
Abstract
Study Design:
Retrospective multicenter study.
Objective:
To evaluate mid- to long-term surgical outcomes of thoracic dumbbell tumors managed by laminectomy and unilateral total facetectomy without instrumented fusion.
Methods:
A total of 15 patients with thoracic dumbbell tumors who underwent primary resection by laminectomy and unilateral total facetectomy without spinal instrumented fusion between 2000 and 2015 were reviewed. Patient characteristics, surgical outcomes (including spinal alignment and stability), disc degeneration, pain, disability, and health-related quality of life were evaluated. Additionally, to analyze the impact of the affected levels on these outcomes, we divided the patients into 2 groups: a middle thoracic group and a thoracolumbar group.
Results:
The mean duration of follow-up was 100.5 months (range, 36-190 months). The affected level was T3-T4 or below in all patients. Although the local kyphosis angle (8.1° to 12.7°), thoracic kyphosis angle (25.6° to 33.9°), and coronal Cobb angle (6.6° to 9.5°) significantly increased from preoperative to the final visit (P ≤ .02), no patient demonstrated spinal instability. From magnetic resonance imaging, no patient had a worse grade of disc degeneration in the affected level than those in the adjacent levels. The percentage of patients who presented with an Oswestry disability index ≤ 22% was 80%. Moreover, the surgical region did not adversely affect the outcomes. No patient required additional surgery due to spinal instability or deformity.
Conclusions:
Unilateral total facetectomy without fusion to resect thoracic dumbbell tumors caused neither spinal deformity nor instability requiring additional surgery at the mid- to long-term follow-up.
Keywords
Introduction
Spinal dumbbell tumors are relatively rare neoplasms characterized by their unique form, connecting 2 or more adjacent regions, including intradural, epidural, intraforaminal, and paravertebral spaces. 1 Most tumors are benign, neurogenic tumors, including schwannoma and neurofibroma; the thoracic spine is the second most common origin of the tumors, following the cervical spine.1,2 Although there are various surgical approaches for thoracic dumbbell tumors, including posterior,3-8 lateral, 9 and posterior and anterior combined approaches,10-12 unilateral total facetectomy with laminectomy or hemilaminectomy are the principal methods for direct visualization of the neural structure and resecting the intraspinal and intraforaminal component of the tumors. Since unilateral total facetectomy can cause postoperative spinal deformity and instability, some authors have described that they perform spinal fusion with instrumentation at the time of index surgery.4,6,7,13 Contrastingly, others reported the results of non-fusion surgery for thoracic dumbbell tumors without major complications.3,5,8,9,11,14 However, because most studies evaluated a small number of patients with short- to mid-term radiologic outcomes, there is a paucity of comprehensive evidence on longer term outcomes. In the current study, we investigated the mid- to long-term surgical outcomes of unilateral total facetectomy without instrumented fusion for resection of thoracic dumbbell tumors, focusing on spinal alignment and stability, degeneration of intervertebral discs and facet joints, pain, disability, and health-related quality of life.
Methods
Patient Population
This was a multicenter, retrospective study of patients who underwent primary resection of thoracic dumbbell tumors using unilateral total facetectomy without spinal instrumented fusion at 3 university hospitals. We received review and approval by the Institutional Ethics Committee of each institution involved.
From 2000 to 2015, 26 adult patients who underwent primary resection for thoracic dumbbell tumors (from T1-T2 to T12-L1) using unilateral total facetectomy were extracted (Figure 1). Of these, we excluded 3 patients for the following reasons: 1 patient presented with preexisting severe spinal deformity associated with neurofibromatosis type 1, and 2 patients received concomitant instrumented fusion at the index surgery because of severe distraction of the vertebral bodies and pedicles. The other 23 patients were invited to participate, and 16 patients agreed to participate and provided informed consent. Of these 16 patients, we excluded 1 patient who had received resection of T7-T8 dumbbell tumors and had T12 osteoporotic vertebral fracture at the final visit. Finally, 15 patients (9 men and 6 women) were analyzed with a follow-up rate of 65.2%. The participants provided written informed consent. We reviewed the medical charts and recorded the patients’ characteristics including the age at the time of surgery, sex, affected levels, Eden’s classification 15 and pathological diagnosis of the dumbbell tumor, the surgical approach, and the type of laminectomy (hemilaminectomy or conventional laminectomy). To analyze the effects of the affected levels on the outcomes, we divided the patients into 2 groups: the middle thoracic group with the affected level of T9-T10 or above and the thoracolumbar group with the affected level of T10-T11 or below.
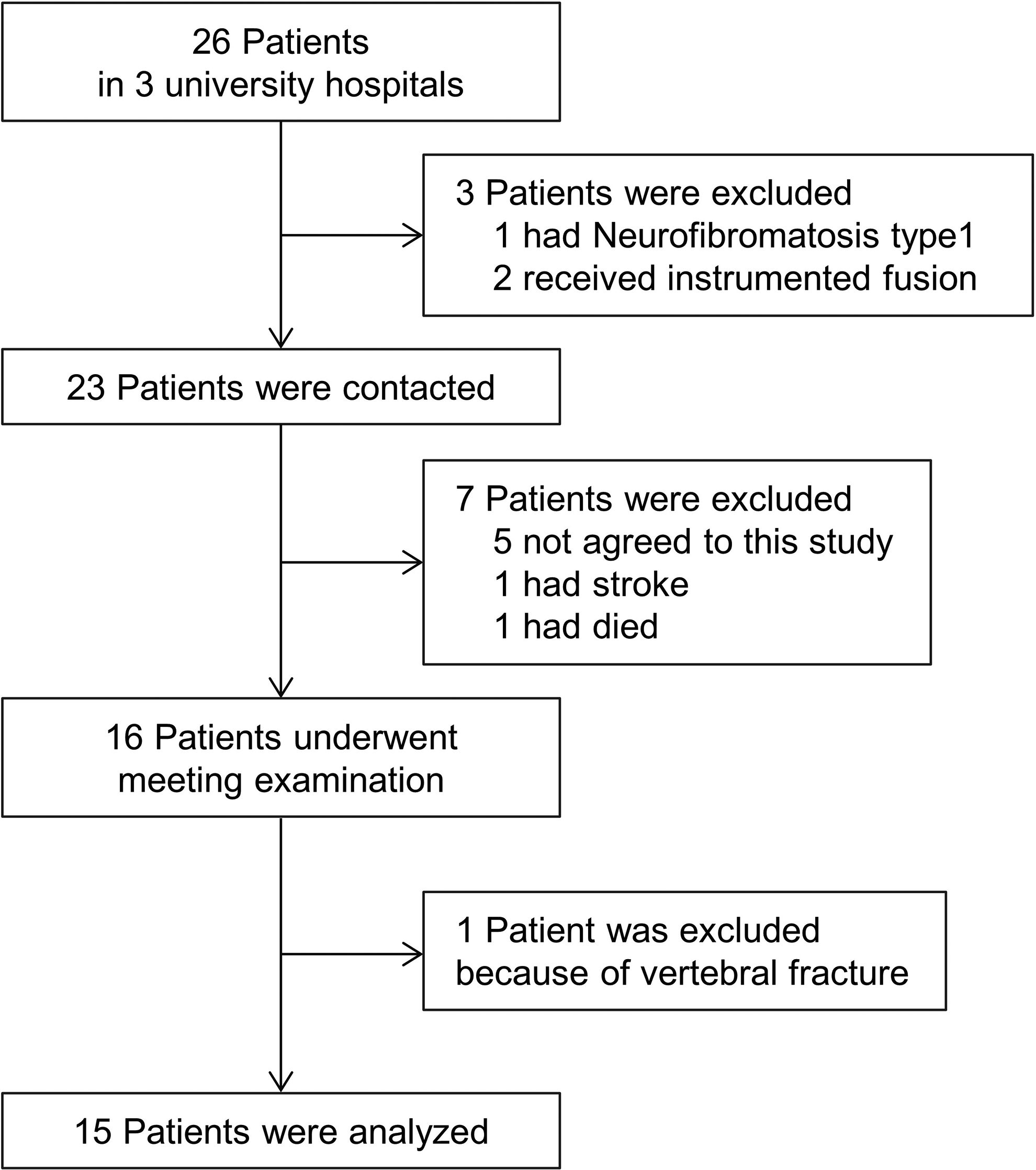
Flow chart showing included and excluded patients.
