
Abstract
Study design:
This was a retrospective review of prospectively collected data.
Objectives:
Few studies have described the relationship between mental health and patient-reported outcome measures (PROMs) after minimally invasive spine surgery. Prior studies on open surgery included small cohorts with short follow-ups.
Methods:
Patients undergoing primary minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) for degenerative pathology were retrospectively reviewed and stratified by Short Form (SF-36) Mental Component Summary (MCS): low MCS (<50, n = 436) versus high MCS (≥50, n = 363). PROMs assessed were back pain, leg pain, North American Spine Society Neurogenic Symptoms, Oswestry Disability Index, SF-36 Physical Component Summary, and MCS. Satisfaction, expectation fulfilment, and return to work (RTW) rates also were recorded at 1 month, 3 months, 6 months, and 2 years.
Results:
Preoperative MCS was 39.4 ± 8.6 and 58.5 ± 5.4 in the low and high MCS groups, respectively (P < .001). The low MCS group had significantly poorer preoperative PROMs and longer lengths of stay. Despite this, both groups achieved comparable PROMs from 3 months onward. The mean MCS was no longer significantly different by 3 months (P = .353). The low MCS group had poorer satisfaction (P = .022) and expectation fulfilment (P = .020) at final follow-up. RTW rates were initially lower in the low MCS group up to 3 months (P = .034), but the rates converged from 6 months onward.
Conclusions:
Despite poorer PROMs preoperatively, patients with poor baseline mental health still achieved comparable results from 3 months up to 2 years after MIS-TLIF. Preoperative optimization of mental health should still be pursued to improve satisfaction and prevent delayed RTW after surgery.
Keywords
Introduction
Degenerative spine conditions, including spinal stenosis and degenerative spondylolisthesis, are among the leading causes of pain, functional impairment, and decline in quality of life in the general population. 1 Transforaminal lumbar interbody fusion (TLIF) is a common surgical treatment option. However, a small group of patients may not experience significant improvements and may remain dissatisfied after lumbar fusion surgery. 2 As health care systems transition toward value-based care, it is imperative to determine which patients benefit the most from high-cost procedures, including lumbar fusion. Researchers have recognized the need to study preoperative factors that influence patient-reported outcome measures (PROMs) and quality of life in order to identify optimal surgical candidates.
It is widely acknowledged that psychological factors may influence the clinical course of lower back pain (BP). 3 Several spine centers have begun to incorporate psychological screening and subsequent treatment in their spine surgery programs. 4 Whereas some studies have demonstrated an association between preoperative mental health and outcomes following spinal surgery, 5 -10 others have failed to do so. 11,12 The current literature on open lumbar fusion has identified a correlation between psychological factors and PROMs of pain and disability. 5,6,10,13 -16 However, there is a paucity of literature conducted in the context of minimally invasive spine surgery.
Although preoperative mental health may predict outcomes of lumbar spine surgery, the change in mental health status after lumbar spine surgery has yet to be described. Chronic BP and functional limitations associated with degenerative lumbar spine conditions may contribute to poor mental health preoperatively; however, these symptoms have the potential to improve postoperatively.
Therefore, the purpose of this study was 2-fold: (1) to assess the influence of preoperative mental health on PROMs and (2) to analyze the change in mental health after minimally invasive TLIF (MIS-TLIF) using a large cohort followed over 2 years. We hypothesized that patients with poor baseline mental health would have poorer PROMs, although mental health would improve after MIS-TLIF because of a reduction in pain and disability.
Methods
This study was approved by a centralized institutional review board (CIRB 2018/2356). Prospective registry data was retrospectively reviewed for patients who underwent primary MIS-TLIF for degenerative pathology between 2006 and 2015. The indications for surgery were grade 1 or 2 degenerative spondylolisthesis with nerve compression symptoms, including radicular pain, paresthesia or neurogenic claudication. Patients were excluded if they had previous spinal surgery, inflammatory conditions, metabolic bone disease, infection, fracture, or tumor. All patients failed a trial of nonoperative treatment of at least 3 months and underwent preoperative evaluation with erect and dynamic flexion/extension lumbar spine radiographs and magnetic resonance imaging. All surgeries were performed by the senior authors (W-MY, S-BT), and a standardized postoperative rehabilitation program was conducted.
