
Abstract
Study Design:
Retrospective chart review with matched control.
Objective:
To evaluate the indications and complications of spine surgery on super obese patients.
Methods:
A retrospective review assessed super obese patients undergoing spine surgery at a level-1 trauma and spine referral center from 2012 to 2016. Outcomes were compared to age-matched controls with body mass index (BMI) <50 kg/m2. The control group was further subdivided into patients with BMI <30 kg/m2 (normal) and BMI between 30 and 50 kg/m2 (obese).
Results:
Sixty-three super obese patients undergoing 86 surgeries were identified. Sixty patients (78 surgeries) were in the control group. Age and number of elective versus nonelective cases were not significantly different. Mean BMI of the super obese group was 55 kg/m2 (range 50-77 kg/m2) versus 29 kg/m2 in the controls (range 20-49 kg/m2). Fifty-two percent of surgeries were elective, and the most common indication was degenerative disease (39%). Compared with controls, super obese patients had a higher complication rate (30% [n = 19] vs 10% [N = 6], P = .0055) but similar 30-day mortality rate (5% vs 5%), a finding that was upheld when comparing super obese with each of the control group stratifications (BMI 30-50 and BMI <30 kg/m2). The most common complication among super obese patients was wound dehiscence/infection (n = 8, 13%); 2 patients’ surgeries were aborted. Complication rates for elective surgery were 21% (n = 7) for super obese patients and 4% (n = 1) for controls (P = .121); complication rates for nonelective procedures were 40% (n = 12) and 14% (n = 5), respectively (P = .023).
Conclusion:
The complication rate of spine surgery in super obese patients (BMI ≥ 50 kg/m2) is significantly higher than other patients, particularly for nonelective cases.
Introduction
Obesity is an epidemic with widespread individual and public health consequences. According to the Centers for Disease Control and Prevention data published in 2015, the prevalence of obesity was just over 36% in adults and 17% in youth, with the prevalence consistently increasing from 1999 to 2014. 1 In adults, obesity is defined as a body mass index (BMI) of greater than or equal to 30 kg/m2, with BMI calculated as mass in kilograms divided by height in meters squared. Although the World Health Organization classifies obesity into 3 classes (with class III obesity representing patients with BMI ≥40 kg/m2), the rising incidence of extreme obesity has led researchers to further stratify into class IV (super-obesity) with BMI 50 to 59.9 kg/m2, and class V (super-super-obesity) with BMI >60 kg/m2. Increased BMI is associated with cardiovascular disease, diabetes, musculoskeletal disorders, and even some cancers, with annual medical costs in the billions of dollars. 2
The obese population presents particular challenges to the spine surgeon. Studies have demonstrated an association between obesity and back pain, and spine surgeries in the obese are associated with increased perioperative complications, morbidity, and mortality.3-17 There are no studies in the literature, however, specifically addressing the 2 highest subclasses of obesity and those patients’ indications for surgery and outcomes. The purpose of this study was to quantify and elucidate the risk of surgery in super obese (class IV and V) patients when compared to those with a BMI less than 50 kg/m2, including both elective and nonelective cases.
Methods
Institutional review board approval (Protocol #1 611 340 464) was granted; since the study was retrospective in nature, patient consent was not required. The authors performed a chart review on patients with class IV and V obesity who underwent spine surgery by neurosurgical and orthopedic staff from 2012 to 2016 at a level-1 trauma and spine referral center. All patients, including those with polytrauma or multiple comorbidities, were included and reviewed via electronic medical records. BMI at the time of hospital admission was verified, and patient age, gender, operative diagnosis, and procedure were noted, including whether the procedures were elective in nature. In addition, complications and mortality were assessed via review of the inpatient hospital record and outpatient follow-up documentation. As a control, nonobese and class I through III obese patients were also studied and the same measures were recorded. With statistical consultation, the control group was selected based on pre hoc power analysis with a necessary sample size estimated with alpha of .05 and power of 0.8 to obtain 1:1 age-matched controls with BMI < 50 kg/m2 from the same time period, operated on in consecutive fashion. The BMI < 50 kg/m2 control group was further stratified to identify obese control patients with BMI 30 to 50 kg/m2 and nonobese patients with BMI < 30 kg/m2. Chi-square and Fisher’s exact tests were used to assess for significant differences among the categorical variables (gender, mortality, complications). Continuous variables (age, BMI, number of surgeries) were evaluated with independent Student t test. Comparisons were made between the combined class IV and V obese patients and their BMI < 50 kg/m2 controls as well as among the elective and nonelective populations within the BMI ≥ 50 kg/m2 cohort. The primary outcome of the study was the difference in complications between the super obese and non-super obese groups.
