
Abstract
Study Design:
Retrospective cohort study.
Objective:
The goal of this study was to determine how smoking status influences patient-reported outcome measurements (PROMs) in patients undergoing lumbar decompression surgery.
Methods:
Patients undergoing lumbar decompression between 1 to 3 levels at a single-center, academic hospital were retrospectively identified. Patients <18 years old, and those undergoing surgery for infection, trauma, tumor, or revision, with less than 12 months of follow-up were excluded. Patients were divided into 3 groups: (1) never smokers (NSs); (2) current smokers (CSs); and (3) former smokers (FSs). PROMs analyzed included the Physical Component Score and Mental Component Score of the Short Form-12 Health Survey, the Oswestry Disability Index, and Visual Analogue Scale Back and Leg pain scores. One-way ANOVA was used to compare preoperative and postoperative scores between smoking groups, and multiple linear regression analysis was performed to determine whether smoking status predicted change in each outcome score, controlling for factors such as age, sex, body mass index, and other clinical variables. A P value <.05 was considered to be significant.
Results:
A total of 195 patients were included in the final cohort, with 121 (62.1%) patients in the NS group, 22 (11.3%) in the CS group, and 52 (26.6%) in the FS group. There were no significant differences between groups at baseline or postoperatively. Smoking status was also not a significant predictor of change in any outcome scores over time on multivariate analysis.
Conclusion:
These results suggest that smoking status does not significantly affect short-term complications or outcomes in patients undergoing lumbar decompression surgery.
Keywords
Introduction
Lumbar decompression is a commonly performed and successful procedure to address radicular symptoms secondary to spinal stenosis or disc herniations. 1 By removing compression on nerve roots in the lumbar spine, patients experience immediate symptom resolution and long-term relief. 2 However, success of surgical interventions can still depend on patient-specific risk factors. One factor in particular—smoking and nicotine products—has consistently been implicated as a risk factor for increased reoperation rates and surgical site infections (SSIs) following lumbar surgery. 3,4 Nicotine leads to local arterial vasoconstriction, limiting microvascular circulation and inhibiting perfusion—both of which are essential processes in normal physiological healing after surgery. 5,6
Smoking is associated with negative self-reported patient outcomes in a variety of common lumbar spine procedures, including lumbar fusion surgeries. 7 -9 Furthermore, smoking cessation prior to fusion procedures leads to improved postoperative functional status, satisfaction, and return to work rates. 10 Despite these relatively well-known risks associated with smoking, there is currently a paucity of literature evaluating smoking status and its influence on patient-reported outcome measurements (PROMs) in patients undergoing lumbar decompression surgery. 11 Therefore, the goal of this study was to determine how smoking status influences PROMs in patients undergoing lumbar decompression surgery.
Methods
After institutional review board approval was obtained, patients who underwent a primary lumbar decompression surgery (including discectomy or laminectomy) between 2013 and 2017 at a single academic center were retrospectively identified. Patients older than 18 years with at least 1 year of clinical follow-up were included in the cohort. Patients who underwent surgery for infection, trauma, or tumor were excluded from the final cohort. Patient demographics, including age, sex, body mass index (BMI), months followed up, and duration of preoperative symptoms (<3 months, 3-6 months, >6 months) were recorded. Surgical variables, including the number of levels decompressed and whether a minimally invasive surgery (MIS) technique was used were identified. PROMs were collected on a prospective basis at baseline and postoperatively through the institution’s patient outcome collection database (OBERD, Columbia, MO): the Physical Component Score (PCS-12) and Mental Component Score (MCS-12) of the Short Form-12 Health Survey, the Oswestry Disability Index (ODI), and Visual Analogue Scale Back (VAS Back) and Leg (VAS Leg) pain scores. Secondary outcomes, including rates of revision surgery, 30- and 90-day readmission rates, and SSI, as defined by the Centers for Disease Control’s National Healthcare Safety Network were recorded. 12
Patients were divided into 3 groups based on their preoperative smoking status: (1) never smoker (NS), (2) current smokers (CS), or (3) former smoker (FS). Demographic characteristics and surgical factors were then compared between groups using either Kruskal-Wallis H testing with Dunn multiple pairwise comparison post hoc analysis for continuous data or Pearson χ2 analysis and Fisher exact test for categorical data. A paired-samples t-test was used to determine improvement in PROMs within groups. Differences between groups were compared at baseline and postoperative time points. In addition, delta scores (Postoperative score − Baseline score) were also compared. Two additional measures of patient outcome improvement were included: recovery ratios (RRs) and the percentage of patients who achieved the minimum clinically important difference (%MCID) at final follow-up. 13 -16 RRs were defined as [Delta score/(Optimal score − Baseline score)], with 100 and 0 used as optimal scores for PCS-12/MCS-12 and ODI/VAS Back/VAS Leg, respectively. 13 The %MCID was calculated based on the following PROM threshold values: PCS-12, 8.8 points; MCS-12, 9.3 points; ODI, 5.3 points; VAS Back, 2.1 points; and VAS Leg, 2.4 points. 15,16 Multiple linear regression was used to determine whether smoking status was a predictor of PROMs, controlling for the aforementioned demographic and surgical variables. All statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS) version 24 (IBM Corporation, Armonk, NY).
