
Abstract
Study Design:
Modified Delphi study.
Objective:
Adult spinal deformity (ASD) is an increasingly recognized condition, comprising a spectrum of pathologies considerably impacting patients’ health and functional status. Patients present with a combination of pain, disability, comorbidities and radiological deformity. The study aims to propose a systematic approach of gathering information on the factors that drive decision-making by developing a patient profile.
Methods:
The present study comprises of 3 parts. Part 1: Development of prototype of patient profile: The data from the Core Outcome Study on SCOlisis (COSSCO) by Scoliosis Research Society (SRS) was categorized into a conceptual framework. Part 2: Modified Delphi study: Items reaching >70% agreement were included in a 4 round iterative process with 51 panellists across the globe. Part 3: Pilot testing—feasibility: Content validity and usability were evaluated quantitatively.
Results:
The profile consisted of 4 domains.
Conclusions:
The present study, is first to provide a universally applicable multimodal ASD patient profile to methodically describe patients. Physicians are encouraged to assess ASD patients holistically using this profile and not just based on radiographic findings.
Introduction
Adult spinal deformity (ASD) is an increasingly recognized condition, comprising a spectrum of pathologies considerably impacting patients’ health and functional status. The reported prevalence of ASD varies between 1.4%-32% in the general adult population.1-4 The prevalence rate was reported to be as high as 68% in population older than 60 years of age. 5 In spite of the magnitude of the problem, there is still inconsistency in categorizing these patients. One of the greatest challenges in developing an adequate, valid and reliable comprehensive classification is the inherent heterogeneity of the ASD population, characterized by a wide range of clinical symptoms associated with different combinations of comorbidities. 6
Initial attempts toward classifying ASD patients were made by Ponsetti & Freeman, 7 Aebi 8 and later by Simmons. 9 A recently conducted systematic review 10 identified 54 different classification systems for ASD and the most commonly used classification system was that of Scoliosis Research Society (SRS)-Schwab classification. 11 This classification, which is solely based on radiological parameters, considers the coronal curve type, sagittal modifiers such as global sagittal alignment and pelvic parameters, where the modifiers relate to patient-reported outcome measures (PROMs). 12 Glassman et al reported that positive sagittal balance is a significant predictor of clinical status.13,14 However, Jackson et al demonstrated a poor correlation of curve magnitude and sagittal plane measures with pain and moderate correlation between apical vertebral rotation and pain.15,16 Deviren et al, demonstrated a poor correlation between radiographic measures and health in adult spinal deformity. 17
Unlike adolescent spinal deformities, wherein radiological parameters such as curve magnitude and progression of the curve are the main drivers of patient management; classifying and managing ASD patients depend on multiple non-radiological (bio-psychosocial) factors such as disability, comorbidities, frailty, social support, expectation of treatment outcome and underlying etiology.6,9,18-25 Each patient with ASD presents with different combinations of pain, disability and risk factors along with diverse radiological deformities making it difficult to develop a linear classification. Recent reviews on the factors affecting the outcome of ASD patients have reported that in addition to the radiological appearance, various clinical factors such as back pain, leg pain, neurological status and comorbidities drive the decision-making in ASD management.6,20 To capture all the relevant outcome domains, the Core Outcome Study on Scoliosis (COSSCO) project, supported by SRS, has identified the minimal set of outcome domains, accompanying measurement instruments and contributing risk factors for adult spinal deformity. 26 The COSSCO data provides measurement instruments to systematically measure the outcomes.
The present study aims to take these efforts a step forward by methodically describing those drivers and risk factors in a conceptual framework employing a common language for each patient, thereby identifying a unique patient profile. This patient profile to be developed, needs to be applicable in daily practice for surgical and non-surgical patients and needs to balance pragmatic use with sufficient granularity.
Methods
The study was designed in line with the 3-phased mixed methods pathway proposed by Audigé et al 27 which involves 1) Development, including pilot agreement study—i.e. the current study, 2) Reliability and accuracy in clinical setting, and 3) Prospective validation and association with patient outcomes. The present study addresses the Phase 1 and consists of 3 parts: Part 1. To develop a prototype patient profile, Part 2. To obtain formal consensus via a Modified Delphi study, and Part 3. To test feasibility in terms of content validity and usability. (Figure 1).
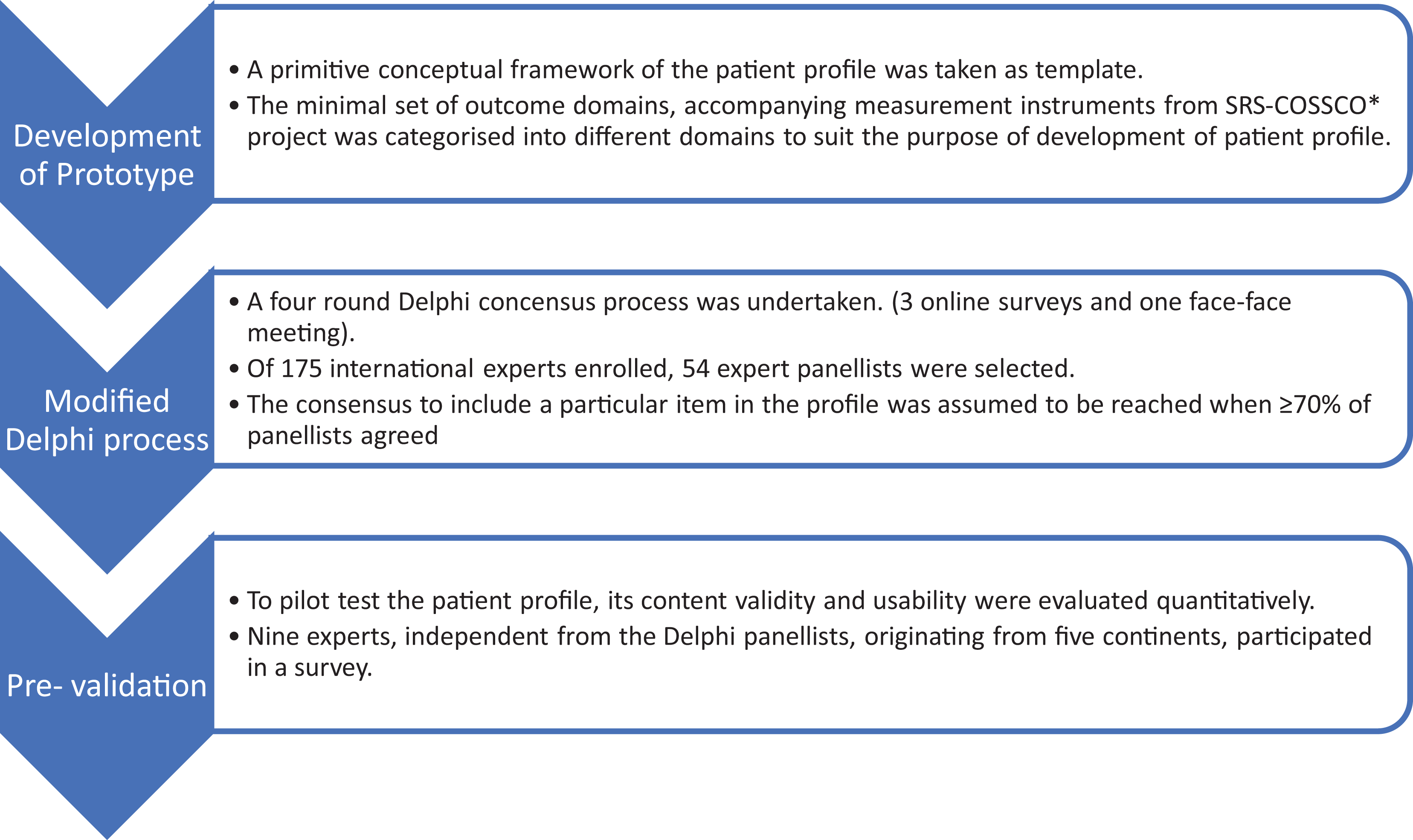
Illustrating the study design consisting of 3 parts.