Results
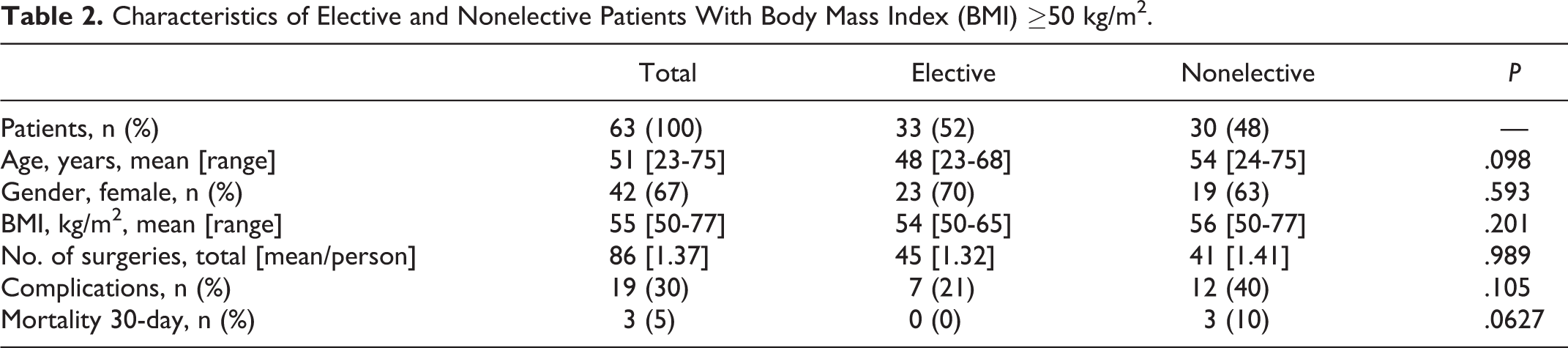
We identified 63 patients in the super obese group (BMI ≥ 50 kg/m2) who underwent 86 surgeries and 60 patients (78 surgeries) in the control group (BMI <50 kg/m2) (Table 1). Mean BMI of the super obese group was 55 (range 50-77) kg/m2 compared with 29 kg/m2 in the control group (range 20-49 kg/m2). Age and the number of elective and nonelective cases were not significantly different between groups. Patients in the super obese group undergoing elective surgery did not vary significantly in baseline characteristics from those undergoing nonelective procedures (Table 2). Elective surgeries included those performed for primarily degenerative pathology (eg, stenosis, radiculopathy, adjacent segment disease), although other miscellaneous elective cases were also included (spinal cord stimulator placement, coccygectomy, and removal of symptomatic spinal instrumentation). Nonelective surgeries were performed for myelopathy, cauda equina syndrome, unstable fractures, instrumentation failure, infection, tumors, or spinal cord compression. Super obese patients had a significantly higher percentage of index surgeries for infection compared with controls (19% vs 4%, respectively; P = .0022), although there was no difference seen for any other indication when comparing the 2 groups (Table 3). Fusion procedures (eg, anterior cervical, posterior cervical, posterior thoracic/thoracolumbar, and posterior lumbar fusions) predominated in both the super obese and control cohorts; however, posterior lumbar decompression was the most common procedure in the super obese group (18%) while posterior cervical fusion was the most common in controls (22%; Table 4). Super obese patients underwent a statistically significantly greater number of washout and irrigation and debridement surgeries compared with controls (13% vs 4%, respectively; P = .0452), reflecting the higher rate of infection as the surgical indication, whereas controls underwent a statistically significantly greater number of posterior cervical fusions (22% vs 7%; P = .0053). There were no significant differences between the groups with regard to the incidence of the other types of surgeries. Sixteen patients in the super obese cohort underwent multiple procedures.
Comparison of Super Obese (Body Mass Index [BMI] ≥50 kg/m2) Patients With Control Patients.
