
Abstract
Study Design:
Review article.
Objectives:
There have been substantial increases in the utilization of complex spinal surgery in the last 20 years. Spinal instrumented surgery is associated with high costs as well as significant variation in approach and care. The objective of this manuscript is to identify and review drivers of instrumented spine surgery cost and explain how surgeons can reduce costs without compromising outcome.
Methods:
A literature search was conducted using PubMed. The literature review returned 217 citations. 27 publications were found to meet the inclusion criteria. The relevant literature on drivers of spine instrumented surgery cost is reviewed.
Results:
The drivers of cost in instrumented spine surgery are varied and include implant costs, complications, readmissions, facility-based costs, surgeon-driven preferences, and patient comorbidities. Each major cost driver represents an opportunity for potential reductions in cost. With high resource utilization and often uncertain outcomes, spinal surgery has been heavily scrutinized by payers and hospital systems, with efforts to reduce costs and standardize surgical approach and care pathways.
Conclusions:
Education about cost and commitment to standardization would be useful strategies to reduce cost without compromising patient-reported outcomes after instrumented spinal fusion.
Introduction
Spinal surgery is associated with high costs as well as significant variation in approach and care. There have been substantial increases in the utilization of complex spinal surgery in the last 20 years. 1 The drivers of cost in instrumented spine surgery are varied and include implant costs, complications, readmissions, facility-based costs, surgeon-driven preferences, and patient comorbidities. 2 -8 Each major cost driver represents an opportunity for potential reductions in cost. With high resource utilization and often uncertain outcomes, spinal surgery has been heavily scrutinized by payers and hospital systems, with efforts to reduce costs and standardize surgical approach and care pathways. It is incumbent upon surgeons to ensure that efforts be made to reduce cost without compromising patient-reported outcomes. The aim of this manuscript is to review the current literature on drivers of instrumented spine surgery costs and describe selected strategies for cost reduction without compromising outcome.
