
Abstract
Study Design:
Descriptive retrospective study.
Objective:
DDH is a common lower limb deformity. It has been reported that this deformity can change the sagittal alignment of spine and pelvis. Sacral obliquity (SO) and iliac obliquity (IO) have been proven simple and reliable pelvic-lower limb coronal parameters to evaluate the coronal balance of the pelvis. To study the spine-pelvic coronal compensation mechanism of pelvic obliquity in patients with developmental dysplasia of the hip (DDH).
Methods:
We collected the data of 110 patients with DDH in our hospital from January 2009 to December 2019, who underwent total hip arthroplasty. We used ICC (Intraclass correlation coefficient) to test the reliability of the measurement result of SO and IO in patients with DDH. A paired t-test was used for the statistical analysis.
Results:
The intra observer reliability of IO and SO was 0.965 and 0.875 respectively, and the inter observer reliability of IO and SO was 0.887 and 0.889 respectively. The sacroiliac joint and spine can compensate for pelvic obliquity in patients with DDH. We classified the compensatory mechanism into 3 types according to the different imaging performances.
Conclusions:
The sacroiliac joint has a considerable compensatory ability to ensure coronal balance. We clarified and classified the compensatory mechanism of pelvic obliquity into 3 types. We differentiated the pelvic obliquity in patients with DDH and in those with scoliosis, which is clinical significant to understand the process of development of the disease.
Introduction
Developmental dysplasia of the hip (DDH) includes a wide range of conditions associated with abnormal hip development in infancy and early childhood,1-4 and is 1 of the most important causes of osteoarthritis of the hip in adulthood. 5 Pelvic obliquity often occurs in patients with DDH due to acetabular dysplasia. In 1983, Offierski and Macnab proposed that pathological changes in the hip joint could cause changes in the sagittal sequence of the spine and affect the overall balance. 6 There are few reports on mechanism of the coronal position alterations in patients with DDH.
Sacral obliquity (SO) is the angle between the line of the transition point of the sacral wing and superior articular process of the S1 vertebra and the horizontal plane. Iliac obliquity (IO) is the angle between the line of the iliac crest and the horizontal plane (Figure 1). Both SO and IO can be used to assess pelvic obliquity. Song et al 7 reported that SO and IO as simple and reliable pelvic coronal parameters to evaluate the coronal balance in patients with lumbar scoliosis. Therefore, the data of 110 patients with DDH was collected in this study to explore the possible way to maintain coronal balance in such patients with pelvic obliquity.
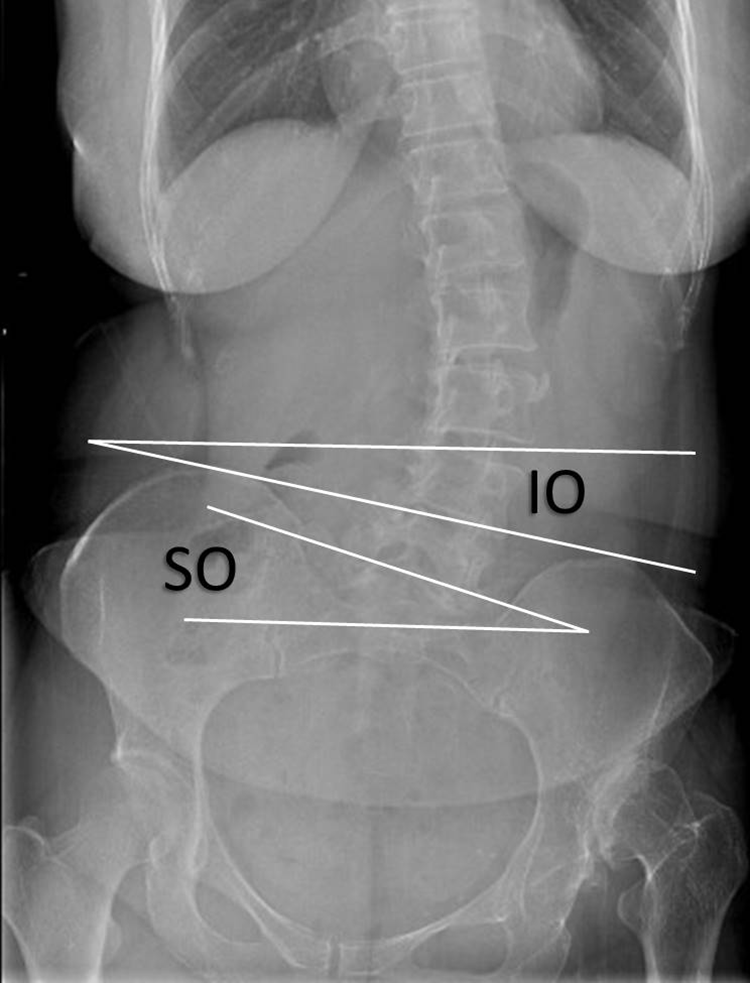
Measurements of radiological parameters: SO and IO. Sacral obliquity (SO) is the angle between the line of the transition point of the sacral wing and superior articular process of the S1 vertebra and the horizontal plane. Iliac obliquity (IO) is the angle between the line of the iliac crest and the horizontal plane.
Methods
Statement for Informed Consent