Surgical Techniques
To resect the dumbbell tumor, all patients underwent unilateral total facetectomy at the affected level without spinal instrumented fusion via the posterior approach. Two of the patients also underwent surgery via the anterior approach to expose and resect the huge paravertebral component of the tumor. All patients received conventional laminectomy or hemilaminectomy depending on the extent of the tumor. The spinous process was preserved during the hemilaminectomy. In principle, the tumors were resected with sacrifice of the involved nerve root. Only 1 patient (case 6) received reconstructive laminectomy in which the resected lamina was repositioned and fixed with polyethylene cable.
Radiologic Evaluation
We evaluated the preoperative and the latest postoperative radiographs. The parameters in the sagittal plane included local kyphosis angle (LKA) and T5-12 thoracic kyphosis (TK). LKA was measured as an angle between the upper endplate of the upper affected vertebra and the lower endplate of the lower affected vertebra. In the sagittal measurements, kyphosis was defined as positive and lordosis as negative. Using flexion-extension radiographs, we calculated the range of motion (ROM) at the affected level as follows: ROM of affected level = flexion LKA − extension LKA. Radiological measurements in the coronal plane included the following: Cobb angle, which was the maximum angle of scoliotic deformity containing affected level; and segmental wedge angle (SWA), which was the angle between the lower endplate of the upper affected vertebra and the upper endplate of the lower affected vertebra. 16
Furthermore, we used magnetic resonance imaging (MRI) at the final examination to evaluate tumor recurrence and degeneration of the intervertebral discs and facet joints. We assigned the Pfirrmann grade, a grading system of disc degeneration, 17 to the discs at the one-level upper, affected, and one-level lower levels. The presence of bulging disc and facet effusion were also assessed. The facet effusion was evaluated in the contralateral facet joint and we considered facet effusion as low intensity on T1-weighted image (WI) and high intensity on T2-WI. 18
Clinical Evaluation
Pre- and postoperative neurological status were evaluated using the Japanese Orthopaedic Association (JOA) scoring system for thoracic myelopathy, consisting of 11 points: 4 for lower motor function, 4 for sensory functions, and 3 for bladder-rectal function, if the patient had myelopathy. The recovery rate was calculated as follows: [postoperative JOA score −preoperative JOA score]/[11−preoperative JOA score]. At the final follow-up, the visual analog scale (VAS, 0-100 mm) was used to quantify neck pain, back pain, low back pain, and pain or numbness in the lower extremities. The rate of patients with VAS ≤ 34 mm in each category, which was considered to be mild symptoms of chronic musculoskeletal pain, 19 was calculated. To evaluate the HRQOL at the final follow-up, patients also completed the Oswestry disability index (ODI) and the short form 36 (SF-36). The rate of patients with ODI ≤ 22, which was considered to be an acceptable state after spine interventions, 20 was calculated. In the analysis of SF-36, we utilized a norm-based scoring (NBS) algorithm where each scale was scored to have a standardized mean (50) and standard deviation (10), relative to the general Japanese population scores.
Statistical Analysis
All statistical analyzes were performed using GraphPad Prism7 (GraphPad Software, Inc., San Diego, CA, USA). Continuous variables were reported as mean ± standard deviation (min-max) and analyzed by Wilcoxon signed-rank test for paired groups and Mann-Whitney U test for unpaired groups. The NBS of each scale in SF-36 was compared to 50 by the one-sample Wilcoxon test. The Spearman rank correlation coefficient was used to examine correlations between the pain which was quantified by the VAS, and amount of change of radiographical parameters from preoperative to the final follow up. P-values < .05 were considered statistically significant.
Results
Patient Characteristics
The patient characteristics are shown in Table 1; the mean age at surgery was 54.3 ± 13.6 years (range, 19-73 years), and mean duration of follow up was 100.5 ± 43.6 months (range, 36-190 months). In total, 13 patients (86.7%) were observed for 5 years or more, and 6 patients (40.0%) were observed for 10 years or more. At the final survey, the mean age was 62.6 ± 12.3 years (29-79 years). According to Eden’s classification, 2 patients was classified as Type 1, 2 as Type 2, 7 as Type 3, and 4 as Type 4. In total, 11 patients received hemi-laminectomy and 4 patients received conventional laminectomy.
Patient Characteristics.
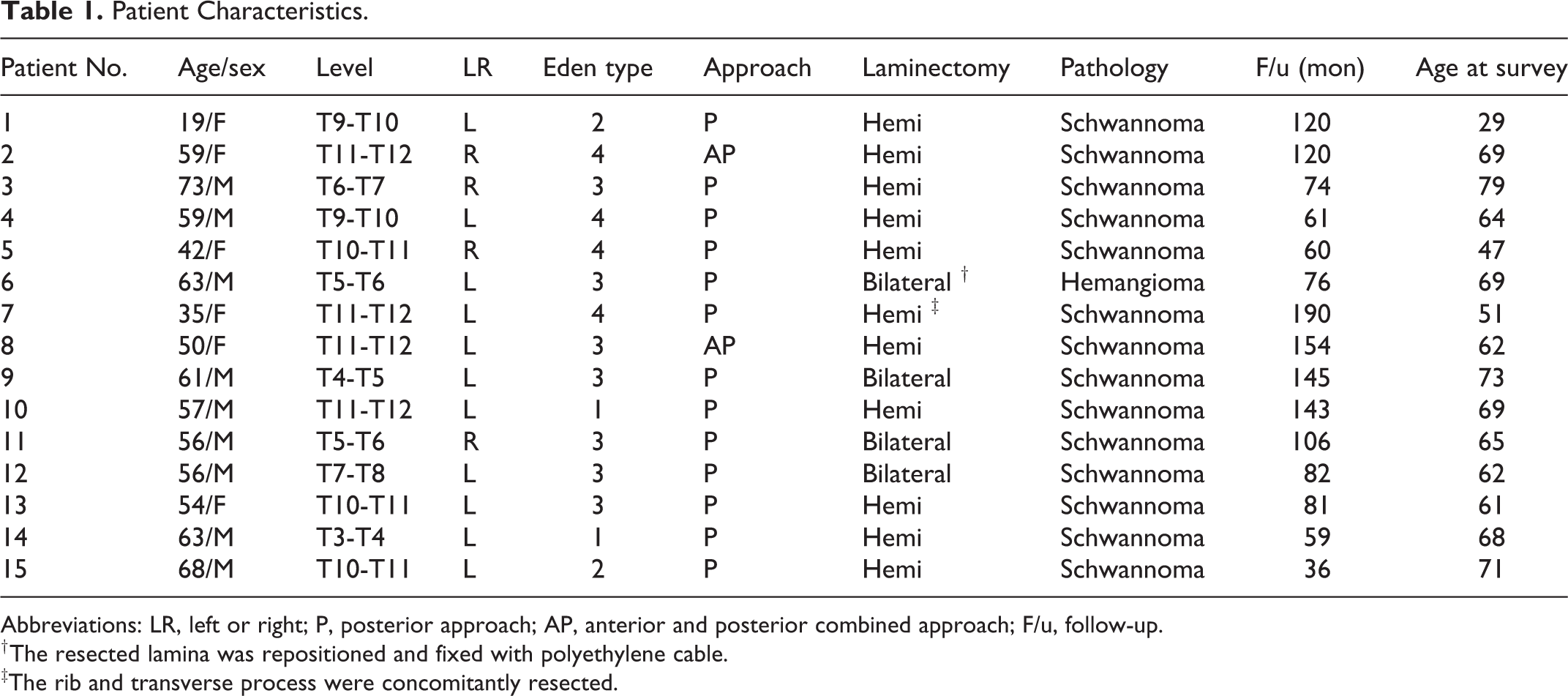
Abbreviations: LR, left or right; P, posterior approach; AP, anterior and posterior combined approach; F/u, follow-up.