Results
A total of 195 patients were included, with 121 (62.1%) in the NS group, 22 (11.3%) in the CS group, and 52 (26.6%) in the FS group. Mean age was 60 [58, 62] years, mean BMI was 30.0 [29.1, 30.8] kg/m2, and total number of male patients was 145 (74.4%). There were 124 (63.6%) patients with symptoms for <3 months, 58 (29.7%) patients with symptoms for between 3 and 6 months, and 13 (6.7%) patients with symptoms for >6 months. A total of 94 (48.2%) patients underwent single-level decompression, 67 (34.4%) patients underwent 2-level surgery, and the remaining 34 (17.4%) patients underwent surgery at 3 levels. A total of 68 (34.9%) patients underwent surgery using the MIS technique. There was a significant difference between groups with regard to age: FSs were significantly older than NSs and CSs (NS, 58.0 years; CS, 59.0 years; FS, 67.0 years; P < .001). Otherwise, there were no differences between groups with regard to sex, BMI, months followed up, symptom duration, number of levels decompressed, or the MIS technique (Table 1).
Demographic Characteristics and Surgical Factors of Cohort, by Smoking Groups.
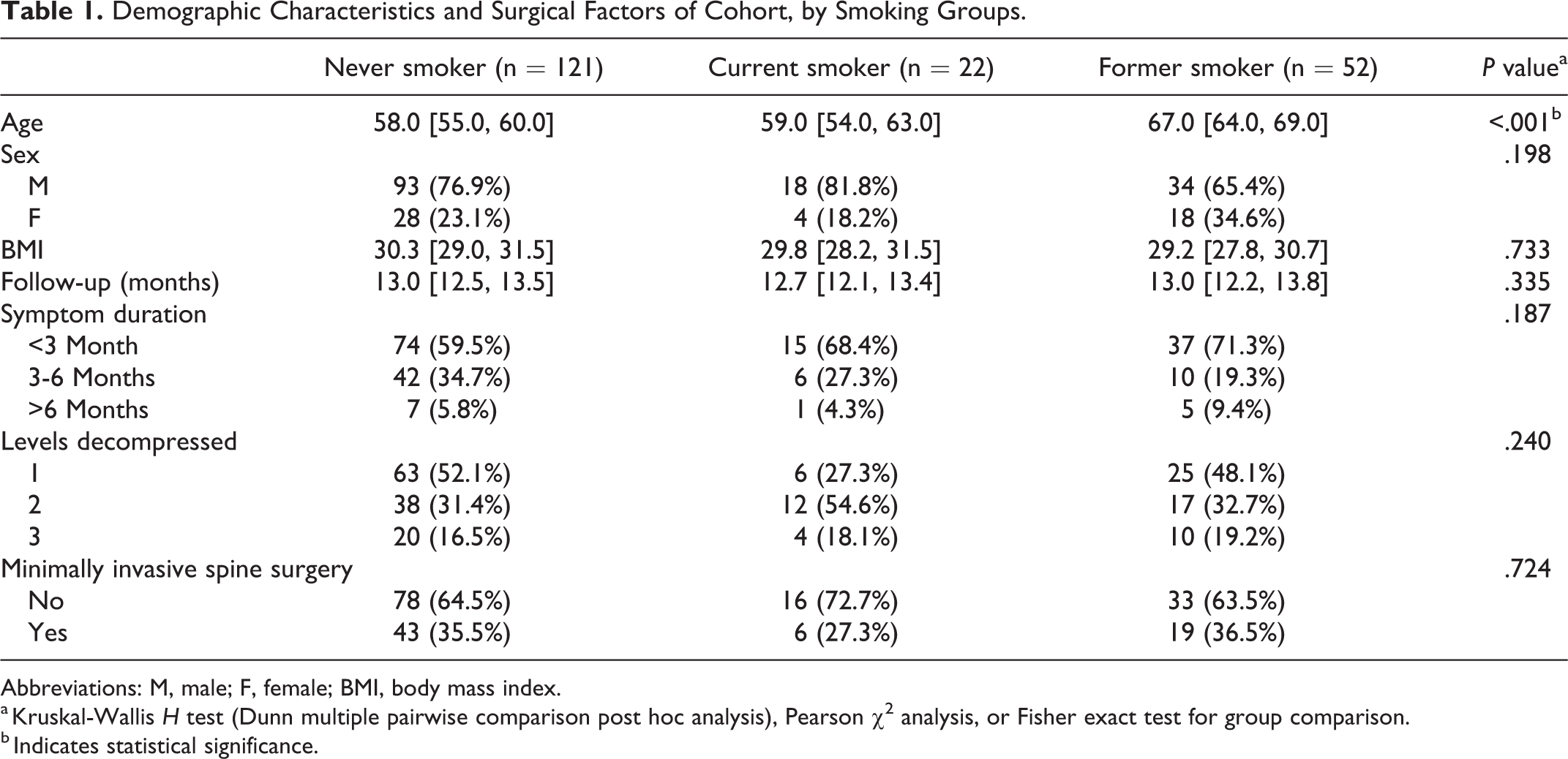
Abbreviations: M, male; F, female; BMI, body mass index.
a Kruskal-Wallis H test (Dunn multiple pairwise comparison post hoc analysis), Pearson χ2 analysis, or Fisher exact test for group comparison.
b Indicates statistical significance.
Patients in all groups improved after surgery with regard to PROMs, except for CSs who did not demonstrate a significant improvement in terms of MCS-12 (P = .600) and VAS Back (P = .084) pain scores and FSs who did not exhibit improvement in MCS-12 (P = .535) scores after surgery. When analyzing differences in PROMs between groups, there were no significant differences found at baseline, postoperatively, or with regard to delta scores. When considering RRs and %MCID between groups, the FS group demonstrated a greater RR (67.4%) than both NS (46.0%) and CS (47.4%) groups (P = .046). Finally, with multivariate analysis, smoking status was not a significant predictor of any PROMs (Table 2).
