
Abstract
Study Design:
Randomized controlled trial.
Objectives:
This prospective trial aimed to compare the effectiveness of etoricoxib and acetaminophen in terms of post-operative morphine consumption and pain score in patients undergoing lumbar laminectomy.
Methods:
Forty lumbar-laminectomy patients aged between 18 and 50 years were enrolled, randomized, and allocated into either the etoricoxib group or the acetaminophen group. The measures assessed were the amount of morphine consumed and pain visual analog score (VAS) at 12, 24, and 48 hours after surgery. Adverse events were recorded.
Results:
Patients in the etoricoxib group had statistically significantly lower morphine consumption than those in the acetaminophen group at 12 hours (P-value = .006), 24 hours (P-value = .006) and 48 hours (P-value = .011). Patients in the etoricoxib group had lower VAS scores than those in the acetaminophen group at 0, 12, 24, 48 hours, the difference being statistically significant at 48 hours (P < .001).
Conclusions:
Compared to acetaminophen, etoricoxib can significantly reduce post-operative morphine consumption and improve the pain score at 12, 24, and 48 hours.
Introduction
Degenerative change of the lumbar spine can cause lumbar stenosis or lumbar nerve root compression. The Spine Patient Outcomes Research Trial (SPORT) reported that surgery has a better therapeutic effect than non-surgical treatment, both in the field of pain reduction and healthy function of organs. 1 Lumbar laminectomy is one of the common operative procedures to treat lumbar stenosis. 2 Conventional lumbar laminectomy usually involves the extensive dissection of soft tissue, ligament, and bone, 3 typically bringing on moderate to severe pain, especially in the first few days after the operation.4,5 The severity of pain depends on the number of affected levels and tissue injuries from the surgical techniques. 6 Proper pain management is essential to allow patients to pass through the surgical treatment experience; pain relief is required to mobilize the patient and speed recovery.
Currently, pain management during the peri-operative period is based on the multimodal analgesia principle, in which a combination of analgesics is used to minimize the dosage, optimize efficacy and minimize the risk of adverse events. 7 The use of non-steroidal anti-inflammatory drugs (NSAIDs) together with opioid drugs also can significantly reduce side effects of the latter, such as nausea, vomiting, bloating and constipation.8,9 NSAIDs are not recommended as the first choice during and post-operative period because of the risk of bleeding, but selective cyclooxygenase-2 (COX-2) inhibitors do not affect platelet aggregation. 10 Etoricoxib is a drug in the selective COX-2 inhibitors group that reportedly reduces pain in acute conditions, such as in patients who have undergone dental surgery, bone and joint surgery, as well as chronic pain such as rheumatoid arthritis.10,11 The dosage for chronic pain is 30 mg-90 mg per day and the dosage for acute pain is 90-120 mg per day. 12 Florescu et al 13 reported that etoricoxib reduced morphine requirement and was superior to placebo (mean difference= −18, P-value < .0001) and to ketoprofen (mean difference= −9.8, P-value < .0001) among patients who had undergone total knee replacement. Lakshmi et al 14 evaluated the use of etoricoxib for post-operative pain relief in patients that had undergone a lumbar laminectomy and found that there was a reduction in the visual analog score in the etoricoxib group when compared with placebo. Acetaminophen inhibits the creation of prostaglandin in the central nervous system. The recommended dosage is 325-1000 mg and can be repeated every 4-6 hours (maximum 1,000 mg and not exceeding 4,000 mg per day). 15 Acetaminophen is effective for the treatment of post-operative pain; it also reduces the consumption of morphine after surgery. 16
There is still minimal research data about the effectiveness of etoricoxib in patients who have undergone lumbar surgery. Therefore, we studied whether post-operative administration of etoricoxib reduces pain and lowers morphine consumption. The primary hypothesis was that etoricoxib would reduce morphine consumption compared to acetaminophen for post-operative analgesia after lumbar laminectomy surgery. The results of the study should inform future pain management in patients following lumbar surgery.
Materials and Methods
Study Design and Setting
This single-center, prospective randomized controlled trial was reviewed and approved by the institute’s Ethics Committee for Human Research (reference number HE 601 275). Informed consent was obtained from all patients included in the study. The study was performed at the university hospital from June 2016 to November 2018.