† The resected lamina was repositioned and fixed with polyethylene cable.
‡The rib and transverse process were concomitantly resected.
Radiologic Evaluation
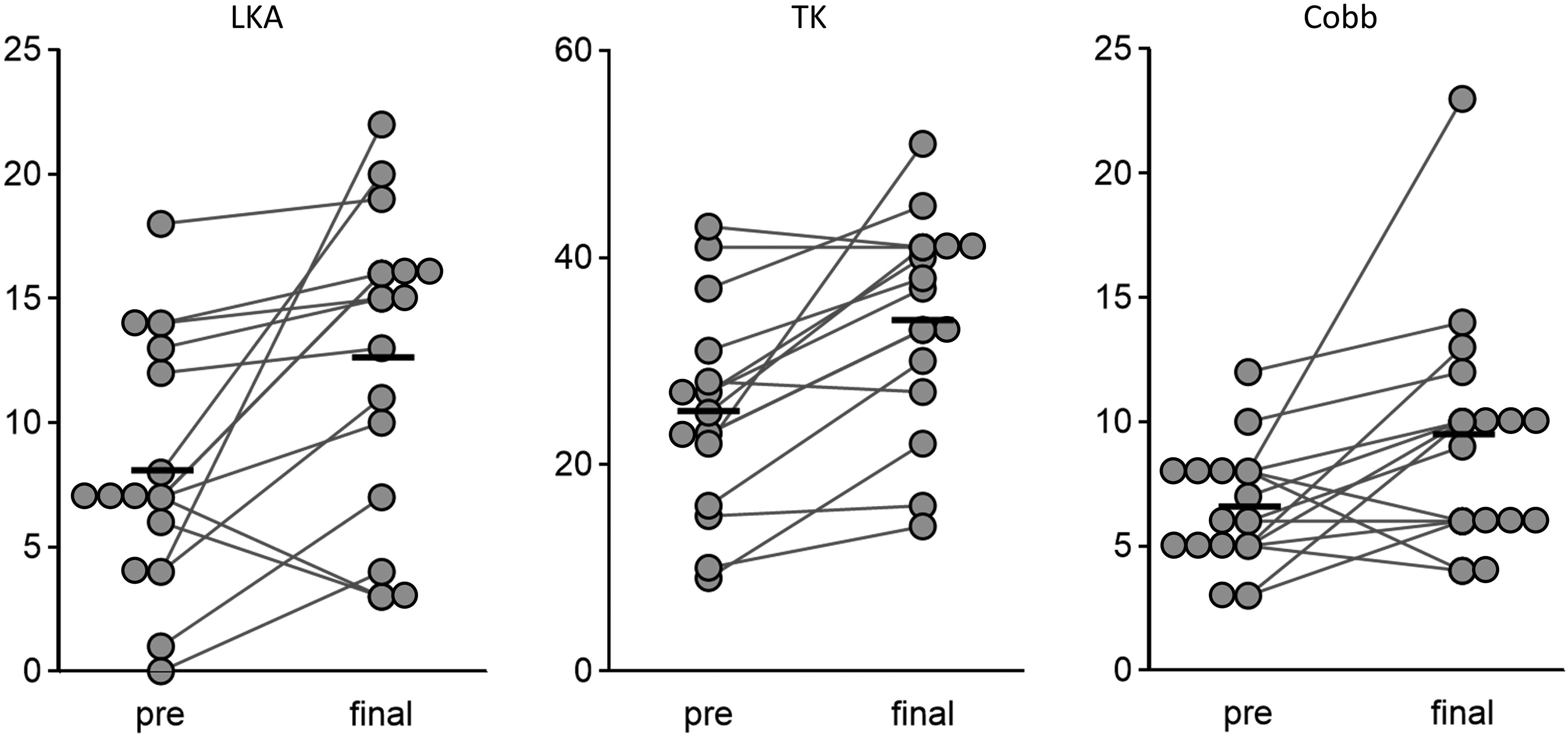
The mean values of LKA (8.1° to 12.7°, P < .01), TK (25.6° to 33.9°, P < .01), and the Cobb angle (6.6° to 9.5°, P = .02) significantly increased from the preoperative to the final follow-up visits (Figure 2), while the SWA did not change significantly (0.5° to 1.3°, P = .16). The average change from preoperative to final follow-up visit was 4.5° ± 5.8° (range, −4° to 18°) in the LKA, 8.8° ± 8.0° (range, −2° to 29°) in the TK, 2.9° ± 4.6° (range, −4° to 15°) in the Cobb angle (Figure 3). Two patients (cases 6 and 7, Figure 4) showed a change in LKA more than 10°. Furthermore, case 6 demonstrated the maximum change and value at the final examination in TK (29° and 51°, respectively), while case 7 demonstrated the maximum change and value in Cobb angle (15° and 23°, respectively) (Figures 3 and 4). Regarding the flexion-extension radiographs at the final visit, the ROM was 2.0° ± 2.1° (range, 0°-5°) and no patient had spondylolisthesis at the level of facetectomy.
Change of radiographical parameters from preoperative to final; each bar indicates mean value. LKA, local kyphosis angle; TK, thoracic kyphosis.