Part1: Development of Prototype of Patient Profile
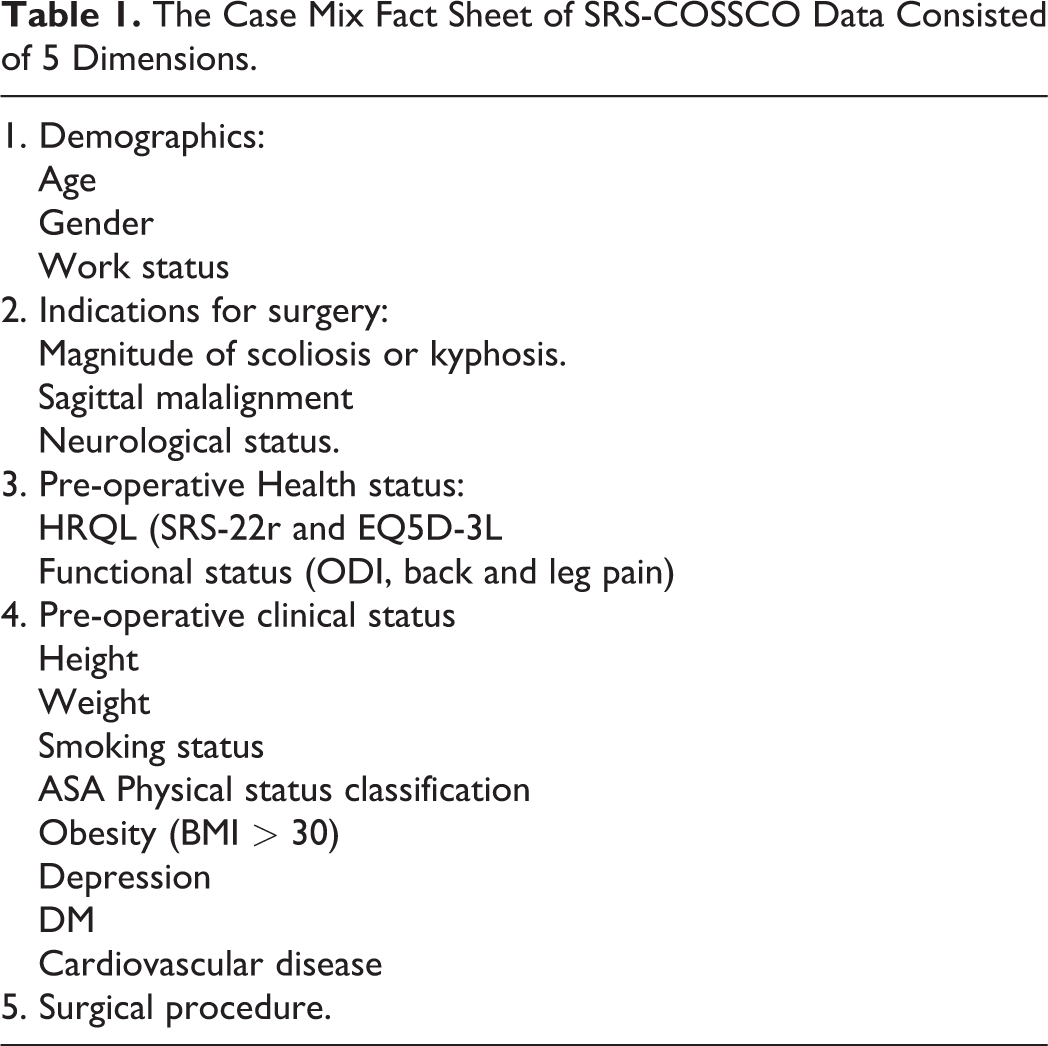
A preliminary conceptual framework of the patient profile consisting of radiological parameters, clinical findings and comorbidities was taken as a template to develop the prototype. The minimal set of outcome domains, accompanying measurement instruments and contributing case-mix and risk factors data as defined in the SRS-COSSCO project (Table 1) was categorized to suit the purpose of the development of the patient profile.
The Case Mix Fact Sheet of SRS-COSSCO Data Consisted of 5 Dimensions.
Part 2: Modified Delphi International Expert Consensus study
The Delphi process was conducted by the project team consisting of the principal investigator along with 2 more spine surgeons and supported by a methodologist and a project manager. The role of project team was to conduct the required literature search, recruit the panellists for Delphi process, preparation of the questionnaire for each survey round, preliminary analysis of data, preparation of feedback reports and monitoring the survey process.
Selection of panellists
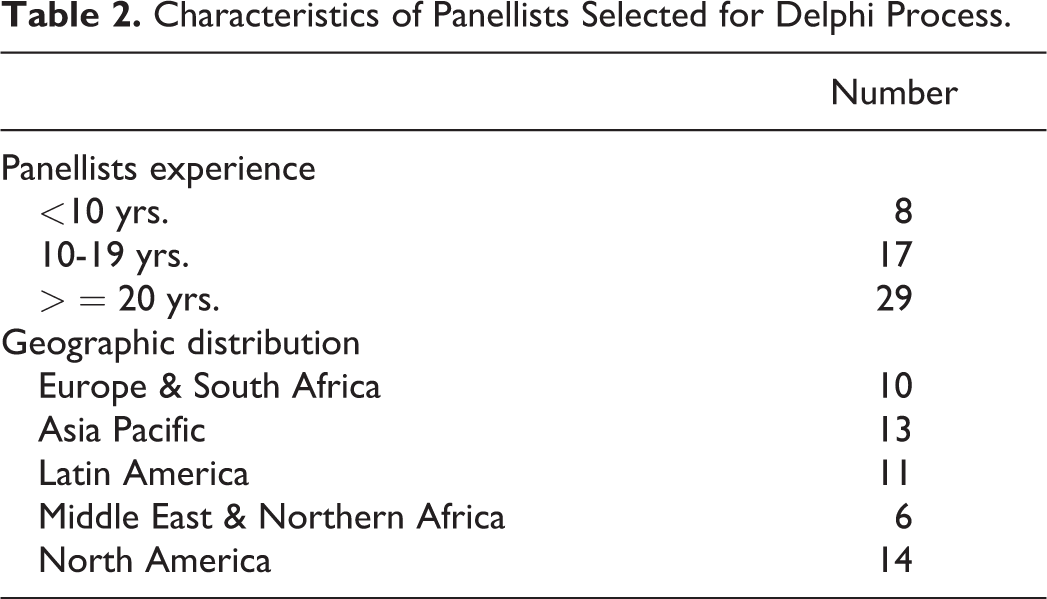
To recruit the expert panellists, an open call detailing the purpose of the study and expected involvement as a panelist was sent to all AO Spine members. 175 international experts responded. The data pertaining to their experience and number of scientific publications related to ASD, as well as their geographical representation was collected. 54 panellists (listed in the appendix), representing 5 continents, were selected based on the best combination of clinical experience, scientific publications and geographical distribution (Table 2).