Demographics and comorbidity data was collected before surgery. Patients were assessed using the Visual Analogue Scale for BP and leg pain (LP), North American Spine Society (NASS) score for neurogenic symptoms, Oswestry Disability Index (ODI), and Short-Form 36 (SF-36). The length of operation and length of stay were also recorded. The medical outcome study approach proposed by McHorney and Ware 17 was used to derive 2 higher-order summary scores from the 8 subscales of the SF-36: the Physical Component Summary (PCS) and Mental Component Summary (MCS). These have been reported using norm-based scoring (mean = 50; SD = 10) in nearly all published studies to date, 17 and the MCS has been validated as an acceptable screening tool for depression. 18 -21 In this study, we used a preoperative MCS cutoff of 50 to stratify the cohort into 2 groups: low MCS (<50) and high MCS (≥50). This cutoff has been used to assess the general population at risk, and MCS <50 has been shown to indicate psychological distress. 22
Clinical improvement was defined using the minimal clinically important difference (MCID). The MCID represents a change in score, compared with the baseline, that is considered a meaningful improvement to the patient. Previously published values of MCID of 14.9 for ODI, 2.1 for BP, 2.8 for LP, 23 and 4.9 for PCS 24 were used to determine if a patient had attained the MCID. Outcome scores were evaluated again at 1 month, 3 months, 6 months, and 2 years postoperatively along with an assessment of the patient’s expectation fulfilment and overall satisfaction with the outcome of surgery. Expectation fulfilment and satisfaction scores were recorded using 7-level and 6-level Likert scales adapted from the NASS Lower Back Pain instrument, respectively, with a higher score indicating a poorer result. The scores were then categorized into satisfied/unsatisfied or expectations fulfilled/unfulfilled (Table 1). The rate of return to work (RTW) was also assessed using the NASS questionnaire.
Evaluation of Patient Satisfaction and Expectation Fulfilment.
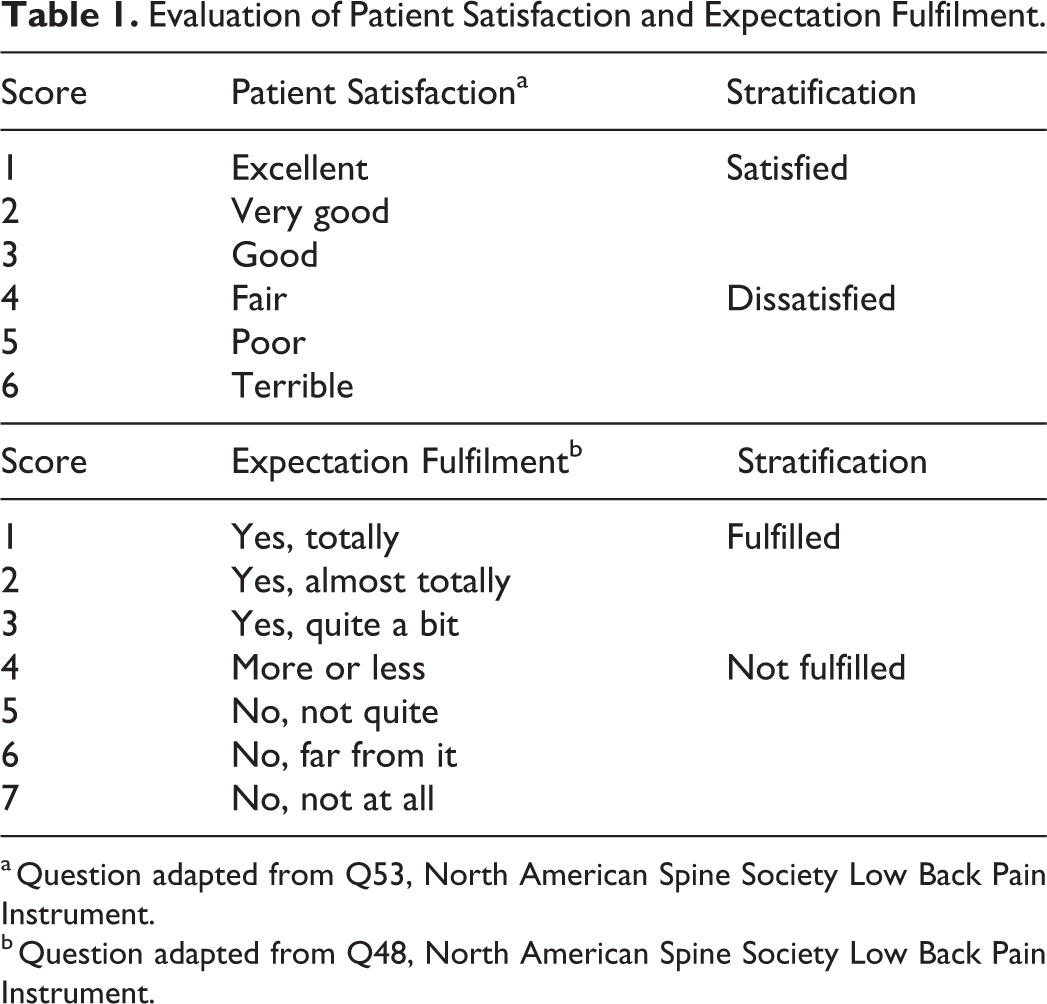
a Question adapted from Q53, North American Spine Society Low Back Pain Instrument.
b Question adapted from Q48, North American Spine Society Low Back Pain Instrument.
