
Abstract
Study Design:
A biomechanical study.
Objectives:
The purpose of this study was to investigate the effects of cruciform and square incisions of annulus fibrosus (AF) on the mechanical stability of bovine intervertebral disc (IVD) in multiple degrees of freedom.
Methods:
Eight bovine caudal IVD motion segments (bone-disc-bone) were obtained from the local abattoir. Cruciform and square incisions were made at the right side of the specimen’s annulus using a surgical scalpel. Biomechanical testing of three-dimensional 6 degrees of freedom was then performed on the bovine caudal motion segments using the mechanical testing and simulation (MTS) machine. Force, displacement, torque and angle were recorded synchronously by the MTS system. P value <.05 was considered statistically significant.
Results:
Cruciform and square incisions of the AF reduced both axial compressive and torsional stiffness of the IVD and were significantly lower than those of the intact specimens (P < .01). Left-side axial torsional stiffness of the cruciform incision was significantly higher than a square incision (P < .01). Neither incision methods impacted flexional-extensional stiffness or lateral-bending stiffness.
Conclusions:
The cruciform and square incisions of the AF obviously reduced axial compression and axial rotation, but they did not change the flexion-extension and lateral-bending stiffness of the bovine caudal IVD. This mechanical study will be meaningful for the development of new approaches to AF repair and the rehabilitation of the patients after receiving discectomy.
Introduction
The tightly arranged structure of the annular fibrosus (AF) resists the tension and tensile strain generated by the spine during the bending and rotation process, as well as the circumferential stress generated by the nucleus pulposus (NP) during compression of the intervertebral disc (IVD).1,2 When AF defects occur, the IVD will asymmetrically produce moments during rotation and bending while having an unstable connection with the upper and lower vertebral bodies. 3 Additionally, defects in the AF cannot completely resist the circumferential stress generated by the NP, which can protrude and impinge the nerve roots, leading to the neurological symptoms. 4 In clinics, the discectomy technique is frequently used for the treatment of IVD herniation. With this technique, some of the AF and the prolapsed NP tissue are removed to relieve the mechanical compression of the nerve roots; after surgery, however, the incision of the AF is left without further treatments.5-7 Undoubtedly, defects in the AF will impair the stability of IVD, and there are several speculations of why this may occur.
It has been determined that bending and compressive stiffnesses, as well as bending moments induced by axial compression, were not changed by a vertical incision to the lateral side of the IVD or a horizontal incision to the anterior side of the distal vertebral rim. 3 Nevertheless, it was indicated that most IVD injuries, such as rim lesions, mid-plane tears, circumferential tears, radial lesions, and puncture injuries, had specific and sensitive effects on IVD biomechanics. 8 Thus, at present, the influence of different AF defect patterns on the biomechanical stability of the IVD is still controversial. 9
Hence, the aim of this study is to investigate the effects of cruciform and square incisions on the mechanical stability of the bovine IVD. This study will extend our understanding regarding the relationship between AF defect patterns and IVD stability and provide a mechanically useful model for the development of biomaterial-based AF repair approaches.
Materials and methods
Animals
All experimental protocols of this study were approved by the experimental animal welfare ethics committee of Shenzhen Peking University-Hong Kong University of Science and Technology Medical Center. The 8 bovine caudal IVD motion segments (bone-disc-bone) (Figure 1A) used in this study were obtained from the local abattoir.