This was a retrospective study. Only the clinical data of patients was collected, and the study did not interfere with the treatment plan, or pose any risk to the physiology of the patients. Considering the retrospective nature of this study, non-disclosure of the information was provided by the patients.
Statement for Institutional Review Board Approval
In China, under national and cantonal laws and for this kind of data collection, no formal approval is required, neither by the national ethics committee nor by the cantonal commissioner for data protection. These are not even recommended by the Medical ethics Expert Committee of national health committee of China. Thus, Institutional review board approval is not suitable for this study.
Measurement of Imaging Parameters
We collected the data of patients with DDH in our hospital from January 2009 to December 2019. All patients underwent total hip arthroplasty. Complete preoperative and postoperative data, including whole-leg standing AP radiographs of 110 patients was available. Among them, whole-spine standing AP radiographs of 48 patients were available. We excluded patients with complete pelvic deformity and those with incomplete clinical data.
The pelvic coronal parameters of the patients were measured preoperatively and postoperatively. Two senior spine surgeons recorded the measurements to reduce the errors. During measurement, the image was partially enlarged to the full screen to improve the accuracy. The measurement parameters were as follows: (1) length of the lower limbs (LLL), which was measured as the distance from the midpoint of the femoral head to the medial malleolus (2) SO (3) IO (4) Cobb angle (in patients with scoliosis).
The coronal parameters of the pelvis and lower limbs were statistically analyzed. We used ICC (Intraclass correlation coefficient) to test the reliability of the measurement result of SO and IO in patients with DDH. A paired t-test was performed preoperatively and postoperatively. Changes in the coronal parameters of the pelvis and lower limbs were compared. P < .05 indicated that the difference is statistically significant difference. Statistical software SPSS 22.0 was used for data analysis.
Results
The average age of the 110 patients with DDH was 40.6 ± 10.7 years. The sample comprised 13 men and 97 women. The intra observer reliability of IO and SO was 0.965 and 0.875 respectively, and the inter observer reliability of IO and SO was 0.887 and 0.889 respectively.
The preoperative LLL of the patients was statistically different (Table 1). The average IO of the 110 patients was 6.3 ± 11.1° and SO was 6.2 ± 11.8°. We categorized patients with IO ≥ SO as group A and those IO < SO as group B. When the preoperative IO was large, the change in its value was greater than that in the SO. When the preoperative SO was large, the change in its value was greater than that in the IO (Table 2). Based on the analysis of 48 patients with whole-spine standing AP radiographs, we divided the compensatory mechanism of pelvic obliquity into 3 types according to the different imaging performances, and observed that the differences in the coronal pelvic parameters were statistically significant (Tables 3 and 4).