Participants/Study Subjects
Patients assessed for eligibility were aged between 18 and 75 years, were undergoing lumbar laminectomy under general anesthesia, assessed as physical status class I according to the American Society of Anesthesiologists guidelines and could operate a patient-controlled analgesia device. Exclusion criteria were: (a) any known allergy to etoricoxib, morphine or acetaminophen; (b) history of previous lumbar surgery; (c) history of a bleeding disorder, hepatic impairment (Child-Pugh score > 5) or renal impairment (creatinine clearance < 30 mm/min); (d) history of uncontrolled hypertension, heart disease or cardiac surgery; (e) opioid drug abuse; (f) pregnancy or lactation; (g) current chronic anticoagulant or antiplatelet therapy; and (h) any contraindication to general anesthesia and inability to give informed consent. All patients were instructed how to use patient-controlled analgesia (PCA) device and how to assess pain using a verbal, visual analog scale ranging from 0 (no pain) to 10 (worst pain possible).
The patients (n = 40) were stratified into 2 groups, the laminectomy group and the laminectomy plus instrumented posterolateral fusion group. A randomization list was generated by computer before recruitment (allocation ratio 1:1). Each random number, containing assigned medication (etoricoxib or acetaminophen), was kept in an opaque sealed envelope. All enrolled patients were randomized and allocated into either the acetaminophen group or the etoricoxib group (Figure 1). The nurse, who was not involved in the randomization procedure, gave the medication to each patient according to the randomization code. The data collector and data analyzer were blinded to group allocation.
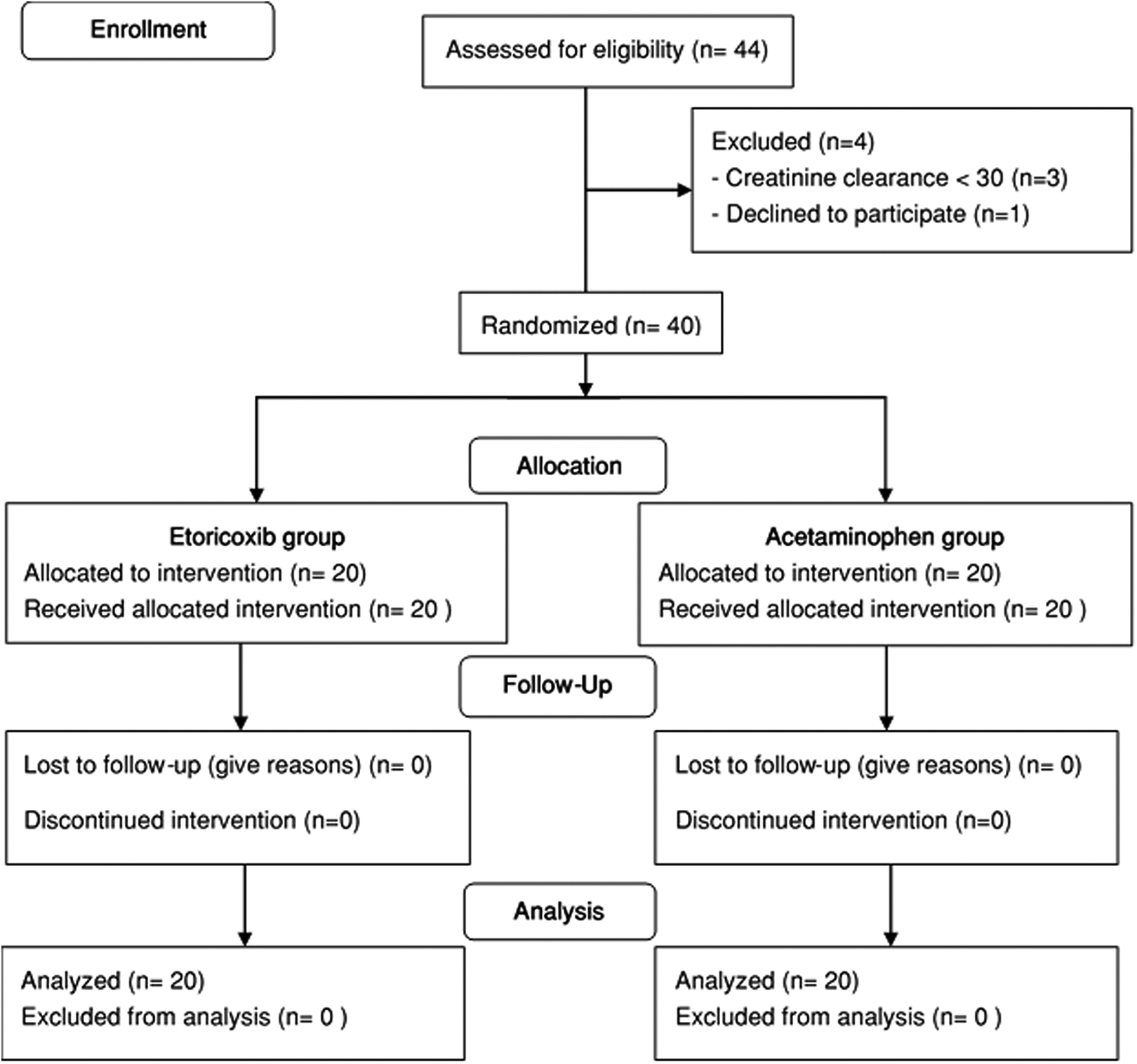
The CONSORT flow diagram describes recruitment, randomization, and follow-up of patients in the study.
