
Abstract
Study Design:
To evaluate the mechanical effectiveness of “tuning fork” plate fixation system by comparing with dual iliac screw fixation under different spinal motion through finite element analysis (FEA).
Objective:
Lumbosacral deficiencies occur from birth defects or following destruction by tumors. The objective of this study was to evaluate the mechanical effectiveness of the tuning fork plate compared to dual iliac screw system which is the gold standard fixation in treating lumbosacral deficiencies. This is an innovative fixation device for treating lumbosacral deficiencies.
Methods:
The deficiency model was prepared using a previously developed and validated finite element T10-pelvis model. To create the lumbo-sacral deficiency the segments between L3 and sacrum were removed from the model. The model was then instrumented from T10 to L2 segments and the ilium using either the tuning fork plate or a dual iliac screw construct. With the ilium fixed, the T10 vertebrae was subjected to 10 Nm moment and 400 N follower load to simulate spinal motions. Range of motion (ROM) of spine and stresses on the instrumentation were calculated for 2 fixation devices and compared with each other.
Results:
The 2 fixation systems demonstrate a comparable motion reduction in all loading modes. Stress values were higher in the dual iliac screw constructs compared with the tuning fork plate fixation system. The factor of safety of the tuning fork plate device was higher than the dual iliac screw fixation by 50%.
Conclusions:
Both fixation devices had similar performance in motion reduction at spine levels. However, based on predicted implant stresses there were less chances of implant failure in the fork plate fixation, compared to the dual iliac screw system.
Introduction
Lumbosacral deficiency can occur due to the destruction of the lumbar and/or sacral segments. This could be due to tumors or as a birth defect such as sacral agenesis. Mechanically, this leads to abnormal load transfers between the spine and pelvis. Clinically, it results in a shortening of the trunk, sitting and ambulation difficulties. The patients often suffer neurological issues involving varying degrees of paralysis of the lower sacral segments with a loss of bladder and anal sphincter control. The bony destruction or failure of formation of the lumbosacral junction leads to instability and a relative hypermobility in the lumbo-pelvic junction (Figure 1). In the sacral agenesis, the iliac wings are parallel to each other and are the sole distal anchor points for instrumentation due to absence of sacrum. 1
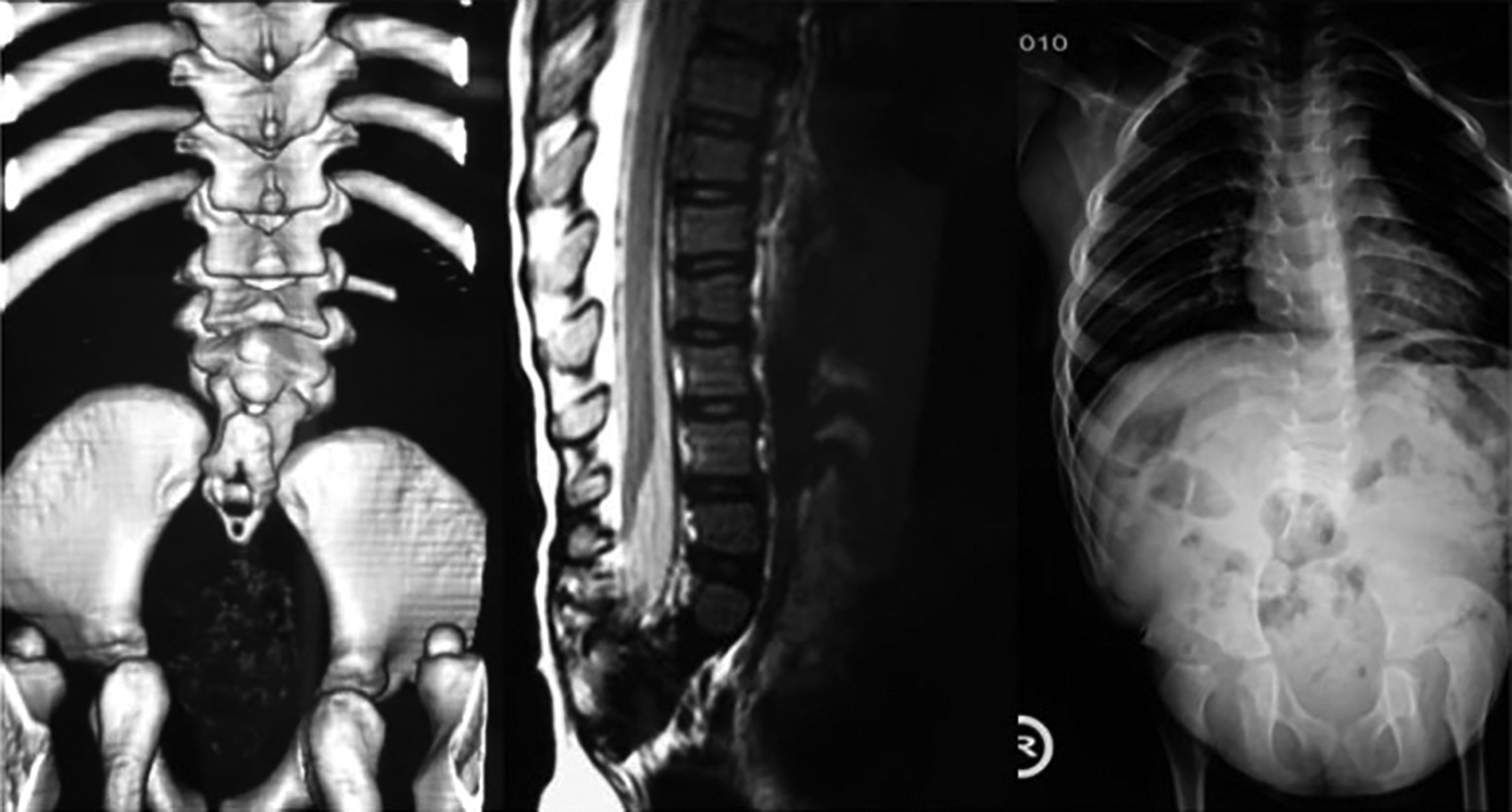
Lumbosacral deficiency. 1
Stabilization of the spinal column with lumbo-sacral deficiency is a surgical challenge. Current fixation techniques pose problems due to fracture and loosening. Dunn-McCarthy hooks can migrate through the ilium and cause problems (Figure 2A). The Galveston technique involves complex rod bending and can lead to, instrument prominence, rods migration, and high incidence of fixation failure (Figure 2B). 2 There are several anecdotal reports and short case series of ad-hoc fixations described in literature which have their own unique problems.3,4 The early success of the Galveston technique led to the evolution of the dual-iliac screw systems. This is technically easier to perform and has greater pullout force compared to other fixation methods (Figure 2C). 5 Although the aim of these techniques is to reach optimal biomechanical spinopelvic stability, clinical evidence has shown that instrumentation failure and loosening are still a challenge. To address biomechanical deficiencies inherent with the current techniques we have developed a customized implant for a secure and rigid fixation to the ilium that links via an integral rod to the spine.