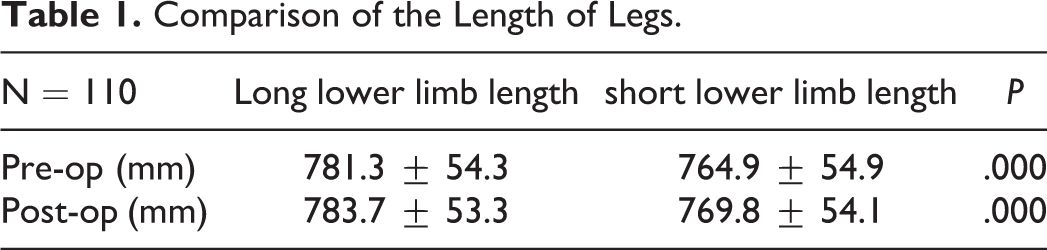
Comparison of the Length of Legs.
Changes of Coronal Pelvic Parameters After Surgery in 2 Groups.
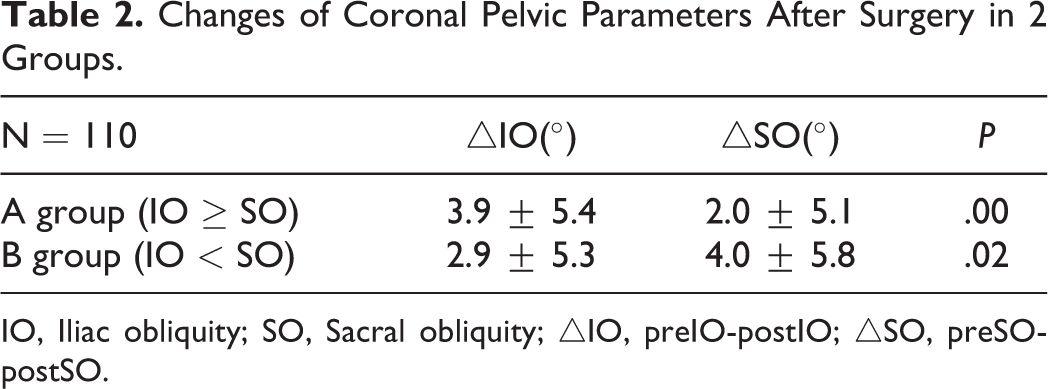
IO, Iliac obliquity; SO, Sacral obliquity; △IO, preIO-postIO; △SO, preSO-postSO.
Comparison of Pelvic Obliquity in 3 Compensation Mechanisms.
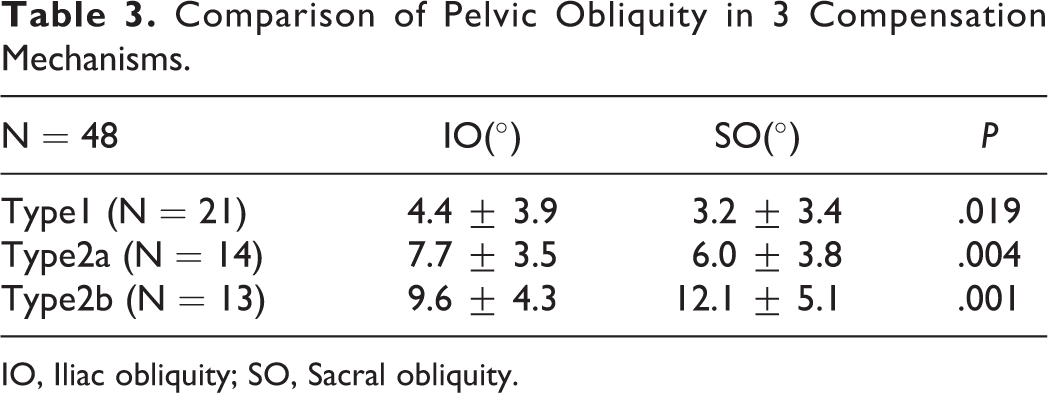
IO, Iliac obliquity; SO, Sacral obliquity.