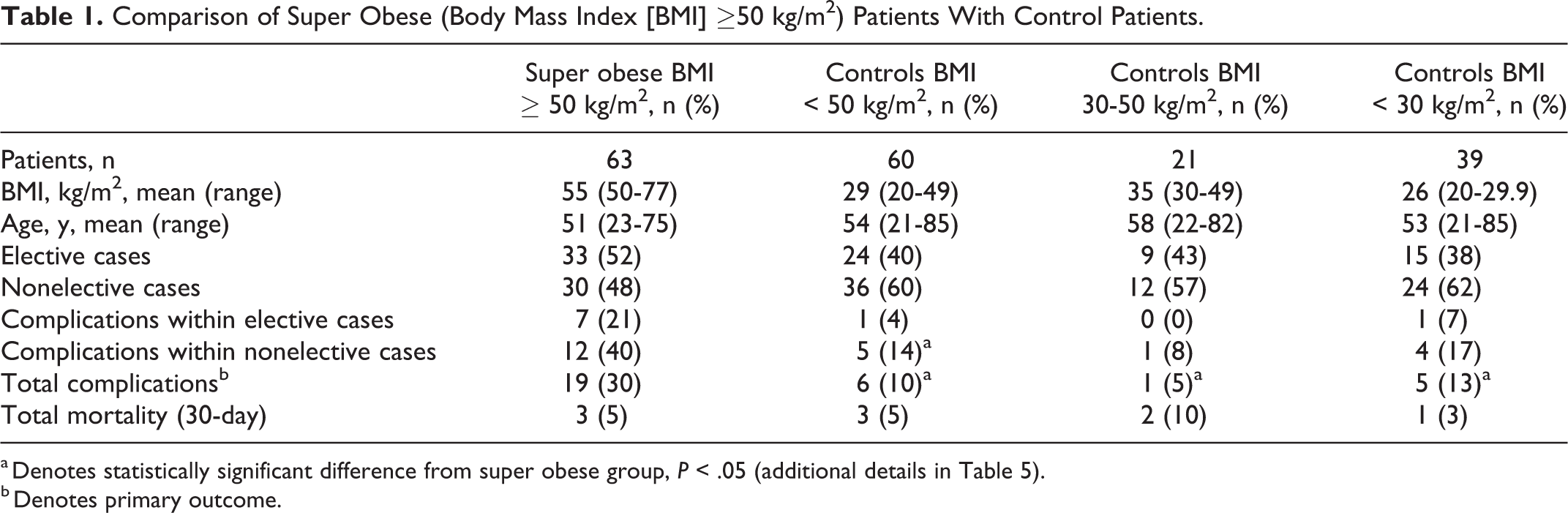
a Denotes statistically significant difference from super obese group, P < .05 (additional details in Table 5).
b Denotes primary outcome.
Characteristics of Elective and Nonelective Patients With Body Mass Index (BMI) ≥50 kg/m2.
Indications for Spine Surgery in Patients With Body Mass Index (BMI) ≥50 Versus BMI < 50 kg/m2 Controls.
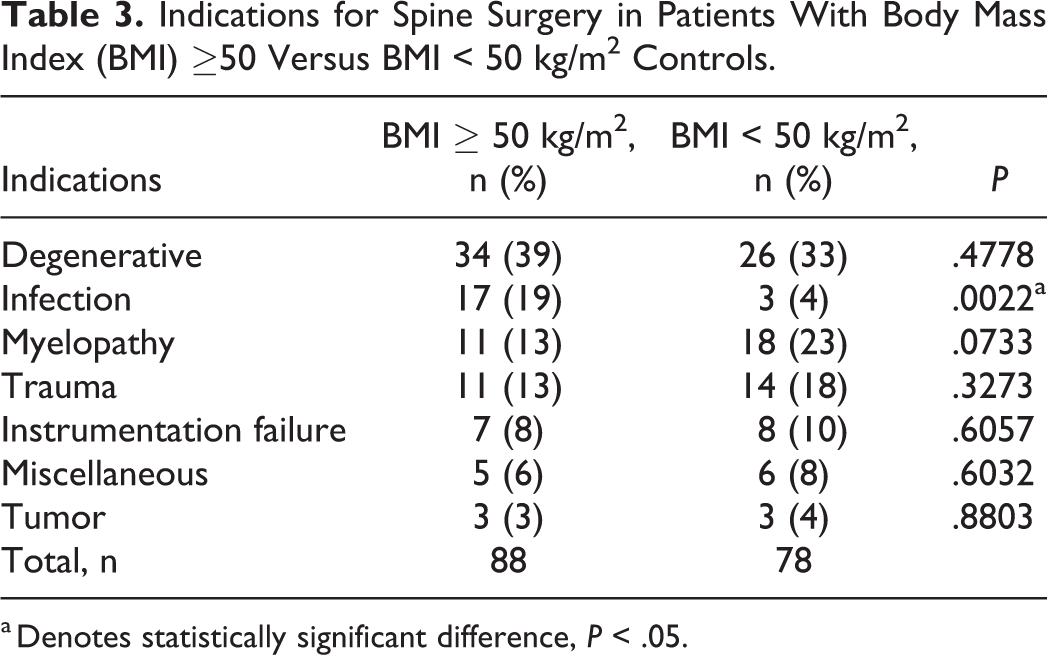
a Denotes statistically significant difference, P < .05.
Type of Surgery in Patients With Body Mass Index (BMI) ≥50 Versus BMI < 50 kg/m2 Controls.
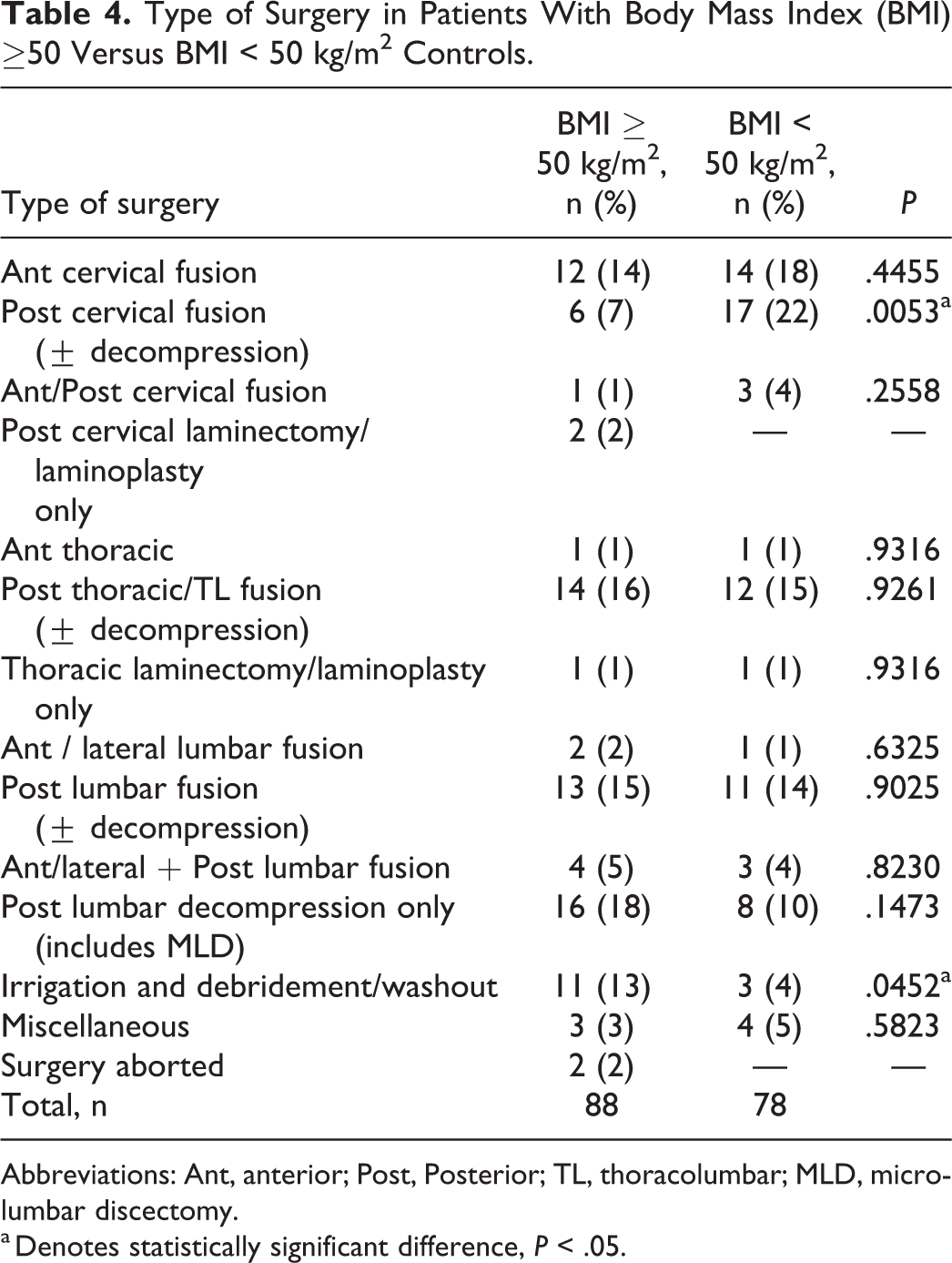
Abbreviations: Ant, anterior; Post, Posterior; TL, thoracolumbar; MLD, microlumbar discectomy.
a Denotes statistically significant difference, P < .05.
The super obese group had a significantly higher complication rate than non–super obese controls (30% vs 10%, respectively; P = .006), particularly within the nonelective subgroup of patients (40% vs 14%, respectively; P = .02 with odds ratio 4.1 and number needed to harm of 4; Table 1). Although the rate of complications for elective cases was nearly 5 times higher for super obese patients, this finding was not statistically significant (21% in super obese vs 4% in non–super obese; P = .12). Further stratification of the BMI < 50 kg/m2 control group was performed to select obese control patients with BMI 30 to 50 and nonobese patients with BMI < 30 kg/m2. Again, the super obese group had a significantly higher complication rate than the obese BMI 30 to 50 kg/m2 controls (30% vs 5%, respectively; P = .018) and nonobese BMI < 30 kg/m2 controls (30% vs 13%, respectively; P = .044; Tables 1 and 5). Among elective surgeries, complication rates were 21% (n = 7) for super obese patients, compared with 4% (n = 1) for BMI < 50 kg/m2 controls (P = .121), 0% (n = 0) for BMI 30 to 50 kg/m2 controls (P = .313), and 7% (n = 1) for BMI < 30 kg/m2 controls (P = .406; Table 1). Complication rates for nonelective procedures were 40% (n = 12) for super obese patients, compared with 14% (n = 5) for BMI < 50 kg/m2 controls (P = .023), 8% (n = 1) for BMI 30 to 50 kg/m2 controls (P = .067), and 17% (n = 4) for BMI < 30 kg/m2 controls (P = .078; Table 1).
Statistical Comparisons of Complications Risk Between Super Obese and Control Patients.
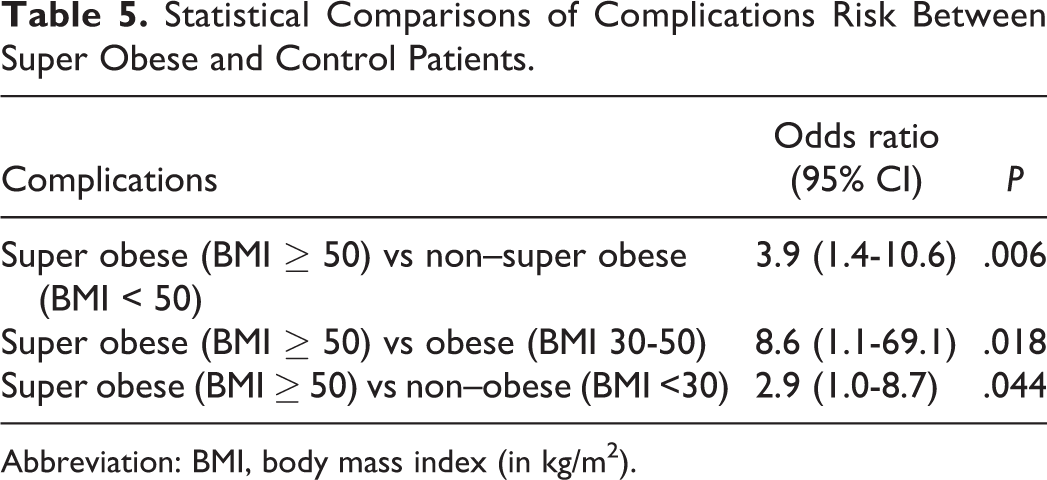
Abbreviation: BMI, body mass index (in kg/m2).
Mortality rate was not statistically different among the groups and was noted to be 5% (n = 3) in the super obese group, 5% (n = 3) in the BMI < 50 kg/m2 controls (P = .951), 10% (n = 2) in the BMI 30 to 50 kg/m2 controls (P = .595), and 3% (n = 1) in the BMI < 30 kg/m2 controls (P = .578). The complication rate of nonelective surgery was greater than elective surgery for the super obese group and all permeations of the control group, although not significantly (BMI ≥ 50, P = .17; BMI < 50, P = .39; BMI, 30-50, P = .38; BMI < 30, P = .63). All mortalities involved nonelective cases.
The most common complications among the super obese group were wound dehiscence and/or infection (n = 8, 13% of patients, 42% of complications); deep vein thrombosis (n = 3, 5%, 16%, respectively), and instrumentation failure (n = 3, 5%, 16%, respectively) (Table 6). In comparison, only 1 patient in the non–super obese control group had wound dehiscence (2% of patients, 17% of complications, P = .019) and only 1 patient had instrumentation failure (2%, 17%, respectively, P = .333; Table 6). Two of the 88 planned surgical cases in super obese patients were aborted intraoperatively prior to incision due to anesthetic complications, including inability to ventilate in prone position, and desaturations resulting from bilateral pulmonary emboli. The 6 postoperative complications in the control group included wound dehiscence, myocardial infarction, loss of fixation, need for additional fixation, hematoma, and postoperative weakness (Table 6).
Comparison of Complications in Patients With Body Mass Index (BMI) ≥ 50 Versus BMI < 50 kg/m2 Controls.
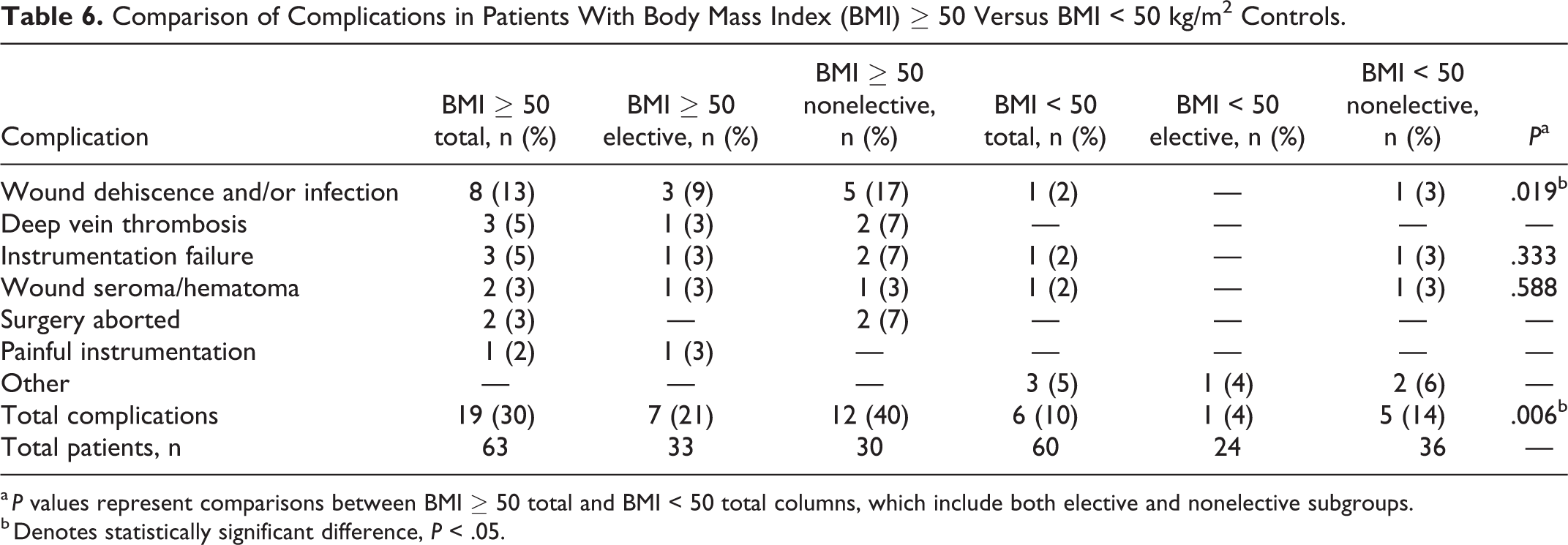
a P values represent comparisons between BMI ≥ 50 total and BMI < 50 total columns, which include both elective and nonelective subgroups.
b Denotes statistically significant difference, P < .05.
Discussion
Recent projections indicate that the prevalence of obesity will continue to increase, with nearly 1 in 4 adults projected to be BMI ≥ 35 kg/m2 by 2030. 18 However, data specifically focusing on patients with BMI ≥ 40 kg/m2 is lacking across all specialties. 19 This study targets an even more focused population, patients with class IV (super-obesity; BMI 50-59.9 kg/m2) and class V (super-super-obesity; BMI >60 kg/m2) obesity. These patients present unique challenges for spinal diagnosis and treatment, yet no literature specifically addresses this population. Several studies have correlated obesity as a whole with worse outcomes. Kalanithi et al, 11 in a large retrospective study of elective spine patients, reported that morbid obesity (BMI > 40 kg/m2; class III obesity) was associated with 97% higher in-hospital complication rates across nearly all complication types (wound, cardiac, renal, pulmonary, etc) as well as higher mortality, average hospital cost, and length of stay. A subset of studies stratifies obesity classes to compare complication risks, but again, none explicitly delineate class IV and V patients. Buerba et al 14 performed a large retrospective study and demonstrated that class I, II, and III obese patients had higher complication rates after lumbar surgery compared with nonobese patients; complication rates increased substantially with each class, particularly for the class III obesity subpopulation (BMI > 40 kg/m2), and obese patients overall had longer operative times, extended hospital stays, and increased risk for wound, urinary, and pulmonary complications. Higgins et al 15 found significant associations between obesity and longer anesthesia times, longer surgical times, increased medical complications, increased wound complications, and increased overall cost of care, with the findings becoming more pronounced in the subpopulation with BMI > 40 kg/m2. McGuire et al 6 similarly compared non-obese patients to various classes of obese patients and demonstrated that obese patients with BMI > 35 kg/m2 had longer operative times and increased infection after elective lumbar spine surgeries. 6 Patel et al 8 performed a retrospective study and demonstrated the probability of a significant complication was related to BMI; the chance of a significant complication was 14% with a BMI of 25 kg/m2, 20% with a BMI of 30 kg/m2, and 36% with a BMI of 40 kg/m2. Finally, Marquez-Lara et al 12 demonstrated that the risk for postoperative complications such as deep vein thrombosis, wound infection, pulmonary embolism, urinary tract infection, acute renal failure, and sepsis increase in higher obesity classes. The current study is the first to isolate patients with class IV and V obesity. We demonstrated that these patients are even more likely to have poorer outcomes, and as such, require careful counseling as well as consideration of potential alternative treatments (including referral for bariatric procedures) before elective procedures.
While there are currently no data for direct comparison in this patient population, the data available seem to follow the trend of increasing BMI leading to increased surgical risk.11-15 Puvanesarajah et al, 13 for example, assessed patients older than 65 years undergoing 1- or 2-level spine surgery for degenerative conditions and demonstrated a rate of 14.2% for medical complications and 6.3% for wound complications in patients with BMI 30 to 39.9 kg/m2 (class I and II), which increased to 20.3% and 10.4%, respectively, in patients with BMI greater than 40 kg/m2 (class III). Class IV and V obese patients in the present study had a 30% complication rate, with 42% of those being wound dehiscence and/or infection and 63% of them occurring in nonelective patients. These findings are expectedly increased compared with other studies not only due to the focus on the subpopulation of class IV and V obese patients but also due to the inclusion of both elective and nonelective patients, which several large database studies exclude. The mortality rate for class IV and V patients in the present study was 5%; all deaths (n = 3) occurred in nonelective patients and the mortality rate was identical to our non–super obese control group. When comparing just the elective subpopulation of the class IV and V patients, the 0% mortality rate was similar to that in the literature which ranges from 0% to 0.5%.6,12,14,20 These numbers, however, should be interpreted cautiously given the limited number of patients and deaths (ie, 6 deaths across both super obese and control patients). Although other studies primarily focus on the elective, healthier obese patients, the trend is nonetheless evident that a higher BMI subclass is associated with increased morbidity and perioperative complications. Compared with BMI < 50 kg/m2 controls, the super obese cohort had a statistically significantly greater number of surgeries that included irrigation, debridement, and washout for the indication of infection.