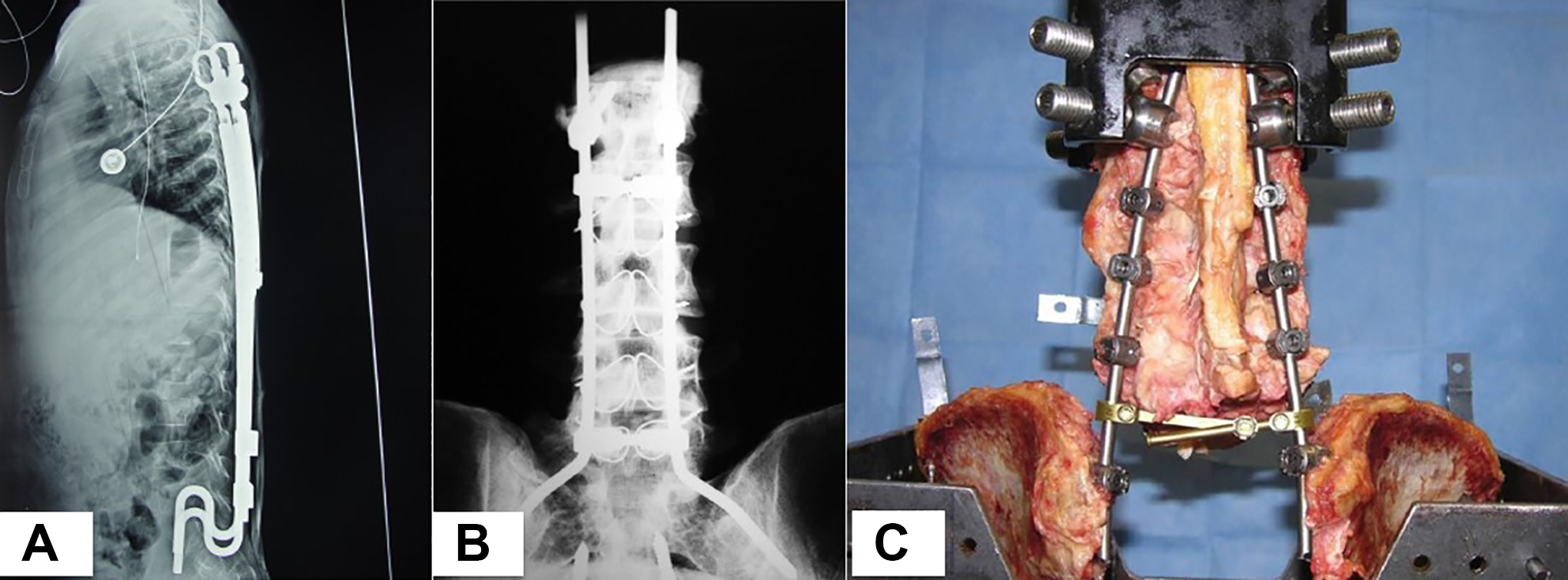
(A) Dunn-McCarthy rods, (B) Galveston technique, (C) Iliac screw system (Hopkins I method).
The new concept is termed the “tuning fork” plate and it evolved from the Variable Screw Placement (VSP—Acromed Corp) rod plate. It comprises a VSP plate doubly bent to resemble a tuning fork. The locking screws engage through the plate. A variable length rod is attached to allow fixation to the spine proximally. The design is available in different rod diameters, to facilitate pedicle screw fixation to the spine (Figure 3). It can be used across various age spectra.
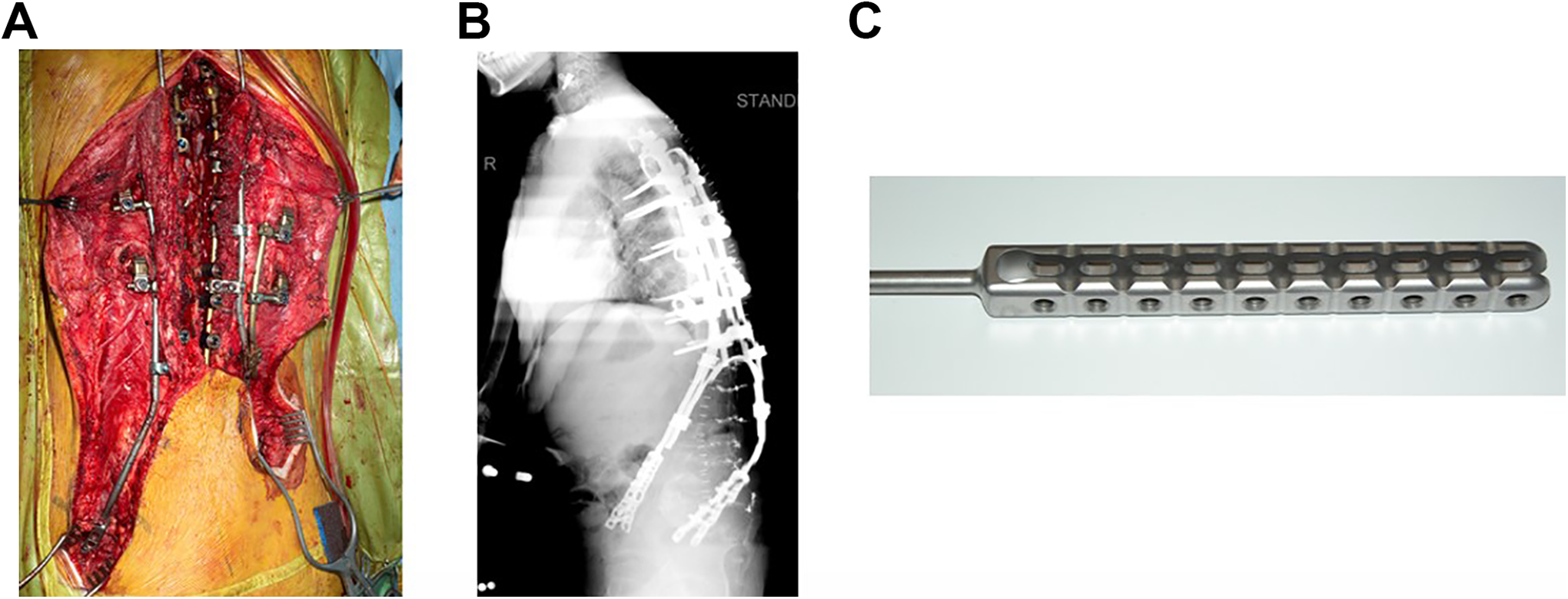
(A, B) Tuning Fork Plate in a patient, (C) Tuning Fork Plate device.
The purpose of the present study is to evaluate the mechanical effectiveness of “tuning fork” plate by comparing with dual iliac screw fixation under different spinal motion through finite element analysis (FEA).
Material and Methods
Institutional review board approval was not needed for this study. The previously developed and validated finite element T10-pelvis model6,7 was used for the deficient model. The 3-dimensional (3D) pelvis geometry was generated using a 1 mm slice of computer tomography (CT) scans of a 55 year old male pelvis without any abnormalities, degeneration or deformation. The 3D reconstruction of spine-pelvis model was accomplished using MIMICS software (Materialise Inc., Leuven, Belgium). After 3D reconstruction of the bones and spinal discs, the structures were imported into Geomagic Studio software (Raindrop Geomagic Inc., USA) to reduce noises, remove spikes, smooth surfaces, and create patches and grids for meshing. Hypermesh software (Altair Engineering, Inc., USA) was used to create the mesh structure from the 3D model.
The spine and pelvis were modeled as trabecular cores surrounded by a cortical layer. The linear hexahedral element was utilized for cortical and cancellous bones of vertebrae and intervertebral discs. Tetrahedral element type was used for the cortical and cancellous bones of the pelvis. The truss elements were employed for ligamentous tissues including the SIJ and spinal ligaments.
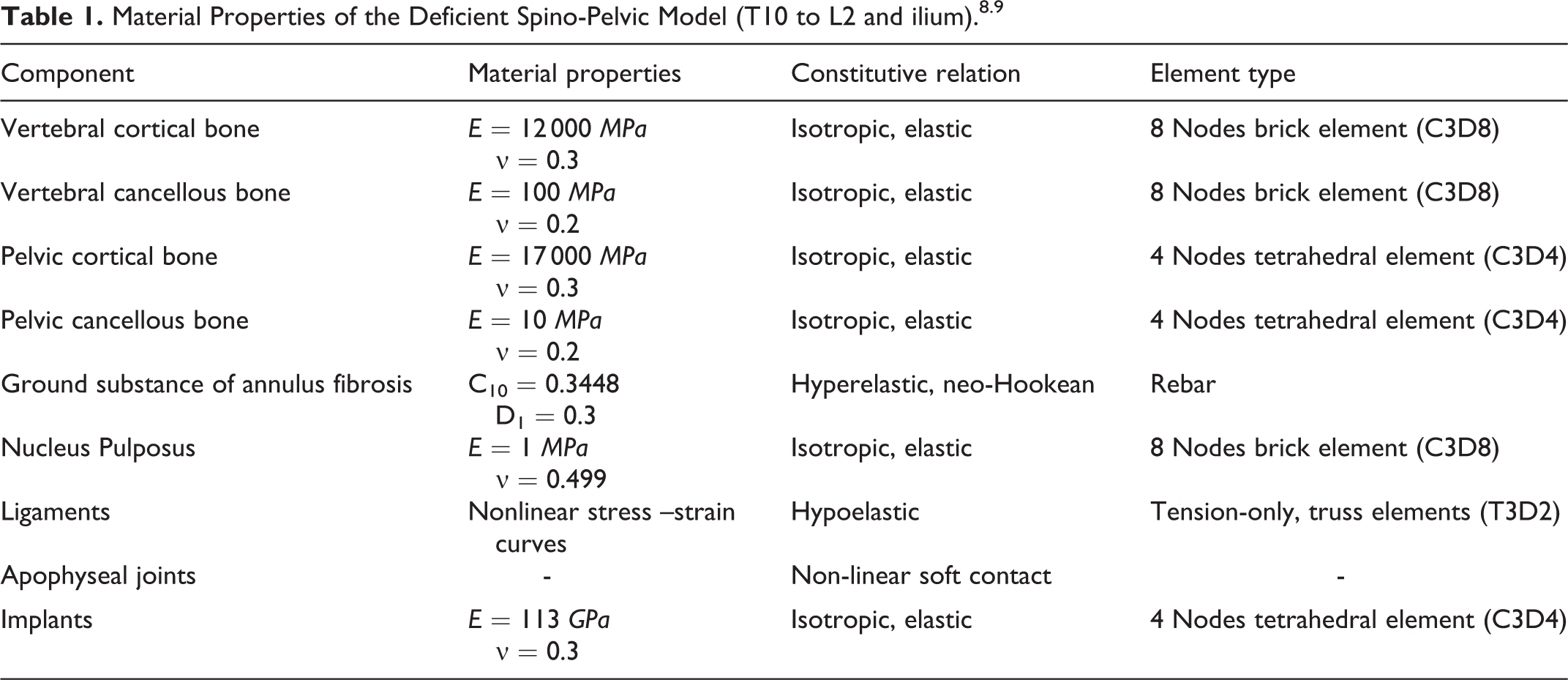
To create the lumbo-sacral deficiency, segments from L3 vertebra through to sacrum were removed from the T10-pelvis model. Cortical and cancellous bone, nucleus and annulus as isotropic elastic, and ligaments as hypo-elastic material properties were modeled and all implants were defined as titanium (Table 1).
The deficient model was then instrumented either with tuning fork plate or the dual iliac screw system. For the dual iliac screw fixation system, 5.5 mm pedicle screws were placed in the pedicles from T10 to L2 and 8.5 mm iliac screws of 45 mm long into the pelvis. The instrumentation was linked with 6 mm titanium rods and cross-linked across the midline (Figure 4). The tuning fork plate construct comprised of 5.5 mm pedicle screws proximally from T10 to L2. The flanges of the tuning fork plate were contoured and locking screws inserted to fix the tuning fork to the pelvis. The locking screws spanned across both the plate flanges and both the iliac wing cortices. The proximal portion of the tuning fork construct comprises of 6.0 mm titanium rods. These were anchored into the proximal part of the construct (Figure 5).
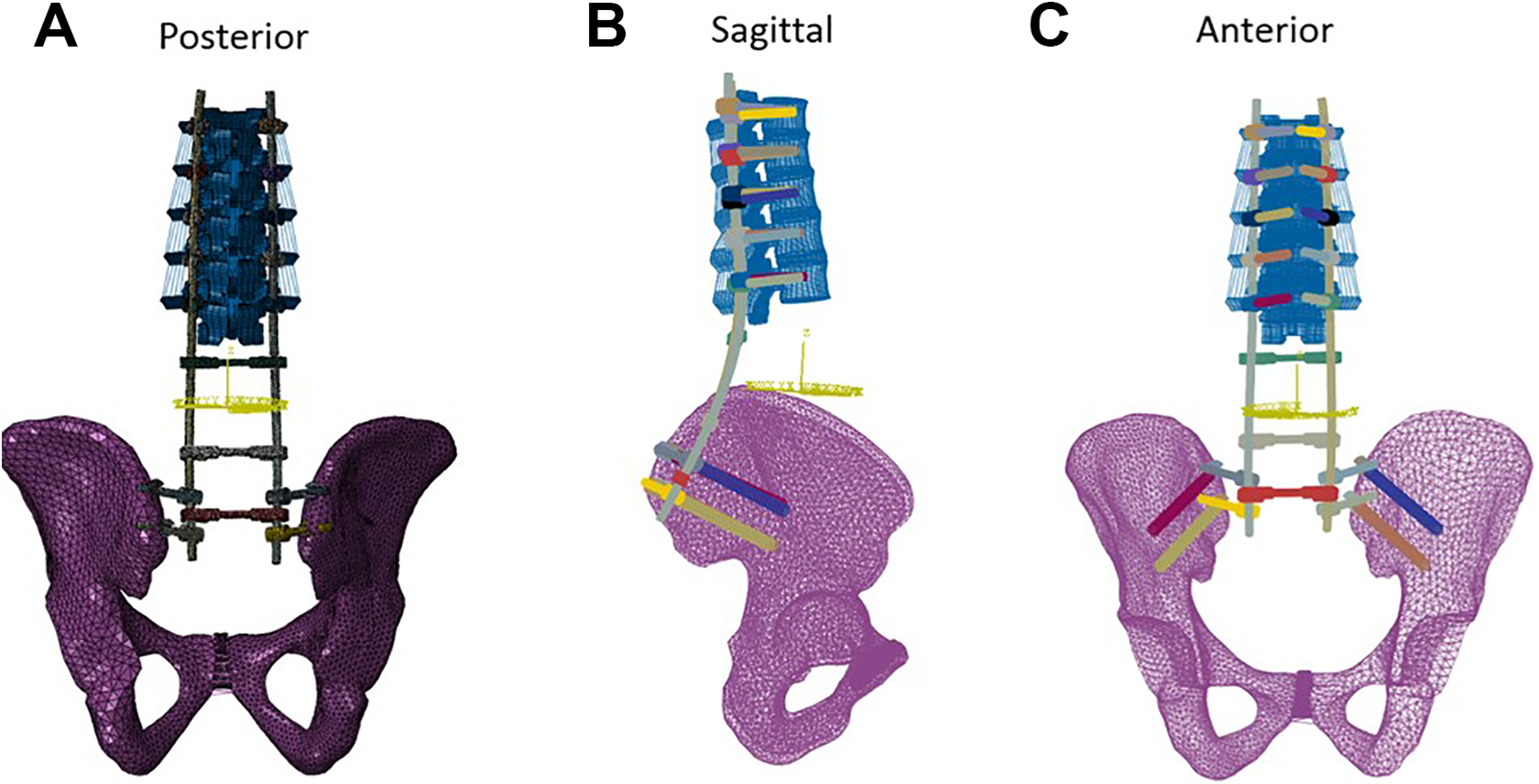
Deficient spinopelvic model instrumented with dual iliac screw system fixation, (A) posterior view, (B) sagittal view, (C) anterior view.
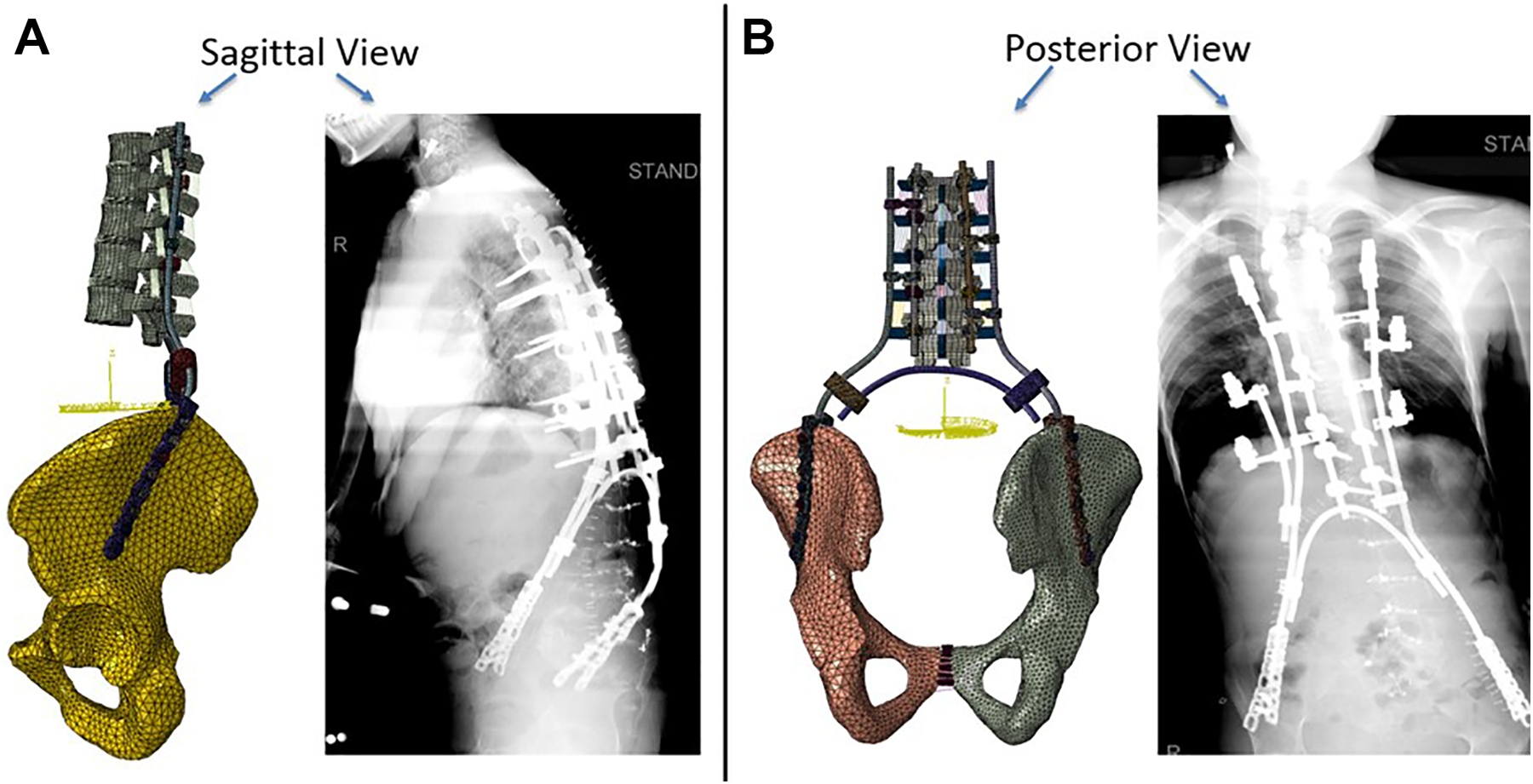
Deficient spinopelvic model instrumented with tuning fork plate fixation system, (A) sagittal view, (B) posterior view.
The deficiency model that was instrumented with tuning fork plate had 596 139 elements and the model instrumented with dual iliac screw had 219 256 elements.
The tie constraints for the tuning fork construct were defined as the contacts between screws-bone, screws-rods, crosslink-rods, and screws-plate. Surface to surface contact was used for plates-bone contacts. The tie constraints for the dual iliac screw fixation system were defined by contacts between screws-bone, screws-rods, crosslink-rods. The ilium was fixed in 6 degrees of freedom. T10 was subjected to 10 Nm moment and 400 N preload to simulate flexion-extension, lateral bending and axial rotation. In all 6 loading modes (or motions), the range of motion (ROM) of spine and stresses on the device were calculated for 2 fixation devices and compared. Stress values were used to calculate the factor of safety (FOS) for both the constructs to assess the chances of failure of the instrumentation. Factor of safety was defined as the ratio of the Titanium yield stress (860 MPa) to peak von Mises stress in the construct for a given loading condition. The higher the FOS the lesser the chances of rod fracture.
Results
Model Validation
The sacrectomy/ lumbopelvic deficiency model was validated against the cadaver based on the Cunningham criteria 5 for the loading and postural conditions. This experiment was carried out for L2 to L5 segments and the ilium which was instrumented with bilateral single iliac screw fixation system (Hopkins 1 Method) under 2 leg stance condition. A 12.5 Nm pure moment load was applied at the superior endplate of L2 to simulate various spinal motions. The motion at each level of lumbar spine was calculated for flexion-extension, lateral bending, and axial rotation. The FE data (shown as FE data in the figure) for all physiological loadings fell within the range experimental data shown as cadaver data in the figure (Figure 6). We used bilateral single screw fixation for validation of our FE model due to lack of data for bilateral dual screw. After the validation, we utilized the validated model to perform the comparison between the dual iliac screw fixation and the tuning fork plate fixation.
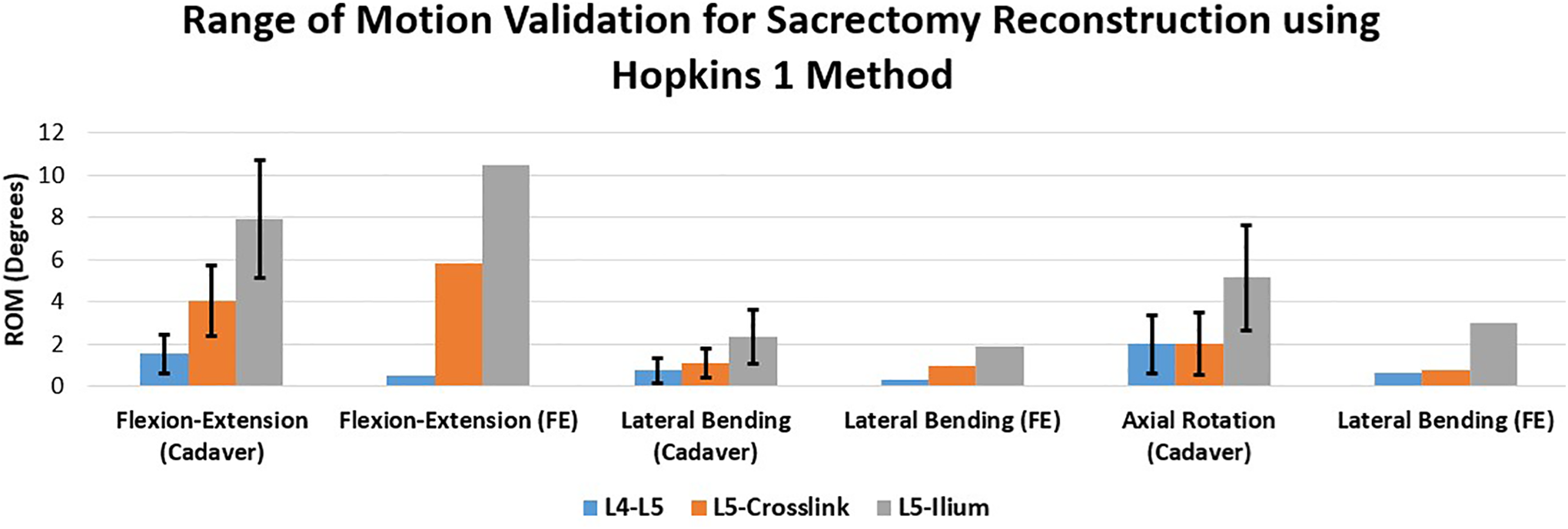
Deficient spine finite element (FE) model validation for L2 to L5 segments and the pelvis instrumented with bilateral single iliac screw fixation system (Hopkins I Method) under 2 leg stance condition and 12.5 Nm pure moment loading.
Range of Motion
The range of motion (ROM) of all spine levels decreased under different loadings after fixation of spine using both tuning fork plate and dual iliac screw fixation systems (Figure 7).
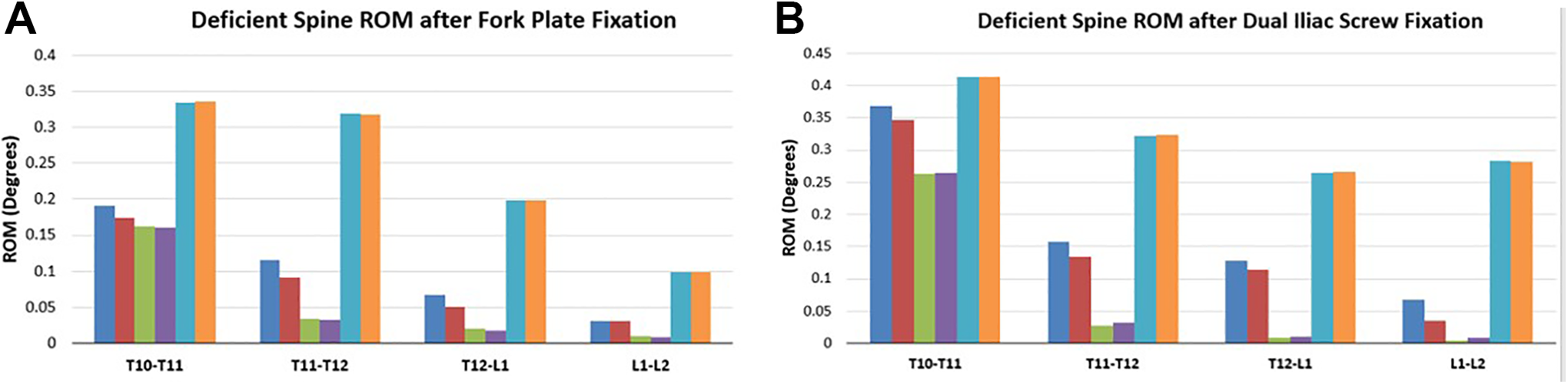
Comparison of deficient spine range of motion (ROM) with instrumentation under 10 N.m moment and 400 N preload, (A) after fork plate fixation, (B) after dual iliac screw fixation.
For both fixations, the highest and lowest motions were noted during axial rotation and lateral bending at all the levels. The fork plate construct demonstrated higher motion reduction in flexion-extension, with similar motion reductions in lateral bending and axial rotation compared with the dual iliac screw constructs. Overall, these 2 fixation systems provided comparable motion reductions.
Stresses
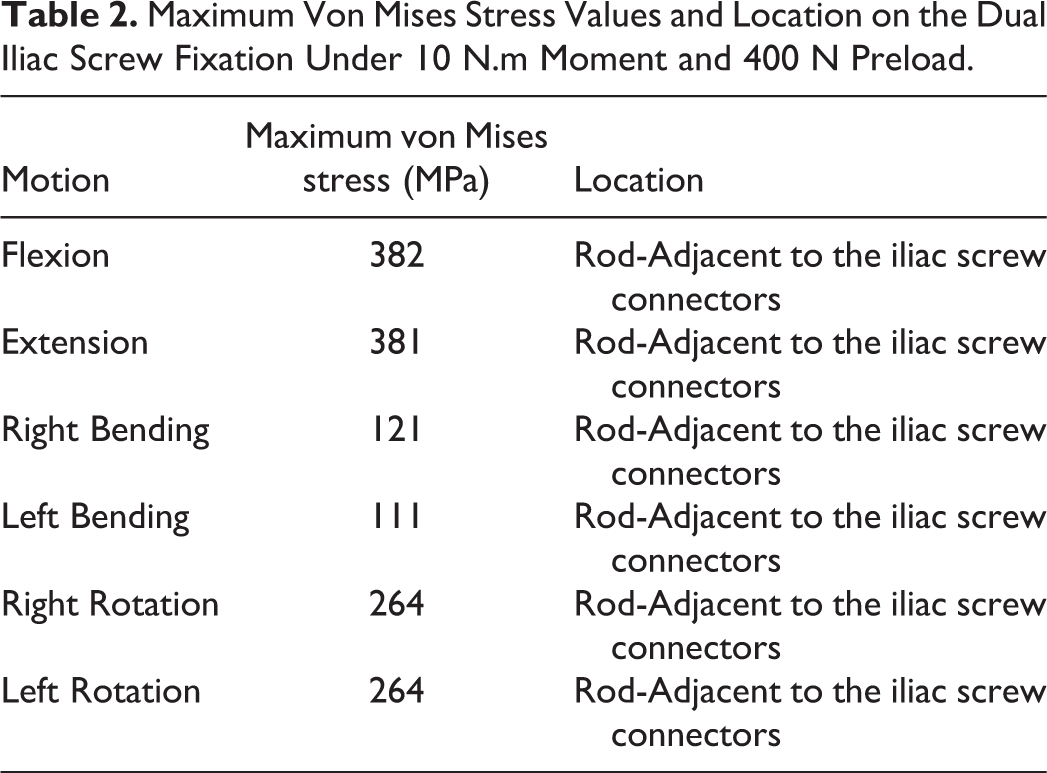
Peak von Mises stresses and locations on the fork plate fixation and dual iliac screw system are shown in Tables 2 and 3.
Maximum Von Mises Stress Values and Location on the Dual Iliac Screw Fixation Under 10 N.m Moment and 400 N Preload.
Maximum von MISES Stress Values and Location on the Tuning Fork Plate Fixation Under 10 N.m Moment and 400 N Preload.
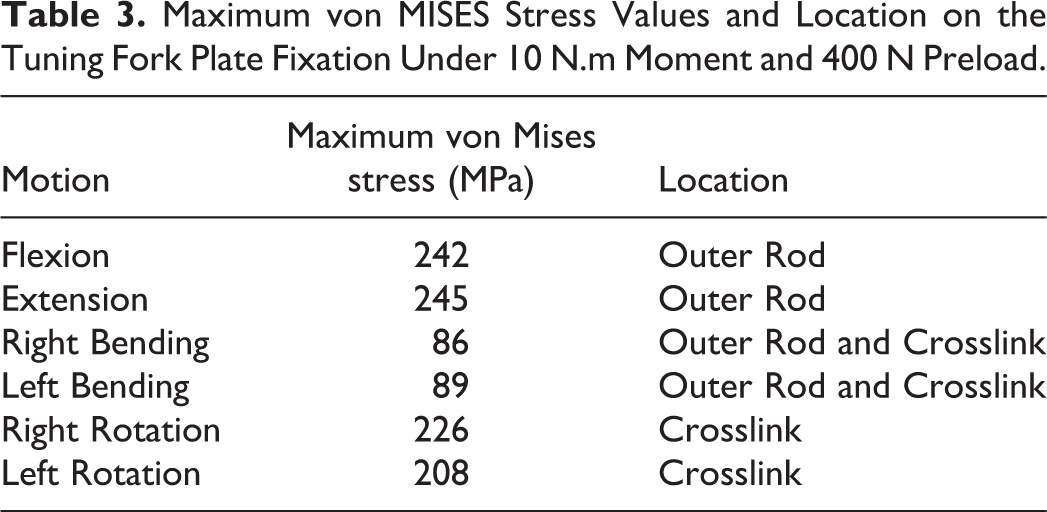
The highest and lowest stresses were noted during flexion-extension and lateral bending for both constructs. The maximum stresses in the dual iliac screw system were located on rods adjacent to the iliac screws connectors. The fork plate device demonstrated maximum stresses on the outer rods and crosslinks for all motions (Table 3). Stress values on the fork plate fixation were lower (22% to 45%) than dual screw fixation.
Figure 8 shows the stress distribution and peak stress locations on the dual iliac screw construct and tuning fork plate construct for 10 Nm flexion motion and 400 N preload. Maximum stresses occurred on the rods in both devices.
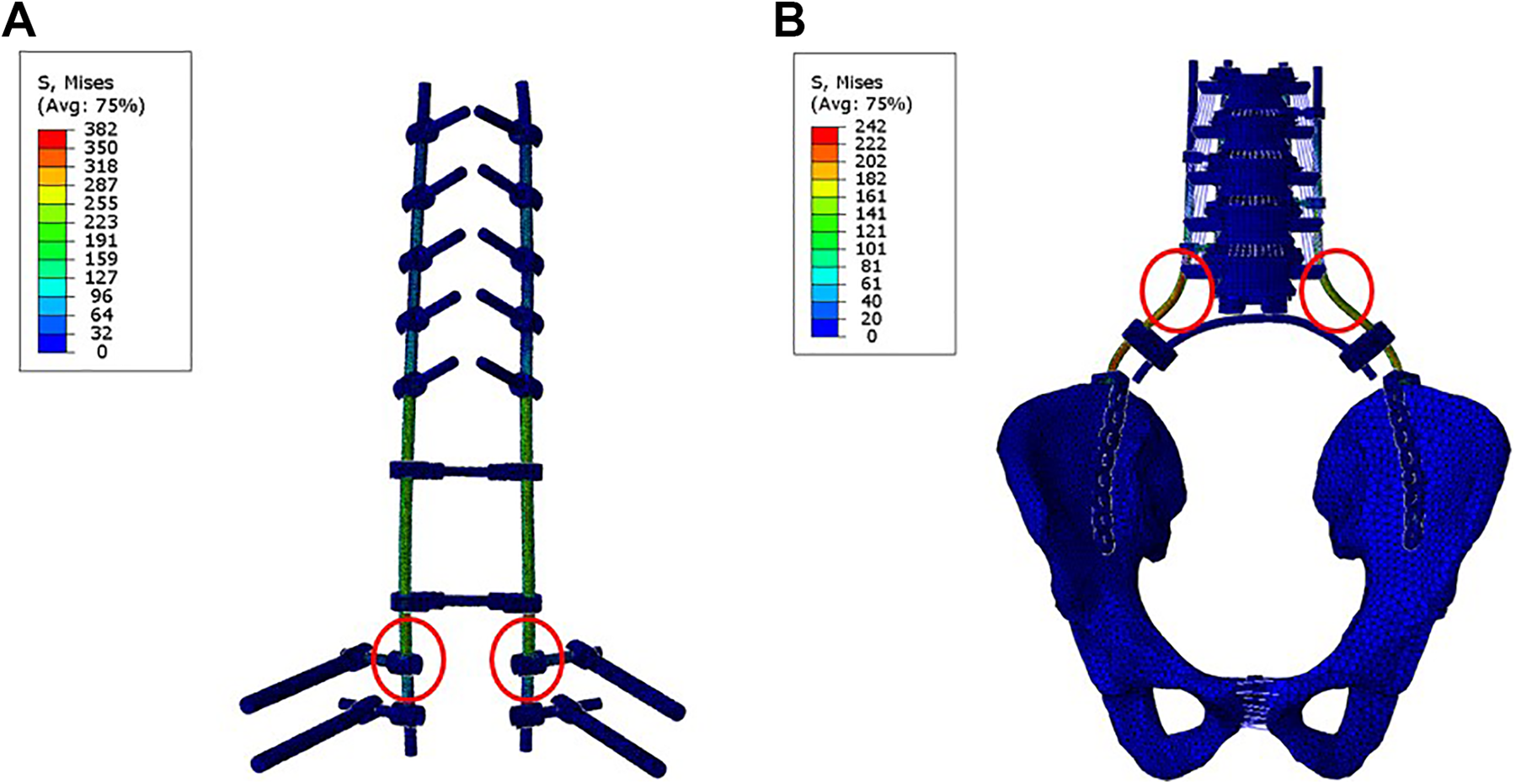
Stress distribution and peak stress location on (A) dual iliac screw construct and (B) tuning fork plate construct during 10 Nm flexion motion and 400 N preload.
Table 4 shows the factor of safety calculated for each device in individual motions. The factor of safety of the tuning fork plate construct was higher than that of the dual iliac screw constructs by up to 50%.
Comparison of Maximum Von Mises Stress and Factor of Safety of the Fork Plate Device vs. Dual Iliac Screw. Factor of Safety Was Defined as the Ratio of the Titanium Yield Stress (860 MPa) to Peak von Mises Stress in the Construct for a Given Loading Condition.
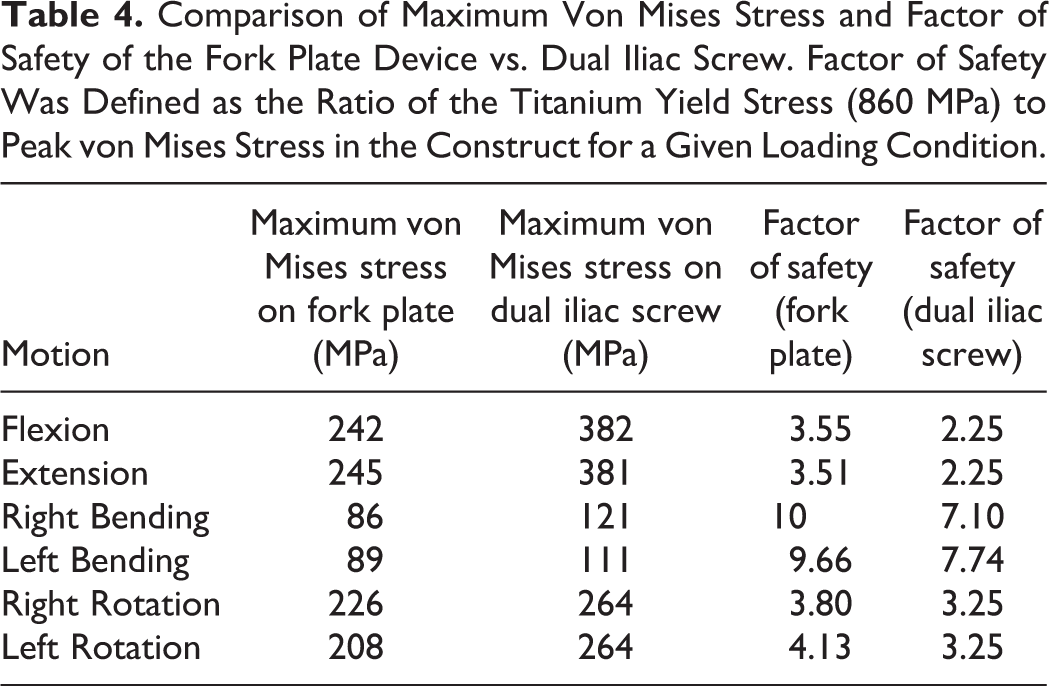
Table 5 and Figure 9 show the maximum stresses values and locations on the plate for the fork plate device.
Maximum Stresses on the Fork Plates Under 10 N.m Bending Moment and 400 N Preload.


Stress distribution and peak stress locations on the plates in the fork plate system during 10 Nm flexion motion and 400 N preload.
The maximum stresses on the plate concentrated on its attachment to the rod.
Discussion
Stabilization of spinal column in the presence of a lumbosacral deficiency is a challenge due to the loss of a stable foundation between the spine and pelvis for load transfer between the trunk and the lower extremities. The absence of the sacrum implies that the iliac wings are the only available anchor points for instrumentation distally. 10 The absence of the sacrum from any etiology can cause a relative shortening of the trunk, problems with sitting and ambulation due to the instability and hypermobility at the lumbo-pelvic junction. Surgical efforts to providing stabilization is fraught with complications such as implant fracture and loosening and loss of fixation. The transition between the relative mobility of the lumbar spine compared with the stable though immobile pelvis creates a stress riser and is a bio-mechanical challenge. The forces across the instrumentation are high resulting in a higher incidence of construct failure. There are several novel, ad hoc and anecdotal constructs described in literature. These have their unique problems such as surgical complexity, access related complications such as vascular injury and prominence of the implants. 3
Cheng et al. 11 demonstrated comparisons between several techniques such as sacral rod reconstruction with single iliac screw, dual iliac screw reconstruction and four-rod reconstruction. They reported that these were not effective in structural stability or in reducing motion.
Studies have showed that a dual iliac screw system is more stable than other fixation systems such as single iliac screw, sacral bar reconstruction or the four-rod reconstruction without anterior support. However, the dual iliac screw system is less stable than four-rod reconstruction with anterior column support or a trans-iliac connector. Such approaches have a much higher morbidity. 12 Dual iliac screws provides sufficient stability for most clinical situations. 13 This should be borne in mind when dealing with sacral deficiencies, as these patients have lower activity demands and surgical reconstruction, is at best damage-limitating.
Le et al. 14 demonstrated that posterior spino-pelvic reconstruction with dual iliac screw system provide sufficient stability. However, in contrast with Chen’s study, 11 there is no incremental biomechanical benefits in using lumbo-sacro-iliac (LSI) screws as anterior supports. The failure mode in their instrumentation occurred at the iliac screw-bone interface. Kawahara et al. performed a finite element analysis 15 and reported that the failure of the dual iliac screw system was noted across the connecting rods closer to iliac screws due to higher stresses. This failure location is consistent with our data of peak stress location in dual iliac screw system (Figure 8A). This illustrates that stress is concentrated along the end-side of the fixation constructs.
Our study also revealed that the dual iliac screw is very stable and effective in reducing the range of motion of the spine after sacrectomy. The tuning fork constructs demonstrated a uniform load distribution evenly across the ilium preventing stress concentrated at any individual screw/bone interfaces.
Dalbayrak et al. 10 utilized iliac wings plates to stabilize patients with sacrectomy, observing that sacral bars are problematic due to the prominence across the iliac wings. The location of failure in one of the cases is consistent with our findings of the location of peak stress in the fork plate constructs (Figure 8B). Dalbayrak’s system 10 lacks a strong connection between spinal rods, however, this issue was mitigated by having a curved rod connected to the spine rod using crosslinks in our system.
Our findings illustrate that fork plate system reduction of the range of motion of the sacrectomy model was comparable with the dual iliac screw construct. However, fork plate system showed a higher factor of safety and hence a lesser chance of failure compared to dual iliac screw system. The lower stress profile on the plate makes it more favorable as compared with a construct with crosslinks.
The only disadvantages are that the need to custom design for each case and the need for a high level of technical accuracy in the screw placement across the tuning fork plate. These operations need careful pre-operative planning for the levels that can be instrumented, the availability of the hooks, rib cradles, cross connectors and the pedicle screw-based instrumentation. The operation room time and blood loss are commensurate with the length of the incision and extent of the instrumentation. This surgery is performed in carefully pre-selected patients. The implant can be used in all ages and has been piloted in a small series of patients.
Conclusions
Instrumentation in the face of lumbo-sacral deficiency either with tuning fork plate or the dual iliac screw fixation reduced the range of motion of spine. Comparisons of segmental range of motion between the dual iliac screw fixation and tuning fork plate fixation did not demonstrate a significant difference. However, stresses on the fork plate fixation were lower (22% to 45%) than dual screw fixation which might lead to less implant failure in the fork plate fixation constructs.
In conclusion, both fixation devices had same performance in terms of motion reduction at spine levels. However, based on predicted implant stresses there was a lesser chance of implant failure in the fork plate fixation, compared to the dual iliac screw system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported in part by NSF Industry/University Cooperative Research Center at The University of California at San Francisco and The University of Toledo.