Comparison of Coronal Pelvic Parameters in 3 Compensatory Mechanisms.

T1, Type1; T2a, Type2a; T2b, Type2b.
Discussion
In 1983, Offierski and Macnab proposed that pathological changes in the hip joint could cause changes in the sagittal sequence of the spine, and affect the overall balance. 6 However, few studies have investigated whether pelvic obliquity affects the coronal balance in patients with DDH. The World Scoliosis Research Society officially refers to the “sacral wing groove connection” and the “iliac crest connection” as the pelvic coronal reference line. The angle between the reference line and the horizontal plane is defined as the pelvic obliquity angle. 8 Dubousset et al 9 proposed the concept of pelvic vertebrae. They believed that the bony structure composed of the sacrum, ilium, and ischium has only 2 non-bone connections, namely the sacroiliac joint and the pubic symphysis; therefore, the pelvis can be considered an immutable bony structure. Song et al 7 reported that the SO and IO are simple and reliable pelvic coronal parameters, which can be used to evaluate the coronal balance in patients with lumbar scoliosis. They found that in patients with lumbar scoliosis, the SO was greater than the IO, which means that the sacrum is more oblique than the ilium. This result proves that the sacroiliac joint has a spontaneous compensation capacity. When the pelvic obliquity arises from the spine, the sacroiliac joint and lower limb compensate for overall coronal balance. When the deformity factor is proximal, such as in patients with scoliosis, it can affect the pelvis and limbs. Therefore we aimed to determine the manner by which coronal balance can be maintained in patients with DDH demonstrating pelvic obliquity and associated compensation mechanism. We assumed that the IO would be greater than the SO in cases where the pelvic obliquity arises from lower limbs.
First, the average IO of 110 patients was 6.3 ± 11.1° and SO was 6.2 ± 11.8°, which denoted pelvic obliquity. Subsequently, we compared the length of lower limbs (LLL) in patients with DDH and found significant difference (Table 1). These observations revealed that the pelvic obliquity was caused by leg length discrepancy (LLD). We established a successful model of pelvic obliquity in patients with DDH.
However, there was no significant difference between the IO and SO, indicating that the compensation mechanism is more complex than that assumed previously. We categorized patients with IO ≥ SO as group A and those with IO < SO as group B. Larger preoperative IO was associated with a greater change in the value .Similarly, larger preoperative SO was associated with a greater change in the value (Table 4). An immobile sacroiliac joint should be synchronous and equal changes in IO and SO. Thus, this result proves that sacroiliac joint has a compensatory ability.
Although we confirmed the existence of sacroiliac joint compensation, we are unaware of the mechanism of compensation for coronal balance. A possible hypothesis is that when the sacroiliac joint compensates for pelvic obliquity, the postoperative change in the sacrum would be less than that in ilium. In case of heavy obliquity wherein the sacroiliac joint cannot compensate, the postoperative change in the sacrum would be greater than that in the ilium.
Giles et al reported that in cases of leg length discrepancy (LLD), functional scoliosis occurred when the lumbar spine compensated for pelvic obliquity to maintain shoulder balance. 10 Therefore, we analyzed the data of 48 patients with DDH based on their whole spine-standing AP radiographs and divided the coronal pelvic obliquity into 3 types according to the shape of the spine. In type 1, IO > SO, the spine does not participate in compensation because the sacroiliac joints can compensate pelvis obliquity completely. In type 2a, IO > SO, both the sacroiliac joint and the spine are required to participate in the compensation. In type 2b, SO > IO, the sacroiliac joint is decompensates (Table 3), and is mainly compensated by the lower lumbar spine. Simultaneously, the sharp curvature of the lower lumbar spine causes the sacroiliac joint to change in the opposite direction (Figure 2 and Figure 3).