The present study quantifies the risk of surgery for the super obese population. The high incidence of complications emphasizes the need for spine surgeons to consider and treat this subpopulation separately from other obese patients. This conclusion is bolstered by the fact that that average BMI in the control group (BMI < 50 kg/m2) reported here was 29, putting the control group in the “overweight” category and on the borderline of obese. Furthermore, when the control group was stratified to compare super obese patients with obese patients with BMI 30 to 50 kg/m2 or nonobese patients with BMI < 30 kg/m2, the findings remained consistent, with significantly higher complications in the super obese group.
These data should help in counseling patients preoperatively, particularly for elective cases in which preoperative weight loss and/or bariatric surgery may be a reasonable prerequisite. Bariatric surgery and weight loss has been associated with decreased complications and length of stay for patients later undergoing spine surgery, as well as improvements in back pain, radicular pain, and myelopathy which may help avoid spine surgery altogether. 21 Not all patients, however, are candidates for bariatric surgery, which itself is not without controversy and has been associated with increased risk of osteoporosis and spine fractures. 21 Consideration should be given to additional steps that may help mitigate the challenges of operating on the super obese population, such as utilizing minimally invasive techniques when feasible, intrawound antibiotics, and early postoperative mobilization. 21 Further research on these mitigation strategies in the super obese population would be worthwhile.
This study should be interpreted in light of its limitations. First, it is a retrospective cohort study done by means of a chart review with a limited patient number, inviting the bias characteristic of such studies. Larger, multicenter studies and direct comparison of prospectively collected outcomes as compared with normal BMI patients would be useful. Perhaps most obviously, our “control” group was rather broad, including not only nonobese patients (those with BMI < 30 kg/m2) but also patients with BMI that placed them into class III (“extreme”) obesity (BMI between 40 and 50 kg/m2). Indeed, the mean BMI for our control group was 29 kg/m2, just below the threshold for class I obesity. Although the inclusion of obese patients (along with their concomitant risk of complications as reported by previous authors) potentially introduces some bias into the reported complications among our control patients, we feel this group more accurately represents the patients undergoing surgeries in real-world clinical practice. Moreover, when the BMI < 50 kg/m2 control group was further stratified to separate patients with BMI < 30 kg/m2 from those with BMI 30 to 50 kg/m2, results were consistent and demonstrated a statistically significant higher complication rate in the super obese group compared with all permeations of the control group.
Last, the super obese and control groups include patients with a variety of surgical indications and procedures, raising the possibility that we are comparing 2 heterogeneous groups. To address these concerns, we compared the super obese group (BMI ≥ 50 kg/m2) and controls (BMI < 50 kg/m2) with regard to indications for surgery (Table 3) and type of surgery (Table 4). As for indications for surgery, the 2 groups were statistically significantly different only for the indication of infection (19% in super obese vs 4% in controls). This finding is not unexpected given the increased risk of infections in the super obese population. As for the other indications (eg, degeneration, myelopathy, trauma, etc), there were no significant differences between the 2 groups. Similarly, with regard to type of surgery, the only differences between the 2 groups were for posterior cervical fusion (more common in controls with 22% vs 7% in super obese patients) and irrigation/debridement/washout surgeries (13% in super obese group vs 4% in controls), the latter difference again not unexpected given the increased indication of infection in the experimental group. Thus, although the indications and surgeries varied across the 2 groups, they were fairly homogeneous without significant bias aside from the incidence of posterior cervical surgery.
In conclusion, patients with class IV and V obesity (BMI ≥ 50 kg/m2) present several challenges to the spine surgeon. This unique patient population has an increased risk of perioperative complications—particularly wound dehiscence and/or infection—and should be considered separately from other obese patients. Super obese patients should be counseled regarding the increased risks, and steps should be taken to mitigate them whenever possible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this article was supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number 2U54GM104942-02. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.