Surgical Procedure
Patients in the etoricoxib group received etoricoxib 30 mg 2 hours before surgery and then 30 mg every 6 hours after surgery. Patients in the acetaminophen group received acetaminophen 500 mg 2 hours before surgery and then 500 mg every 6 hours post-operatively. Anesthetic techniques were standardized among the participating anesthetists. The patients in both groups received general anesthesia. When the patient was in the operating room, blood pressure and oxygen saturation were measured. An electrocardiogram was recorded. Anesthesia was induced by propofol (2 mg/kg). Endotracheal intubation was facilitated by Cisatracurium (0.15 mg/kg). Then anesthesia and muscle relaxation were maintained according to the anesthetic standards. No local anesthetics or any other medications with a possible analgesic effect were administered during surgery or within 48 hours after surgery. At the end of the operation, the anti-muscle relaxant was given, and the oropharyngeal tube was removed.
Two spinal surgeons performed all surgical procedures. Surgical techniques were standardized. For patients with spinal stenosis, decompression was achieved by laminectomy and foraminotomy. For patients with instrumented fusion, pedicular screw fixation was performed followed by posterolateral fusion using the local bone graft.
Aftercare
All patients received the same post-operative management. The PCA device was connected to patients at the post-anesthesia care unit (PACU). The PCA solution contained 1 mg of morphine per 1 ml and the device delivered 1 mg per dose. The lockout interval was 5 minutes. The 1-hour limit was 10 ml.
Description of Follow-Up Routine
The amount of morphine consumed from a PCA device was recorded at 12, 24 and 48 hours after surgery. No other analgesic drug was offered until the PCA device was disconnected from patients (48 hours). However, any patient with severe pain that was not adequately controlled by PCA morphine could withdraw from the study and receive other supplemental analgesic drugs. Patients in this group were still included in the trial and evaluated according to the intention-to-treat principle. The criterion for early termination of the study was severe adverse reactions affecting the benefit-to-risk ratio.
Variables, Outcome Measures, Data Sources and Bias
Demographic data of the patients, including age, sex, weight, height, body-mass index (BMI), duration of surgery, and the amount of post-operative bleeding, was recorded. The primary outcome measurement was the amount of morphine consumed from a PCA device at 12, 24, and 48 hours after surgery. Pain experienced, according to the visual analog score (VAS) was recorded at PACU, 12, 24, and 48 hours by patients indicating their pain rating scale. Adverse events such as respiratory depression (respiratory rate less than 8 breaths per minute), hypotension (systolic blood pressure lower than 80% of baseline or lower than 80 mm Hg), sedation, pruritus and dyspepsia were assessed during 0 to 48 hours. All adverse events were recorded as “yes” or “no.” Post-operative bleeding was measured by drain content (ml).
Accounting for All Patients/Study Subjects
Forty-four consecutive patients undergoing lumbar laminectomy were assessed for eligibility and enrolled. Four patients were subsequently excluded because of having creatinine clearance < 30 mm/min (n = 3) or unwillingness to participate (n = 1).
Statistical Analyses
Patients were evaluated using the intention-to-treat principle. The analysis was performed using SPSS (version 21, IBM Corporation, Armonk, New York). All data was tested for normality using the Shapiro-Wilk test. Continuous parametric data is presented as mean ± SD. A repeated-measures analysis of variance (ANOVA) was used for all repeated measure variables. An independent sample t-test with Bonferroni correction was used to test the mean differences between the treatment groups. All nonparametric data is presented as median with ranges and categorical variables are reported as proportions and percentages. Nonparametric data and categorical data was analyzed using nonparametric tests.
Sample Size Calculation
According to previous studies by Florescu et al 13 and Kesimci et al 17 the post-operative morphine consumption by patients administered etoricoxib averaged 27 mg (standard deviation (SD) 14.3) whereas patients administered acetaminophen consumed on average 40 mg (SD 10.9) of morphine. Spinal surgery and total knee arthroplasty are both major procedures according to the expected levels of pain. 18 We hypothesized that etoricoxib can reduce morphine consumption relative to acetaminophen. Using a statistical significance level of 0.05 and a study power of 0.80, the required number of subjects in each group is at least 16 to give 90% power for detecting a 20% difference in morphine consumption over 48 hours.
Results
Demographics, Description of the Study Population
Forty-four patients (26 females and 18 males) were eligible. Four patients were excluded, because of creatinine clearance less than 30 mm/min (n = 3), unwillingness to participate n = 1). Forty patients were enrolled, randomized and all completed the study. The patient’s peri-operative characteristics were similar in both the etoricoxib and acetaminophen groups (Table 1). There were no significant differences in mean age (59.0 ± 10.9 vs. 58.5 ± 12.6 years), BMI (25.9 ± 4.4 vs. 25.9 ± 4.2 kg/m2) and operative time (74.7 ± 27.2 vs. 75.0 ± 35.1 min). No patient was withdrawn because of severe pain or a severe adverse event.
Peri-Operative Patients’ Characteristics.a
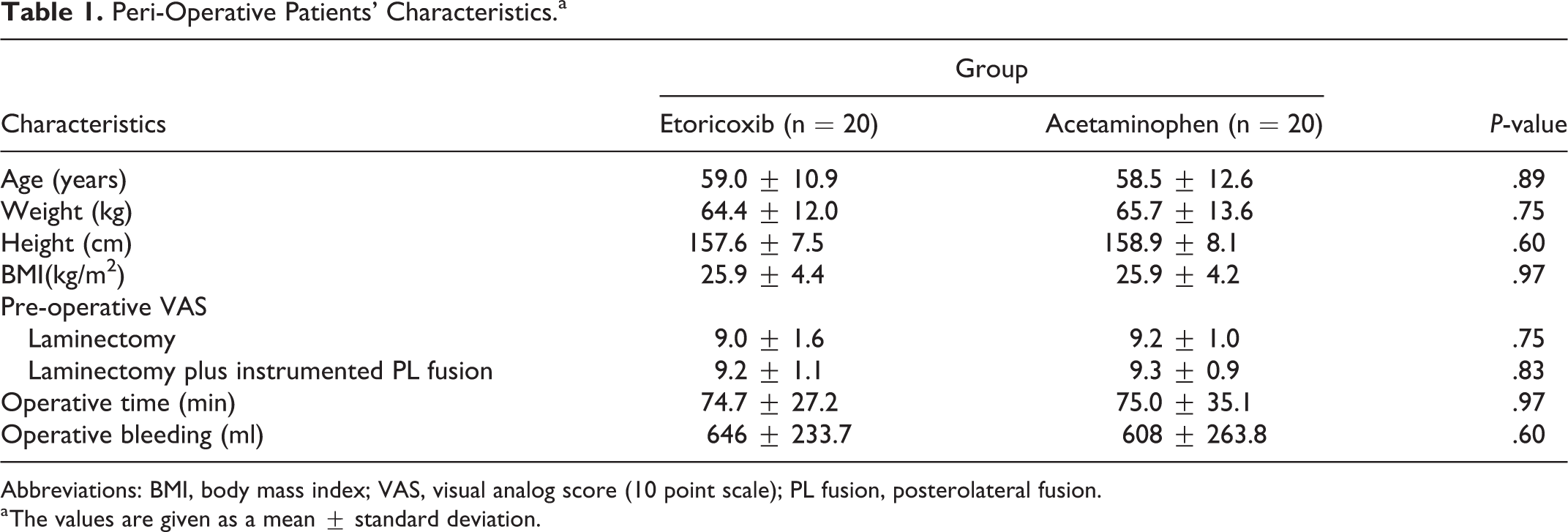
Abbreviations: BMI, body mass index; VAS, visual analog score (10 point scale); PL fusion, posterolateral fusion.
a The values are given as a mean ± standard deviation.
Etoricoxib significantly reduced morphine consumption compared to acetaminophen at all-time intervals after surgery (repeated-measures ANOVA, P-value = .0001) (Table 2 and Figure 2). The difference in morphine consumption was statistically significant at 12 hours (P-value = .006), 24 hours (P-value = .006) and 48 hours (P-value = .011) (Table 3).
Mean of Cumulative Morphine Consumption and Visual Analog Score at 12 Hours, 24 Hours and 48 Hours After Surgery.

Abbreviations: CMC, cumulative morphine consumption; VAS, visual analog score; SD, standard deviation.