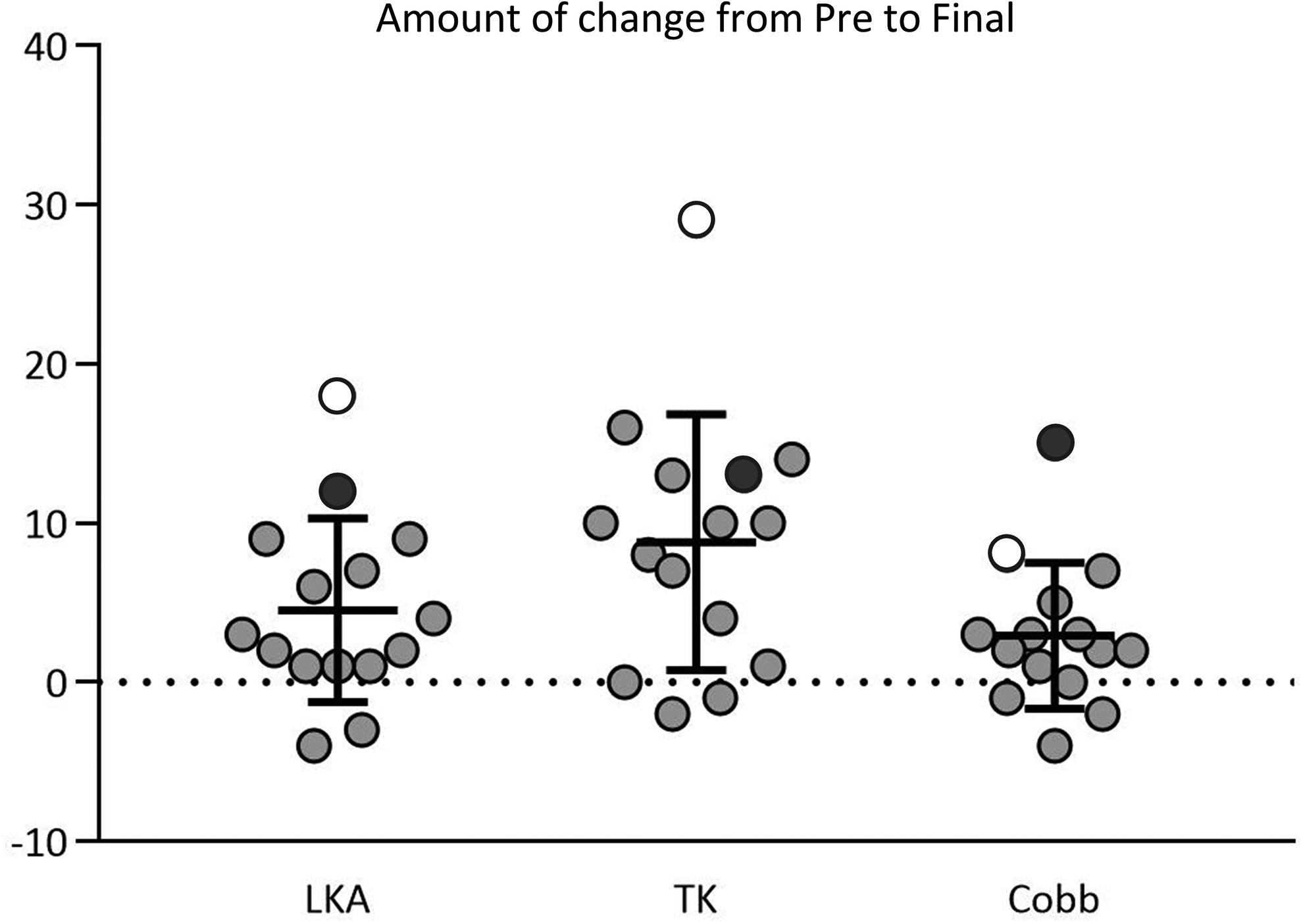
Changes in radiographical parameters from preoperative to final follow-up; bar graphs indicate mean value and standard deviation; white circles indicate the values of case 6 and black circles indicate the values of case 7. LKA, local kyphosis angle; TK, thoracic kyphosis.
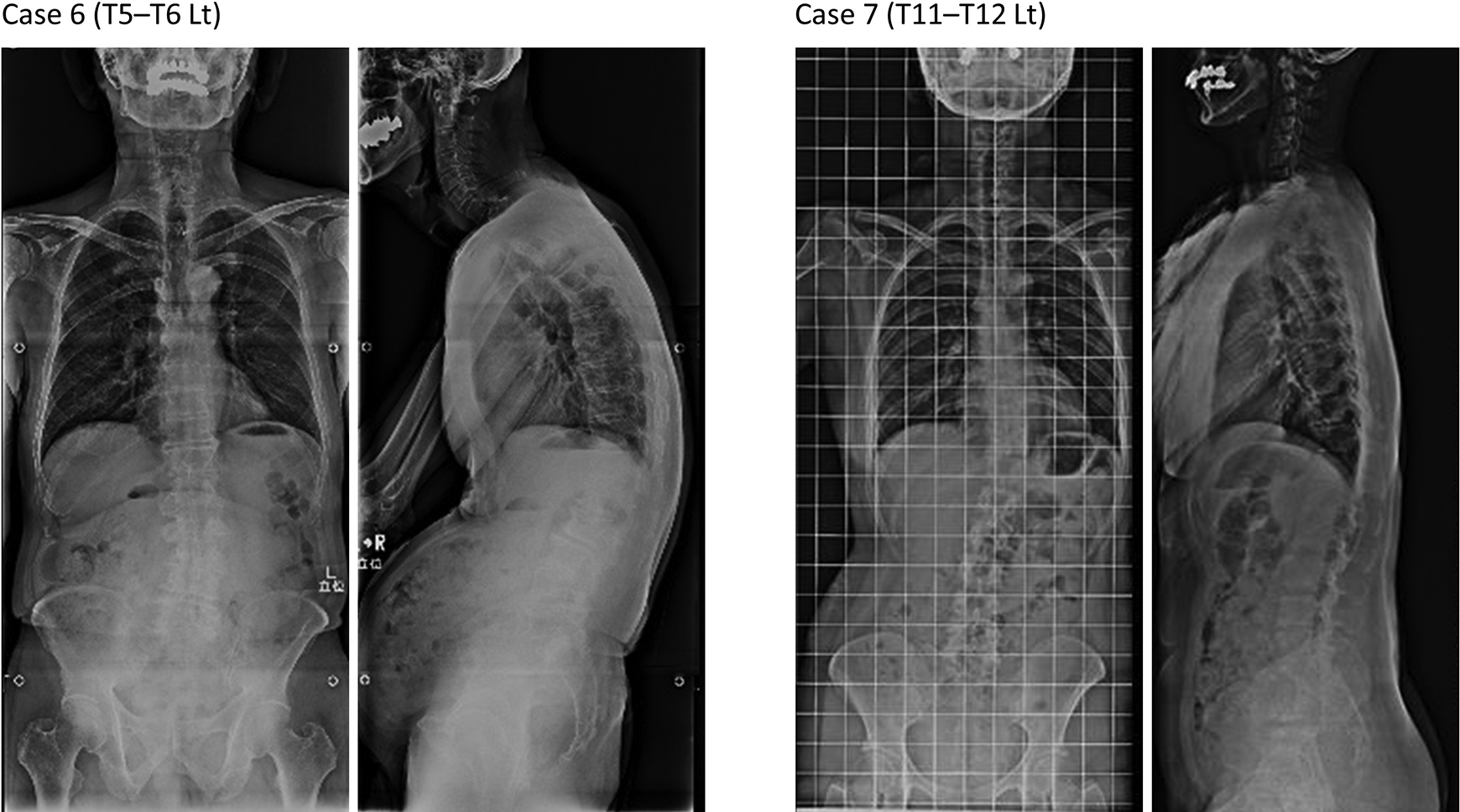
Radiographs of 2 cases who developed deformity at the final follow-up. A, Case 6 showed 29° increase in thoracic kyphosis after surgery. B, Case 7 showed 15° increase in Cobb angle after surgery.
In the evaluation of disc degeneration using MRI at the final follow-up, the Pfirrmann grade at the affected level was grade 2 in 5 patients, 3 in 8, and 4 in 2 (Table 2). Moreover, no patient had a worse grade in the affected level than those in the upper or lower levels. We observed bulging disc in 1 patient and facet effusion in 3 patients (Table 2); all of the facet effusions demonstrated thickness ≤ 1 mm.
Radiologic Evaluation.