A power analysis was performed prior to this study. To detect a MCID of 14.9 points in ODI from a baseline score of 45 with a SD of 15, a sample size of at least 32 patients in each group would be required to achieve a power of 0.80. Baseline patient characteristics and perioperative outcomes were compared between the groups using the χ2 test for categorical variables and the Student t-test for continuous variables. Preoperative and postoperative PROMs were analyzed between the groups using multivariate linear regression controlling for age, gender, body mass index, and number of levels. All statistical analyses were performed using SPSS Version 23.0 (SPSS Inc, Chicago, IL). Statistical significance was defined as P ≤.05.
Results
Patient Demographics and Baseline Clinical Parameters
There were 436 patients in the low MCS group and 363 patients in the high MCS group. The mean MCS was 39.4 ± 8.6 in the low MCS group and 58.2 ± 5.4 in the high MCS group (P < .001; Table 2). Of note, there was no overlap in SDs between the mean MCS of each group. Patients with low MCS were significantly younger (P = .001) and female (P < .001). They also had a longer length of stay (P = .001).
Patient Demographics and Preoperative Clinical Scores (n = 799).
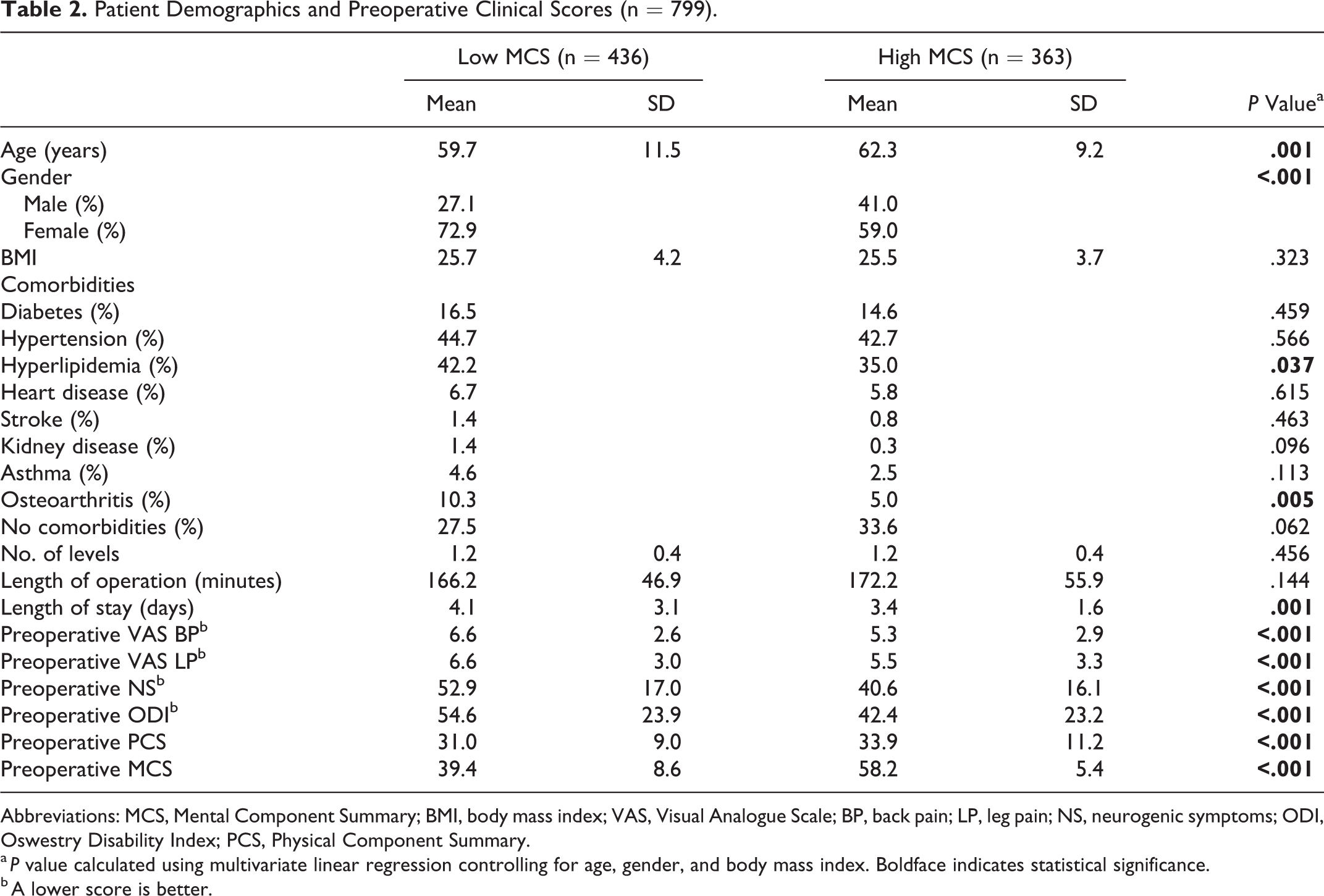
Abbreviations: MCS, Mental Component Summary; BMI, body mass index; VAS, Visual Analogue Scale; BP, back pain; LP, leg pain; NS, neurogenic symptoms; ODI, Oswestry Disability Index; PCS, Physical Component Summary.
a P value calculated using multivariate linear regression controlling for age, gender, and body mass index. Boldface indicates statistical significance.
b A lower score is better.