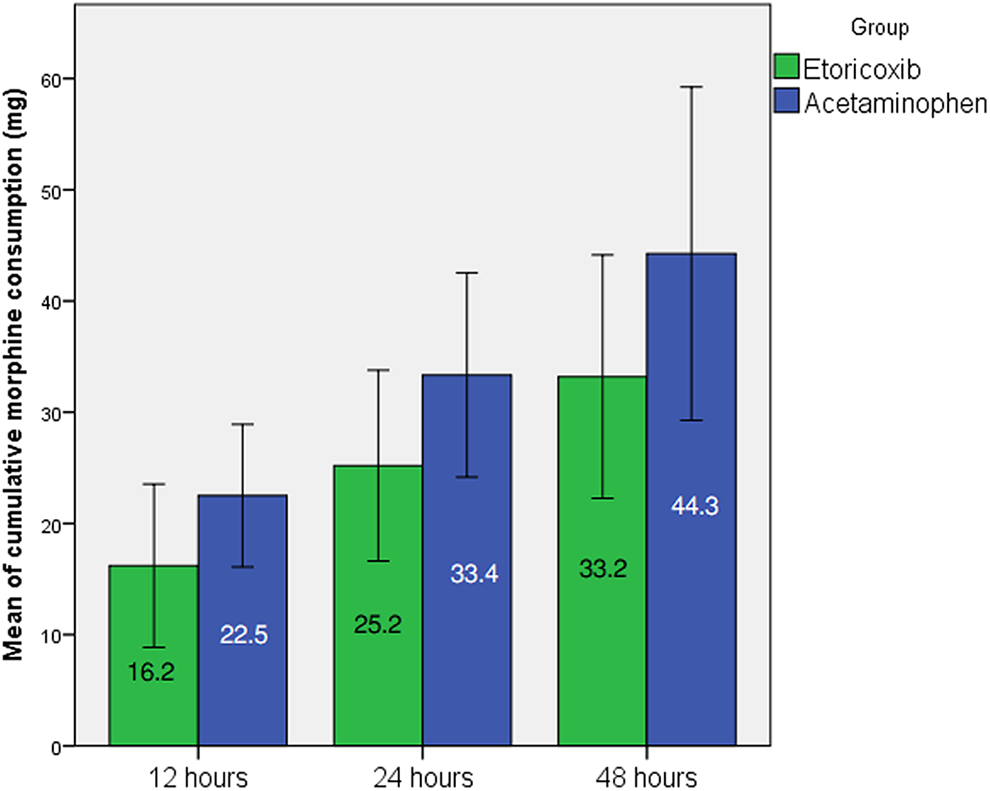
Mean of cumulative morphine consumption at 12 hours, 24 hours, and 48 hours after surgery (Error bars represent standard deviation).
Mean Difference and 95% CI Mean Difference of Cumulative Morphine Consumption and Visual Analog Score Between the Treatment Groups at 12 Hours, 24 Hours and 48 Hours After Surgery.a
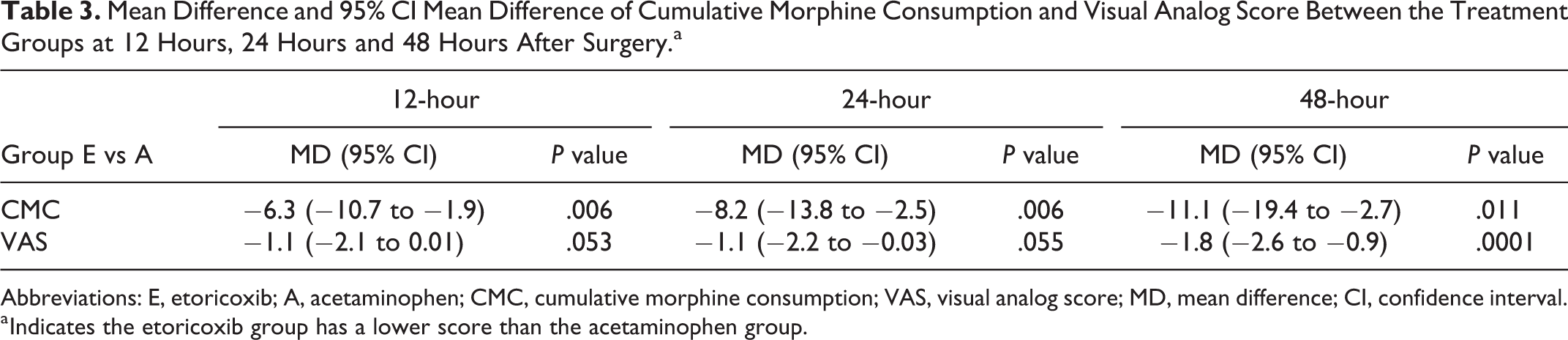
Abbreviations: E, etoricoxib; A, acetaminophen; CMC, cumulative morphine consumption; VAS, visual analog score; MD, mean difference; CI, confidence interval.
a Indicates the etoricoxib group has a lower score than the acetaminophen group.