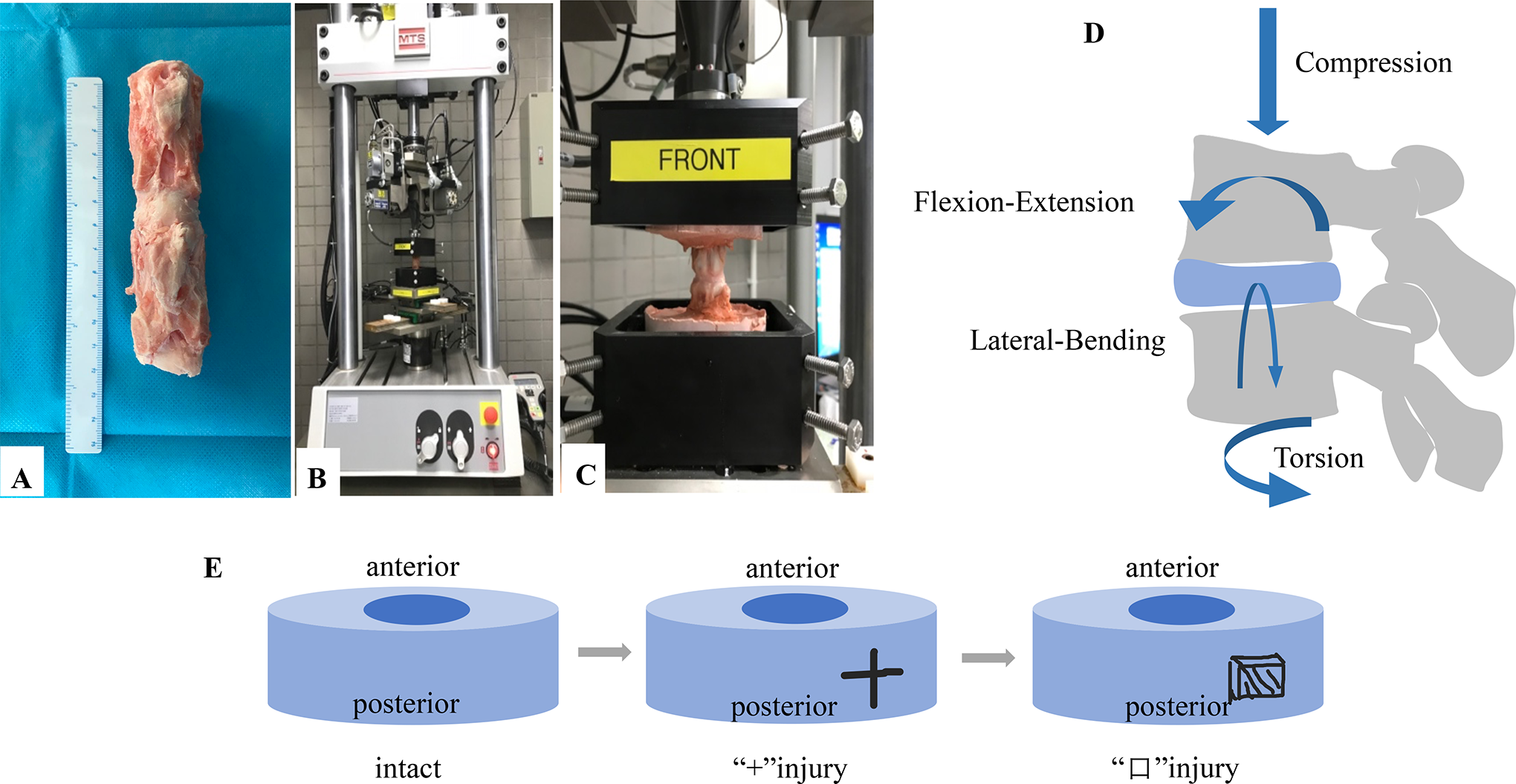
Experimental methodology A: Bovine caudal IVD motion segments (bone-disc-bone). B, C: Specimens potted with Denture powder fixed on the MTS machine. D: The specimens were subjected to a biomechanical testing process, followed by axial compression testing, axial rotation testing, flexion-extension testing, and lateral-bending testing. E: Intact annulus fibrosus, a cruciform incision to the right side of the disc, and a square incision of the disc.
Specimen Preparation
After removal of the surrounding muscle and ligaments, the IVD from the tail was sawed off, leaving the caudal vertebrae discs C2 to C3 and C4 to C5 as the motion segments. Before the experiment, the specimens were examined by X-ray to exclude tumors, inflammations, trauma, and anatomical variations. None of the specimens was excluded. The specimen was then wrapped in saline-soaked gauze, sealed in a double-layer plastic bag, and stored in a -20 Celsius (C) refrigerator. Before testing, the specimens were left to thaw gradually to room temperature and then potted in steel cubic containers filled with Denture powder. After the experiment, the specimens were examined by X-ray to confirm that all specimens were firmly fixed with Denture powder without loosening.