Characteristics of Panellists Selected for Delphi Process.
Delphi procedure
A modified Delphi technique was used to seek consensus on the items to be included in the profile. 28 The Delphi process aims to obtain “formal group consensus” among panellists by presenting a series of surveys pertaining to the structure and items of the prototype. An anonymous and controlled feedback of group response was presented to the panellists before each subsequent round. The synthesis of responses in one round was used to design the following round. This iterative process was continued until consensus was reached. The Delphi process was modified by incorporating a face-to-face meeting in addition to online surveys. The modified process involved 4 rounds. Rounds 1, 2 and 4 were designed and distributed using an online survey program (SurveyMonkey Inc, SurveyMonkey.com, California, USA). 29 Round 3 was a face-to-face meeting moderated by 2 non-voting chairpersons. In order to further substantiate the third round (a face-to-face meeting with 13/54 panellists), a fourth round including all panellists was added to confirm the derived patient profile.
In each round, the panellists were provided with a series of “Yes or No” questions. They were asked to consider their own opinion as well as the evidence provided from literature and were encouraged to provide free-text feedback. The survey related to the agreement of items in the prototype profile constituted Round 1; the group response was summarized, comments and suggestions were categorized and presented to the panellists as controlled anonymous feedback along with a second set of questions and new items in Round 2. The face-to-face meeting (Round 3) consisted of presenting group response, anonymous feedback report of previous round and guided discussions by chairpersons on profile structure and items. The fourth round of survey completed the iterative process. The end-product of Round 4 was subjected to pilot testing.
Consensus definition
When ≥70% of panellists agreed on a particular item, consensus was considered reached and the item was included in the profile. The items with less than 30% agreement were excluded. For those items with 30-69% agreement, additional information (e.g. literature) was provided and the item was subjected for voting in the subsequent round. If such items still failed to achieve consensus, the panellists were asked if they agree for alternative proposals. If ≥70% agreed for alternate proposals, they were developed and submitted for voting in the subsequent round.
Part 3: Pilot Testing—Feasibility of Patient Profile
The content validity and usability of the profile were evaluated quantitatively in the pilot test utilizing 8 de-identified case examples. Content validity refers to “the degree to which the content of an instrument is an adequate reflection of the construct to be measured”30,31; and deals with the relevance (all items are relevant for the construct of interest within a specific population and context of use), comprehensiveness (no key aspects of the construct should be missing), and comprehensibility (the items should be understood as intended; clarity).30-32
Content validity
Nine experts, independent from the Delphi panellists, from 5 continents participated in the testing. The panellists indicated the relevance, comprehensiveness, and comprehensibility of the patient profile. First, panellists answered questions based on Consensus-based Standards for the selection of health status Measurement Instruments (COSMIN) content validity checklist. 32 Second, panellists rated the items of the patient profile in terms of its “relevancy” and “clarity” on a 4-point ordinal scale (1 [not], 2 [somewhat], 3 [quite], 4 [highly]).
Content validity is operationalized by the content validity index (CVI) for the relevance (I-CVIr) and the clarity of each item (I-CVIc). For the full patient profile, the content validity ratio (CVR) and the average CVI (Ave-CVI) for relevance were calculated. The CVR, I-CVIr; c and Ave-CVI were calculated using formulae as described by Almanasreh et al. 33 The CVR varies between −1 and 1. The higher score indicates agreement of panellists on the necessity of the patient profile. For 9 panellists a CVR <0.78 would mean that the profile needed revision. The I-CVI ranges between 0 to 1. Excellent content validity would be achieved in the case that I-CVI is ≥0.78 (relevant or clear) and Ave-CVI is ≥0.90 (≥0.80 acceptable).
Usability
The panellists completed questions on whether they were satisfied with use of the patient profile. Usability survey with a 7-point Likert scale for agreement was completed that was adapted from Brouwers et al. 34 Ratings were dichotomized with 1 indicating agreement (i.e. strong, somewhat, agree) and 0 indicating no agreement (strong, somewhat, disagree, neutral). Acceptable usability was defined as having at least 60% response in positive ratings.
Results
The Modified Delphi Process
The response rates for online survey were 94.4% (n = 51/54) for Rounds 1 and 2, and 90.7% (n = 49/54) for Round 4. Thirteen panellists participated in the face-to-face survey. The results of Delphi rounds were summarized in the Figure 2.
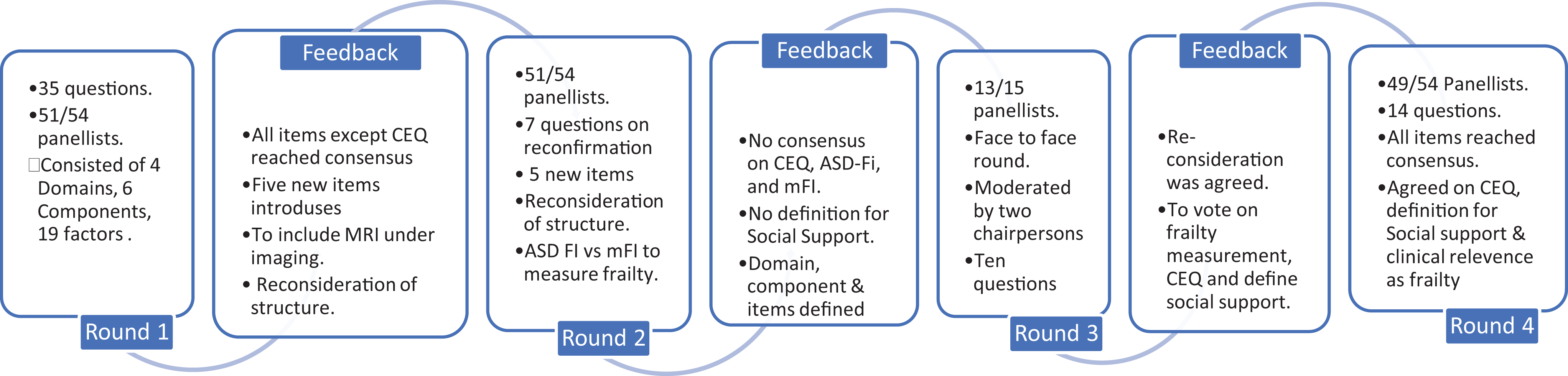
The 4 round modified Delphi process outlining the details of questionnaire and feedback response.