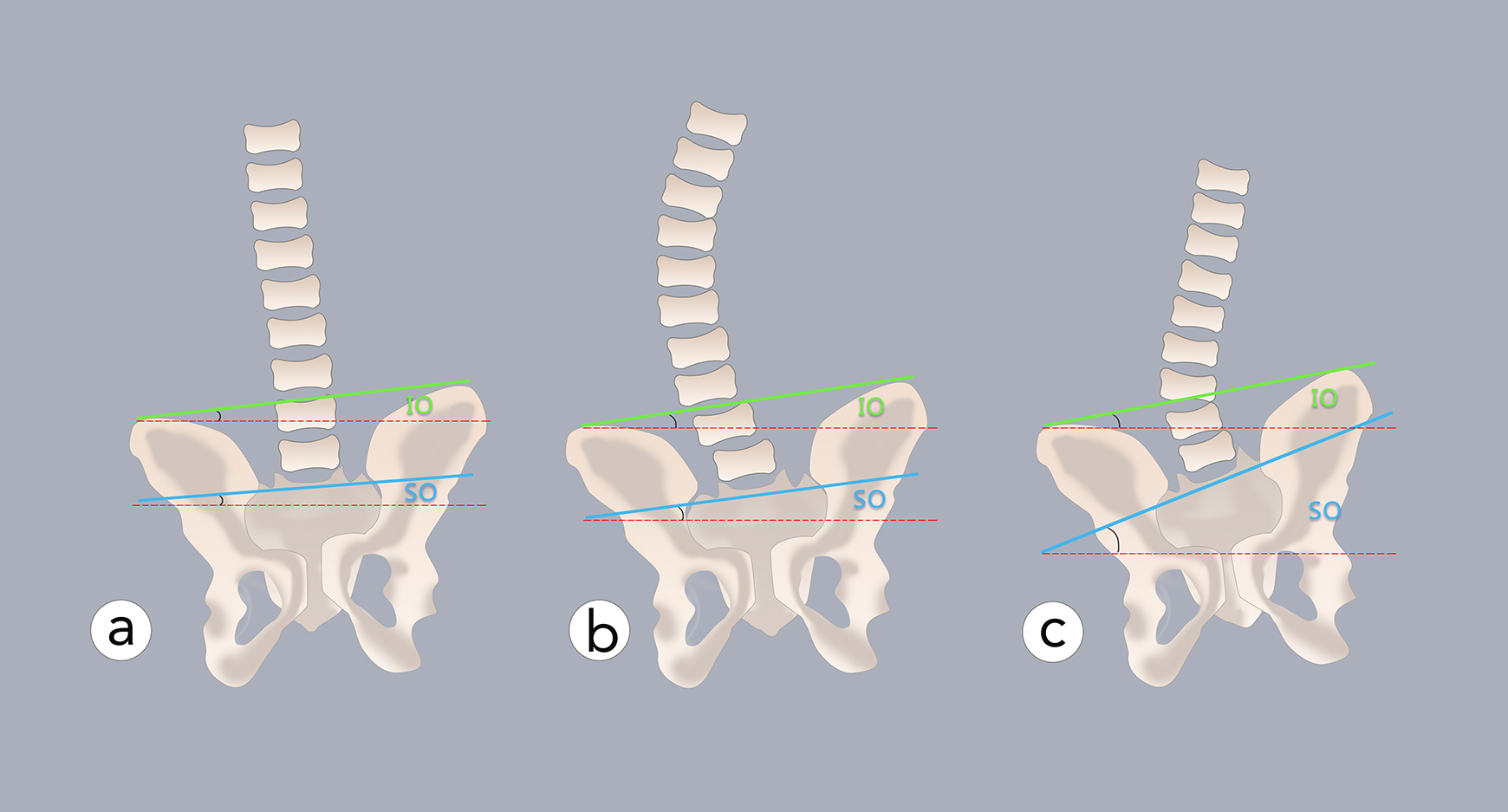
A, Type1 the pelvic obliquity is small and is compensated by the sacroiliac joints without the spine participating in the compensation of coronal balance. B, Type2a the pelvic obliquity is aggravated, and the sacroiliac joint alone is not enough to fully compensate. The spine participates in the compensation of the coronal balance, which manifests as a long and gentle c-shaped curve. C, Type2b the pelvic obliquity is severe, the sacroiliac joint is decompensated, and the sacrum becomes part of the compensatory curve of the lumbosacral curve. It manifests as a sharp short curve in the lumbosacral area.