Patients on etoricoxib reported reduced pain scores (relative to those on acetaminophen) at all-time intervals after surgery (Table 2 and Figure 3). The differences were statistically significant at 48 hours (P-value < .001) (Table 3).
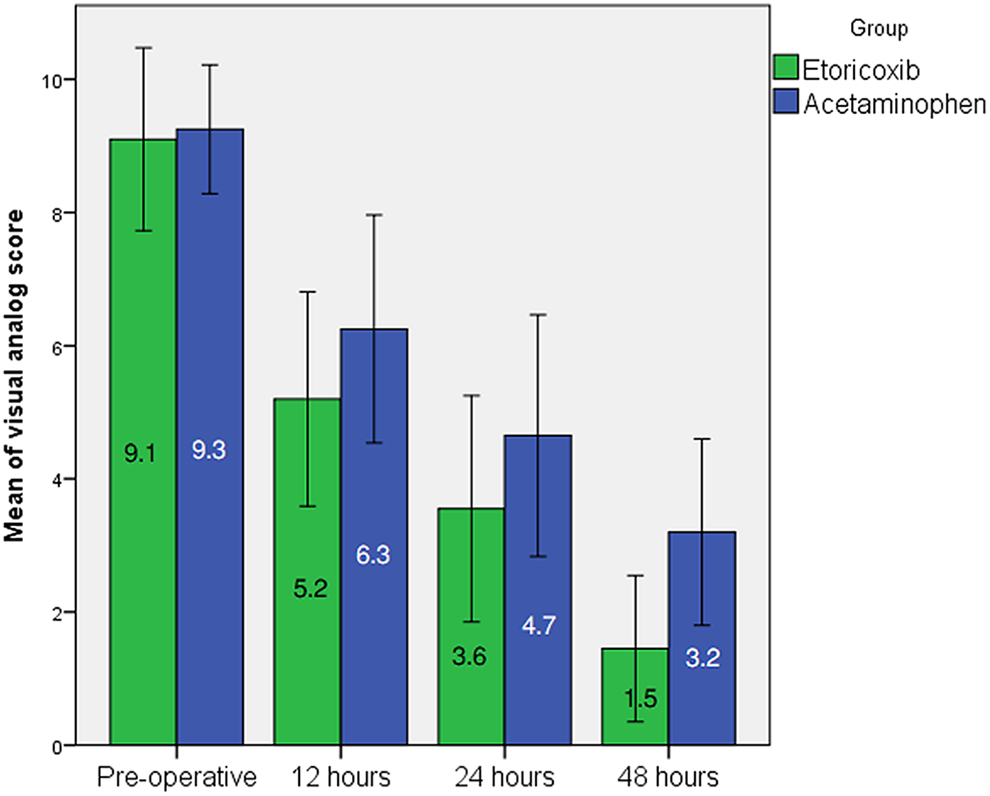
Mean of the visual analog score at pre-operative period together with 12 hours, 24 hours, and 48 hours after surgery (Error bars represent standard deviation).
Patients were evenly divided into laminectomy alone group (n = 20) and laminectomy plus posterior instrumented posterolateral fusion group (n = 20). All of 20 patients in the laminectomy group underwent 2 levels of decompressive laminectomy without fusion. For laminectomy plus posterior instrumented posterolateral fusion group, 1 patient underwent 2 levels, 9 patients underwent 3 levels, 4 patients underwent 4 levels and 6 patients underwent 5 levels surgeries. The repeated measure ANOVA was used to test the equality of group means. Comparing between laminectomy alone group and laminectomy plus instrumented posterolateral fusion group, there was no statistically significant VAS at anytime (P = .69 at initial, P = .16 at 12 hours, P = .11 at 24 hours, and P = .11 at 48 hours). In the aspect of morphine consumption, there was also not statistically significant (P = .89 at 12 hours, P = .62 at 24 hours, and P = .81 at 48 hours).
Adverse Events
The overall incidence of adverse events is summarized in (Table 4)—no statistically significant differences were noted between the study groups in any reported adverse events, except for pruritus. The overall incidence of pruritus was 35%, but the incidence was significantly higher (P-value = .04) in the acetaminophen group. No severe adverse event (such as respiratory depression, severe allergy, or severe cardiovascular event) was detected.