Biomechanical Testing
Biomechanical testing was performed on the specimen using a biomechanical torsion material testing machine (MTS Bionix with Spine Simulator, MTS, Eden Prairie, Minnesota, USA) (Figure 1B-C). Following the suggestion from the previous study, the specimen was given a 30-minute preload before testing with 100 Newtons (N) of compressive force at 0.1 Hertz (Hz) to reduce the adhesion of the specimens. 10 Immediately after preloading, the following mechanical tests were performed on the intact specimens in turn (Figure 1D): (1) axial compression at 0-0.5 mm; (2) axial torsion at ± 5°; (3) flexion-extension at ± 1°; and (4) lateral bending at ± 2°. All tests were conducted for 15 cycles at a rate of 0.1 Hz, with the 12th cycle used for further biomechanical analysis. After the intact specimens test was completed, we used a surgical scalpel to make a cruciform incision (Figure 1E) with a transverse length of 0.8 mm and a longitudinal length of 0.5 mm at the right side of the specimen’s AF. We then performed the second round of biomechanical testing. After the second round of mechanical testing was completed, we used a surgical scalpel to make a square incision of 0.8 × 0.5 × 0.5 mm on the original incision to remove part of the AF. We then performed the third round of biomechanical testing. Force, displacement, torque, and angle were recorded synchronously by the built-in sensor on the dedicated MTS computer. The specimen reverted to its original state after each test. During testing, the specimens were sprayed with physiological saline regularly to keep them moist.
Axial compression stiffness was calculated as the axial maximum compression force divided by the axial maximum displacement; torsional stiffness was calculated as the maximum torque divided by the maximum rotation angle. The stiffness values of the intact group were standardized, and the measured values of the other groups were converted into percentages of the intact group for comparison, as described in previous research.11-13
Statistical Analysis
Statistical analysis was performed using SPSS 16.0 software. All data was calculated as a mean ± standard deviation. Two-way analysis of variance (ANOVA) with the least significant difference method (LSD) post-hoc analysis was used for statistical analysis of the data. P values <.05 were considered statistically significant.
Results
Defects in the AF Reduce the Axial Compressive Stiffness of the IVD
The axial compressive stiffness value were (175.78 ± 109.37) N/mm, (70.46 ± 104.62) N/mm and (38.45 ± 84.02) N/mm in the intact specimens, cruciform incision specimens and square incision specimens, respectively, which was significantly lower in cruciform and square incisions specimens than that in the intact specimens (intact specimens vs. cruciform incision specimens, P < .01; intact specimens vs. square incision specimens, P < .01; cruciform incision specimens vs. square incision specimens, P > .05; Figure 2A-B).
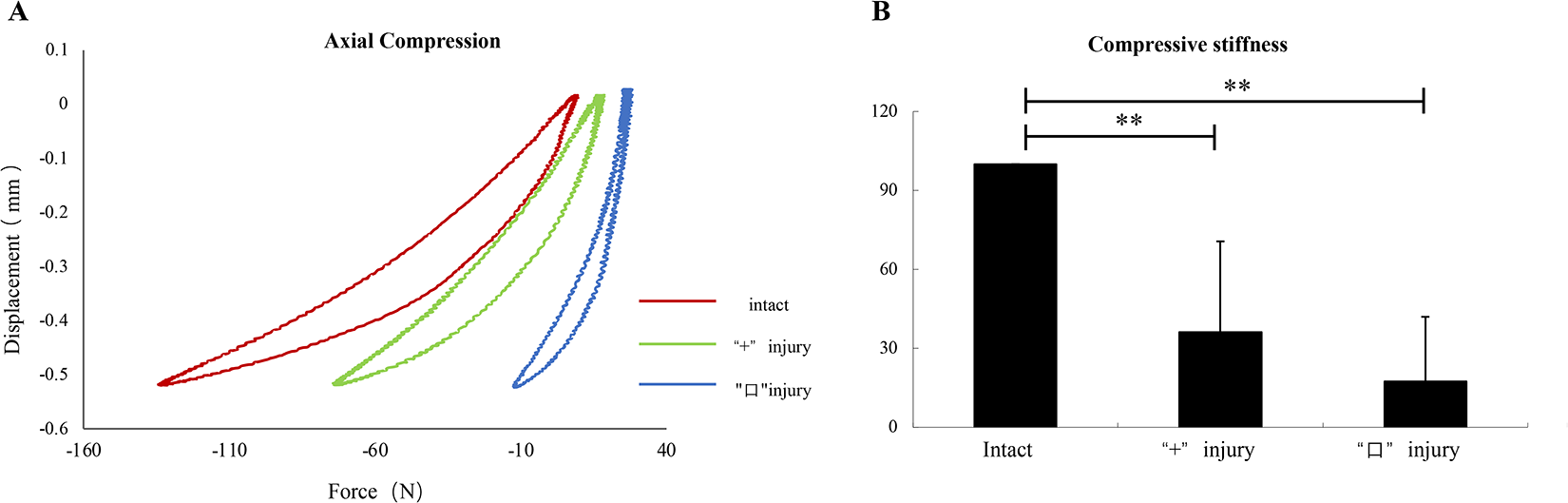
A: Axial compression--displacement curves. B: Histogram showing the mean values and standard deviations of compressive stiffness for the different incision of annulus fibrosus: intact, cruciform incision, square incision. **P < .01
Defects in the AF Reduce the Axial Torsional Stiffness of the IVD
The left-side axial torsional stiffness value were (400.91 ± 180.05) N·mm/deg, (346.28 ± 151.21) N·mm/deg and (276.80 ± 112.71) N·mm/deg in the intact specimens, cruciform incision specimens and square incision specimens, respectively, which was significantly lower in cruciform and square incisions specimens than that in the intact specimens (intact specimens vs. cruciform incision specimens, P < .01; intact specimens vs. square incision specimens, P < .01; cruciform incision specimens vs. square incision specimens, P < .01; Figure 3A-B).
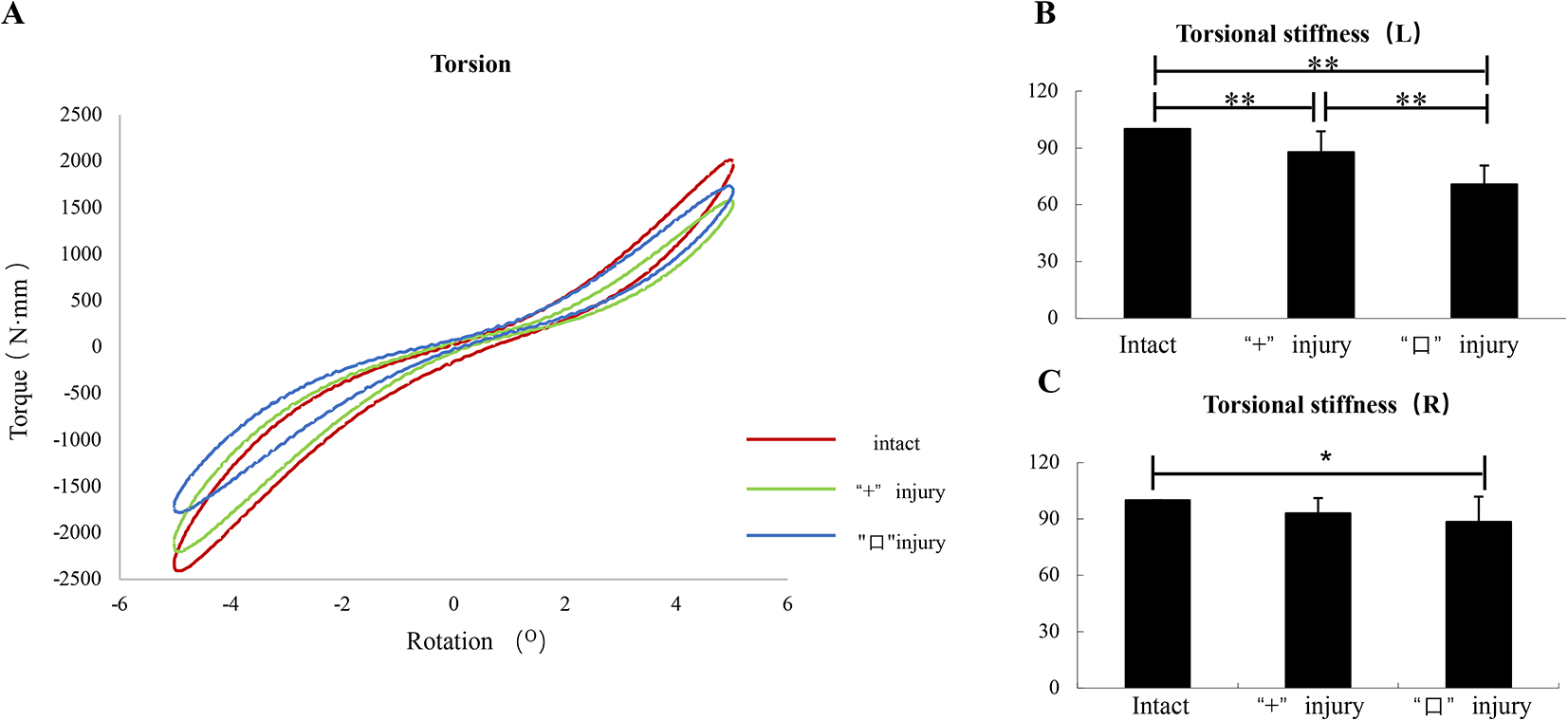
A: Axial torque-rotation curves. B/C: Histogram showing the mean values and standard deviations of torsional stiffness for the different incision of annulus fibrosus: intact, cruciform incision, square incision. **P < .01; *P < .05
The right-side axial torsional stiffness value were (328.87 ± 148.22) N·mm/deg, (301.03 ± 129.24) N·mm/deg and (276.97 ± 91.31) N·mm/deg in the intact specimens, cruciform incision specimens and square incision specimens, respectively, which was significantly lower in square incisions specimens than that in the intact specimens (intact specimens vs. cruciform incision specimens, P > .05; intact specimens vs. square incision specimens, P < .05; cruciform incision specimens vs. square incision specimens, P > .05; Figure 3C).
Defects in the AF do not Reduce the Flexional-Extensional Stiffness and Lateral-Bending Stiffness of the IVD
The flexional stiffness value were (8670.92 ± 3793.24) N·mm/deg, (8515.91 ± 3902.62) N·mm/deg and (8402.73 ± 3887.99) N·mm/deg in the intact specimens, cruciform incision specimens and square incision specimens, respectively. The extensional stiffness value were (7330.64 ± 2647.04) N·mm/deg, (7008.91 ± 2231.06) N·mm/deg and (6753.52 ± 2352.71) N·mm/deg in the intact specimens, cruciform incision specimens and square incision specimens, respectively. The left-side lateral-bending stiffness value were (9439.28 ± 9119.19) N·mm/deg, (9363.38 ± 9033.81) N·mm/deg and (9098.31 ± 8735.60) N·mm/deg in the intact specimens, cruciform incision specimens and square incision specimens, respectively. The right-side lateral-bending stiffness value were (9096.12 ± 8950.59) N·mm/deg, (9135.97 ± 8950.59) N· mm/deg and (8578.87 ± 8323.85) N·mm/deg in the intact specimens, cruciform incision specimens and square incision specimens, respectively. The flexional-extensional stiffness and lateral-bending stiffness of the IVD between different incisions and in the intact AF did not change significantly. No statistical difference was found between the intact specimens and the cruciform incision and square incision specimens in the flexional-extensional stiffness or lateral-bending stiffness (Figure 4A-C and Figure 5A-C).
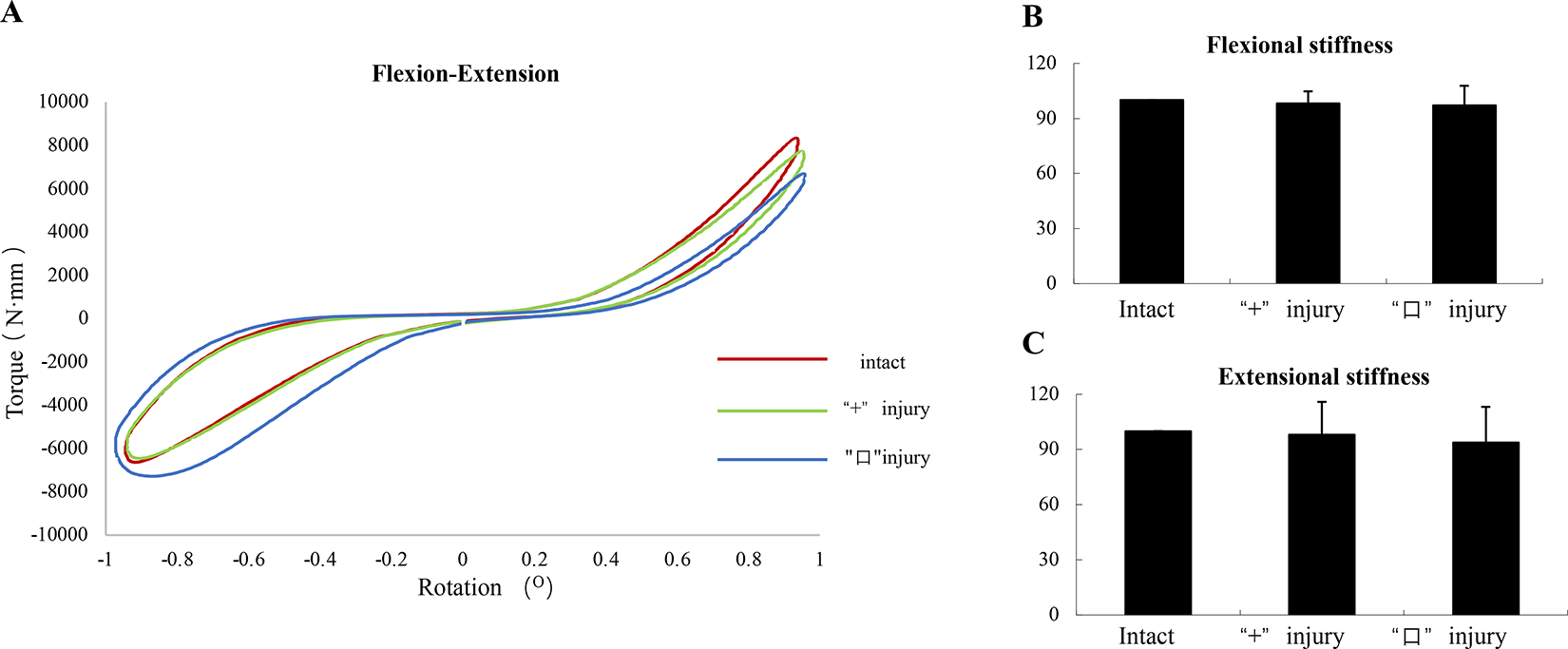
A: Flexion-Extension curves. B/C: Histogram showing the mean values and standard deviations of Flexional-Extensional stiffness for the different incision of annulus fibrosus: intact, cruciform incision, square incision. *P < .05
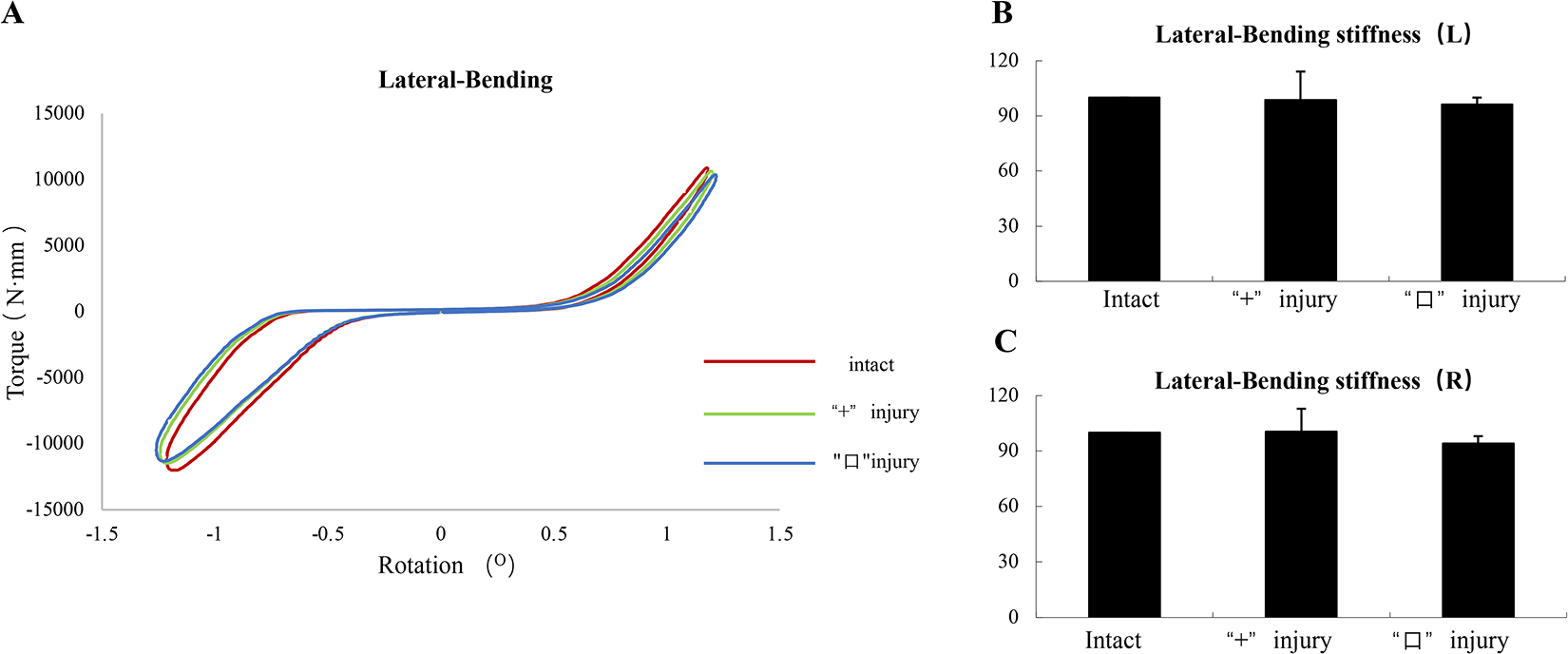
A: Lateral-Bending curves. B/C: Histogram showing the mean values and standard deviations of Lateral-Bending stiffness for the different incision of annulus fibrosus: intact, cruciform incision, square incision. *P < .05
Discussion
The discectomy is the main treatment for IVD herniation; after discectomy, the incision of the AF is often left without further treatments. 7 Previous studies showed that performing a nucleotomy or discectomy, did not lower the re-herniation rate. 14 Another studies reported a re-operation rate of 21%, when the defect in the AF is larger than 6 mm. 5 This suggests that the recurrence of postoperative disc herniation may be related to the patterns of AF incision type, and the postoperative spinal movement mode which may have an impact on the spinal biomechanics. In this regard, this study was conducted to investigate the effects of two incisions on the mechanical stability of the IVD.
The major findings of this study were that the cruciform and square incisions of the AF were able to reduce the axial compression and torsional stiffness of the IVDs, indicating that the elasticity of the IVDs has decreased and the function of the IVDs has deteriorated. It was suggested that axial torsion impair the components of the intralamellar matrix, thus making the IVD more susceptible to herniation. 15 Previous study showed that the AF played the most important role in transferring load and absorbing energy in the IVD at high strain rates. 16 According to the results of this study, the following useful suggestions could be provided for patients after lumbar discectomy surgery: the patients should reduce weight-loading on the lumbar spine and reduce axial rotational movements, especially the rotational movement that moves in the opposite direction from the AF incision.