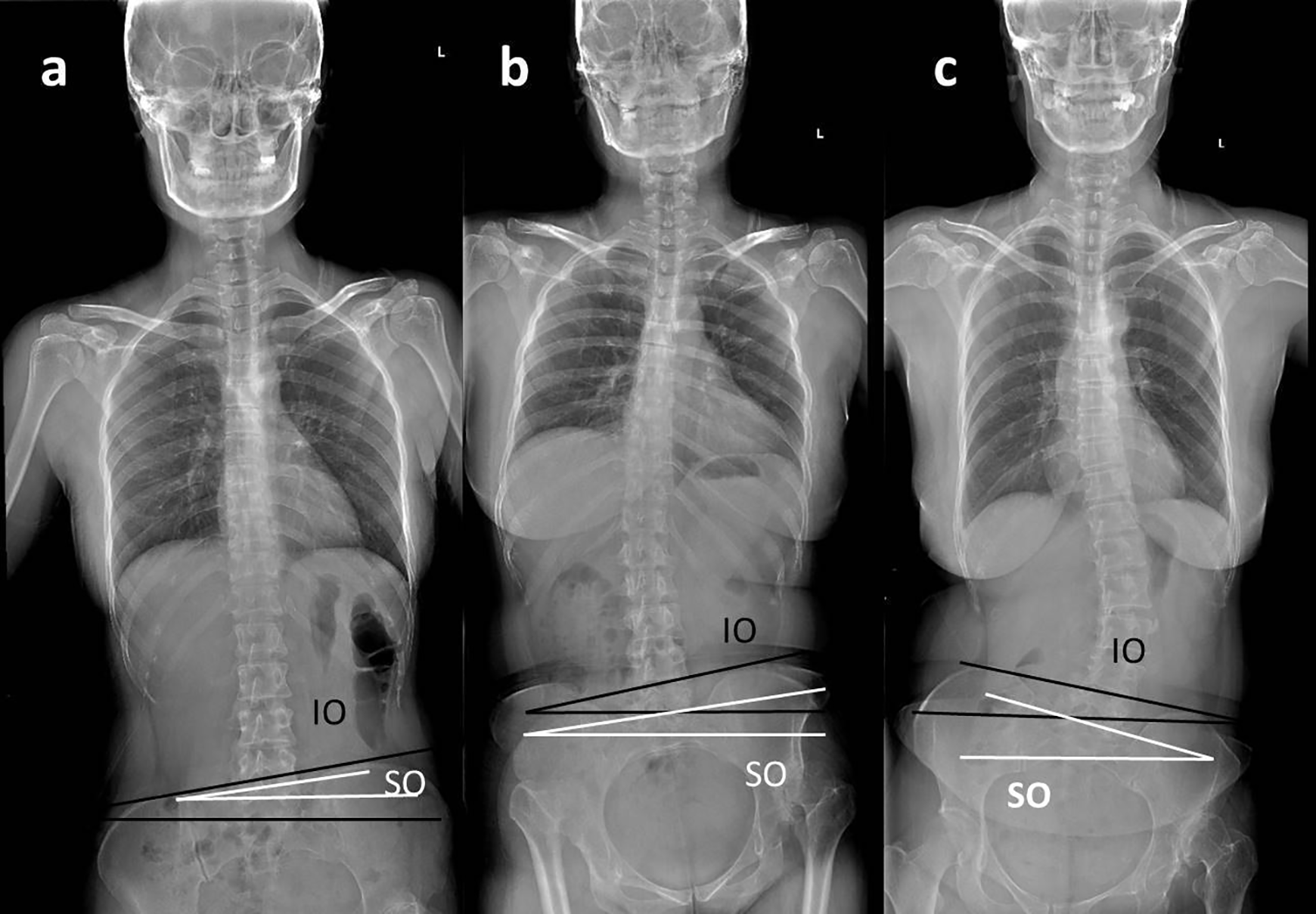
A, 36 years old woman classified in type1, IO = 3°, SO = 2.7°. B, 48 years old woman classified in type2a, IO = 9.7°, SO = 8.3°. C, 25 years old woman classified in type2b, IO = 12°, SO = 16.5°.