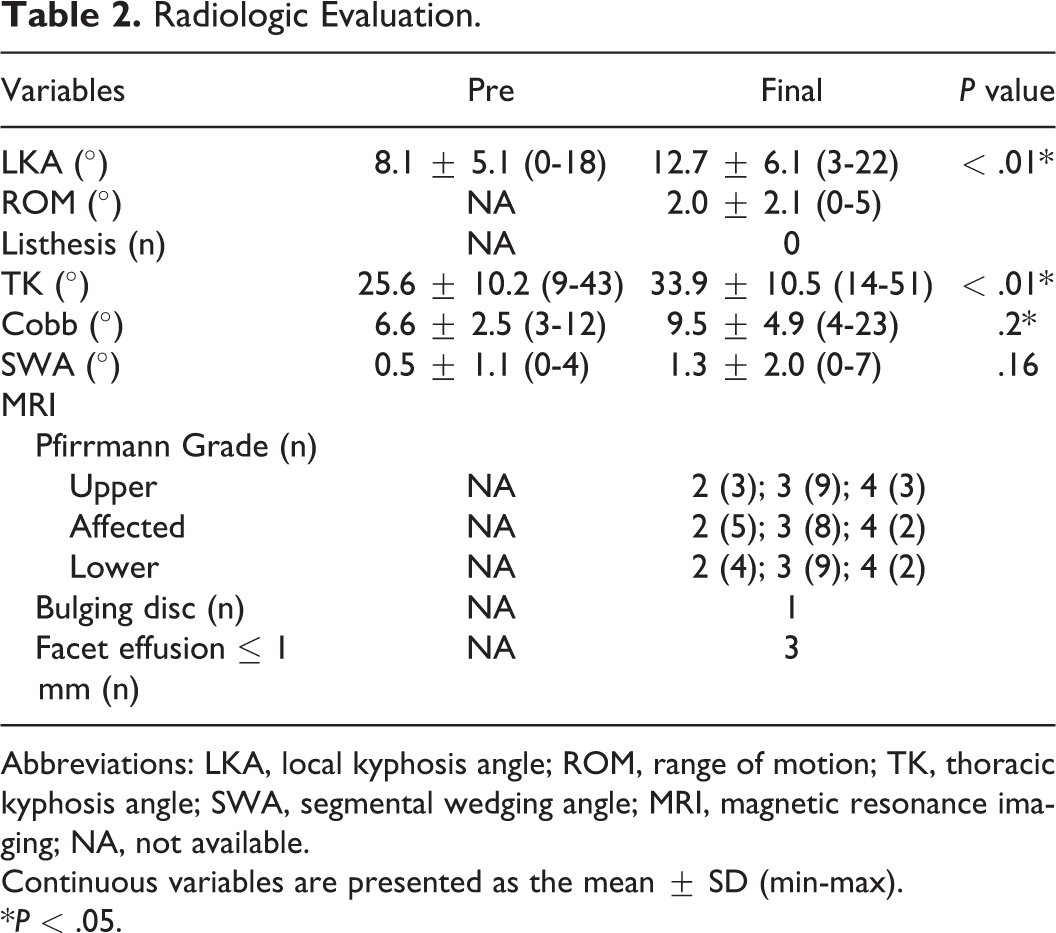
Abbreviations: LKA, local kyphosis angle; ROM, range of motion; TK, thoracic kyphosis angle; SWA, segmental wedging angle; MRI, magnetic resonance imaging; NA, not available.
Continuous variables are presented as the mean ± SD (min-max).
*P < .05.
Regarding tumor recurrence, 1 patient (case 13) presented with regrowth of the paravertebral component, which had no symptoms and did not require reoperation at 81-month postoperatively.
Clinical Evaluation
The neurological and patient-reported outcomes are shown in Table 3. The mean JOA score was significantly improved from 5.7 ± 2.6 (range, 2-10) preoperatively to 10.5 ± 0.7 (range, 9-11) at the final follow-up (P = .004). At the final follow-up visit, the rates of the patients with VAS ≤ 34 mm were 66.7% with neck pain, 93.3% with back pain, 86.7% with low back pain, 86.7% with pain or numbness in the lower extremities. Moreover, the rate of the patients with ODI ≤ 22% was 80%. The 2 patients (cases 6 and 7) who developed spinal deformity had no substantial pain or disability, except for the neck pain in case 7 (VAS = 50 mm). Regarding the SF-36 at the final follow-up, the mean NBS in the social functioning and mental health domains were significantly higher than those in the general Japanese population (P = .003, 0.04, respectively), while those in the other domains did not differ significantly between our patient group and the general Japanese population. In addition, there was no statistically significant correlation between the pain and the amount of angular change (Table 4).
Neurological Status and Patient-Reported Outcomes.
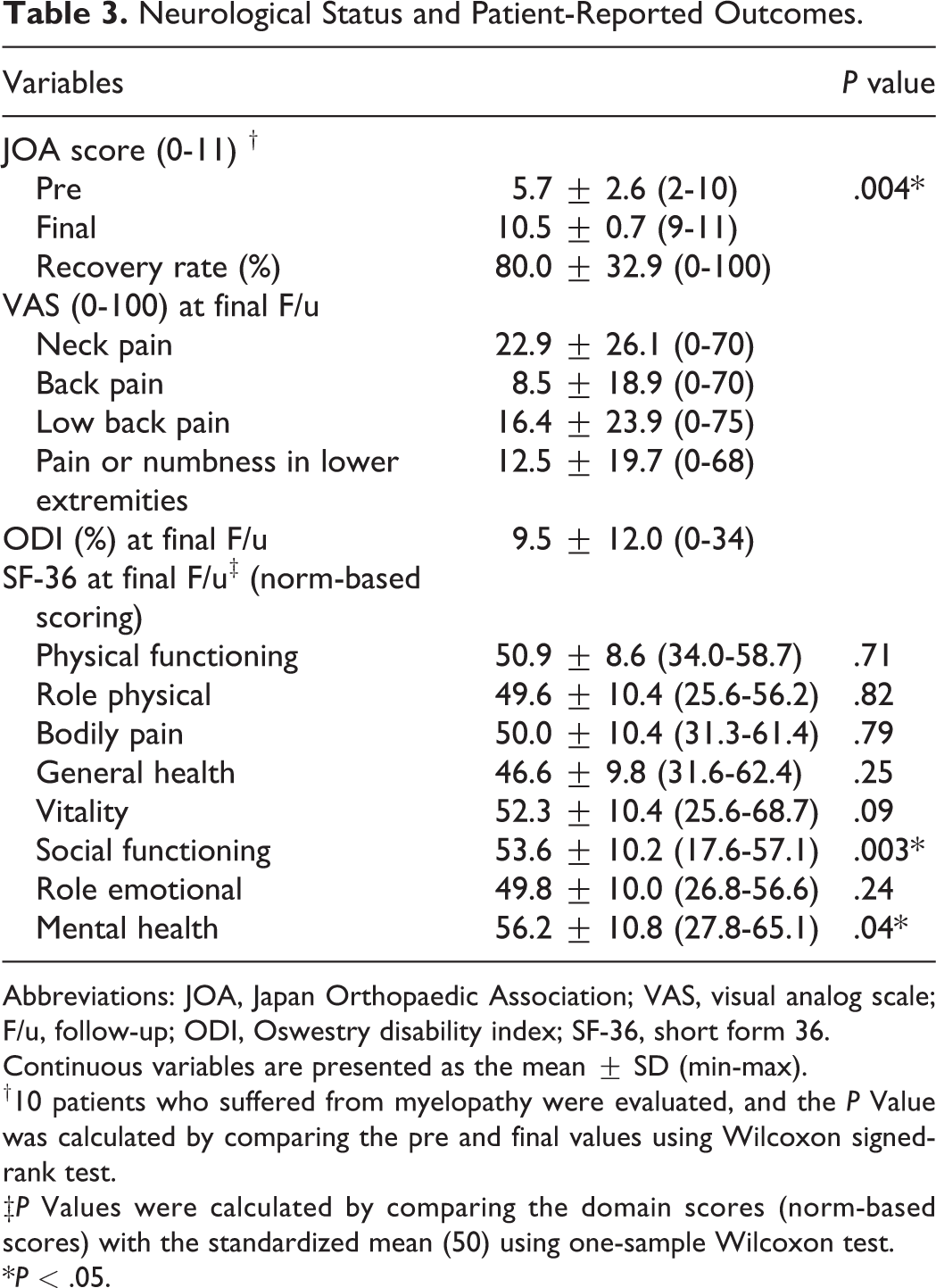
Abbreviations: JOA, Japan Orthopaedic Association; VAS, visual analog scale; F/u, follow-up; ODI, Oswestry disability index; SF-36, short form 36.
Continuous variables are presented as the mean ± SD (min-max).
†10 patients who suffered from myelopathy were evaluated, and the P Value was calculated by comparing the pre and final values using Wilcoxon signed-rank test.
‡P Values were calculated by comparing the domain scores (norm-based scores) with the standardized mean (50) using one-sample Wilcoxon test.
*P < .05.
Correlation Between Pain (VAS) and Amount of Change of Radiographical Parameters.

Abbreviations: VAS, visual analog scale; LKA, local kyphosis angle; TK, thoracic kyphosis angle; r, Spearman rank correlation coefficient.
Comparisons Between the Middle Thoracic and Thoracolumbar Tumor Groups
The comparisons of radiographic measurements between the 2 groups are shown in Table 5. The middle group included 8 patients affected at from T3-T4 to T9-T10 and thoracolumbar group included 7 patients affected at T10-T11 or T11-T12. The preoperative and final radiographic measurements, including LKA, ROM, TK, and Cobb angle, did not differ significantly between the 2 groups (P > .2 for all but TK at the final follow-up [P = .10]).
Comparisons of Radiographic Measurements Between the Middle Thoracic and Thoracolumbar Tumor Groups.
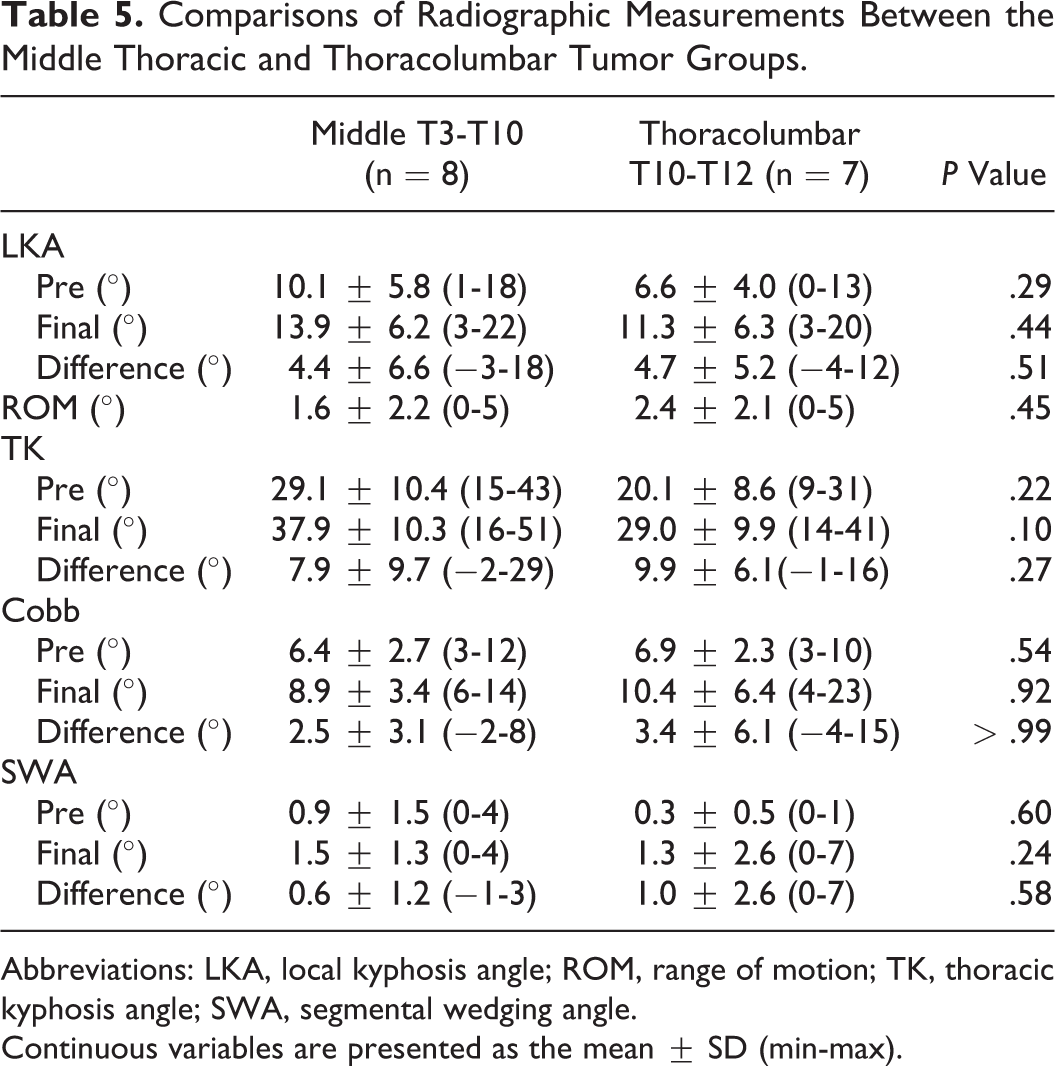
Abbreviations: LKA, local kyphosis angle; ROM, range of motion; TK, thoracic kyphosis angle; SWA, segmental wedging angle.
Continuous variables are presented as the mean ± SD (min-max).
Group comparisons of clinical outcomes are shown in Table 6. Although the preoperative JOA score was lower in the middle thoracic group than in the thoracolumbar group, the JOA score at the final follow-up showed no significant difference between the 2 groups. Moreover, there were no significant group differences in VAS, ODI, and SF-36 at the final follow-up (P > .1 for all).
Comparisons of Neurological Status and Patient-Reported Outcomes Between the Middle Thoracic and Thoracolumbar Tumor Groups.