Methods
Literature Search
A comprehensive literature search was performed using PUBMED/Medline for all articles published from 2000 to 2020 using the MeSH and keyword term: (“Health Care Costs”[Mesh]) AND “Spinal Fusion”[Mesh] NOT ((scoliosis) OR (“deformity”) OR (“trauma”)) with keywords: (“Cost driver*”) AND ((“Spin*”) OR (“spinal Fusion”)). Inclusion criteria included all articles in the English language, published after the year 2000, and those that covered drivers of cost in spine fusion surgery. We excluded articles that were published in a different language other than English, publications involving cost comparison of different surgical approaches (i.e. MIS vs. open TLIF, arthroplasty vs. fusion), abstracts, and cost of spine surgery outside the United States. Other exclusion criteria included cost publications related to spine trauma, spine deformity, spine oncology, non-instrumented spine surgery, and articles that combined fusion costs with decompression only costs. Pertinent articles were manually selected, reviewed, and extracted for review. The articles that were selected focus mainly on cost drivers of instrumented lumbar and cervical surgeries.
Results
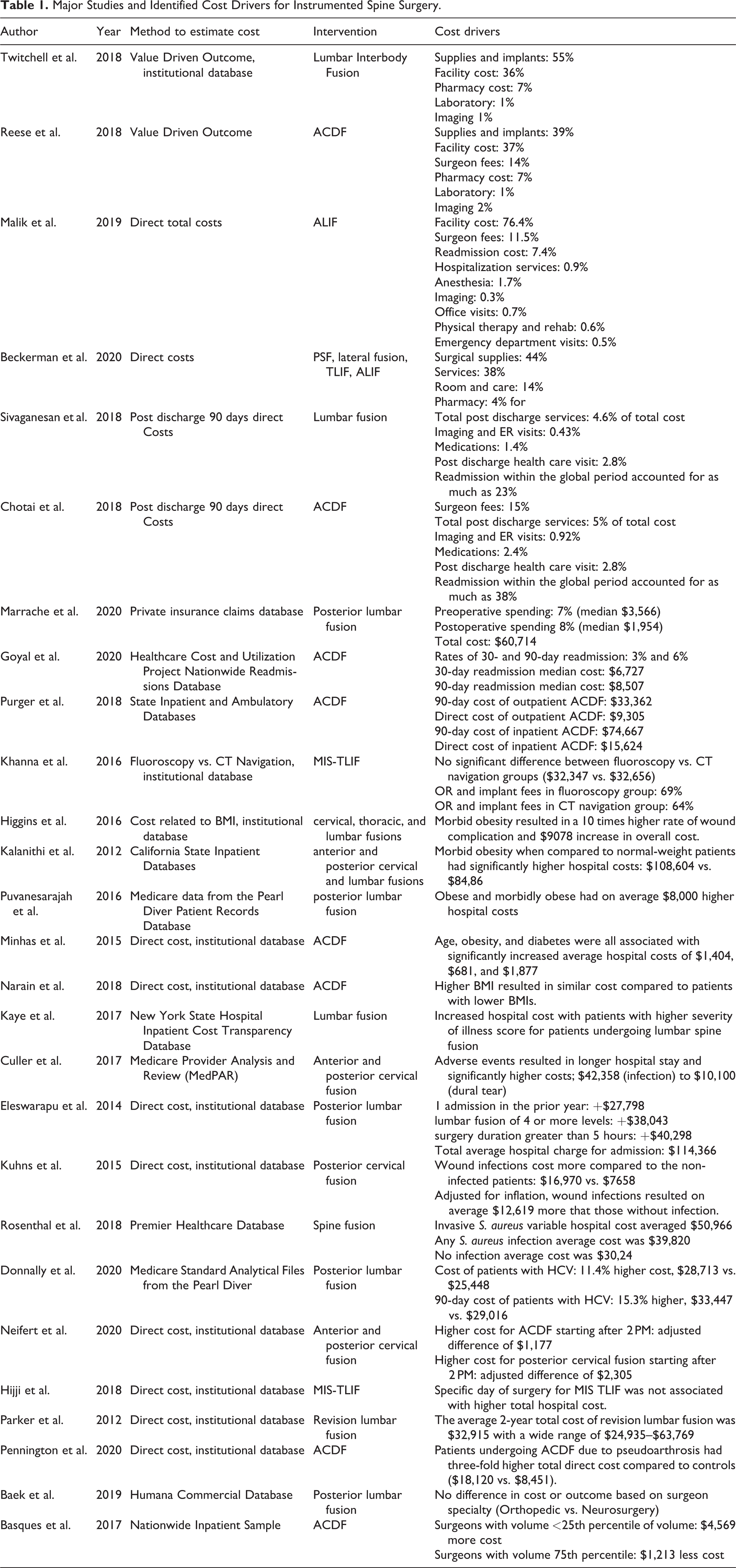
The search using the keywords and MeSH terms yield a total of 217 publications. Based on our inclusion and exclusion criteria, we were able to narrow the search to a total of 27 articles (Figure 1). The reasons for excluding studies from further analysis are outlined in Figure 1. The articles were published between the years of 2012-2020. 59% of the articles were published between 2018-2020. The articles utilized either an internal database or a registry to evaluate cost related to spine fusions. 8 studies were on ACDF (Anterior cervical discectomy and fusion), 1 study on posterior cervical fusion, 2 studies on ACDF and posterior cervical fusion, 9 studies on posterior lumbar fusion, 1 study on anterior lumbar interbody fusion (ALIF), 4 studies on spine fusion, and 2 studies on minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF). Drivers of costs were identified in the literature as they relate to hospital costs during the index surgery and the subsequent 90-day period, patient related cost drivers, timing factors, surgeon factors, readmission, revision surgery, and infections. The hospital costs include facility costs, supplies and implants, pharmacy costs, imaging and laboratory, surgeon fees, and post discharge 90-day costs. (Table 1)
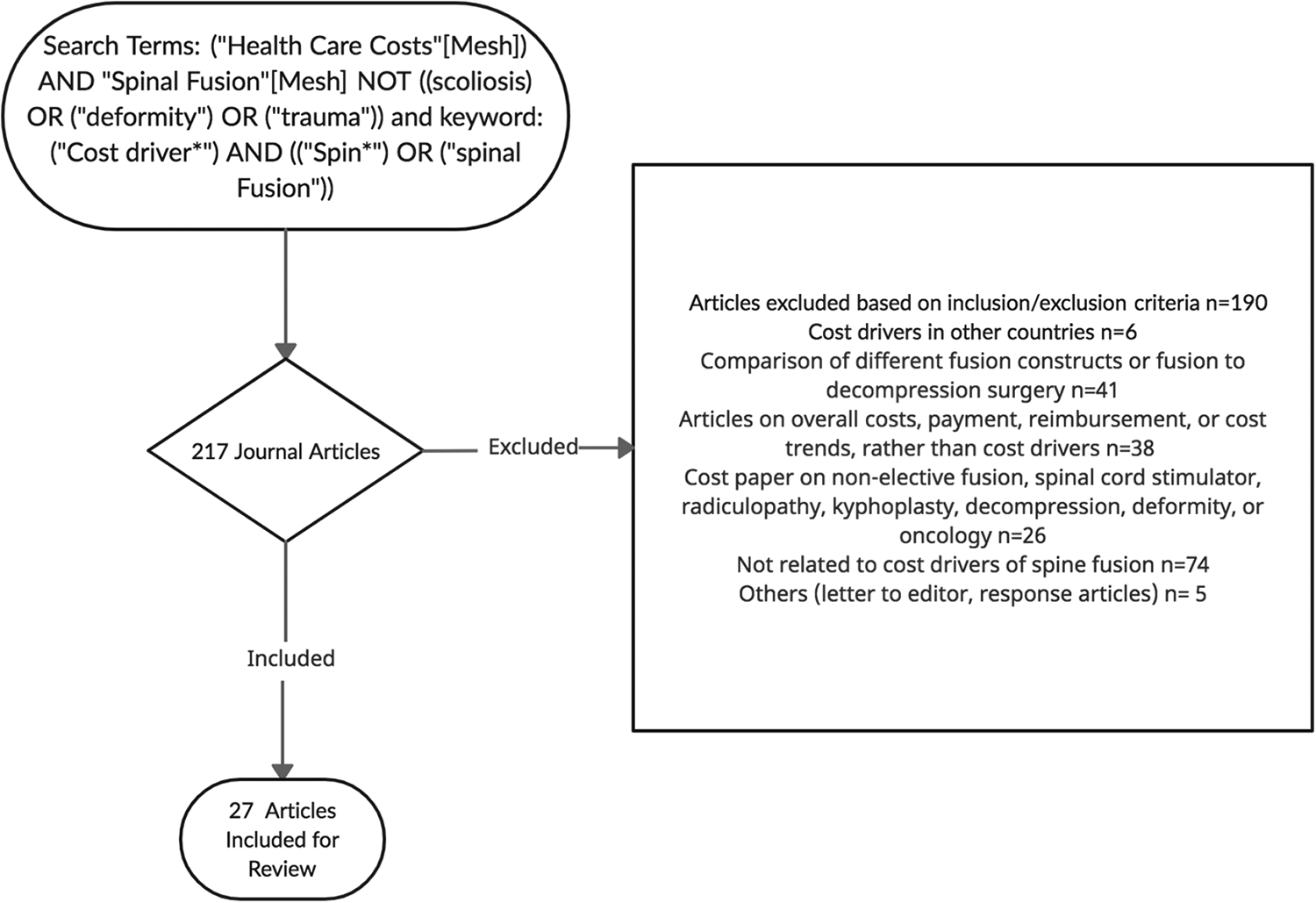
Flow diagram of the literature search for studies on cost drivers in spine fusion.
Major Studies and Identified Cost Drivers for Instrumented Spine Surgery.
Cost Drivers - Overview
The reported cost for treatment of degenerative spine pathologies was reported in 2006 to be close to $85 billion. 9 Recent trends data showed an increase of 138% from 2004 to 2015 in elective lumbar fusion in patients over the age of 65. 10 Furthermore, cost of elective lumbar fusion surpassed that of other spine fusions in 2015 with lumbar fusions representing 42% of total fusion cost of $10.2 billion. 10 Cost of spine surgery is heavily reliant on technology which has exponentially advanced at a tremendous pace over the last decade. ‘Cost driver’ as defined in this study is the factor that results in a change in the cost of a procedure cost while ‘cost’ is represented by the actual cost for the procedure or what the medical system was reimbursed for the procedure. A surgeon’s understanding of the cost and cost drivers in his/her practice allows for identification of variances in cost which ultimately allow for development of strategies that could allow for cost reduction in the current climate of increasing health care expenditure. All cost drivers for spine instrumented surgery were identified by the literature search and are detailed below. Cost drivers were identified in the preoperative, perioperative, and postoperative periods. Additionally, specific factors are discussed such as timing of surgery, surgeon specialty, surgeon volume, imaging, revision surgery, and patient related factors as to whether or not they drive costs of spinal fusion surgery.
Cost Drivers in Lumbar Fusion
Twitchell et al. published their experience with cost drivers of elective lumbar posterolateral instrumented fusion in 2018. The Utah group identified 276 patients who underwent 1 or 2 level elective lumbar fusions. They determined that total cost included 55% for supplies and implants, 36% for facility cost, 7% for pharmacy costs, and 2% for laboratory and imaging. When supplies and implants were combined with facility cost, this accounted for 91% of total cost. Surgeon fees were not mentioned in the study. 8 Beckerman et al. reported the cost drivers for a single level lumbar fusion including single level posterior fusion, lateral fusion, TLIF, and ALIF. Their findings demonstrated that 44% of total cost was for surgical supplies, 38% for services, 14% for room and care, and 4% for pharmacy. Surgeon fees were not discussed in this study as well. Their major drivers of cost included surgical approach, implants, operating room time, and length of hospital stay. They found that the use of an interbody device represented a high portion of the direct cost for instrumented fusions. 3 Malik et al. studied the overall 90-day cost for Medicare patients who underwent ALIF surgery and reported that 76.4% of the cost were related to facility charges, 11.5% for surgeon fees, 7.4% for readmission cost, 0.9% for hospitalization services, 1.7% for anesthesia, 0.3% for imaging, 0.7% for office visits, 0.6% for physical therapy and rehab, and 0.5% for emergency department visits. 6 Overall major costs in lumbar fusion are driven by facility charges and cost of supplies and implants. Surgeon fees and imaging account for a small percentage of total cost.
When cost is divided into preoperative, hospital admission, and postoperative groups as done by Marrache et al. for patients undergoing a single-level posterior lumbar spinal fusion, they reported a total median spending of $60,714. Preoperative spending accounted for 7% (median spending of $3,566) of total spending and postoperative spending accounted for 8% (median spending of $1,954) of total spending which highlights that a majority of cost occurs during the perioperative period driven by previously stated factors. Major drivers of cost during the preoperative period were related to imaging which consisted 33% of the preoperative spending followed by injections which accounted for 15% of total preoperative cost. Unplanned postoperative readmission resulted in the highest cost to postoperative spending and second highest to overall costs. 11
Cost Drivers in ACDF
Reese et al. published on the cost drivers of ACDFs which demonstrated that total cost included 39% for supplies and implants, 37% for facility costs, 14% for physician fees, 7% for pharmacy, and 3% for imaging and laboratory studies. When facility costs and supplies were combined, this accounted for 76% of total cost. 2 The cost utility of performing a 1-level or 2-level ACDF in the outpatient vs. inpatient setting was evaluated by Purger et al. 90-day charges were significantly lower for procedures performed in the ambulatory setting ($33,362 vs. $74,667). The direct cost was also significantly lower for outpatient ACDFs ($9,305 vs. $15,624). Interestingly, patients undergoing outpatient surgery tended to be younger, white males from wealthier ZIP codes with less co-morbid conditions. 12 Similar to lumbar fusions, the major cost drivers in ACDF are related to supplies, implants, and facility costs. ACDF performed in the outpatient setting reduces the facility costs which are a major driver of cost.
Post Discharge 90 Days Costs and Readmissions
Several papers discuss the drivers of variability in 90-day cost for elective lumbar fusion and ACDF. Sivaganesan et al. reported post discharge health care resource utilization (health care visits, pain medications, and imaging/ER visits) accounted for 4.6% of total cost or average cost of $1,371. Imaging and ER visits accounted for 0.43% of total cost, medications (1.4%), and post discharge health care visits (2.8%). Readmission within the global period accounted for as much as 23% of total cost. The readmission rate was 5% in their study. 7 Similar results were demonstrated by Chotai et al. looking at 90-day post discharge cost drivers. Post discharge health care resource utilization accounted for 5% of total cost; imaging and ER visits (0.92%), medication cost (2.4%), and postoperative health care visits (2.8%). Readmission accounted for as much as 35% of total costs. 4 Goyal et al. performed an analysis from a national all-payer database looking at factors associated with the costs of readmission after elective ACDF. The study found that national rates were 3% and 6% for 30-day and 90-day readmissions. The median cost of a 30-day readmission event was $6,727 and the median cost for a 90-day readmission event was $8,507. Predictors for readmissions at 30-days and 90-days were number of procedures at the index admission, length of stay at the index admission, length of time between index admission and readmission. The study also found that even though cervical myelopathy accounted for 3.6% of all 30-day readmissions, it resulted in the largest share (8%) of 30-day readmission costs. 5 Overall, readmission costs are the major drivers of cost in the postoperative period.
Imaging Costs
Imaging plays an important role in the diagnosis, intraoperative treatment, and post-operative surveillance of spine fusion. Numerous studies have evaluated the costs of imaging in spine surgery as an area to target for cost savings. Studies have shown that imaging can cost anywhere from 0.3-6.45% of total cost associated with spine fusions. 2,4,6 -8,13,14 Twitchell et al. reported imaging cost to account for 1% of total cost for lumbar interbody fusion. Reese et al. reported imaging cost of 2% of total cost for ACDFs. Malik et al. reported imaging to cost 0.3% of total costs for ALIFs. To evaluate if different imaging modalities would change cost, Khanna et al. compared cost of intraoperative fluoroscopy to computed tomography guided navigation for single level MIS TLIF. Total cost analysis showed no significant difference between fluoroscopy vs. CT navigation groups ($32,347 vs. $32,656). 15 Further analysis demonstrated that OR and implant fees contributed to 69% of total charges in the fluoroscopy group and 64% in the CT navigation group. Direct imaging costs revealed that the intraoperative imaging cost was higher in the fluoroscopy group ($4,829 or 5% of total cost) vs. the CT navigation group ($3,297 or 3% of total cost), however, the cost differences were not statistically significant. Parker et al. evaluated imaging costs for revision lumbar fusion surgery. Imaging cost amounted to an average $1,284 of the total cost of $32,915 which amounts to 3.9% of total 2-year cost. 13 In revision ACDF due to cervical pseudoarthrosis, imaging costs accounted for 6.45% ($1,169) of total direct costs. 14 In conclusion, imaging, despite its crucial role in spine surgery, is not a major driver of cost.
Patient Related Cost Drivers
Several studies assessed the role of patient comorbidities on cost related to spine fusion. Most studies demonstrate that higher BMI, age, diabetes, adverse events, and higher severity of index score all resulted in higher cost for patients undergoing spine fusion.
Numerous studies demonstrated that obesity was associated with higher costs. Higgins et al. evaluated the role of body mass index (BMI) on in-hospital cost after cervical, thoracic, and lumbar fusions. They found a significant association between obesity and longer anesthesia times and surgical duration. Morbid obesity resulted in a 10 times higher rate of wound complication and $9,078 increase in overall cost. Kalanithi et al. showed that morbid obesity was associated with increased in-hospital complication rate especially for anterior cervical and posterior lumbar fusions. 16 Morbid obesity when compared to normal-weight patients was associated with significantly longer hospital stays (4.8 days vs. 3.5 days) and significantly higher hospital costs ($108,604 vs. $84,860). Puvanesarajah et al. found that obese and morbidly obese patients undergoing posterior lumbar fusion were also associated with increased length of stay, higher 30-day readmission rates, and on average $8,000 higher hospital costs. 17 Minhas et al. found that age, obesity, and diabetes were all associated with significantly increased average hospital costs ($681- $1,877 in patients undergoing anterior cervical fusions). 18 In contrast, one study by Narain et al. demonstrated that a higher BMI resulted in similar cost compared to patients with lower BMIs in patients undergoing 1-level or 2-level ACDF. 19
Other factors that are drivers of cost include severity of illness score, adversity events, and prior hospital admissions. Kaye et al. reported significantly increased hospital cost for patients with higher severity of illness score for patients undergoing lumbar spine fusion. 20 Adverse events were reported by Culler et al. to result in longer hospital stay and significantly higher costs; $42,358 (infection) to $10,100 (dural tear). 21 Eleswarapu et al. found that a history of more than 1 admission in the prior year, lumbar fusion of 4 or more levels, and surgery duration greater than 5 hours were predictors of increased hospital charges. 22
Infections
Infections following spine fusion surgery can impose significant financial impact on the health care system. Several studies evaluated the cost burden of post-operative wound infections and presence of systemic infections with spine surgery. Kuhns et al. found that patients with post-operative wound infections after posterior cervical fusions incurred significantly higher post-operative costs compared to the non-infected patients ($16,970 vs. $7,658). 23 Adjusted for inflation, wound infections were associated with higher cost of an average $12,619 more that those without infection. Rosenthal et al. conducted a study assessing cost and hospital utilization related to postsurgical staph aureus superficial site infection (SSI) and blood stream infection (BSI) during a 180-day follow up period post elective spine fusion. 24 The study found that the rate of contracting a S. aureus during the 180-day period was 2.22%. Additionally, 96.03% of patients with invasive S. aureus infection had at least one readmission compared with 19.18% patients without S. aureus infection. The S. aureus infected group had on average 14.21 and 6.38 more days of hospital stay at the index hospitalization and readmission than the non-infected group. S. aureus infection resulted in higher hospital costs. Invasive S. aureus (BSIs, deep or organ/space SSIs) variable hospital cost averaged $50,966, any S. aureus infection average cost was $39,820, and no infection average hospital cost was $30,243. Donnally et al. observed that patients with hepatitis C virus (HCV) without liver disease undergoing lumbar fusion had higher costs and complication rates. Patients with HCV incurred an 11.4% higher surgery cost and 15.3% higher 90-day hospital reimbursement cost. The surgical cost between patients with and without HCV were $28,713 vs. $25,448 and 90-day costs were $33,447 vs. $29,016. The cost increase was not due to length of stay or 90-day readmissions, but the cost difference was due to patient complications. Patients with HCV undergoing lumbar fusion had higher incidence and odds of requiring a blood transfusion, developing pneumonia, respiratory failure, UTIs, wound infections, and cerebrovascular accidents. 25
Perioperative Factors
The role of the timing of surgery was also investigated as it related to hospital length of stay and cost burden. While the day of the week did not impact cost, the time of surgery did affect cost due to increased length of stay resulting in higher facility fees. Neifert et al. evaluated the role of surgical start time on length of stay and cost in patients undergoing ACDF and posterior cervical fusion. 26 ACDF starting after 2 PM had longer length of stay and significantly higher costs of hospitalization (adjusted difference of $1,177). Patients undergoing posterior cervical fusion starting after 2 PM also had longer length of stay and significantly higher costs (adjusted difference of $2,305). Not surprisingly, the day of the week did not have an impact on cost as Hijji et al. observed in a study of MIS TLIF patients where specific day of the week was not associated with length of inpatient stay or higher total hospital cost. 27
Revision Surgery
Cost of revision surgery is associated with increasing costs. In patients who have had lumbar spine surgery, 10-40% of patients have persistent or recurrent symptoms requiring revision surgery due to failure of fusion, continued symptoms, or adjacent segment disease. 28 Parker et al. demonstrated that for revision surgery, both pre- and perioperative factors correlated with increased cost, with perioperative factors being the primary driver. Drivers of cost for revision lumbar fusion were related to the diagnosis of CHF, higher VAS-measured severe leg pain, greater ODI, and worse SF-12 mental health scores. These factors resulted in 1.1 to 1.2-fold increase in cost. SSI, return to the OR, and readmission during the 90-day period were also associated with higher costs. The average 2-year total cost of revision lumbar fusion was $32,915 with a wide range from $24,935 to $63,769. 13
In the cervical spine, symptomatic pseudoarthrosis after ACDF occurs in only 3% of cases, but also represents higher cost for revision surgery. Pennington et al. demonstrated that ACDF revision surgery for pseudoarthrosis was associated with significantly higher total costs. Patients undergoing ACDF due to pseudoarthrosis had a three-fold higher total direct cost compared to controls ($18,120 vs. $8,451). Major drivers of increased cost were hospital stay and surgical costs. 14
Surgeon Factors
Surgeon fees were also evaluated in the literature by several authors. Chotai et al. reported surgeon fees accounting for 15% of total cost for ACDFs. Reese et al. reported comparable surgeon fees for ACDFs accounting for 14% of the total cost. Malik et al reported surgeon fees of 11.5% of total cost for ALIFs. Additionally, surgeon related factors evaluated in the literature that have cost implications include the role of surgeon specialty and surgeon volume. A study by Baek et al. compared the total 90-day outcome and cost between neurosurgeons and orthopedic surgeons using the Humana Commercial Database for elective 1-level or 2-level posterior lumbar fusion. 29 The study found no difference in cost or outcome based on surgeon specialty demonstrating that different training pathways do not affect outcome or cost. Basques et al. performed a retrospective study using the Nationwide Inpatient Sample (NIS) to investigate the effect of surgeon volume on cost as it relates to length of stay and complications for anterior cervical fusion. 30 The findings demonstrated that surgeons with <25th percentile of volume (i.e. 5 cases per year) had significantly increased costs compared to surgeons with volume 75th percentile (i.e. 67 cases per year). Hospital costs were on average $4,569 more for surgeons with <25% volume and $1,213 less for surgeons with volume 75th percentile. The increased cost associated with low volume surgeons were related to increased hospital stay and complications.
Cost Reductive Strategies
Cost-effectiveness analysis is used to estimate the economic cost of a technology to provide a unit of improvement in patient health. 31 With increasing cost and frequency of spine surgery, spine surgeons should be focused on ways to improve outcomes while lowering cost. The next section focuses on cost reduction strategies that can assist surgeons in reducing cost without compromising care. It is vital that surgeons be focused on measuring outcome when initiating cost reduction programs to ensure quality and safety for patients.
Surgeon Awareness of Implants and Biologics Costs
Within our technology-driven field, a major cost driver for spinal surgery continues to be innovative implants and biologics used in complex spinal operations. Surgeons balance the increased cost and lack of evidence of a new device, with the promise of better patient outcomes and advancing surgical progress. In a retrospective analysis of a single-institution database of patients who underwent anterior cervical discectomy and fusion (ACDF), the greatest cost driver was implants, followed by facility utilization. 2 Several studies have demonstrated that increased surgeon awareness of implant costs results in decreased implant costs. 32,33 After providing cost education to surgeons, one prospective study demonstrated cost reductions for ACDF implants. 34 There have been efforts to track and publicly display the costs of individual surgeon waste by health systems, also resulting in decreased expenditure. 35 Intraoperative waste in spinal surgery was prospectively measured at a single-institution, before and after surgeon education, and was shown to decrease from 20.2% of cases to 10.3% of cases, resulting in a cost savings of over $70,000 per year. 36 Surgeons should be knowledgeable not only about the instruments they use, but also about their cost. Awareness of implant cost is thus essential in the pursuit of cost reduction.
Transparency and Vendor Pricing
The cost of spinal fusion implants varies widely between different medical systems, with little transparency. 37 Hospital systems have increasingly made efforts to aggressively negotiate lower implant prices, and limit the number of vendors to allow bulk-purchasing discounts. In one study, University Health System Consortium implant pricing benchmarks and national pricing data were used to create a reference cost for each implant. 38 Any vendor that matched its pricing to the reference cost could make their products available to the surgeons. Cost savings from this practice resulted in a 20% decrease in spinal implant cost, and inter-surgeon cost variability for single-level ACDF decreased by 31.9%. The Cleveland Clinic published their experience transitioning from multiple vendors for spinal implants to a single vendor. 39 There were no changes in revisions, complications, and patient-reported outcomes during the transition, and costs savings were 24% initially after moving to a two-vendor system, followed by an additional 21% moving to a single vendor. The authors note that surgeon participation in selection of a single spinal implant vendor is paramount to successful transition. 40
Standardization
Surgeon implant preferences may vary widely for the same procedure, with a study demonstrating a 10-fold difference ($4,062 vs. $40,409) in instrument charges between surgeons for the same case. 33,41 Additional work has shown that surgeons with high costs do not translate into improved patient outcomes, or conversely, low cost surgeons do not have poorer outcomes. 42 In a single academic institution, wide variability of 90-day and in-hospital costs were found between five surgeons for ACDF, after adjusting for patient co-morbidities, with no difference in patient-reported outcomes. 43 This work suggests that standardization of protocols and implants between surgeons may result in greater cost savings, without compromise of patient outcomes. This process must be delicately balanced with surgeon autonomy and comfort-level using various instrumentation. 44
Ambulatory Care Centers
There has been significant interest in performing more surgery in ambulatory care centers as opposed to traditional hospitals. Much of the cost of spinal surgery is tied to hospital metrics such as length of stay and inpatient utilization of expensive resources. Drivers of cost variability for elective spinal surgery have been studied in large population datasets. One study listed variables such as age, body mass index (BMI), ASA grade, hypertension, opioid use, length of stay, duration of surgery, and inpatient rehab as all influential for 90-day costs following lumbar fusion. 7 In a recent meta-analysis, patients undergoing outpatient ACDF were younger, and less likely to have comorbidities such as diabetes mellitus, than patients who underwent inpatient ACDF. 45 The authors show that outpatient procedures are associated with fewer reoperations, readmissions, complications, and have lower costs, likely related to the selection bias of healthier patients for these procedures. Similar patient characteristics have been reported as drivers for increased 90-day costs after adult deformity surgery, including chronic obstructive pulmonary disease (COPD) and diabetes. 46 Not surprisingly, variables related to the complexity of the operation including revision surgery, number of levels fused, and duration of surgery, were also associated with higher costs. 46,47 While spinal surgery in ambulatory care centers appear to cost less and have at least equivalent outcomes, more careful studies balancing co-morbidities are needed in order to determine which patients are optimal for surgery in an ambulatory setting.
Patient Selection and Complication Avoidance
While surgeons recognize the importance of patient selection for optimizing surgical outcome and reducing costs, it is often not ethical to deny a patient surgery based upon risk factors such as age and medical co-morbidities. Several efforts have been published to develop more comprehensive preoperative evaluation protocols, including multi-disciplinary conferences and careful anesthetic preparations prior to complex spine operations. 48,49 These team approaches to complex spine operations have been shown to reduce reoperation, wound infection, deep venous thromboembolism, and other perioperative complications. 50 Spinal surgeons and insurance payers are increasingly focused on optimizing modifiable patient risk factors prior to surgery, such as smoking, osteoporotic bone density, and elevated hemoglobin A1C. 51 -53 Patient education related to the perioperative risks associated with smoking, osteoporosis, and uncontrolled diabetes is important for both encouraging behavior modification and acceptance of delay in surgery.
As surgical outcomes and complications are closely associated with costs, efforts to optimize patient outcomes and reduce known complications will clearly result in lower health resource utilization. There is a large body of literature related to these topics and an exhaustive review is beyond the scope of this paper. However, surgeons should focus on broad categories of complication avoidance in spinal surgery: infection, bleeding, neurologic deficit, cerebrospinal fluid leak, pseudoarthrosis, and spinal alignment parameters. Careful attention to these areas during surgery, with application of evidence-based guidelines, will reduce complications and costs. For example, use of topical Vancomycin powder for thoracolumbar fusion has been shown in multiple studies to significantly reduce the risk of a surgical site infection by gram positive organisms. 54 Pseudoarthrosis remains a challenge for surgeons, particularly for patients with either large fusion constructs, or with underlying medical comorbidities. A large percentage of the expense of spinal fusion surgery may be tied to products such as recombinant human bone morphogenetic protein (rhBMP) or mesenchymal stem cells within a cellular bone matrix. 55 As observed with instrumentation, surgeon preferences for these products or other bone graft extenders vary widely, and are often based upon a combination of the literature, anecdotal experience, and the local trends. However, costs and the utilization of these products will likely decrease with increased education of surgeons and efforts to standardize fusion algorithms.
Enhanced Recovery after Surgery Protocols
Recently, there has been increasing focus upon the use of enhanced recovery after surgery (ERAS) protocols in spinal surgery. One of the major goals of ERAS protocols has been the reduction in opioid utilization. Wang et al have demonstrated that the use of ERAS protocols for transforaminal lumbar fusion patients not only reduces opioid utilization but also substantially reduces length of stay from 4 to 1.4 days. 56 Reduction in hospital length of stay would be expected to significantly reduce hospital costs associated with spinal fusion surgery. One of the underlying principles of ERAS protocols is standardizing the approach to pain control, education, and early mobilization after spinal surgery. Adherence to these standardized protocols is variable and therefore the results are not always associated with lowering hospital costs. 57 However, standardization of hospital peri-operative protocols has been associated with lower costs and improved outcomes for a number of surgical procedures. 58 -60
Limitations
Due to the limited quantity and heterogeneity of the literature available, a descriptive analysis only was performed. When more formal cost-utility studies are available, it will be feasible to perform more quantitative analyses. The study was also restricted to the English language and focused on studies performed only in the United States. Thus, a limitation of the manuscript is that this study only considered American costs of instrumented spine surgery and therefore further studies are necessary (to take lessons learned from US practice) to include international data in order to inform the global spine community.
Summary
In many scenarios, spinal surgery has been shown to be cost-effective when compared to continuation of non-surgical options over the long term. 61 Nevertheless, the costs of spinal surgery are high and are increasing as our population ages. With declining financial margins in most hospital systems, it is becoming more important to focus on opportunities to reduce cost while preserving patient-reported outcomes. We have briefly reviewed cost drivers and strategies which can be implemented to lower costs without compromising outcome. To summarize, surgeons should go beyond participation in cost effective strategies and spearhead initiatives to reduce cost without compromising outcomes. It begins with education around the overall costs associated with spine instrumented surgery with a focus on identifying the cost drivers. This can be followed by creating an atmosphere of transparency as it relates to facility fees and implant cost. Price matching and/or narrowing options toward a double or single vendor can lower cost for hospital systems. Surgeons can also standardize operating room protocols and implant utilization to further reduce cost. Other strategies involve identifying which procedures and in which patients are optimal for outpatient surgical centers. More importantly, surgeons should also be meticulous about complication avoidance and optimizing patient selection to prevent re-operation and readmissions as they result in increased cost. Surgeons should be motivated to implement ERAS protocols to enhance recovery and reduce hospital length of stay and thus cost. Ultimately, it is the spine surgeon who can help lower costs. The field of spine surgery has benefited from much advancement. Careful adoption of new technologies with attention to cost and ultimately documenting effectiveness will pave the pathway forward.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by a grant from AO Spine North America.