
Abstract
Study Design:
Prospective cohort study.
Objective:
Evaluate changes in gait, pain, and psychosocial factors among degenerative lumbar spondylolisthesis (DLS) patients before and 3 months after surgical intervention.
Methods:
Forty-four symptomatic DLS patients performed clinical gait analysis 1 week before surgery and 3 months after surgery. Patients performed a series of over-ground gait trials at a self-selected speed. Twenty-two matched asymptomatic controls underwent the same battery of tests. Three-dimensional motion tracking was used to analyze gait kinematics. Patient-reported outcomes, gait range of motion, and spatiotemporal parameters compared before and after lumbar decompression with fusion.
Results:
Surgical intervention resulted in significant improvements in walking speed (P = .021), stride time (P = .020), step time (P = .014), and single-support time (P = .038). Significant improvements in joint range-of-motion were found for knee (P = .002) and hip flexion (P = .006). Degenerative lumbar spondylolisthesis patients reported significant reductions in pain, disability, and improved psychological perceptions for fear-avoidance of pain and motion (all P < .001).
Conclusions:
Surgical treatment of DLS resulted in a faster, more efficient gait in addition to significant reductions in pain, disability, and psychological fear associated with pain and motion. These beneficial changes that we identified early in the postoperative period indicate that patients return to the quality of life they seek early on. Clinical gait analysis provides objective, quantifiable measures of gait parameters that provide new insight into both the preoperative disability associated with DLS and into the early postoperative function of patients during their rehabilitation.
Keywords
Introduction
Degenerative lumbar spondylolisthesis (DLS) is common in individuals older than 50 years and occurs four times more frequently in women (Figure 1). 1,2 Symptoms of DLS often present as singular instances or combinations of neurogenic claudication, radicular pain, or mechanical low back pain. 3 -6 Typically DLS patients are assessed with patient-reported outcome measures (PROMs) like the visual analogue scale (VAS) for pain levels, the Oswestry Disability Index (ODI) for degree of disability, and neurological examinations for qualitative evaluation of function. 1,3,6 In order to better elucidate the modality in which spinal pathology causes disability, impairment of daily activities, and overall reduced quality of life, it is important to measure and record objective data points in addition to subjective metrics like PROMs. 1,5 -8 The validity of PROMs can be discontent by recall bias, inaccuracies in patient recording, secondary gain motivation, or other psychologic factors. 3,4,9
As with many other musculoskeletal and neurologic disorders, degenerative spine conditions can produce significant changes in ambulation and gait. 7,10,11 Walking limitations are a hallmark of DLS. 12 Anatomically, DLS is characterized by a narrowing of the lumbar spinal canal or nerve root foramen. 12 Symptoms of neurogenic claudication may include cold feet, buttock and back pain, numbness or weakness in the leg(s), altered gait, and “drop episodes,” wherein the patient unexpectedly falls while walking. 12 -14 Several studies have previously investigated the effects of degenerative lumbar spondylolisthesis and stenosis and the effects of surgical decompression on gait using a variety of gait evaluation techniques. 10,11,15 The findings of these studies showed positive effects of decompression surgery on gait function among patients over follow-up periods ranging from 6 to 12 months after treatment. These studies provide initial validation of gait analysis as a useful tool for objectively measuring postoperative improvements in gait among lumbar stenosis patients and for correlation of gait measures to standard PROMs.
Consensus on treatment strategies for DLS has varied, however current literature indicates beneficial outcomes are often associated with combined use of decompression and fusion. 3,16 Current North American Spine Society (NASS) guidelines recommend surgical decompression with fusion for DLS given its strong association with significant improvements in pain, disability, and functional ability. 3 Furthermore, such surgeries are found to produce changes in psychological factors, including depression, anxiety, and fear avoidance. 17,18 While the literature suggests that surgical treatment of degenerative lumbar conditions improved gait function, there is currently a lack of information regarding the effects of decompression and fusion surgery specifically for DLS patient’s gait parameters. The purpose of our study was to evaluate gait parameters changes in DLS patients before and 3 months after surgical intervention using three-dimensional (3D) kinematic gait analysis in addition to standard PROMs and psychosocial factors.
Methods
Institutional review board approval was obtained for a prospective cohort study. Patients were recruited among symptomatic DLS patients who presented to our clinic and who were deemed eligible for surgical intervention. Clinical evaluation of gait was performed 1 week before (Pre) and 3 months (Post) following surgical intervention (Figure 1).
Subjects
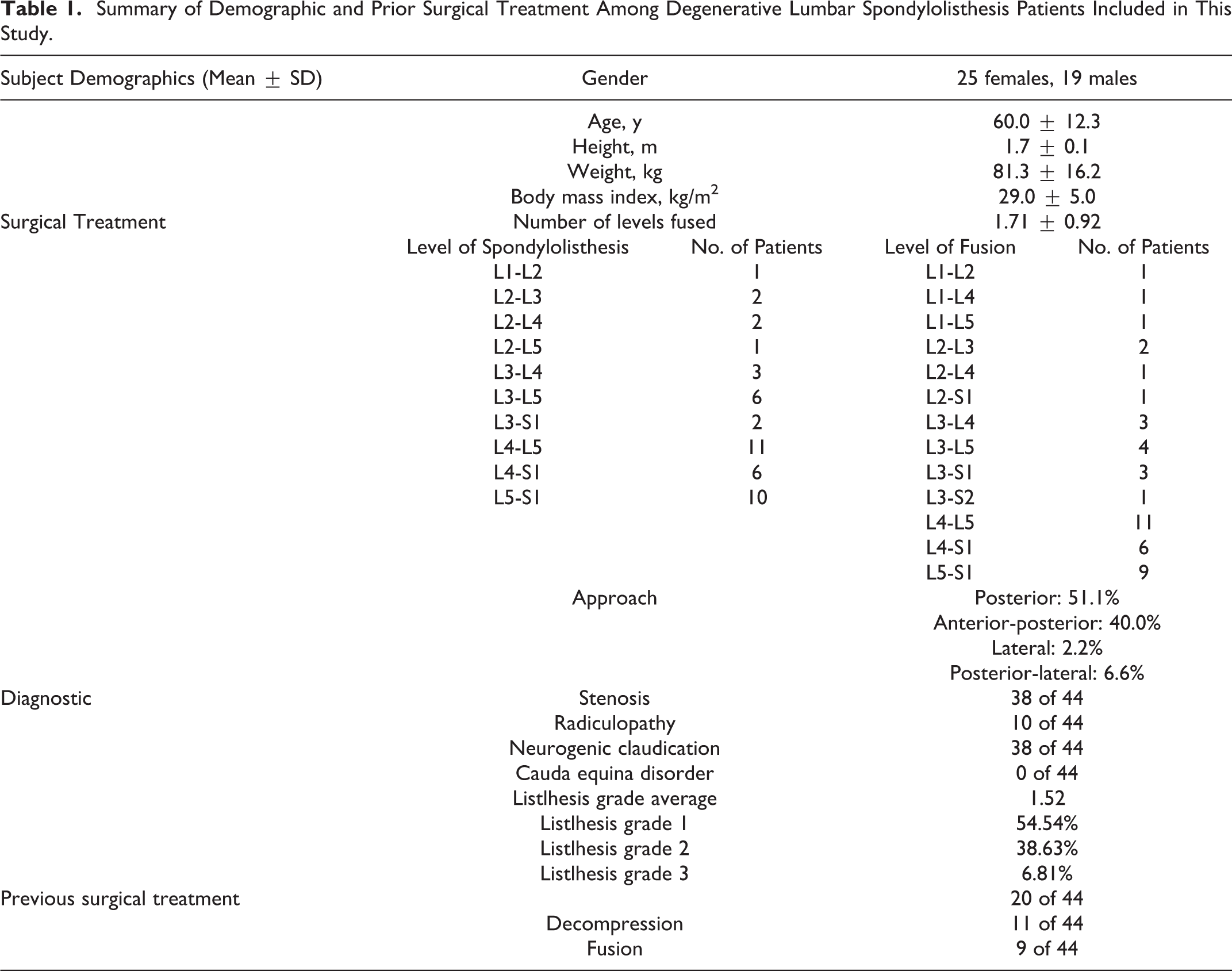
A total of 44 DLS patients and 22 matched asymptomatic controls were enrolled in this study were enrolled in this study. Table 1 provides a summary of DLS subject demographics and surgical treatment approach. Patients were included in this study if they were between the ages of 40 and 75 years, presented with symptomatic DLS, were deemed eligible for surgical intervention (DLS grade II or higher), and were able to stand and walk without assistance.
Summary of Demographic and Prior Surgical Treatment Among Degenerative Lumbar Spondylolisthesis Patients Included in This Study.
Preparatory Procedures
During each clinical evaluation, patients first completed a series of PROMs, including VAS for back and leg pain, the ODI, and 3 psychological questionnaires: the Fear Avoidance Beliefs Questionnaire (FABQ), the Tampa Scale for Kinesiophobia (TSK), and the Demoralization Scale (DS). Patients were fitted with a set of full-body reflective markers for 3D gait analysis (Figure 2). 7
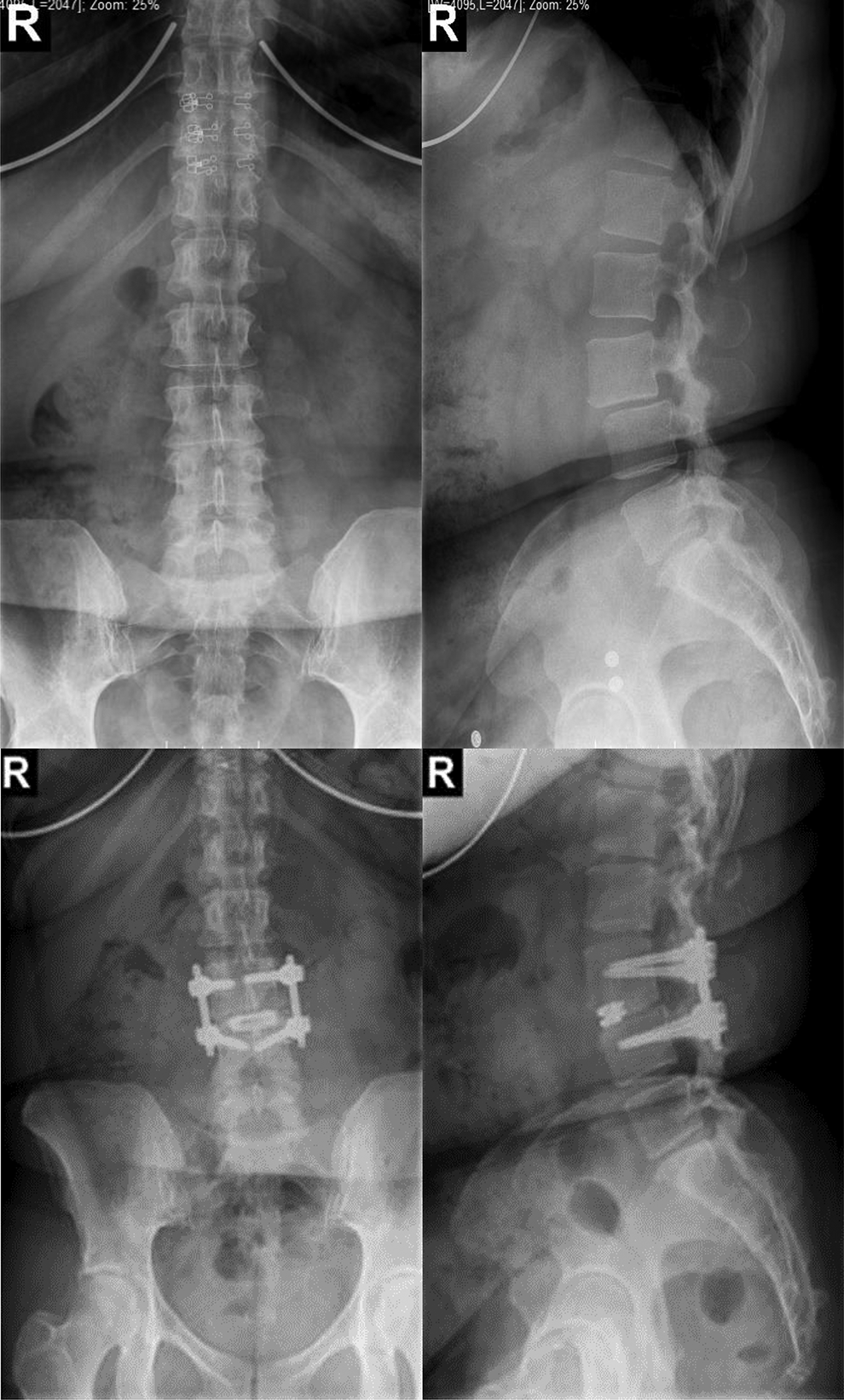
Example radiographs of degenerative lumbar spondylolisthesis (top images) and surgical treatment, including decompression, lumbar interbody fusion, and posterior instrumentation (bottom images).

Example of a patient performing an over-ground walking trial for analysis of kinematic joint range-of-motion (ROM) and spatiotemporal parameters while wearing a set of full-body reflective markers for 3-dimensional motion tracking.
Gait Evaluation
For gait analysis, patients performed a series of 5 over-ground walking trials at a self-selected speed. During each trial, a full gait cycle from the middle of the trial was selected for analysis of spatiotemporal and joint range-of-motion (ROM) parameters. Spatiotemporal parameters included cadence, walking speed, stride time, step time, single-support time, double-support time, stride length, step length, and step width. 7 Joint ROM parameters included lumbar spine, pelvis, hip, knee, and ankle in both the coronal and sagittal planes. Measurements for the trunk ROM were made during the right stance phase only of the analysis cycles. Joint ROM angles were measured such that positive angles represent dorsiflexion, flexion, pelvic ante-version, and right-sided flexion (Figure 3). The Gait Deviation Index (GDI) was also calculated to serve as a composite measure of overall gait abnormality and to provide a reference to healthy individuals. 19 The aim of GDI is to simplify complex gait cycle patterns and to quantify global gait abnormality. 19
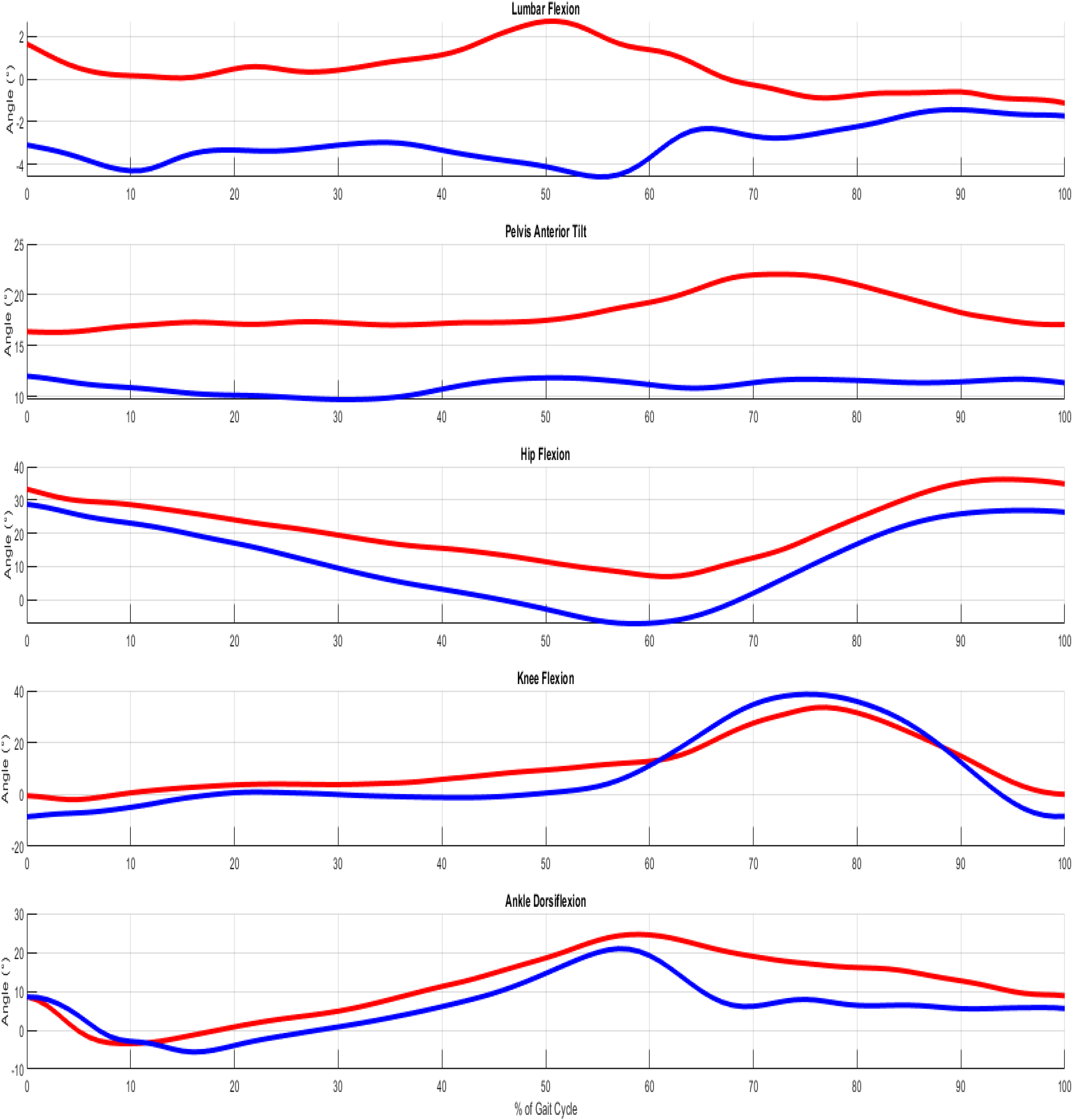
Example plot of sagittal joint range-of-motion for lumbar spine, pelvis, hip, knee, and ankle from a full gait cycle of the right leg before (red) and after (blue) degenerative lumbar spondylolisthesis (DLS) corrective surgery.
The identical gait test was performed on matched asymptomatic controls at a single time point.
Data Acquisition
Full-body kinematic and spatiotemporal data was collected at 100 Hz using a Vicon 3D motion capture system (Vicon, Oxford, UK). Kinematic data was filtered with a fourth-order Butterworth low-pass filter at a 6-Hz cutoff frequency. All outcome measures were averaged across the 5 trials. Data processing was done using Vicon Nexus and custom Matlab programs (The Math Works, Natick, MA, USA).
Statistical Methods
Repeated measurement analysis of variance was used to determine differences in spatiotemporal, joint ROM, and PROMs data before and after surgical intervention. Statistical analyses were conducted using SPSS, Version 23.0 (IBM Inc, Armonk, NY).
Results
There were no statistically significant differences between the surgical patients and healthy controls with regard to age (54.14 ± 9.17 years), height (1.71 ± 0.07 m), weight (73.50 ± 132.64 kg), and body mass index (25.00 ± 3.42; all P > .050).
Spatiotemporal Parameters
Table 2 provides a summary of spatiotemporal gait parameter results. DLS patients demonstrated slower walking speed (P < .001), reduced cadence (P < .001), extended stride and step time (P = .001), longer single and double support time (P < .013), shorter stride and step length (P = .003), and wider step width (P = .027) in comparison with matched controls (Table 2). Significant improvements were seen after surgery in increased walking speed (P = .021), reduced stride time (P = .020), reduced step time (left P = .014, right P = .037), and reduced single support time (left P = .038). Notable increases in mean cadence were also seen; however, they did not reach significance (P = .087). When we compared the spatiotemporal parameters of postsurgical DLS patients with controls, although most of the variables normalized after surgery, it was still statistical differences between the groups (P < .047; Table 2).
Summary of Spatiotemporal Gait Parameters of Degenerative Lumbar Spondylolisthesis Patients 1 Month Before (Pre), and 3 Months After (Post) Surgical Treatment.
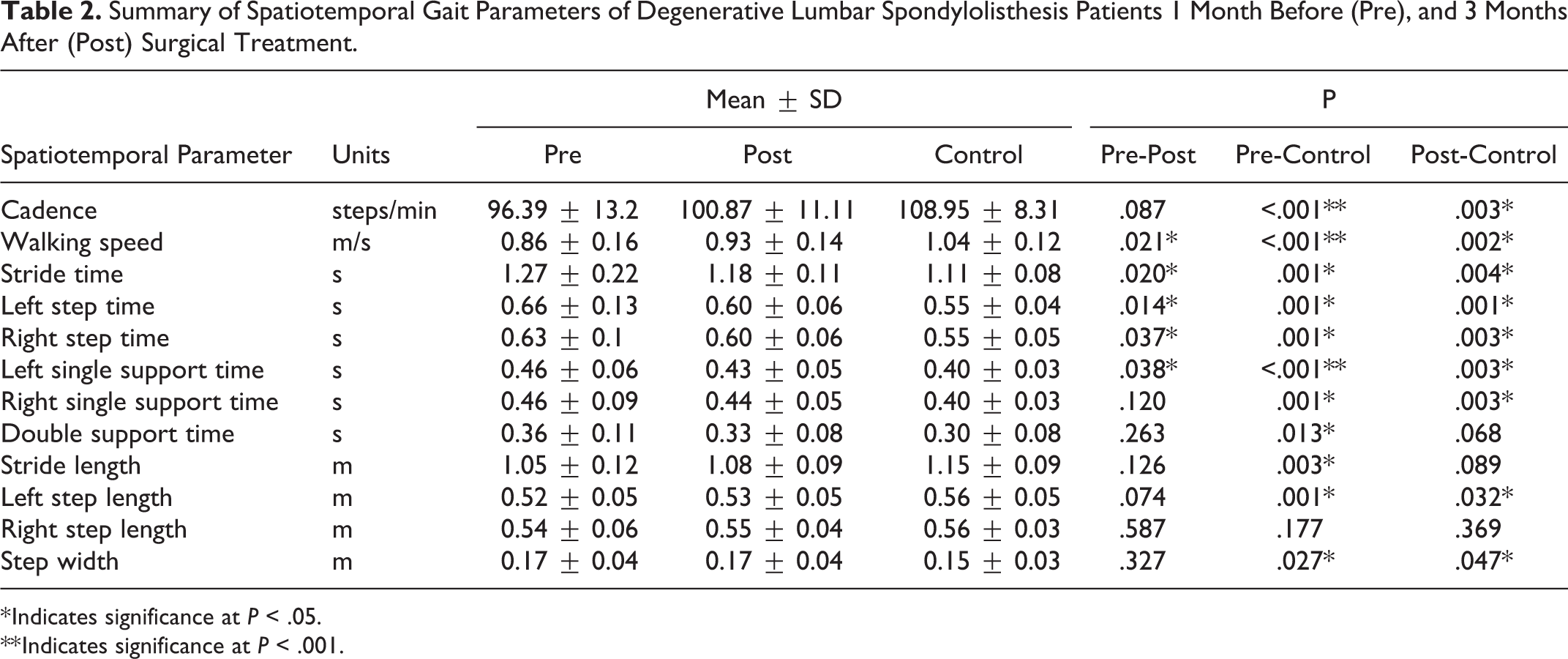
* Indicates significance at P < .05.
** Indicates significance at P < .001.
Joint Range of Motion
Joint ROM results are summarized in Table 3. DLS patients had significantly greater ankle ROM (P < .046), less hip ROM (P < .045), larger pelvic tilt ROM (P = .006) in the sagittal plane, and increased ankle (P < .002) and knee (P < .012) ROM in the coronal plane during gait compared with controls (Table 3). