
Abstract
Study Design:
Broad narrative review.
Objective:
To review and summarize the current literature on the cost efficacy of performing ACDF, lumbar discectomy and short segment fusions of the lumbar spine performed in the outpatient setting.
Methods:
A thorough review of peer- reviewed literature was performed on the relative cost-savings, as well as guidelines, outcomes, and indications for successfully implementing outpatient protocols for routine spine procedures.
Results:
Primary elective 1-2 level ACDF can be safely performed in most patient populations with a higher patient satisfaction rate and no significant difference in 90-day reoperations and readmission rates, and a savings of 4000 to 41 305 USD per case. Lumbar discectomy performed through minimally invasive techniques has decreased recovery times with similar patient outcomes to open procedures. Performing lumbar microdiscectomy in the outpatient setting is safe, cheaper by as much as 12 934 USD per case and has better or equivalent outcomes to their inpatient counterparts. Unlike ACDF and lumbar microdiscectomy, short segment fusions are rarely performed in ASCs. However, with the advent of minimally invasive techniques paired with improved pain control, same-day discharge after lumbar fusion has limited clinical data but appears to have potential cost-savings up to 65-70% by reducing admissions.
Conclusion:
Performing ACDF, lumbar discectomy and short segment fusions in the outpatient setting is a safe and effective way of reducing cost in select patient populations.
Introduction
As the United States healthcare system has proven to be the most expensive of all developed countries, 1 changes that aim to increase cost efficiency of diagnosis and management of common medical conditions are being implemented. Outpatient surgery has become increasingly popular in specific fields including eye surgery, soft tissue cases, arthroscopy and now arthroplasty. Sweden, being a prime example of a cost-effective healthcare system, is now performing more than half of their surgeries in the outpatient setting, and the US is following suit. 2 As the demand for surgery outweighs many hospitals capacity to supply operative time, ambulatory surgery centers (ASCs) have increased by 60%, followed by an increased in outpatient surgeries in the Medicare population 40%. 3,4 Additionally, ASCs are able to perform the same procedure as a hospital at a lower cost by accepting a lower facility reimbursement fee. 5,6
Spine surgery is a high expenditure of the current US healthcare system with nearly 90 billion dollars per year spent on the diagnosis and management of back and neck pain. 7 As such, spine surgery is a major target of the healthcare system to reduce overall cost. A primary method for reducing this cost has been shifting operations from the inpatient to the outpatient setting, which may reduce the cost by 43%. 8 Routine spine procedures safely performed in an outpatient setting are being increasingly reported. 9,10 As spine surgeons in the United States aim to reduce costs of procedures through outpatient surgery in carefully selected patients, understanding of the current literature is essential. Thus, the purpose of this article is to discuss the cost efficacy of performing anterior cervical discectomy and fusions (ACDFs), lumbar microdiscectomy, and short segment fusions of the lumbar spine in the outpatient setting.
Results
Anterior Cervical Discectomy and Fusion (ACDF)
Although ACDFs are relatively safe procedures, the complications of these procedures can be potentially devastating. 11,12 Ranging from the rare but dreaded esophageal perforation with a 0.1% mortality rate, to the less severe postoperative dysphagia of up to 9%. However, the most concerning is postoperative hematoma which can threaten the airway occurring in up to 6% of cases. 13 Given this complication profile, the safety of performing an ACDF in an outpatient setting requires careful assessment.
ACDFs have been increasingly performed on an outpatient basis since 1996, when it was first introduced as a feasible option by Silvers et al. 14 Further early studies confirmed the safety of performing 1-2 level ACDFs on a carefully selected patient population. 15 -18 These studies identified a very low rate of complications of up to 2% and only 1 patient converted to inpatient status for monitoring. However, as the largest sample size in these studies was 99 patients treated on an outpatient basis, they lacked power to demonstrate any statistical difference between the outpatient and inpatient cohorts. Following this, National Surgeon Quality Improvement Program (NSQIP) data was utilized to assess the safety of this new trend. After performing propensity score matching and multivariate regression analysis of 7288 cases, McGirt el al. reported that the outpatient cohort had 58% less major morbidity events and 80% lower rate of reoperation within 30 days. 19 Adamson et al. followed this with a cohort study of 1000 consecutive patients classified as American Society of Anesthesia (ASA) I or II undergoing 1-2 level ACDFs prior to noon in an ACS and 484 patients undergoing ACDF in an academic hospital center. With only 8 patients requiring admission after a 4-hour observation period, and no differences in 30- and 90- day reoperation and readmission rates between the 2 groups. 20
Given the safety profile of outpatient ACDF in carefully selected patient populations, the promise of cost savings seems possible. 21 In analyzing statewide databases of New York, California and Florida, Purger et al. found that overall charges of outpatient ACDF was significantly lower than that of inpatient ACDF ($33 362.51 vs. $74 667.04). 22 This was further supported by a meta-analysis of 16 studies including multiple outpatient spine surgeries that reported a mean cost savings of $121 392.72. 23
Notably, outpatient ACDF is often selectively performed in healthier patients. Mundell et al. found that patient selection may bias outpatient surgery to have superior results to inpatient surgery. 23 They reported that younger patients undergoing outpatient ACDF had significantly less cost savings compared to those older than 65 years old. The cost savings for the outpatient surgery in an older population is likely due to fewer comorbidities than their inpatient counterparts that may necessitate surveillance. Although age plays a major role, medical comorbidities seem to be the most important factors in complications. Purger et al. studied these differences by stratifying the outpatient and inpatient ACDF groups by Charlson comorbidity index (CCI). Even when matched, the outpatient group resulted in lower ED visits, readmissions and reoperations within 30 days. Similarly, patients undergoing ACDF in the outpatient setting had higher satisfaction than their inpatient counterparts. 22
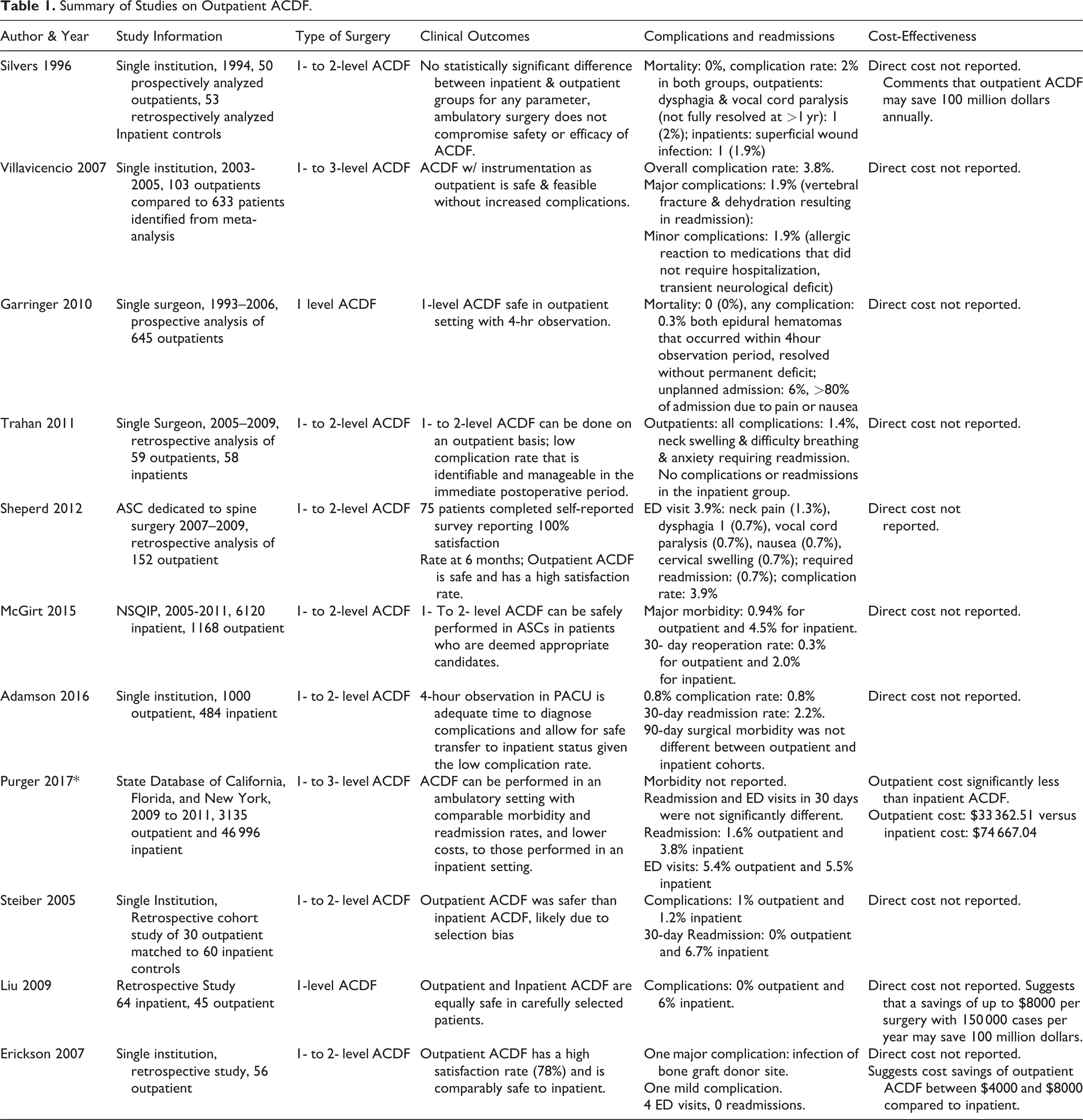
As stated, in the appropriately screened and selected patients, the authors feel primary single, and possibly 2-level ACDFs can be performed safely and effectively in the outpatient setting. There is recent literature to guide appropriate patient selection, suggesting patient’s should be under 65 years old, BMI less than 35, ASA 2 or lower and no history of coagulopathies, bleeding disorders, TIAs or CVAs. There are also day of post-operative protocols and goals outlined which selected patient’s must meet in order to be considered for same day discharge including no operative complications, hemodynamic stability in the recovery room, no respiratory alarm symptoms, and so on (Shenoy et al)19?. Patient’s who fail to meet ALL of these criteria should not be considered to undergo ACDF in the outpatient setting. Descriptive information regarding studies examining outpatient ACDF are listed in Table 1.
Summary of Studies on Outpatient ACDF.
Lumbar Discectomy
Lumbar discectomy is the most commonly performed spine surgery in the United States with over a quarter million cases a year. 24 -26 There is an overwhelming body of evidence supporting the efficacy of lumbar discectomy in relieving pain and improving function, with a reported 75-90 percent success rate. 27 Additionally, lumbar discectomy can be performed in a number of different ways. These range from the classic open procedure to microscopically assisted discectomy to the novel endoscopic microdiscectomy approach. Minimizing the invasiveness of the open procedure has assisted in performing lumbar microdiscectomy in an outpatient setting for over 20 years. 28
However, lumbar microdiscectomy has the potential for costly complications. Durotomy, deep infection, and hematoma are the most common complications that ultimately lead to hospital admission, reoperation and increased cost. 29 In order to safely perform these procedures in an outpatient setting, protocols for patient selection may reduce these risks. 30 In a retrospective cohort study, Bekelis et al. found male gender, private insurance, lower CCI, and being at a higher volume center to be associated with improved success in performing outpatient lumbar discectomy. 31
As many variables effect the success of outpatient lumbar discectomy, the cost can vary greatly. 32 Major driving forces of the cost variability are obesity, history of myocardial infarction, opioid independence, length of surgery, length of hospital stays, and time in rehabilitation centers post-operatively. 32 Some suggest the grand majority of cost occurs from the length of surgery and admission to hospital and rehabilitation centers postoperatively. Readmission within the 90-day global period also accounted for 36% of the overall cost. 32 It is therefore important to recognize that lumbar microdiscectomy has similar complication rates and readmission rates when performed in the inpatient setting, outpatient setting at an ASC, or hospital based outpatient setting. In a recent insurance based database study, Malik et al. reported that lumbar microdiscectomy performed at an ASC compared to a hospital based outpatient setting (HOS) procured a total cost saving of $2000 and $3500 for Medicare and Commercial Insurance respectively. 33 This further supports that identifies that hospital operative fees are greater than those of ASCs even without the additional cost of inpatient admission.
Ultimately, primary lumbar microdiscectomy can be safely performed in an outpatient setting in a select patient population. Performing these procedures with recuperation at home is safe and effective at reducing cost without compromising patient satisfaction. 34 As is the case for ACDFs, appropriate patient selection is of the utmost importance when considering performing lumbar microdiscectomies in the ambulatory setting. To date however, there is a paucity of evidence-based literature dedicated to guiding appropriate patient selection. Generally, the authors suggest following the selection guidelines laid out above for ACDFs when choosing patients to undergo lumbar microdiscectomies in the outpatient setting.
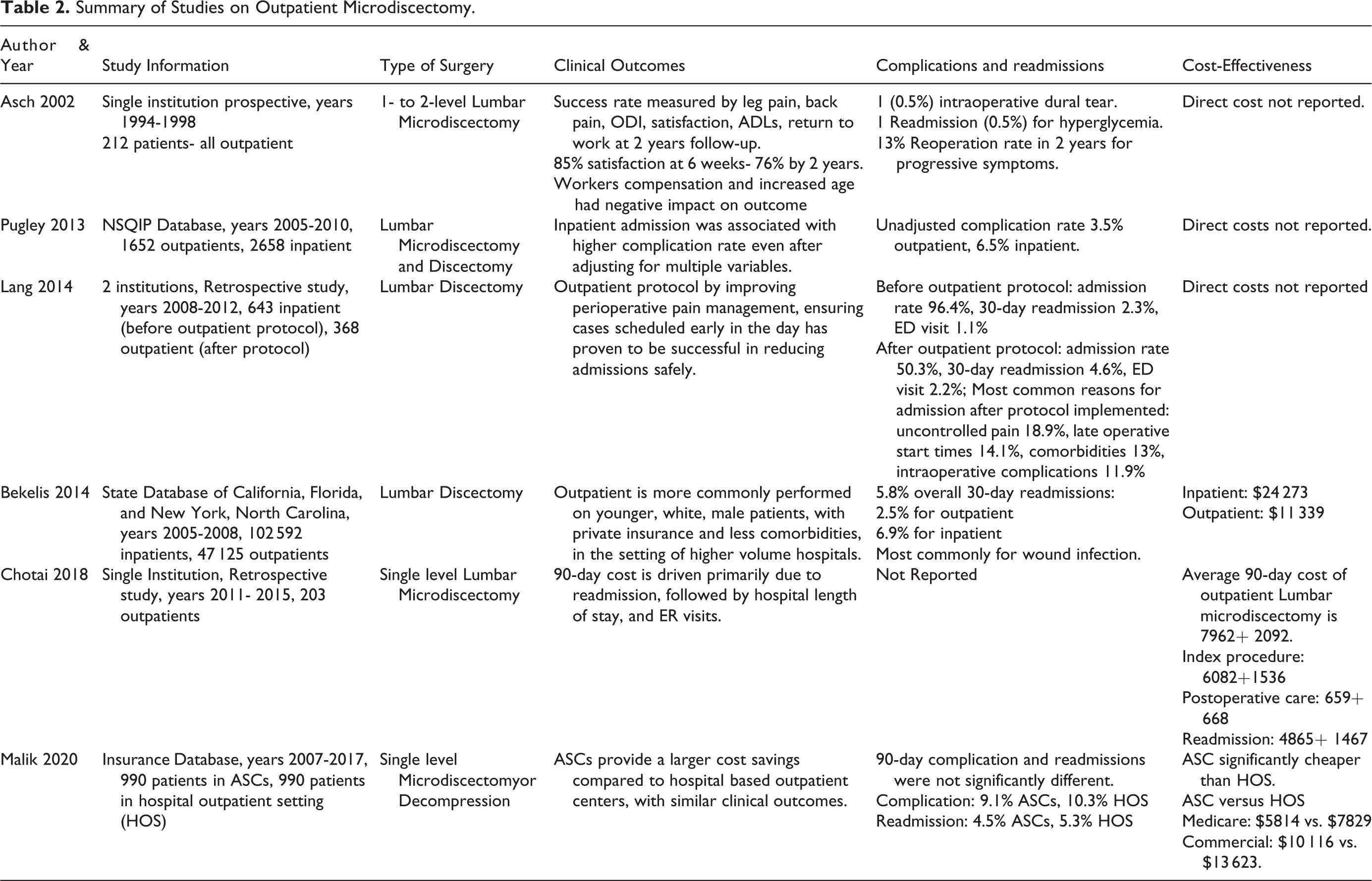
Of note, there is very little data regarding performing revision discectomy in the outpatient setting. As revision discectomy can have similar or higher complication rate, this decision should ultimately be left to the surgeon’s discretion. 35,36 Descriptive information regarding studies examining outpatient lumbar discectomy are listed in Table 2.
Summary of Studies on Outpatient Microdiscectomy.
Short Segment Fusion
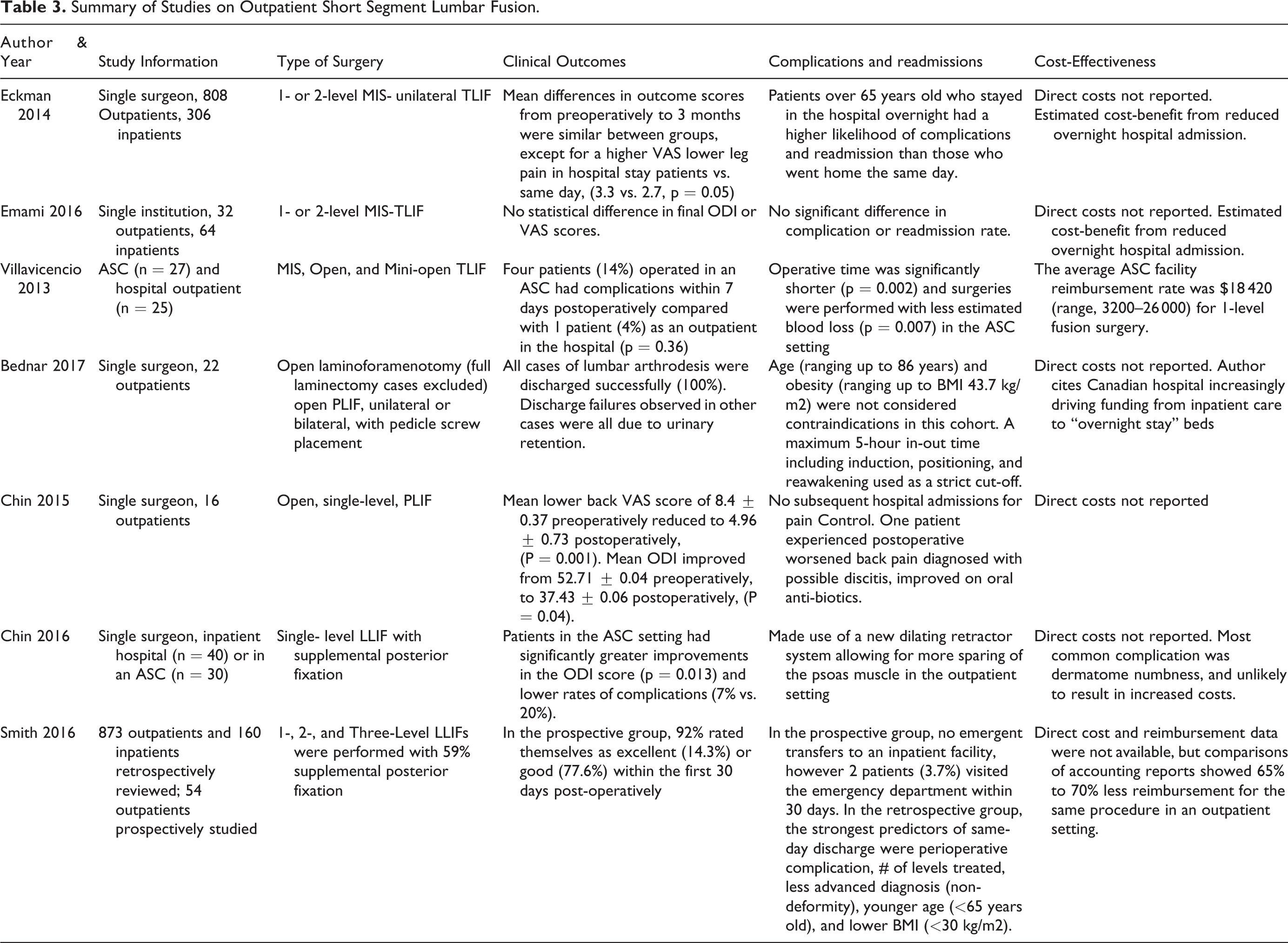
While the main barrier to performing ACDFs in the outpatient setting may be the complication profile, lumbar fusions offer a different set of challenges. The increased morbidity from a more invasive procedure directly tests our ability to control post-operative pain and decrease recovery time. Fear of increased readmissions and revisions associated with open approaches for lumbar fusion have previously limited the adoption into the outpatient setting. 37,38 However, the number of lumbar fusions has increased from 5% of outpatient spine surgeries in 1994 to 17% in 2006. 39 Table 3 summarizes the literature on short-segment fusions performed as same-day surgery.
Summary of Studies on Outpatient Short Segment Lumbar Fusion.
Historically, standard open posterior surgical approaches for lumbar fusion, such as posterolateral fusion (PLF) and posterior/transforaminal lumbar interbody fusion (PLIF/TLIF), are associated with significant muscle dissection, increased blood loss, extensive pain control requirements, use of urinary catheters, and surgical drains. All of which create obstacles for early mobilization, including patients’ fear of movement and injury, let alone same-day discharge. 39 However, minimally invasive surgery (MIS) techniques for lumbar fusion, such as the MIS TLIF, have demonstrated reduced blood loss, decreased pain control requirements, avoidance of patient controlled analgesia pumps, urinary catheters, and surgical drains, and reduced length of stay. 40 -42 Cheng et al. estimated their own ability to shorten inpatient hospitalizations via MIS TLIFs compared with open (4.8 days vs. 6.05, respectively, p = 0.006) translated to an average cost reduction of $3885 per patient based on the average cost of 1 day on an acute care inpatient ward ($2590). 43 Further, long-term outcomes such as patient satisfaction and fusion rates are similar to conventional open approaches. 44,45 As MIS techniques and enhanced recovery after surgery (ERAS) protocols advance, properly selected patients undergoing short segment lumbar fusions have been able to be successfully transitioned to the outpatient setting with large cost-saving potential. 38,46 -51
In one of the largest case series, Eckman et al. reported on their 10-year experience of discharging patients the same-day after an MIS TLIF. 48 Among a total 1114 procedures performed by a single surgeon, 808 were discharged same-day with an overall 73% same-day discharge rate and similar improvement for scores for function and pain in both groups on follow-up. Emami et al. likewise reported on 96 patients undergoing MIS TLIF with 32 (33%) discharged same-day. 49 In both, the outpatient cohort was significantly younger, had less comorbidities, and had a lower rate of transfusions and intraoperative complications confounding comparative analysis.
While the MIS TLIF technique offers potential, it is often associated with longer operating times that is counter-productive to the ambulatory setting. Villavicencio et al documented efforts to transition TLIFs to at an ambulatory surgery center (ASC) and found that the MIS or percutaneous approach had the longest operative times (245 minutes), followed by open (175 minutes), and a mini-open approach (131 minutes). 51 The average ASC facility reimbursement rate was $18 420 (range, 3200–26 000) for 1-level fusion surgery, compared with the average inpatient cost of $33 784, range from $27 984 to $42 082, with 2-4 days length of stay. 52 Accordingly, open lumbar fusion techniques still have a potential to be shifted to outpatient surgery. While not technically same-day, Bednar described 22 patients discharged after an overnight-stay, totaling less than 24 hours, following standard open lumbar fusions. 46 This was accomplished through a well-defined comprehensive protocol for patient selection, screening, and optimization, including a maximum 5-hour “in-out” time for the operating room. Chin et al. also reported experience with an open PLIF procedure in the outpatient setting. 47 Sixteen consecutive patients were able to be discharged same-day (versus 23-hour observation) without a drain in all patients. Thus, with proper planning traditional open or more invasive procedures may still be safely “fast-tracked” without requirement for formal hospital inpatient admission.
More recent publications include moving lateral lumbar interbody fusions (LLIF) to the ambulatory setting. In a retrospective comparative analysis of 70 patients, outcomes and complications were evaluated for LLIF in an inpatient hospital (n = 40) or in an ASC (n = 30). 53 There were no significant differences in baseline demographics or VAS back pain scores, however patients in the ambulatory setting had significantly greater improvements in the ODI score (p = 0.013), lower rates of complications (7% vs. 20%), and had shorter surgical times (224 ± 103 vs. 97 ± 49 min, p = 0.005). While no multi-variate analysis was performed, these results suggest improved efficacy and safety in the outpatient setting; although in a separate publication the same authors report use of a modified trans-psoas technique for use in the outpatient setting that may account for the improved results. 54 Smith et al. also demonstrated that same-day discharge after LLIF is well tolerated with results from 1033 patients retrospectively reviewed and 54 patients in a prospective arm. 50 Among the prospective patients there were no transfers to an inpatient facility, however 2 additional patients (3.7%) visited the emergency department within 30 days—one <24-hour admission for urinary retention, and one admission for pain control after a three-level fusion.
Reports of same-day discharge after lumbar fusion have overall limited clinical data regarding its safety and efficacy, but appears to have potential in cost-savings by reducing admissions. 55 As all the techniques described require a high degree of surgical expertise, even further consideration in terms of patient selection and a vast experience with these procedures is necessary to prevent complications. Moreover, in addition to ideal patients and masterful technique, advanced anesthesia and pain control protocols are necessary given the increased invasiveness that comes with lumbar fusion procedures. 56 Indeed, a new frontier of rapid recovery after lumbar fusion is to avoid general anesthesia altogether with the “awake TLIF,” which employs several key innovations including conscious sedation and long-acting local analgesia. 57,58
Future studies are needed to standardize the appropriate patient screening and selection criteria for consideration of ambulatory short-segment lumbar fusions. These authors believe that, at a minimum, potential patients would meet the criteria for the “less invasive” spine procedures (i.e. ACDF and lumbar microdiscectomy) outlined above which are already commonly being performed in the ambulatory setting.
Conclusion
The increasing pressure of cost-effective treatment modalities have caused spine surgeons to search for ways of safely reducing the cost of common procedures. ACDF, lumbar discectomy, and short segment fusions are commonly performed spine surgeries with potential to move to the ambulatory setting. There is increasing literature to support this transition as a safe and effective way of reducing cost in select patient populations. Ultimately, the ability to perform these routine procedures in the ambulatory setting is multifactorial and should be left to each individual surgeon’s discretion.
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr. Cho has financial relationships with Corentec (paid consultant), Medtronic (paid consultant), Globus (paid consultant), and Zimmer (paid consultant, research support). None of the remaining authors have any financial interests or affiliations with institutions, organizations, or companies relevant to the manuscript. None of the authors received payment or support in kind for any aspect of the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by a grant from AO Spine North America.