Patient-Reported Outcome Measurement (PROM) Comparisons Between Smoking Groups.a
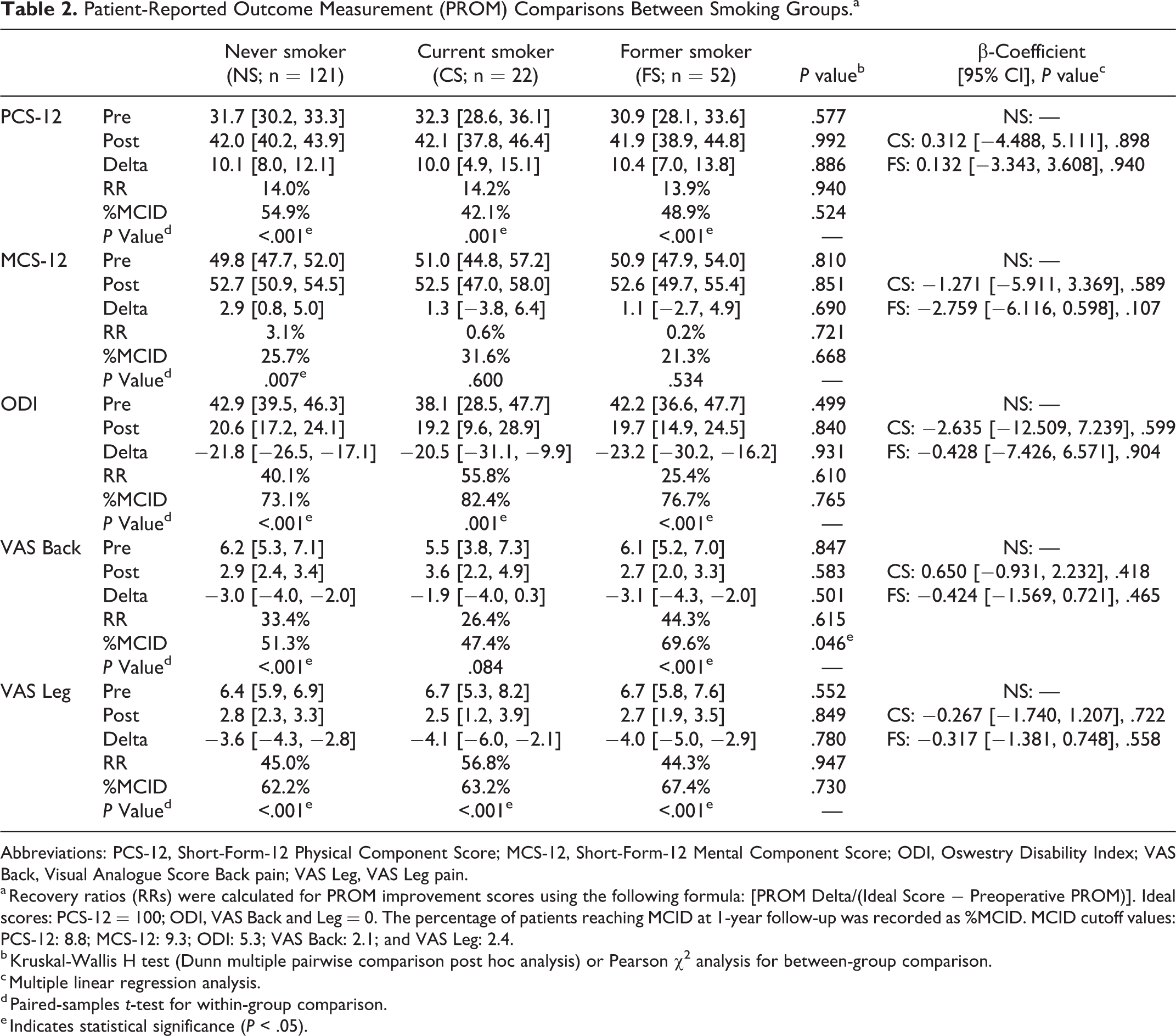
Abbreviations: PCS-12, Short-Form-12 Physical Component Score; MCS-12, Short-Form-12 Mental Component Score; ODI, Oswestry Disability Index; VAS Back, Visual Analogue Score Back pain; VAS Leg, VAS Leg pain.
a Recovery ratios (RRs) were calculated for PROM improvement scores using the following formula: [PROM Delta/(Ideal Score − Preoperative PROM)]. Ideal scores: PCS-12 = 100; ODI, VAS Back and Leg = 0. The percentage of patients reaching MCID at 1-year follow-up was recorded as %MCID. MCID cutoff values: PCS-12: 8.8; MCS-12: 9.3; ODI: 5.3; VAS Back: 2.1; and VAS Leg: 2.4.
b Kruskal-Wallis H test (Dunn multiple pairwise comparison post hoc analysis) or Pearson χ2 analysis for between-group comparison.
c Multiple linear regression analysis.
d Paired-samples t-test for within-group comparison.
e Indicates statistical significance (P < .05).