Incidence of Adverse Events.
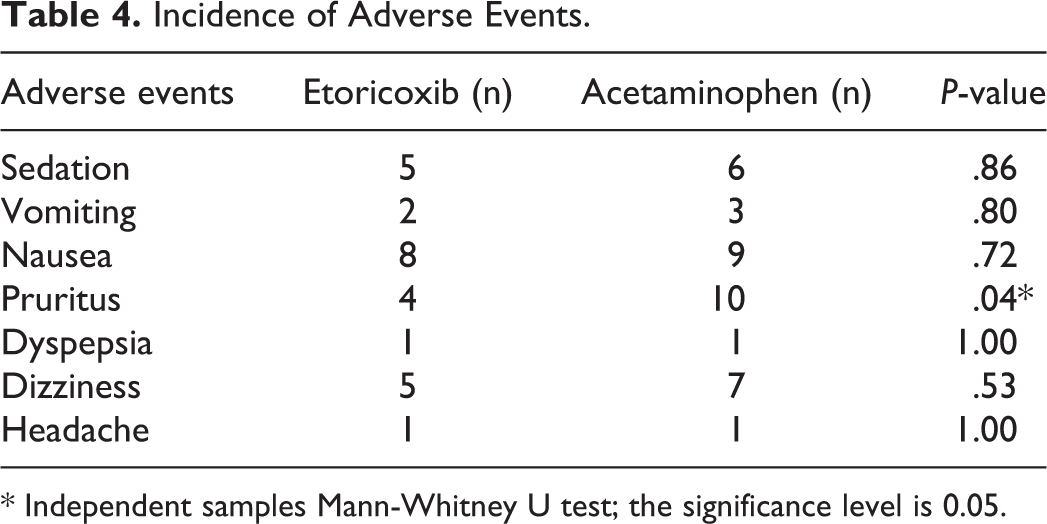
* Independent samples Mann-Whitney U test; the significance level is 0.05.
Discussion
Background and Rationale
Acetaminophen is useful for the treatment of post-operative pain. The analgesic effect seems comparable with NSAIDs. 19 Opioid and non-opioid analgesic combinations appear to be safe and effective after lumbar laminectomy. Patients demonstrate lower intravenous morphine requirements, better pain scores, and earlier time to solid food intake. 20 Therefore, we studied whether postoperative etoricoxib improves post-operative pain and reduces morphine consumption. We performed stratified block randomization by type of surgery. This approach ensured an appropriate balance across intervention groups. We studied the effectiveness of etoricoxib for 48 hours because most patients experience intense pain during the immediate post-operative period and require analgesic drugs for 48 hours after surgery, especially following spinal decompression and fusion procedures.5,21 Previous studies have reported that etoricoxib can reduce peri-postoperative pain better than placebo in spine surgery.22-24 However, these studies did not compare the post-operative pain relief of etoricoxib with that of acetaminophen, which was the usual pain-management drug. So, the current study was designed to compare the effectiveness of etoricoxib with that of acetaminophen at dosages similar to those used in previous studies of spine surgeries.23,25 According to drug information of FDA Thailand Ministry of Public Health, the dose of acetaminophen was 500 mg to 750 mg every 4 to 5 hours for bodyweight 50-67 kg. The minimum dosing interval of 4 hours. 26 In addition, McNeil Consumer Healthcare, which produces the Tylenol brand of acetaminophen, has voluntarily reduced the maximum recommended daily adult dose of its 500 mg tablet product to 3 g and of its regular-strength 325 mg tablet to 3250 mg. 27 Dosage from drug monograph was 325 to 650 mg PO every 4 to 6 hours, as needed. 28 We used 500 mg every 6 hours which was 2000 mg per day in the protocol. Etoricoxib is a long-acting drug and could be used as a separate dose. Shi et al used 120 mg per day for degenerative lumbar scoliosis fusion and reported a good result. 23 We used the same interval of drug administration (both acetaminophen and etoricoxib) to equalize the nurse visiting periods that may bias the result (patient-reported outcomes).
We found that peri-operative administration of etoricoxib resulted in less morphine consumption, lower pain scores, and the number of adverse events compared with acetaminophen after lumbar laminectomy with or without instrumentation. The results support our hypothesis that etoricoxib is superior to acetaminophen in reducing total morphine consumption. Previous studies in lumbar spine surgery have demonstrated the analgesic efficacy of etoricoxib in association with the peri-operative administration of celecoxib, rofecoxib and parecoxib.21,29 Patients on etoricoxib used 24% less total morphine compared with acetaminophen. The results will inform post-operative pain management in a lumbar laminectomy. Due to the positive outcomes of using both etoricoxib and acetaminophen, a combination of these drugs can be used in lumbar spine surgery for multimodal pain management.