Therefore, we can conclude that in patients with DDH demonstrating pelvic obliquity, the sacroiliac joint will first participate in compensation to avoid coronal imbalance. The spine participates in the compensation when the sacroiliac joint cannot fully compensate for the imbalance, manifested as a gentle C-shaped long curve. In other words, the sacroiliac joint and spine participate in the compensation in a coordinated manner to achieve coronal balance. In cases where the compensation of the sacroiliac joint cannot correct the coronal balance, that is, when the sacroiliac joint is decompensated, it is mainly corrected by a larger lumbosacral curve. The sacrum then becomes a part of the lumbosacral sharp curve. The aggravation in obliquity results in the sacrum being in a state of reverse compensation, causing heavy obliquity of the sacrum.
The Cobb angle, IO, and SO values were in the following order: type 2b > type 2a > type 1 (Table 4). This shows that the sacroiliac joint is more likely to be decompensated and the Cobb angle is larger in cases of severe pelvic obliquity. However, this is only the overall trend. In fact, compensation of the sacroiliac joint in the coronal plane is affected by the compensatory ability of the joint itself. The compensatory ability of the patient’s sacroiliac joint and the severity of pelvic obliquity determine the compensation method of the joint.
Through this study, we could understand the compensation mechanism in patients with DDH demonstrating pelvic obliquity. Song et al proved that the lumbosacral curve and sacroiliac joint participate in the adjustment of pelvic balance in cases of pelvic obliquity caused by scoliosis. 7 In this article we observed that the spine and sacroiliac joint adjusted to maintain coronal balance in patients with DDH demonstrating pelvic obliquity. We could clearly recognize the difference between pelvic obliquity caused by scoliosis and by DDH, which have different compensatory mechanisms.
It is worth mentioning that the SO measured in this study was the line connecting the transition point of the sacral wing and the supra-sacral articular process, which is more reliable than direct measurement of the S1 lamina or pedicle projection.
In this study, we established a model of patients with DDH demonstrating pelvic obliquity and confirmed that the sacroiliac joint has a considerable compensatory ability to ensure coronal balance. In addition, we classified the compensatory mechanism of pelvic obliquity in patients with DDH into 3 types, which is clinically significant to understand the process of development of the disease.
Coronal pelvic obliquity can be divided into spinal and lower extremity origins. Through this study, we found that the compensation mechanism of pelvic obliquity in patients with DDH was significantly different from that in patients with scoliosis. The compensation mechanism of coronal balance should be the same in cases where pelvic obliquity arises from the lower limbs, such as in patients with leg length discrepancy (LLD). In fact, it is often found that both scoliosis and LLD occur in patients with adult spine deformity. All these factors lead to coronal pelvic obliquity, and individualized treatment should be provided to the patients. In cases where pelvic obliquity arises from the lower limbs, orthopedic shoes can correct the LLD, resulting in good clinical effects and reduction in unnecessary surgical treatment. Therefore, understanding this mechanism would help us to better identify and distinguish the factors causing pelvic obliquity, and determine a more suitable treatment for patients. It is suitable not only for patients with DDH, but also for those with other deformities.
Footnotes
Authors’ Note
This was a retrospective study. Only the clinical data of patients was collected, and the study did not interfere with the treatment plan, or pose any risk to the physiology of the patients. Considering the retrospective nature of this study and non-disclosure of the information provided by the patients, the need for informed consent was waived.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.