Impact of Preoperative Mental Health on Postoperative Recovery
After controlling for preoperative differences in age, gender, and body mass index, it was determined that low MCS was associated with worse preoperative BP, LP, ODI, and PCS (P < .001 for each). The low MCS group also had significantly poorer PROMs at 1 month (P < .001 for each). Interestingly, PROMs in the low MCS and high MCS groups converged at 3 months (Figure 1) and remained comparable at 6 months and 2 years (P > .05; Table 3).
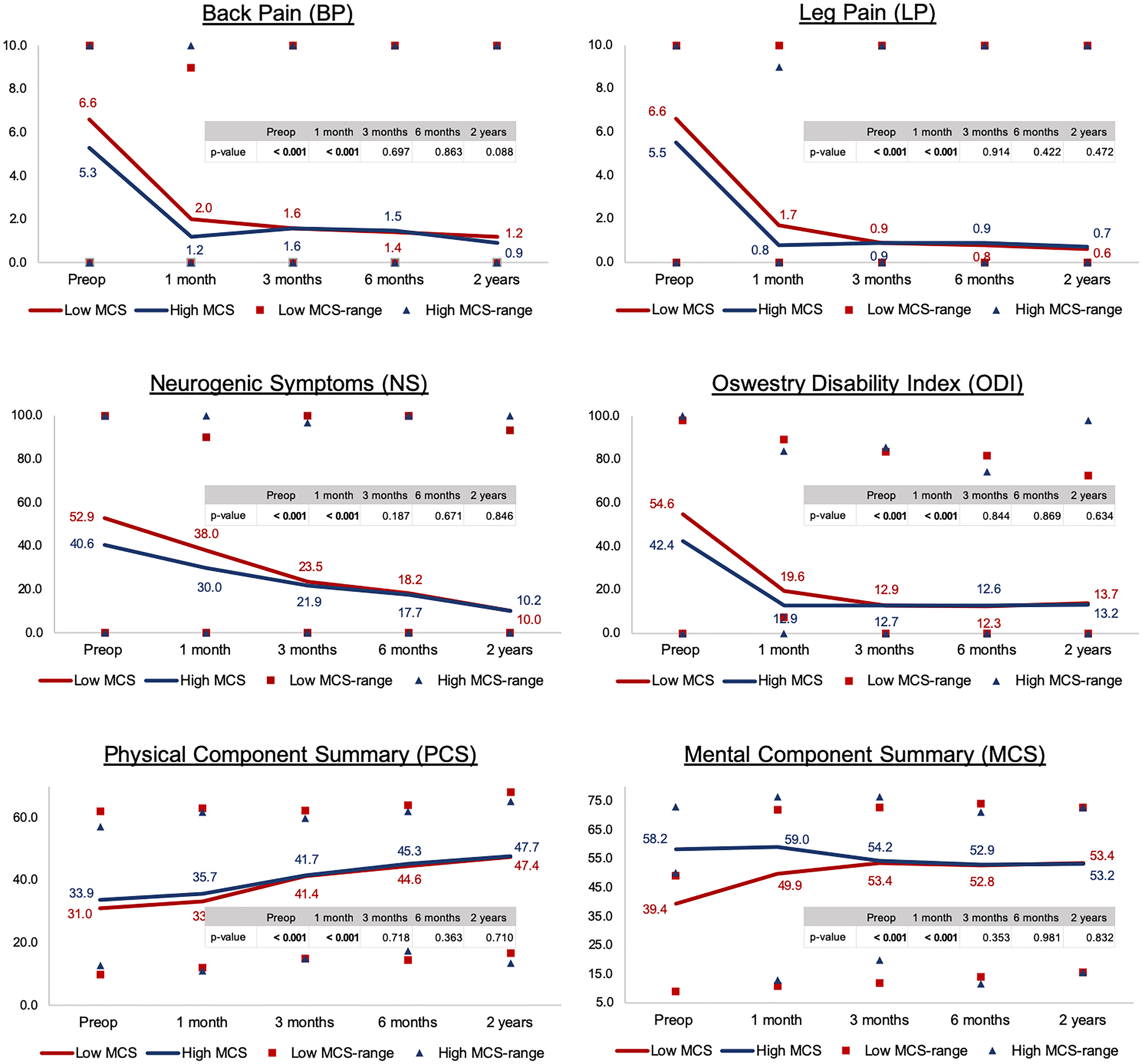
Patient-reported outcome measures at different time intervals.
Comparison of Clinical Outcomes Between Groups at Different Time Intervals (n = 799).
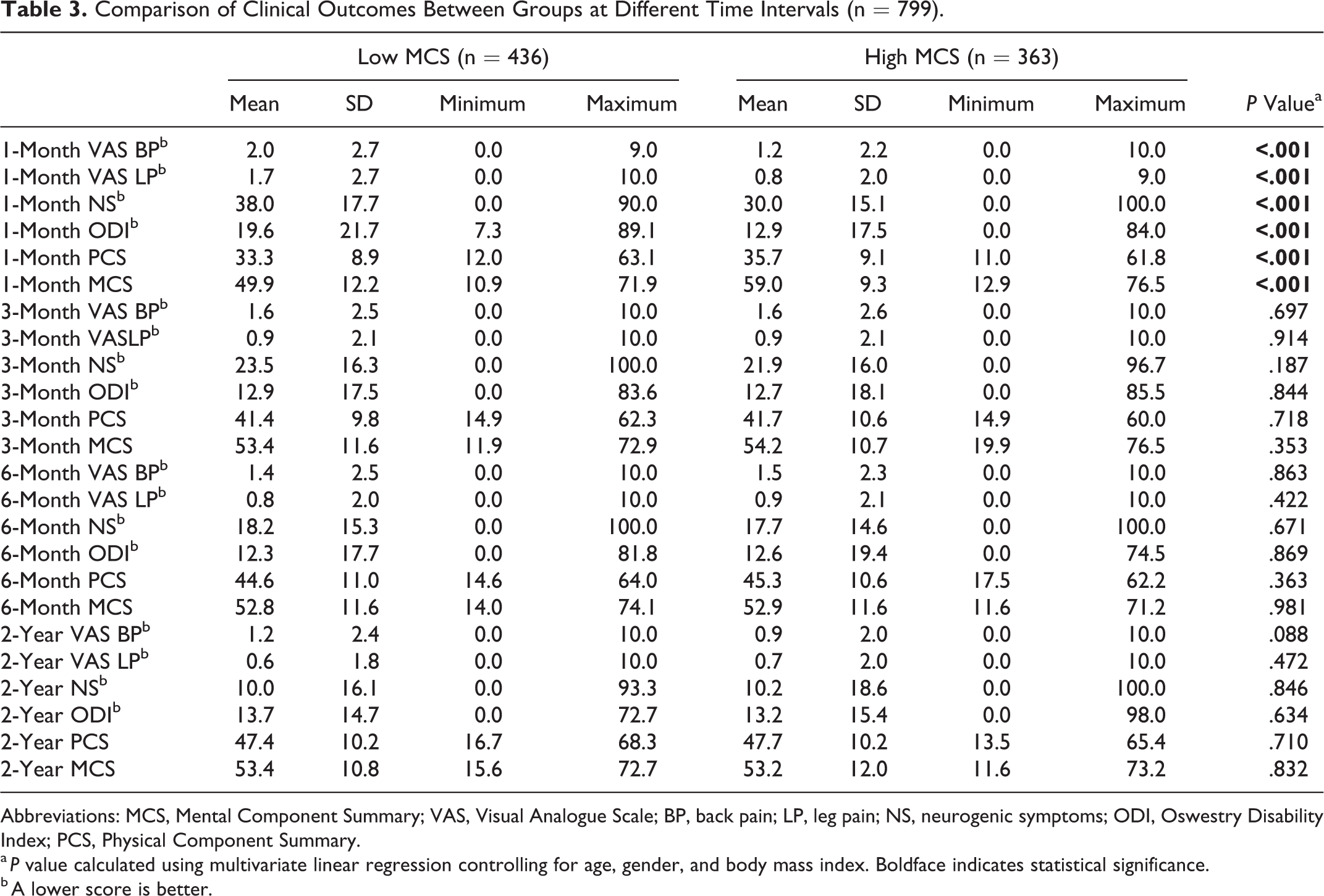
Abbreviations: MCS, Mental Component Summary; VAS, Visual Analogue Scale; BP, back pain; LP, leg pain; NS, neurogenic symptoms; ODI, Oswestry Disability Index; PCS, Physical Component Summary.
a P value calculated using multivariate linear regression controlling for age, gender, and body mass index. Boldface indicates statistical significance.
b A lower score is better.
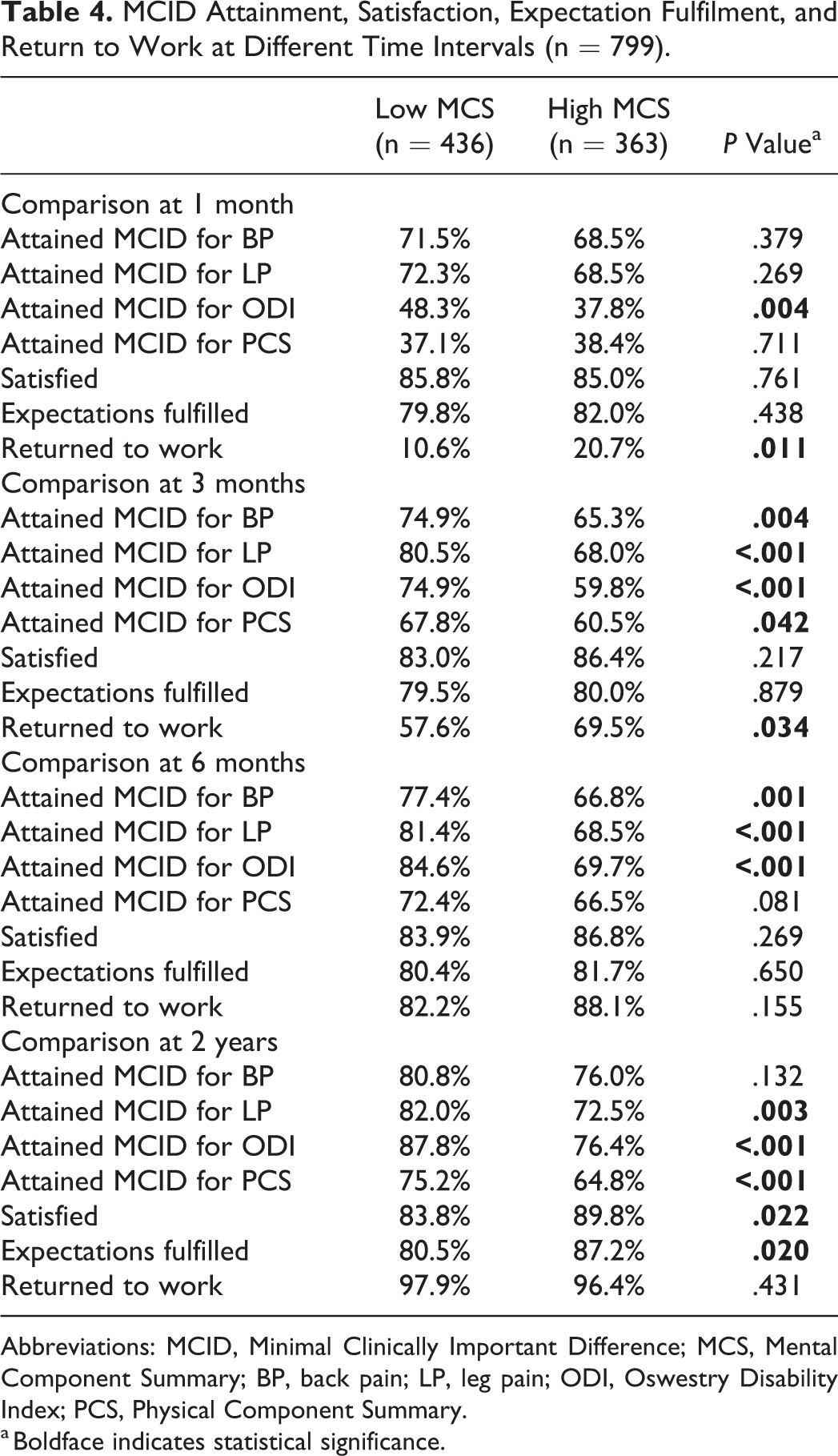
A greater percentage of patients in the low MCS group attained MCID for various PROMs at different time points (Table 4). Of note, the low MCS group had higher MCID attainment for ODI from 1 month (P = .004) and up to 2 years postoperatively (P < .001). At final follow-up, the low MCS group had a higher MCID attainment for LP, ODI, and PCS (P < .05 for each).
MCID Attainment, Satisfaction, Expectation Fulfilment, and Return to Work at Different Time Intervals (n = 799).
Abbreviations: MCID, Minimal Clinically Important Difference; MCS, Mental Component Summary; BP, back pain; LP, leg pain; ODI, Oswestry Disability Index; PCS, Physical Component Summary.
a Boldface indicates statistical significance.
Whereas satisfaction and expectation fulfilment rates were similar in the early postoperative period, the rates diverged at 2 years, with the high MCS reporting greater satisfaction (P = .022) and expectation fulfilment (P = .020).
RTW rates were initially lower in the low MCS group at 1 month (P = .011) and 3 months (P = .034); however, the rates converged from 6 months onward and remained comparable at 2 years (P > .05; Table 4).
Change in Mental Health After MIS-TLIF
The mean MCS in the low MCS group improved by 14.0 points at 2 years (P < .001). Interestingly, the mean MCS was no longer significantly different between the groups by 3 months postoperatively (P = .353). Although 54.6% of the cohort was categorized as mentally distressed preoperatively, this decreased to 35.7% at 2 years. Lower preoperative MCS was predictive of greater improvement in MCS at 6 months (r = −0.798; P < .001) and 2 years (r = −0.900; P < .001).
Discussion
A large proportion of patients undergoing spine surgery may experience some degree of psychological distress. 25 The relationship between mental health and clinical outcomes after lumbar spine surgery is complex. Patients with psychiatric disorders may suffer from long-term disabilities, in part, because of chronic lower BP. 6,26 This study represents the largest series in the literature comparing PROMs in psychologically distressed and nondistressed patients undergoing lumbar fusion. We found that preoperative mental health may influence the early outcome of MIS-TLIF, but this discrepancy resolved after 3 months. Patients with poor mental health had a greater improvement in pain, function, and quality of life, although more subjective outcome measures such as patient satisfaction and expectation fulfilment remained poorer at final follow-up. Patients with psychological distress also had a greater improvement in their mental health, to the extent that the mean MCS was no longer significantly different between the distressed and nondistressed groups by 3 months postoperatively.
Although studies have shown that patients with psychiatric comorbidities such as anxiety or depression may have poorer outcomes after lumbar spine surgery, 8 -10,27 -29 conflicting results still exist. 11,12,30,31 Ng et al 12 studied 100 patients who underwent posterior decompression for spinal stenosis and found that preoperative anxiety and/or depression was not associated with postoperative PROMs. Similarly, Katz et al 11,31 did not find an association between preoperative depression and postoperative satisfaction or improvement in PROMs following lumbar spine decompression with or without fusion. In contrast, Wilhelm et al 32 found that patients with depression not only had greater pain and disability, but also higher medical costs. Although the above studies utilized questionnaires specifically designed to measure anxiety and depression, such as the Beck Depression Inventory, Hospital Anxiety and Depression Scale, Distress and Risk Assessment Method, and Minnesota Multiphasic Personality Inventory, these questionnaires are not routinely administered in spine clinics. As health care systems shift toward value-based care, the collection of PROMs is becoming a routine practice, and the SF-36 is one such instrument commonly used to measure generic health-related quality of life. A recent systematic review noted that the most frequently investigated predictor variables were depression (5 times) followed by the SF-36 MCS (3 times). 32 However, the term depression has been defined using more than 40 different methods in the literature, leading researchers to conclude that a better form of standardization in future studies is required. 33 The SF-36 MCS is a widely used standardized questionnaire that has been validated as an acceptable screening tool for depression. 18 -21 Using this instrument, this study categorized 54.6% of patients as psychologically distressed at baseline (defined as MCS < 50). 17 These patients were more likely to be younger and female, as described in previous epidemiological studies, 34 although these factors were not found to influence outcomes recently. 35,36 Using multiple regression to control for differences in baseline demographics, we found that although patients with low MCS had significantly poorer metrics of pain, function, and quality of life preoperatively, all PROMs in the low MCS and high MCS groups converged at 3 months and remained comparable at 6 months and 2 years. In contrast to previous findings that a lower MCS was associated with poorer 1- and 2-year PCS, 10,37 this study also found no significant difference in PCS, a measure of physical well-being. Despite the subjective interpretation of the PROMs by patients with a differing mental attitude, patients with psychological distress, after having their spine pathology addressed and experiencing a decrease in pain and disability, may also experience an improvement in the overall perception of their physical health.
To adequately address questions on how suitable these patients are to undergo MIS-TLIF, the concept of MCID was also studied. From 3 months onward, the low MCS group had a higher rate of MCID attainment for LP, ODI, and PCS, likely because of the lower baseline scores. This indicates that even patients with psychological distress may perceive a meaningful improvement in pain, function, or quality of life after MIS-TLIF. To our knowledge, this is one of the first studies to investigate the influence of psychological factors on the clinical outcomes of minimally invasive spine surgery. MIS-TLIF has been shown to decrease soft-tissue injury, blood loss, postoperative pain, length of stay, and recovery time for patients with degenerative lumbar conditions. 38 It is plausible that the faster recovery provided by MIS-TLIF 39 may have minimized the delay in functional improvement usually observed in psychologically distressed patients, allowing these patients to attain a normalized score by the 3-month mark. However, longer follow-up studies are required to determine if these improvements are durable over time.
The relationship between psychological distress and patient satisfaction after lumbar fusion has also not been established. Recently, Abtahi et al 2 reported that psychologically distressed patients had significantly lower scores in overall satisfaction and satisfaction with their provider, whereas Sinikallio et al 40 showed that preexisting psychiatric disorders could also influence patient expectations and affect satisfaction. We used the NASS scoring method, which is a standardized and validated outcome instrument. 41 Consistent with previous studies, this study found that despite achieving comparable PROMs, patients with poor baseline mental health had poorer subjective outcomes in terms of satisfaction and expectation fulfilment. Although satisfaction and expectation fulfilment are essential parameters in patients with good mental health, these are highly subjective and must be treated cautiously in patients with psychological distress.
The costs of lower BP are estimated to increase beyond US $100 billion annually, with two-thirds of this directly related to decreased productivity and lost wages. 42 Although previous studies have assessed the functional outcomes after TLIF, there is a paucity of data on RTW after lumbar spine surgery in mentally distressed patients. Parker et al 28 in a 2-year longitudinal cohort study found that of the 32 patients working before TLIF, all 15 patients in the top half of the Zung score (better depression score) returned to work postoperatively, whereas only 11 (65%) patients in the bottom half did so. In contrast, our study results differed slightly—although poor baseline mental health delayed RTW in the initial 3 months after surgery, this did not affect RTW rates from 6 months onward. This is the first and largest study investigating the effect of mental health on a patient’s ability to RTW in the early postoperative period up to 2 years after surgery.
The change in mental health status after surgery was analyzed using longitudinal data at 1 month, 3 months, 6 months, and 2 years. Patients who were psychologically distressed preoperatively had a substantial improvement of 14.0 points at final follow-up, whereas patients who were not psychologically distressed had a slight decrease of 5.0 points. The overall percentage of distressed patients also declined from 54.6% to 35.7% at final follow-up. Interestingly, the largest improvement in MCS was observed within 3 months after MIS-TLIF, to the extent that the mean MCS was no longer significantly different between the groups by 3 months. This finding has not been reported previously. Comparison with existing literature is difficult because of differing study populations; hence, it is possible that cultural or socioeconomic factors may have explained this difference in mental health improvement. For instance, our study was conducted in an Asian population. Because Asian patients often feel more stigmatized by mental illnesses, 43 they could have overreported/inflated their mental health status on patient-derived outcome instruments such as the SF-36. Mental health improvements in distressed patients who underwent MIS-TLIF for degenerative spinal disease may be the result of pain relief and improved function postoperatively. Conversely, poorer preoperative mental health could be driven by spinal disability, chronic pain, and the use of opioid analgesia, which is associated with increased depressive symptoms. 44 Given the bidirectional relationship between opioid use and mental health, 45 it is also possible that surgeons may be overprescribing opioids to psychologically distressed patients who may experience a heightened perception of pain postoperatively but ultimately achieve outcomes similar to those of their nondistressed counterparts, as shown in this study. In light of the multifaceted relationship between chronic pain, poor mental health, and opioid use, further studies focusing on opioid consumption patterns in distressed patients with spinal pathology are necessary.
Several limitations must be noted. This was a retrospective review of a consecutive series of patients. However, outcomes used were prospectively collected in a spine registry routinely according to an established protocol, likely eliminating any bias in terms of data collection. Age and gender were significantly different between the groups, which could confound the study findings. However, a recent study using similar PROMs has shown that gender does not affect the outcomes of MIS-TLIF. 36 Patel et al 46 also noted a higher proportion of young patients in the group with greater Patient Health Questionnaire-9 score. Furthermore, we used multiple regression analysis to control for these baseline differences. The type of work undertaken by our study cohort was not routinely recorded in our spine registry. Because patients who were involved in heavy labor may require a longer time to RTW, this may have confounded our RTW data. However, this was not the focus of our study because previous studies have already described the impact of occupational characteristics on RTW after lumbar spine surgery. 47 Instead, our study focused on the RTW of non-Workers’ Compensation patients, who were less likely to be involved in heavy labor. 48 Next, we used the SF-36 MCS to measure mental health status. Although it is a validated instrument that also covers psychological symptoms described by other disease-specific questionnaires, such as depressive and anxiety symptoms, it is not designed to diagnose specific psychiatric disorders. Consequently, it is important to note that this study focuses on patients with a poor mental health status as measured by a generic health-related quality-of-life instrument, not on specific psychiatric diagnoses (eg, depression, anxiety) and their impact on PROMs. Because we did not analyze the psychiatric histories of patients or conduct any preoperative psychological evaluation, the presence or absence of specific psychiatric disorders within each MCS group could not be determined and, therefore, could have confounded the results. In addition, the fact that these patients chose to undergo surgery for their spine condition reflects significant pain and functional impairment that may have biased upward our finding of psychological distress. For these patients, a cutoff of 50 might be too high. However, Vilagut et al 20 previously reported that the optimal cutoff for the detection of depressive disorders was 40.2 to 45.6. Several others have also used a cutoff of 50 on the SF-36 mental health subscore or MCS to identify psychological distress in patients undergoing joint arthroplasty. 22
Conclusion
MIS-TLIF has the potential to provide greater improvements in mental health in patients with psychological distress, especially within the first 3 months after surgery. Despite poorer PROMs preoperatively, patients with low preoperative MCS undergoing MIS-TLIF still achieved comparable outcomes from 3 months onward, and a greater proportion of these patients experienced a clinically meaningful improvement in pain, function, and quality of life. However, given that the range of each postoperative score was very wide, the clinical implications on PROMs at the individual level may be limited, and it is likely that some patients with poor preoperative MCS may still achieve poorer PROMs postoperatively. Overall, this study suggests that poor baseline mental health may not be a contraindication to MIS-TLIF for degenerative spondylolisthesis among well-selected surgical patients, and it may be unnecessary to screen out such patients at spine surgical centers. On the contrary, surgeons should reassure them that they may attain clinical benefits similar to those of their nondistressed counterparts. Notwithstanding, preoperative optimization of mental health should still be pursued to improve patient satisfaction and prevent a delay in RTW after surgery.
Footnotes
Authors’ Note
Centralised institutional review board (IRB) approval (CIRB 2018/2356) was obtained for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.