Round 1
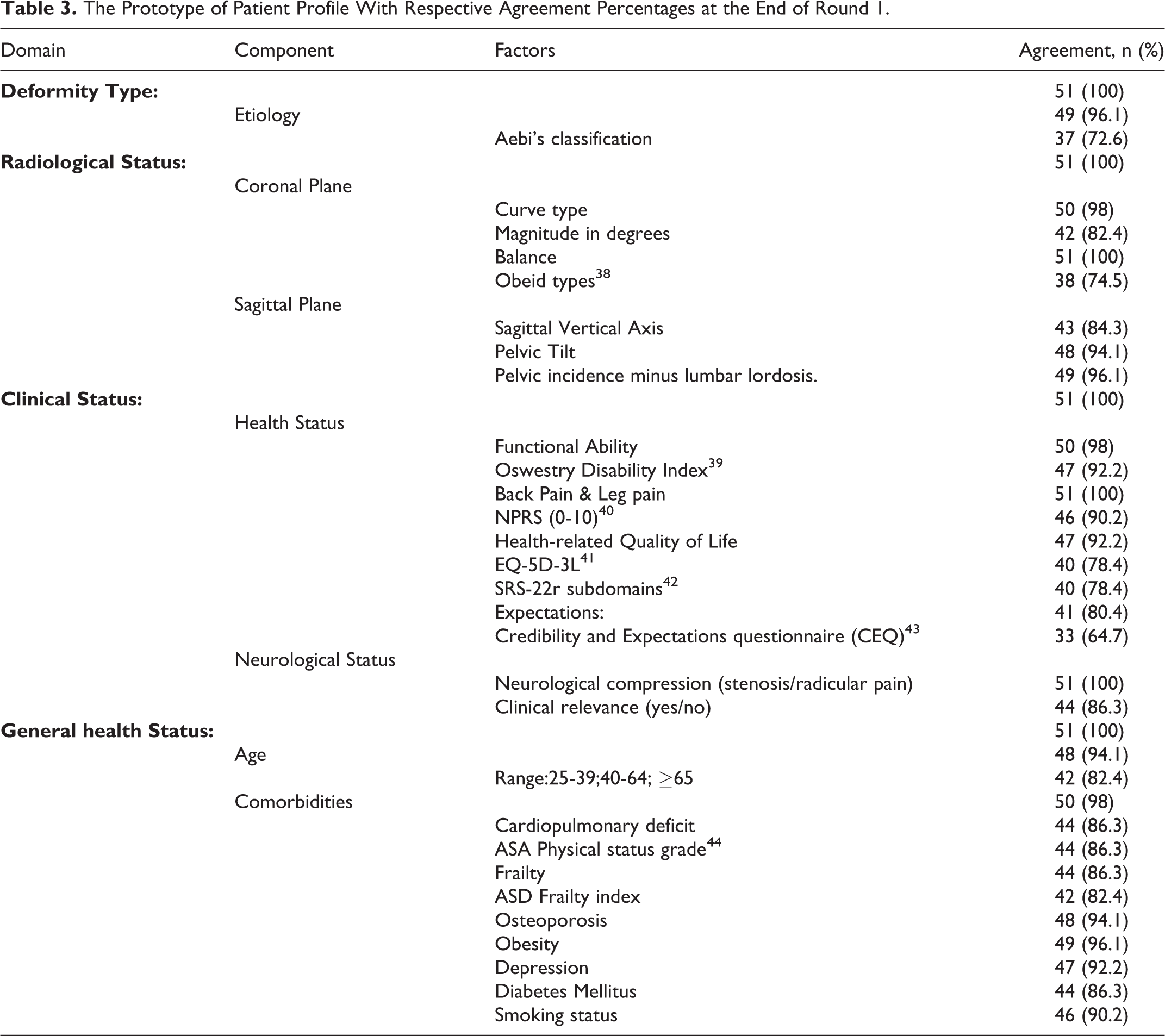
The survey consisted of 35 questions. There was 100% agreement (51/51) on the need for the development of a comprehensive multimodal patient profile system (Table 3). Although all the components and items reached consensus, one measuring instrument for expectations of treatment outcome (i.e. the credibility and expectancy questionnaire (CEQ)35-37) failed to reach consensus (64.7%). In addition, 32 of the 51 panellists suggested to include other components not yet listed.
The Prototype of Patient Profile With Respective Agreement Percentages at the End of Round 1.
Feedback and follow-up action
Literature and supplementary material with explanation was made available on CEQ item for the next round.35-37 After analyzing 32 open-ended responses, 5 new themes and 5 new items (Previous surgery, Social support, Compensated spine (radiological), Neurological function and Frailty measure) were identified (Table 4). Other comments included concerns about ASD-FI as a measure of frailty45-48 and need for imaging with MRI.
The 5 New Items Proposed With Respective Agreement Percentages at the End of Round 2.
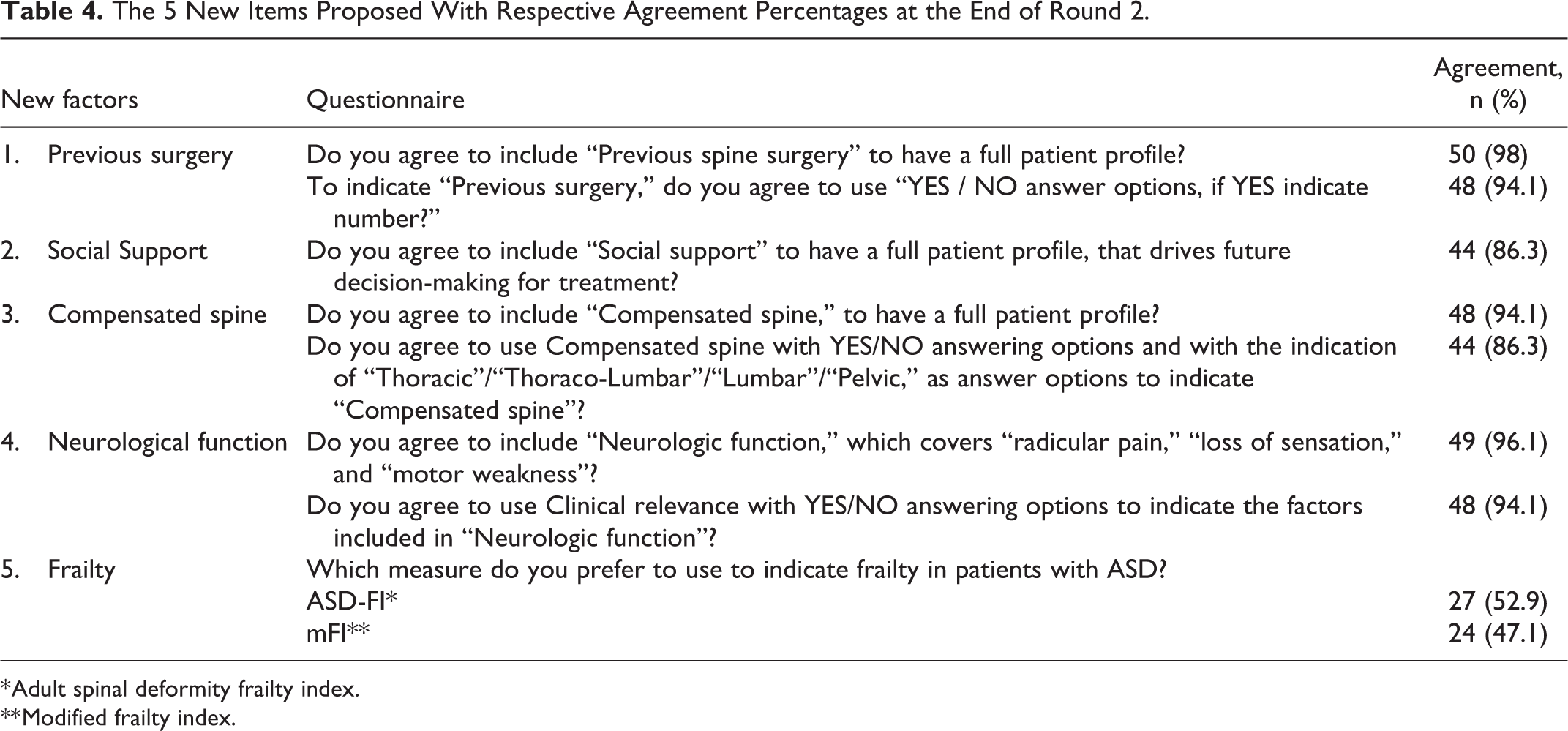
* Adult spinal deformity frailty index.
** Modified frailty index.
Round 2
The survey consisted of 7 questions related to reconfirming Round 1 agreed items, identifying measurement instruments for treatment expectations (1 CEQ item and 4 questions CEQ) and introduction of 5 new items. The 1 CEQ item achieved 58.8% agreement, the 4 questions CEQ achieved 33.3% agreement, and 7.8% panellists voted for none. The consensus was achieved to rename the domain “Radiological Status” into “Imaging” and MRI was introduced as another component in this domain (with 100% agreement). The agreement was tested between modified (11-item) frailty index (mFI) and the ASD Frailty Index (ASD-FI).45-48 Both instruments failed to reach consensus, with ASD-FI reaching 52.9% agreement.
Feedback and follow-up action
Consensus was not yet achieved on the measurement of expectations and forwarded to the next round. The item “Social Support” lacked a clear definition and was carried to the next round.
Round 3(face-to-face meeting)
13 panellists participated in this meeting. Two non-voting moderators (MdK & LL) led the discussions. This round consisted of 10 questions. In view of the challenges to implement currently available frailty instruments in routine practice, extensive discussions were held regarding frailty and how this can be measured in a pragmatic way in daily practice. Consensus was reached to carry out voting in the next round for measure of frailty (91.7%), expectations of treatment outcome (92.3%) and social support (100%) (Table 5).
The List of Questions Moderated by Chairpersons During Face to Face Meeting in Round 3.
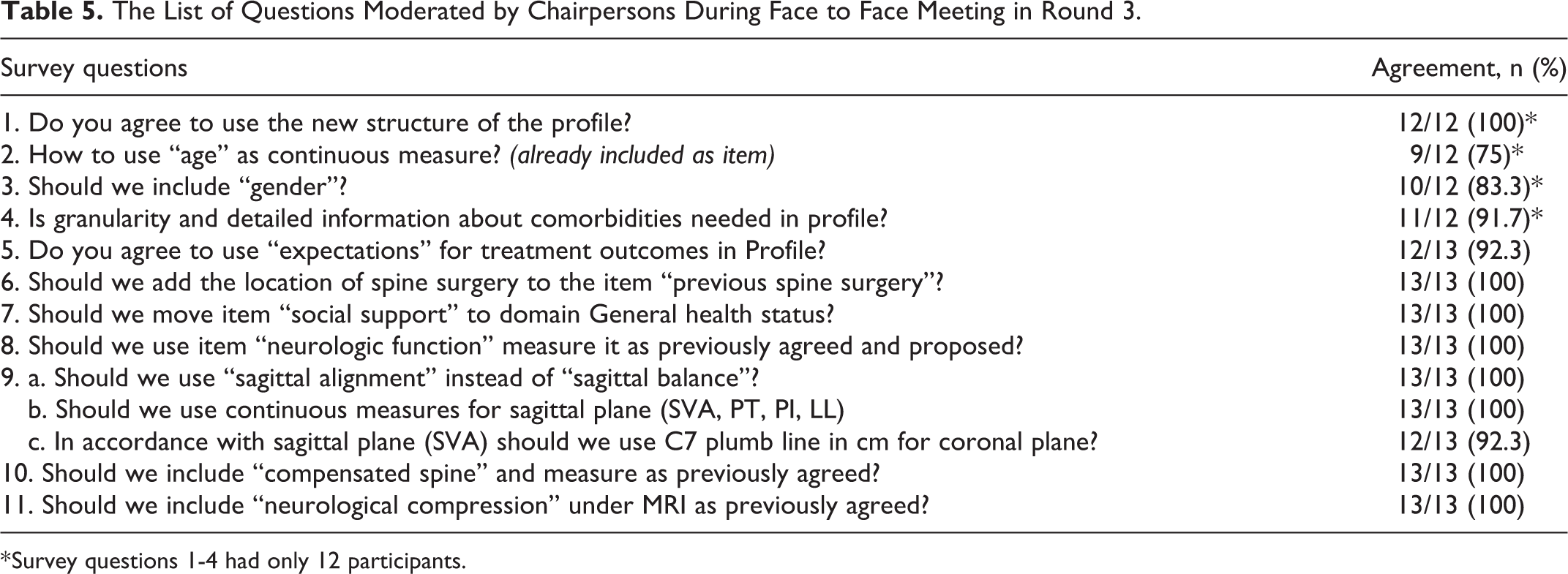
* Survey questions 1-4 had only 12 participants.
Feedback and follow-up action
Three options along with a supplemental literature information for frailty i.e. modified Frailty Scale (mFI), 48 ASD Frailty Index (ASD-FI)45-47 and the Edmonton Scale 49 was provided.
Round 4: (confirmation round)
49 of the 54 panellists participated in the survey. This round consisted of 14 questions. The final consensus was achieved for all the 4 domains i.e. General health status (98%), Spine-Specific Status (100%) Imaging (94%) and Type of Deformity (100%).
Regarding the outstanding items, the 3 proposed measurement instruments for frailty i.e. mFI (39%), ASD FI (22%) and Edmonton scale (39%) failed to reach the consensus. In the follow-up question, 92% consensus was achieved to use “clinically relevant” frailty as a binary (yes/no) measure rather than one of the existing frailty measures. The proposed criteria for social support (1. informal care such as family, friends and neighbors, 2. formal professional care such as home care and 3. no social support) reached 100% consensus. Set 1 item 4 of CEQ reached (94%) consensus as a measurement instrument for expectations of treatment outcome. 98% of the panellists agreed to list neurological impairment in to 3 parts 1.Radicular pain (Yes with dermatome involvement, Yes with no specific dermatome involvement and No), 2.Motor Weakness (Yes & clinically relevant, Yes & clinically not relevant and No) and 3.Loss of Sensation (Yes & clinically relevant, Yes & clinically not relevant and No).
The project team developed the final patient profile, which was subjected for pilot feasibility testing (Figure 3).
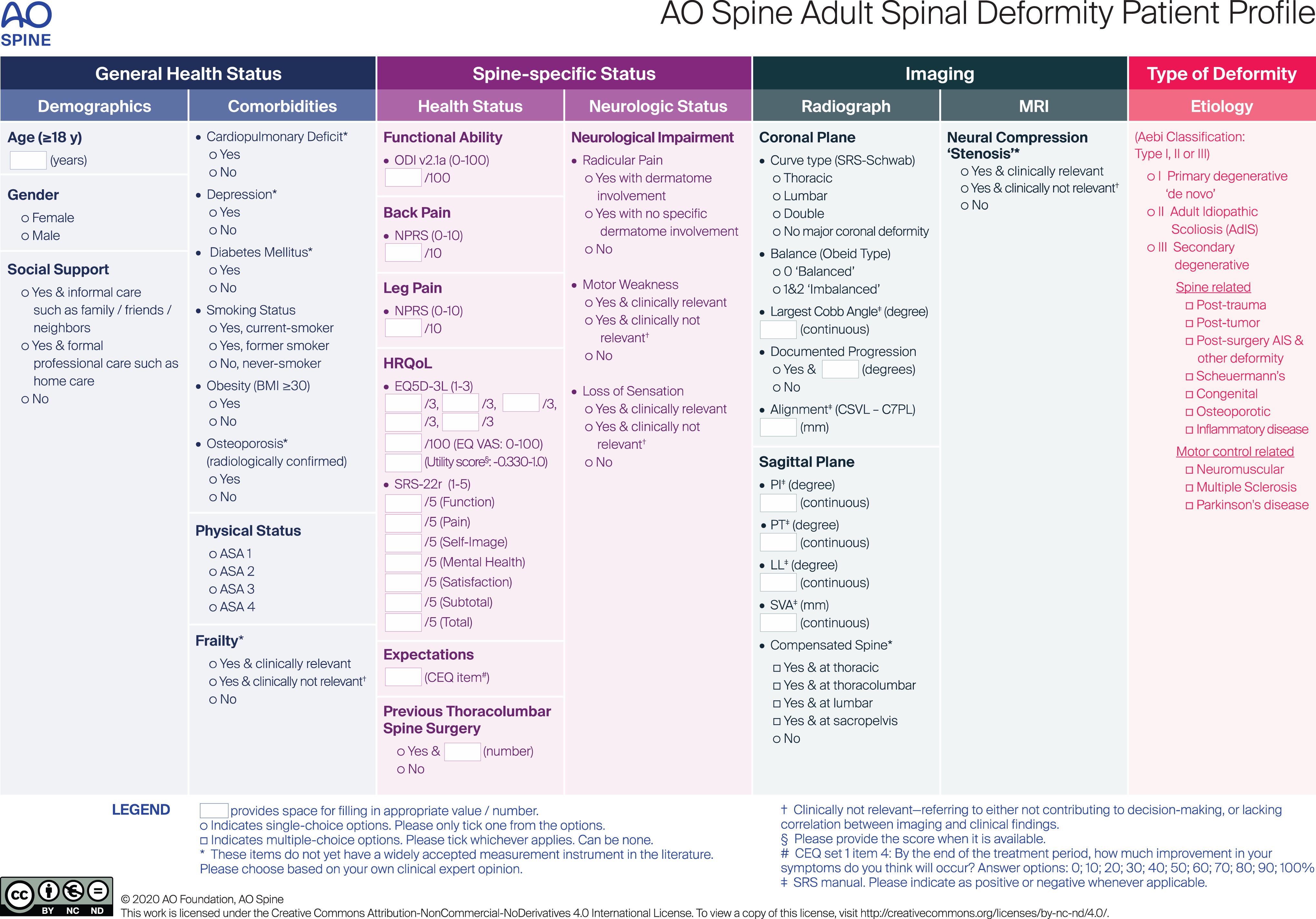
The AO Spine adult spine deformity patient profile.
Pilot Feasibility Test
Content validity
I-CVIr ranged from 0.78 to 1.00 (Table 6) and the average I-CVI (ave-CVI) for relevance is 0.92. The panellists valued comprehensibility lower (I-CVIc 0.33-1.00; Table 6). The I-CVIc of comorbidities, frailty, balance, progression, compensated spine, and neurologic compression “stenosis” was <0.78, indicating that these items lacked clarity and needed revision. Overall the Patient Profile had excellent content validity (I-CVIr 0.78-1.00; Ave-CVI 0.92). This was further substantiated by the COSMIN content validity checklist (67-100%; Table 6).
Content Validity per Item (n = 9 panellists).
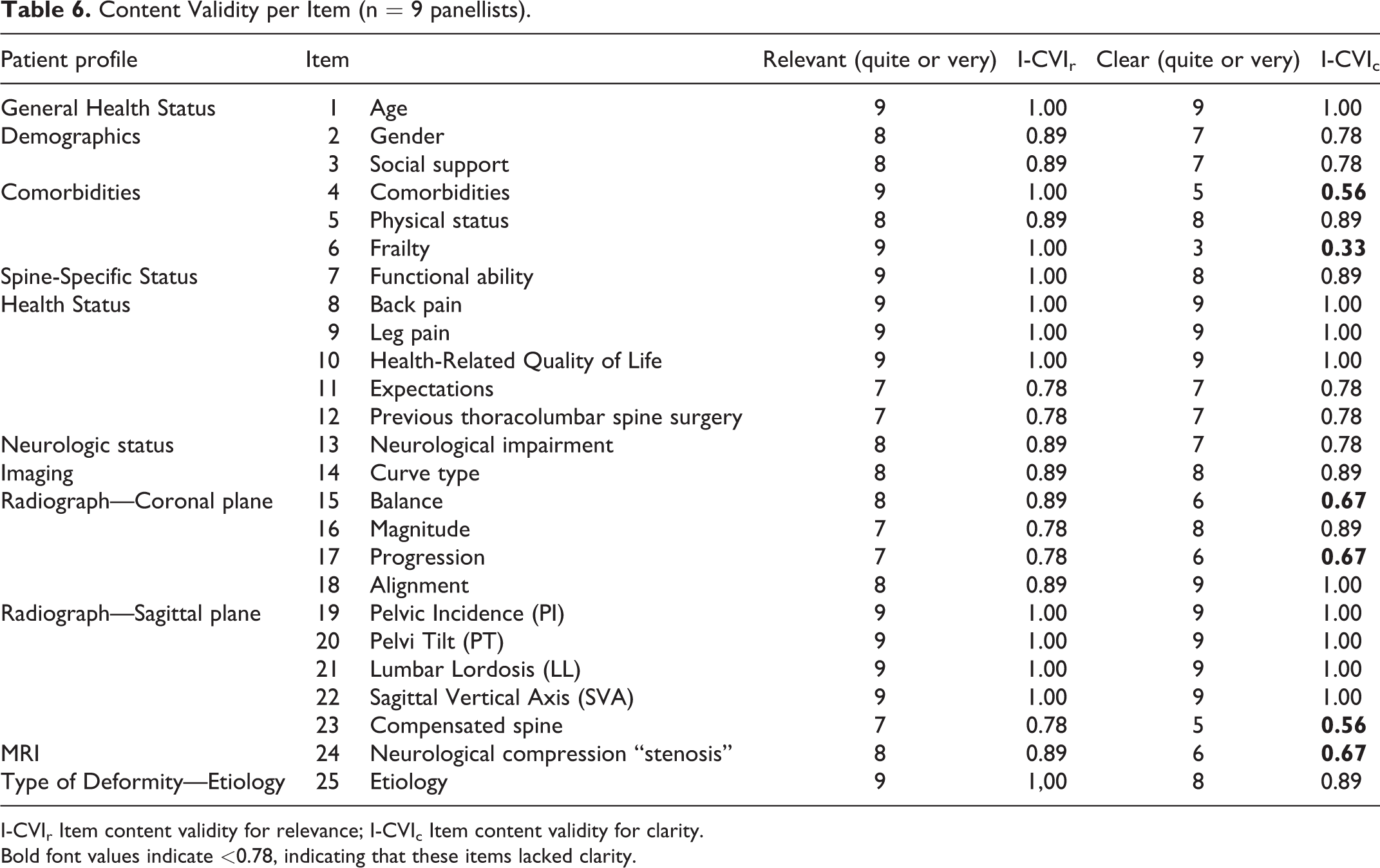
I-CVIr Item content validity for relevance; I-CVIc Item content validity for clarity.
Bold font values indicate <0.78, indicating that these items lacked clarity.
Usability
Overall, the panellists indicated the patient profile as acceptable (range 78% [7/9]-100% [9/9]), rated the overall quality as 71/100, and 78% (7/9) recommend the Profile for use (Tables 7 and 8).
Usability; Content Validity (Relevance and Comprehensiveness; n = 9).
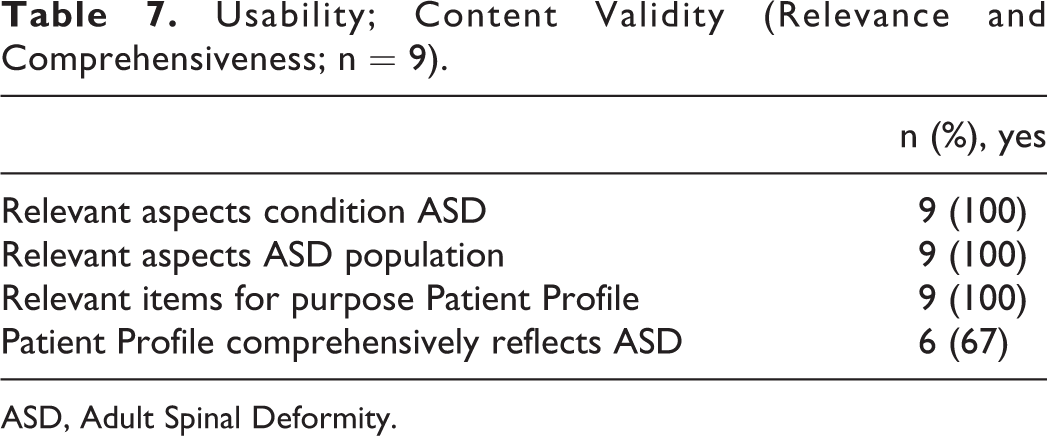
ASD, Adult Spinal Deformity.
Usability Survey.
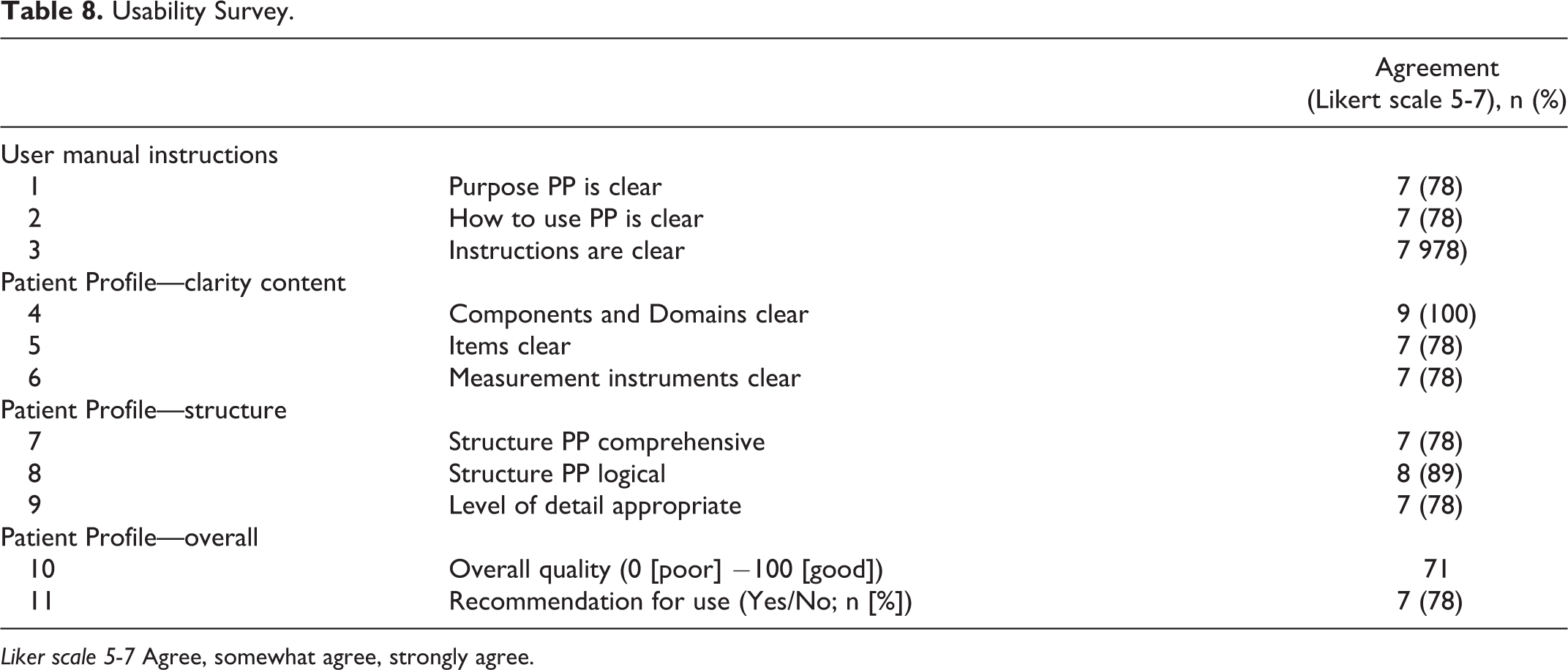
Liker scale 5-7 Agree, somewhat agree, strongly agree.
Discussion
In this study, a comprehensive patient profile was developed with the aim of being universally applicable. Patients with a spinal deformity present with a spectrum of signs and symptoms, such as back pain, neurogenic leg pain, fatigue, stooped posture, and these symptoms change over time.22-25
To guide treatment, classification systems are needed that describe patient characteristics that might ultimately guide management. Currently available classification systems are mainly based on radiological parameters.7-12 However, multivariate analysis of radiological sagittal parameters and various preoperative factors demonstrated that the effect of sagittal parameters on PROMs was not as strong as it was described in previous studies. 50 In addition, age, gender, ASA score and BMI were found to be associated with preoperative PROMs. 50 Recently, categorizing ASD patients purely based on radiological parameters has received considerable critical attention.6,20 Even among the patients with identical radiological features, each patient can potentially present with different levels of pain, disability and comorbidities. 20 The patient profile developed in this study incorporates most, if not all, critical factors in addition to radiographic parameters.
The Structure of Profile
The proposed profile was developed using a rigorous, well-established methodology and encompasses 4 domains: General health status, Spine-specific health, Imaging, and Type of deformity (Etioloy). The profile is intended to be used in daily practice, and this necessitated balancing granularity with the applicability. Some of the items are well-established and can be easily measured such as age and gender. For other items that lack a standardized measuring instrument (i.e. frailty) or for items requiring clinical judgment (i.e. motor weakness or loss of sensation), the pragmatic concept of “clinical relevance” was adopted.
General Health
The general health status domain comprises 2 components: demographics and comorbidities. It is well known that frailty and social support play a very important role in assessing the patient’s ability to cope with their spinal deformity. None of the currently available frailty measurements have been validated in the adult spine deformity population, and all require the use of relatively long questionnaires. Furthermore, institutional abilities to manage the frail patients vary across the globe. The treating physician’s judgment of the clinical relevance of frailty was adopted as a measuring instrument. Similarly, availability of social support is known to have favorable effects on the wellbeing of elderly adults. It is defined as the amount of companionship, care and affection from family members, friends, and other individuals. 36 However, the social support systems are different among countries and cultures which makes it a complex item to quantify. Available tools like Social Support Rating Scale (SSRS) are too elaborate to be adopted in the profile for daily practice.51,52 Instead, a simple description in the form of informal care, or formal professional care or no social support was agreed and adopted.
Spine Specific Status
The spine-specific status domain consists of 2 components: “Spine Health Status” and “Neurological Status.” The important drivers of ASD management i.e. functional ability, back and neurogenic leg pain were quantitatively documented in this domain. An assessment of expectations is required to improve the management of these patients. A study on elderly patients undergoing surgery for lumbar spinal stenosis identified that patients’ expectations were the best predictive factor of satisfaction after treatment. 53 Currently no validated instrument is available to measure expectations regarding treatment outcome in ASD population. The CEQ set one item 4 i.e “by the end of the treatment period, how much improvement in your symptoms do you think will occur?” in a 0-100% scale as adopted with consensus. 43
Imaging
The imaging domain consists of 2 components i.e. “Radiograph” and “MRI”
The radiographic measurements consisted of simple coronal and sagittal parameters to quantify osseous/skeletal spinal deformity and MRI to quantify neurogenic component. The literature on coronal malalignment in ASD is limited. Coronal malalignment can be a potential source of functional impairment. 54 To address this, the Obeid classification 38 was adopted. Similarly, the compensation of spine in sagittal plane in the setting of spinopelvic mismatch was included in the profile. MR imaging plays an important role in the management of adult spinal deformity especially in ASD presents with leg pain or neurological claudication. MRI also aids in planning the decompressive procedures as stand-alone procedure or in combination with spinal fixation and corrections. As MRI is very sensitive in documenting anatomical stenosis, whether it is “clinically relevant” or “clinically not relevant” is documented in the profile.
Type of Deformity (Etiology)
To categorize the ASD patients according to the etiology, the classification proposed by Aebi 9 was adopted into the profile. This categorizes ASD patients into Type I Primary degenerative “de novo” deformity resulting from degenerative changes in intervertebral discs and subsequent development of adult spinal deformity, Type II Adult Idiopathic Scoliosis (AdIS) which is an adolescent origin idiopathic scoliosis in adult life, Type III Secondary degenerative (Spine related or Motor control related). Each of these patient population significantly differ in terms of their clinical presentation, management strategies, surgical needs and deliverables.
The proposed patient profile has the potential to fill the knowledge gap of current ASD patient management by capturing comprehensive patient data, creating uniformity in evaluation and potentially helping to develop decision-making pathways by identifying clusters of patients with similar profiles. In the pre-validation by a group of independent experts (i.e. not one of the Delphi panellists or authors) the currently proposed patient profile has been shown to have an excellent content validity, is appropriate, relevant and is useful as assessed.
The multifaceted, time dependent, bio-psychosocial, nature of ASD patients, offers an opportunity for application of advanced analytics and artificial intelligence in nonsurgical and surgical care. Recently, Ames et al 55 demonstrated the use of unsupervised learning via hierarchical clustering to create a novel classification system for ASD based on large data of patient and surgical characteristics. The data captured in the proposed patient profile provide a good scope for adoption of these technologies.
Limitations of the Study
The AOASD Patient Profile was developed based on the available literature, complimented by expert consensus and feasibility test for usage in clinical practice. The profile is limited to the initial evaluation of the ASD patients to drive decision-making for treatment management. It does not take perioperative and surgical drivers into consideration, such as team experience, hospital facilities and setting etc. Several items proposed in the profile are evolving and no universally agreed measurement tool for ASD exists in the literature (e.g. frailty and CEQ). To address these items, subjective judgments such as “clinical relevance” were introduced as a pragmatic alternative that achieved very high consensus. The developed profile is not a classification system, as it does not attempt to guide treatment. In future, further studies involving testing of reliability, accuracy, validation, and association with patient outcomes in clinical practice, this profile could ultimately mature into a classification system. The profile involves incorporation of substantial amounts of data and has shown to have an excellent content validity, relevance, appropriateness and usefulness, but the time consumed to collect the data in the clinical setting, needs to be further evaluated.
Conclusions
The present study, is the first to provide a universally applicable multimodal patient profile that can be used as a framework to methodically describe patients with adult spinal deformities. Physicians managing adult spine deformities are encouraged to assess their patients holistically using this profile, and that decision-making regarding treatment should be made with this profile in mind, and not just based on radiographic findings. Different combinations of these factors can give an indication of the severity of the disease, help in patient counseling, facilitate shared decision-making, future risk stratification and treatment recommendations. This will ultimately improve quality of care for patients with ASD. Additionally, identifying groups of ASD patients with similar profiles can potentially help classifying ASD and developing respective decision-making pathways.
Footnotes
Appendix: List of Panelists in the Delphi Process
Acknowledgments
The study was proposed by AO Spine Indian Subcontinent (AOSIN) on behalf of AO Spine Asia Pacific (AOSAP) in response to the AO Spine Global Research Grant call for proposals. This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department. The consensus based on Delphi process was reached thanks to the contributions of expert surgeons and radiologist, as panelists, across the globe. The list of panelists is provided in the Appendix. The experts were identified through the recommendations provided by AO Spine Asia Pacific, AO Spine Europe and Southern Africa, AO Spine Latin American, AO Spine Middle East and Northern Africa, and AO Spine North America.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department.