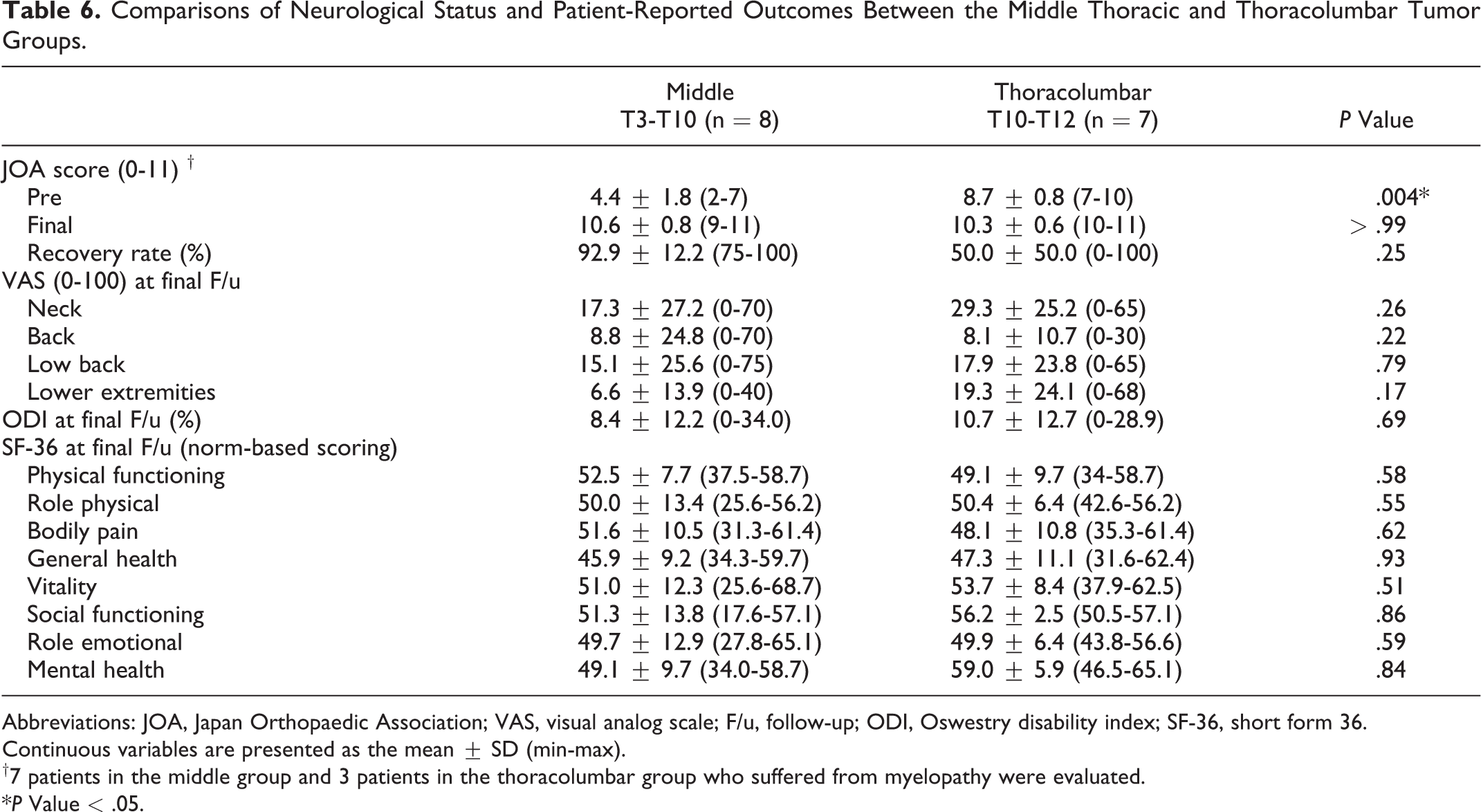
Abbreviations: JOA, Japan Orthopaedic Association; VAS, visual analog scale; F/u, follow-up; ODI, Oswestry disability index; SF-36, short form 36.
Continuous variables are presented as the mean ± SD (min-max).
†7 patients in the middle group and 3 patients in the thoracolumbar group who suffered from myelopathy were evaluated.
*P Value < .05.
Illustrative Case: Case No. 11
A 56-year-old man presented with progressive myelopathy due to a dumbbell-shaped Schwannoma at T5-T6 level (Figure 5A and B). He underwent laminectomy of T5, as well as right T5-T6 facetectomy and the tumor was totally resected (Figure 5C). His myelopathy improved from 5 points preoperatively to 11 at 9 years postoperatively (recovery rate, 100%). Postoperative spinal imaging did not demonstrate any significant progression of degeneration or instability (Figure 5E-G) compared to preoperative radiographs (Figure 5D). Moreover, at the final follow-up, the VAS was 0 mm in neck pain, 0 in back pain, 22 in low back pain, and 0 in pain or numbness of lower extremities. With regard to the SF-36, the NBS was more than 50 in all domains except Physical Functioning (48.1), Bodily Pain (49.0), and General Health (46.2).
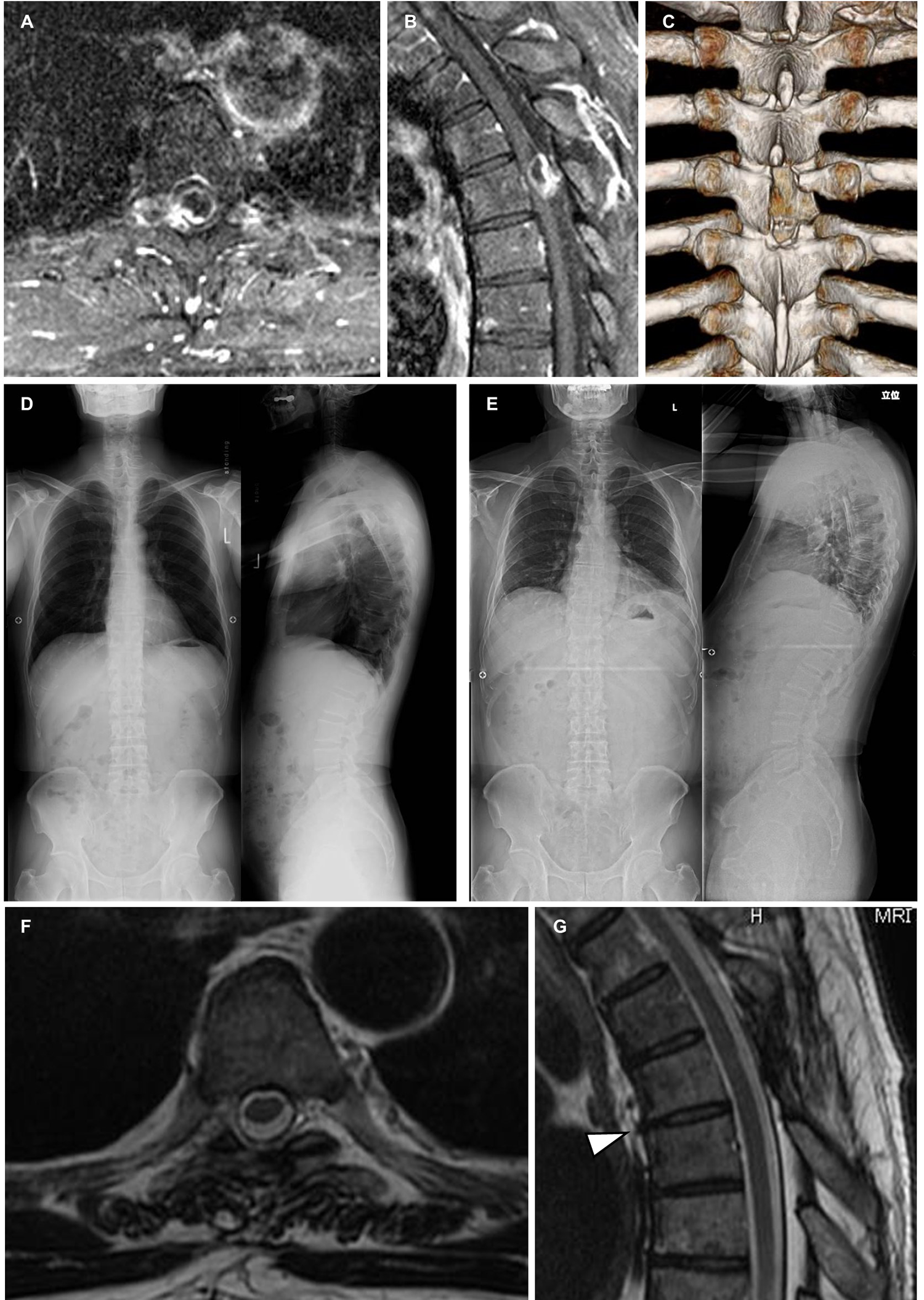
A 56-year-old man presented with progressive myelopathy demonstrated the dumbbell-shaped mass compressing spinal cord at T5-6 in his preoperative enhanced T1-weighted MR images (A, B); postoperative reconstructive 3D-CT image showed the range of laminectomy of T5 and right T5-6 facetectomy (C); standing, full-length plain radiographs did not demonstrated significant changes from preoperative (D) to at 9-year postoperatively (E) in both coronal (Cobb angle, 6° to 6°; SWA, 0° to 1°) and sagittal planes (LKA, 18° to 19°; TK, 41° to 41°); the T2-weighted MR images at the final follow-up showed neither fluid effusion in the contralateral facet joint (F) nor worse disc degeneration relative to the adjacent discs (G).
Discussion
The present study is the first to comprehensively evaluate the mid- to long-term clinical and radiological outcomes of unilateral total facetectomy without instrumented fusion for the resection of dumbbell tumors at the middle thoracic and thoracolumbar regions. The radiological and clinical outcomes, including patient-reported outcomes, were satisfactory, and no patient demonstrated instability or spinal deformity that required additional surgery. Moreover, we compared the outcomes between the middle thoracic and thoracolumbar groups, and showed no significant group difference in radiological and clinical outcomes at the final follow-up visit.
Unilateral total facetectomy with laminectomy or hemilaminectomy provides sufficient exposure of the intraspinal and intraforaminal components of dumbbell tumors, allowing surgeons to manipulate the nervous structure safely. However, since the methods may still lead to postoperative development of spinal instability or deformity, some authors have performed concomitant fusion with spinal instrumentation routinely.4,6,7,13 In addition, Ahmad et al 21 and Sebai et al 22 reported their institutional experience of spinal peripheral nerve sheath tumors, and demonstrated that total facetectomy was associated with the decision for concomitant arthrodesis. Contrastingly, some authors reported management of thoracic dumbbell tumors by laminectomy and unilateral total facetectomy without concomitant fusion, although there is limited evidence about postoperative spinal instability and/or deformity.3,5,8,9,11,14 Thorat et al 3 reported 11 patients with thoracic dumbbell tumors with a mean 20 months follow-up, consisted of 5 middle thoracic regions managed without fusion and 6 junctional regions managed with fusion. Two patients in the middle thoracic region, 1 of whom was an 11-year-old child, developed mild scoliosis but did not require additional surgery. Aizawa et al 5 reported 10 patients who underwent unilateral facetectomy and hemilaminectomy without fusion, and showed limited changes in local kyphosis angle and local scoliosis angle in plain radiographs from preoperative to mean 3.7 years postoperative. Rong et al 8 treated 14 patients and revealed no aggravating deformity or instability after a mean 32.4 months of follow-up. In addition, Ito et al 23 managed 18 patients of ventral intradural thoracic spinal tumors, although their cases did not include dumbbell tumors, and reported no significant changes in local kyphosis angle observed at a mean 32.4 months after surgery in patients who received laminectomy and one-level unilateral total facetectomy without fusion. However, these studies only evaluated the short- to mid-term outcomes of a limited number of radiographic parameters.
In the present study, we evaluated longer-term (3-15.8 years, mean 8.4 years) radiographic outcomes, which were in line with the previous studies. However, 2 patients (case 6 and 7) acquired a spinal deformity in our series. The patient in case 6 underwent T5-T6 total facetectomy with laminectomy, even though the lamina was repositioned and fixed with a polyethylene cable. He had a postoperative increase in T5-12 TK and LKA, which at the latest visit were 51° and 22°, respectively. Disruption of posterior ligaments by laminectomy, even though the lamina was recapped after the resection of the tumor, might cause postoperative kyphosis in T5-6 segments. The patient in case 7 underwent left-sided hemi-laminectomy, T11-T12 total facetectomy, and T11 costotransversectomy. She demonstrated a mild, left-convex thoracic scoliosis (Cobb = 23°), which occurred within 2 years and persisted for approximately 16-years of follow-up. In this patient, costotransversectomy might have been the cause of the thoracic scoliosis. Fortunately, both patients showed satisfactory outcomes with respect to the VAS and ODI, except for neck pain in case 7 (VAS = 50 mm), but this did not require additional surgery. We also demonstrated that unilateral total facetectomy with laminectomy or hemilaminectomy did not accelerate disc and facet joint degeneration, as evaluated by MRI. With regard to the patient-reported outcomes, VAS for pain and ODI were acceptable in ≥ 80% of the patients, except for neck pain which was acceptable in 66.7%. Moreover, health-related quality of life, as evaluated by SF-36, demonstrated comparable or better scores compared to the reference values of the normal Japanese population. These findings indicate that the mid- to long-term outcomes were radiologically and clinically stable and satisfactory, suggesting that unilateral total facetectomy with laminectomy or hemilaminectomy do not need concomitant instrumented fusion at the middle thoracic and thoracolumbar regions in the initial operation.
Our findings are supported by biomechanical studies of the thoracic spine. The stability of the thoracic spine is supplemented by connection to the ribs and sternum.24-26 Moreover, the intervertebral discs serve as more important stabilizers than the facet in the thoracic spine.27,28 In this context, Healy et al 29 and Lubelski et al 30 performed sequential unilateral decompression (laminectomy, facetectomy, and costotransversectomy, at T4-T5 and T8-T9, respectively) and revealed no significant change in motion.
Another issue we should consider is that the involvement of the thoracolumbar region may be still associated with the need for concomitant instrumented fusion. Indeed, some authors altered their management between the middle thoracic and thoracolumbar spine.3,14 However, our results showed comparable outcomes in the thoracolumbar group to those in the middle thoracic group, suggesting that instrumented fusion is not mandatory, even for patients with dumbbell tumors at the thoracolumbar region.
The limitations of the current study include its small sample size, retrospective study design, and a lack of data from patients aged ≤18 years and from a control group treated with instrumented fusion. Due to the retrospective nature of our study, we lack preoperative information regarding the VAS, ODI and SF-36. In addition, we could not evaluate disc degeneration using preoperative MRI due to the differences in imaging conditions and technology. Our study excluded child patients who may be susceptible to laminectomy and radiation therapy and develop spinal deformity. 31 Moreover, there were no patients with dumbbell tumors at the cervicothoracic junction, which has been reported to be highly associated with the need for concomitant spinal fusion.22,32 We also excluded patients who had preexisting severe deformities or those who required concomitant instrumented fusion at the index surgery due to destructive changes in the thoracic spine.
In our study, 2 patients developed deformity at the final follow-up. Because of a lack of healthy controls, small sample size, and the large standard deviation of the data, we acknowledge that it might be insufficient to reach a clear conclusion whether the deformity was a normal evolution with age or an iatrogenic consequence. Nevertheless, because of the rarity of thoracic dumbbell tumors, we believe our findings provide meaningful evidence to decide surgical procedures and their impacts on mid- to long-term radiological and clinical outcomes.
Conclusion
In unilateral total facetectomy with laminectomy or hemilaminectomy to manage dumbbell tumors in the middle thoracic and thoracolumbar region, concomitant instrumented fusion is unnecessary at the initial surgery in patients without severe preexisting deformity or destructive changes of the spinal column.
Footnotes
Authors’ Note
The present study was performed in accordance with bioethics standard of each institutional ethics committee written below. The Ethics Committee of Niigata University; number 2664. Independent Ethics Committee of Tohoku University School of Medicine; 2017-1-235. The Ethics Committee of Yamagata University; 2017-137. All participants of our study provided written informed consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.