In total, 7 (3.6%) patients required revision surgery for one of the following reasons: deep SSI, disease at an adjacent level, or recurrent stenosis or disc herniation, with no difference in revision rates (P = .814). There were 2 (1.7%) patients who were readmitted prior to the 30-day postoperative mark and 7 (3.6%) who were readmitted up to 90 days postoperatively, with no statistical differences noted between groups (P > .05; Table 3).
Revisions, Readmissions, and Infections Between Smoking Groups.a
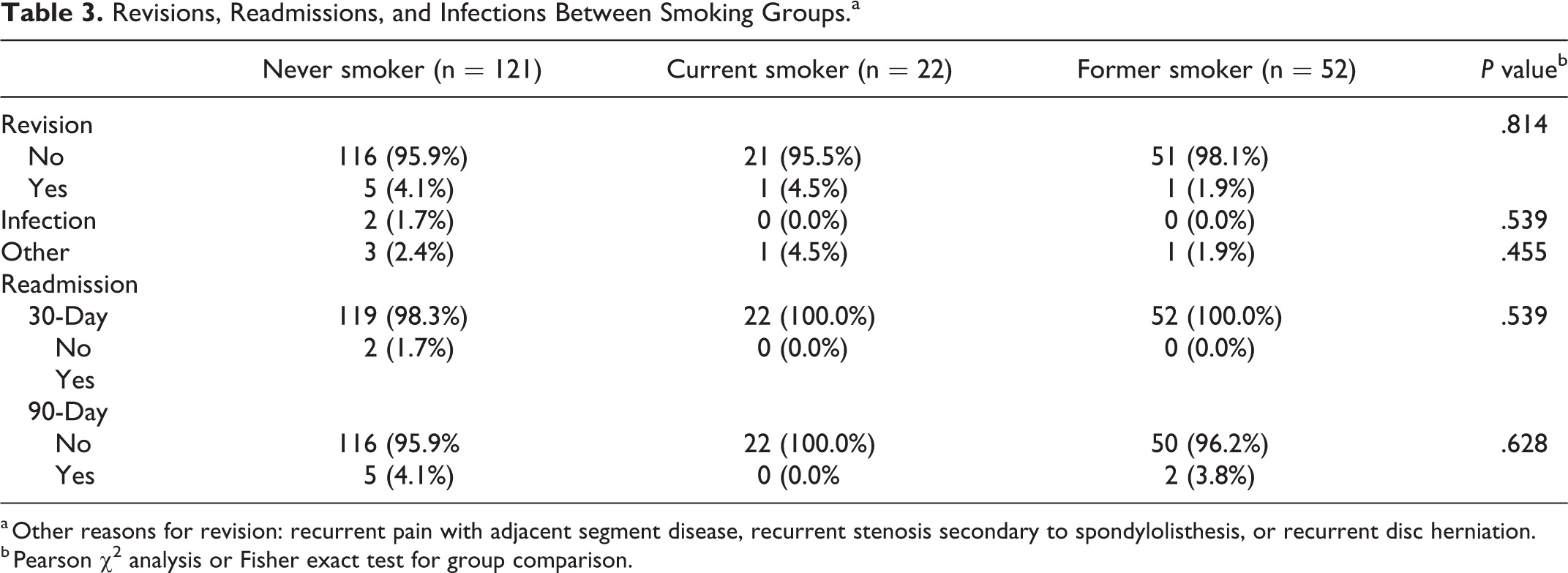
a Other reasons for revision: recurrent pain with adjacent segment disease, recurrent stenosis secondary to spondylolisthesis, or recurrent disc herniation.
b Pearson χ2 analysis or Fisher exact test for group comparison.
Discussion
The adverse effects of smoking have been well documented in patients undergoing lumbar fusion. 17 In addition to decreasing vascularity at the postoperative site, smoking is associated with increased rates of osteoporosis with reduced trabecular bone thickness and overall poor bone health. 18 These factors all contribute to result in increased rates of pseudarthrosis following lumbar fusion surgery. 8,19 In addition, smoking has been shown to be associated with worse PROMs in lumbar fusion patients. 20 -22 Despite these known risks in fusion surgery, postoperative outcomes in patients undergoing lumbar decompression surgery are less well established.
