complex, a better understanding of SES-related risk factors may help to attenuate health disparities. The findings corroborate previous data from non-spine populations that worse neighborhood SES associates with worse surgical outcomes including an increased risk of long-term opioid use and length of stay.
Limitations
This study has some limitations that should be considered. First, it should be noted that only patients who underwent surgery were included in the study. Patients who were conservatively treated and those with prohibitive surgical risks due to severe comorbidities were consequently excluded. Opioid intake preoperatively, intra-operatively, or while the patient was in the post-anesthesia care unit was not included as these medications are linked to the immediate peri-anesthesia period and are often linked to induction. Although the surgeries between income brackets were similar and done within a single institution and a limited number of providers, it would have been valuable to assess the association between socioeconomic status and the various parameters of access to and quality of healthcare within our medical center. Another limitation stems from multiple statistical testing which, given the unadjusted nature of the univariate statistical analysis, may modestly increase type 1 error rates. However, given the low P values in several significant quartile 4 outcomes in the setting of significant linear and quadratic trend support the conclusions drawn from these data. In future studies, it will be important to increase the number of the patients and complete a stepwise regression to address confounding variables. Baseline demographic variables may act as confounders for each income group, but demographic considerations also go hand-in-hand with health disparities one might expect for lower income groups.
Additionally, exploring the surgical decision-making of spine surgeons in our institution could lead to an effort to understand the impact of provider attitudes on the different aspects of access and quality of care, and potential interactions between specific providers and patients. Finally, previous studies in the United States that have reported on SES-related outcomes and healthcare disparities often describe discrepancies between racial groups as well. Due to limited number of patients within the groups, racial disparities could unfortunately not be investigated as independent factors. Future prospective multi-institutional studies correlating patient characteristics and provider attitudes to surgical outcomes are warranted.
Being a retrospective cohort study at a large single institution, recall and sampling bias have likely affected our results. Similarly, the composition of the population studied is unique to the institution’s catchment region and limits the external validity of the findings. Zip code-based determination of SES status is not without fault, as it may not capture individualized nuance irrespective of where one lives. Gross household income is the most common income measure used in the classification of SES, with most researchers defining a range of low, medium, and high-income categories according to the federal poverty line. Studies often capture income by ZIP code or county as a proxy for individual income; however, it is important to consider the validity of using a pooled community measure, since it may not necessarily reflect individual-level characteristics. 17 Further, we divided patients into quartiles within our cohort, which may not be representative of the current national income quartiles. Lastly, there is potential for differences in how physician’s practice opioid prescriptions based on geography, institution, or preference.
Conclusions
In conclusion, this analysis demonstrates that low median household income, as an indicator of low SES, is a risk factor for overall opioid consumption and length of stay following surgery. These results are consistent with previous studies and provide a more in-depth analysis of our collective understanding of postoperative patient opioid consumption and length of stay in the spine patient population. Considering the equality in access to and provision of healthcare provided by this study setting, our results suggest that the observed health hazards accompanying low socioeconomic status are likely to be caused by patient and provider factors, rather than differences in medical care. Surgeons must be cognizant of biases and specific factors influencing outcomes on low SES patients and of the patient’s capacity, whether it’s individual income, insurance status, or their access to necessary non-pharmacologic treatment resources, to execute the postoperative recovery plan. Although the exact mechanism mediating the postoperative SES-related opioid consumption risk remains unclear, increased physician awareness and improvement of known SES-related risk factors and behaviors may help to improve surgical outcome among low SES patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Compliance Statement and Ethical Adherence
This Study Was Written in Compliance With Our Institutional Ethical Review Board (IRB #STU-2019-0519)