Three randomized controlled studies 24,30,31 have compared etoricoxib to codeine combined with acetaminophen in dental surgery: all described a better outcome in the etoricoxib group. Pain scores and rescue medication were used by these studies to represent the result. Some recent studies of etoricoxib in orthopedic surgery13,14,24,31 have yielded results consistent with our study: the etoricoxib group used less morphine and experienced lower pain intensity. Florescu et al 13 reported that etoricoxib reduced morphine requirement and was superior to placebo (mean difference= −18, P-value < .0001) and ketoprofen (mean difference= −9.8, P-value < .0001) in patients following total knee transplant. Lakshmi et al 14 evaluated the effect of etoricoxib on post-operative pain relief in patients who had undergone a lumbar laminectomy and found that there was a reduction in visual analog score in the etoricoxib group when compared with placebo. We used morphine consumption (accurately recorded via PCA devices) as a primary measure to demonstrate the superior efficacy of etoricoxib over acetaminophen for post-operative pain relief in a lumbar laminectomy. Not surprisingly, the VAS showed no clinically significant differences between the groups of treatment. All patients used the PCA when they required morphine for their pain. From this situation, we compared the differences of drugs based on morphine consumption.
Adverse events were frequent regardless of treatment, as is common during the immediate post-operative period. No severe adverse events (such as respiratory depression, severe allergy, thromboembolism, or severe cardiovascular adverse event) were seen with etoricoxib. The incidence of adverse events was similar between etoricoxib and acetaminophen except for pruritus, which was significantly more frequent in the acetaminophen group. This result may be explained by the lower morphine consumption in the etoricoxib group. Opioid-induced pruritus (OIP) is a common adverse effect, occurring in 10% to 50% of patients receiving intravenous opioids. 32 We observed the incidence of pruritus to be 35%.
Strengths and Limitations
This present study is the first to compare etoricoxib with acetaminophen in lumbar laminectomy in the same setting and same period. The sample size had adequate power to detect an effect. There was no missing data because all the patients were admitted and measured. The collection of data was finished before patients were discharged from the hospital. Some limitations of the study need to be acknowledged. First, the shape of the etoricoxib tablet was different from acetaminophen so that some patients may have known to which group they were allocated. Second, the VAS is a subjective way to measure pain intensity and may not represent the true pain intensity experienced by the patients. However, morphine consumption is an objective measurement, and our results on morphine use were consistent with the VAS. Third, we assessed pain only at rest: pain during movement may not be similar. Fourth, the duration of the study was short, and we did not evaluate patients in terms of complications after they left the hospital. To minimize these limitations, we used a blinded outcome assessor and reported only early post-operative pain management. It is of clinical relevance that patients on etoricoxib used 24% less total morphine compared with those on acetaminophen. The results should be useful in guiding post-operative pain relief with minimal complications. Pain relief is important for the early mobilization of the patient, leading to a reduction in complications and length of hospital stay. Further studies, especially on clinically relevant outcomes such as venous thromboembolism and length of hospital stay, are required.
In conclusion, the administration of etoricoxib significantly reduces (relative to acetaminophen) post-operative morphine consumption and improves pain scores at 12, 24, and 48 hours after surgery. However, both acetaminophen and etoricoxib are effective in treating acute post-laminectomy pain. Among adverse events, only pruritus was significantly different between the groups, having a higher incidence in the acetaminophen group.
Footnotes
Acknowledgments
The authors are deeply indebted to Professor Kitti Jirarattanaphochai for suggestions in preparing the manuscript. The authors would like to thank Professor David Blair for editing the manuscript via Publication Clinic Khon Kaen University, Thailand.
Authors’ Note
S. Weraarchakul, MD, Orthopaedic Resident, Department of Orthopaedics, S. Sae-Jung, MD, PhD, FRCOST, Associate Professor, Department of Orthopaedics, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand. S. Weraarchakul: Designed the study, performed the surgeries, edited and reviewed the manuscript. S. Sae-Jung: Designed the study, performed the surgeries, compiled and analyzed the data, wrote and reviewed the manuscript. The manuscript submitted does not contain information about medical device(s)/drug(s). Ethical approval was obtained (reference number HE 601 275) and patients provided written consent. Thai Clinical Trials Registry (identifier TCTR20181223001).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received the fund from The Invitation Research Grant, Faculty of Medicine, Khon Kaen University, Thailand.