In this study, there were no significant differences in baseline, postoperative, or delta outcome scores between groups. Similarly, there were no differences in complication or readmission rates, and results of multiple linear regression analysis indicated that smoking status was not a significant predictor of worse outcomes for any PROMs. All groups also demonstrated significant improvement from baseline to final follow-up for most PROMs except for the following: CS did not significantly improve in MCS-12 scores (P = .600) or VAS Back scores (P = .084) after surgery, and FS did not improve MCS-12 scores only (P = .534). Furthermore, the FS group had a higher proportion of patients that achieved MCID in VAS Back scores compared with the NS and CS groups (67.4% vs 46.0% and 47.4%, respectively; P = .046).
Few studies have evaluated smoking status and outcomes following lumbar decompression surgery, with mixed results. Mehta and Sharma 23 reviewed 143 patients undergoing either lumbar microdiscectomy or decompression surgery and found no significant differences in ODI, VAS Back, or VAS Leg scores between groups. In a separate prospective study conducted by Stienen et al, 24 a total of 102 nonsmokers, CSs, and FSs were followed up to 1 year postoperatively with no differences between groups at the 4 week and 1-year postoperative time points in terms of PCS-12 and VAS pain scores. 24 Furthermore, the authors found that smokers were as likely to achieve favorable outcome scores for PCS-12 and MCS-12 compared with their nonsmoking counterparts. In a separate follow-up analysis, the same authors noted a similar trend between smokers and nonsmokers up to 4.5 years after surgery. 25 The results of these studies are similar to the findings in the present study, with little postoperative differences in short-term PROMs.
However, other studies analyzing smoking and lumbar decompression surgery have found contrary findings. A previous study performed by Jazini et al 22 found that whereas preoperative PROMs did not vary between groups, CSs undergoing decompression surgery had significantly worse 12-month ODI scores (P = .013). This study, however, did not incorporate a multivariate analysis in the assessment of smoking and outcomes; hence, baseline differences between groups were not controlled for in the analysis. 22 Gulati et al 26 compared nonsmokers and CSs in a retrospective review of 825 patients after microdecompression surgery and found that CSs not only had worse preoperative ODI, but also significantly worse changes in ODI improvement at 1 year (P = .01). Additionally, the authors reported that 69.6% of nonsmokers achieved MCID compared with only 60.8% of CSs (P = .008). 26 However, Gulati et al included only microdecompression surgeries, whereas the present study also included multilevel laminectomies. That being said, it is difficult to make even comparisons between the aforementioned studies and the present analysis, based on inherent differences between the 2 cohorts. The present analysis demonstrated no significant differences in patient-reported outcomes between smoking groups on univariate and multivariate analysis. Although smoking seems to have a physiological effect on microcirculation and, hence, overall perfusion in previously mentioned studies, the present study did not observe any clinical differences between groups based on smoking status. Hence, practitioners may consider not precluding patients from receiving simple, decompression surgery for degenerative lumbar pathology based solely on smoking status until further evidence is available.
Few studies have examined differences in complication rates or readmission rates in decompression surgery. 27,28 Similar to the present study, Stienen et al 25 noted no significant differences in deep wound infections or reoperations between nonsmoking and smoking groups. However, Bydon et al 3 demonstrated smoking to be a significant predictor of reoperation after lumbar laminectomy.
There are several limitations to this study. It is a retrospective review of prospectively collected data and is, thus, subject to reporting bias. Smoking status was self-reported by patients, which could result in incorrect categorization of FS patients who identified as nonsmokers. In addition, the total number of pack-years and perioperative smoking cessation status was not available for CSs or FSs, further decreasing the study’s ability to categorize patients. There were a relatively low number of patients in the CS group, creating relatively uneven patient groups, which limited the extent of our statistical analysis.
Conclusion
The results of this study suggest that short-term patient outcomes after lumbar decompression may be similar regardless of smoking status. Further research with larger cohorts is needed to validate these findings.
Footnotes
Authors’ Note
This study was approved by the institutional review board at the Thomas Jefferson University Hospital. Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.