Additionally, it was determined that AF defects could reduce the axial torsional stiffness of IVD and that the torsional stiffness of the intact side decreased more than that of the incision side. This was similar to previous study, in which it was shown that axial torsional stiffness under resting compressive load was the parameter most sensitive to large annular injury. 3 The obvious reduction of left torsional stiffness may be due to the reduction of viscoelasticity in the right IVD after the incisions in the right AF, resulting in the spinal segment failing to return to the neutral position after the left axial rotation.
In this study, the latest biomechanical torsion material testing machine was used, which completely simulated the three-dimensional and six-degrees-of-freedom motion of the spine. Nevertheless, in this study, there are several limitations we should acknowledge. First, bovine caudal IVDs were used in this experiment, although several studies have noted that the mechanical performance and elastic modulus of bovine caudal IVDs and human lumbar IVDs are quite similar.17-21 Second, the real-time range of motion of the IVD and the mechanical changes in different regions of the IVD were not measured during testing. Last, but not least, it would be ideal to perform a histological examination of the IVDs to observe the histological changes in the AF, endplate and NP after the biomechanical testing.
Conclusion
The AF defects with cruciform and square incisions were able to reduce the mechanical stability of the axial compression and axial rotation of the IVD, but they had negative effects on the flexion-extension and lateral-bending of the IVD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (No.81 702 171), the Shenzhen Double Chain Project for Innovation and Development Industry supported by the Bureau of Industry and Information Technology of Shenzhen (No.201 806 081 018 272 960) and the Shenzhen Science and Technology Innovation Committee Projects (No. JCYJ20190809182213535).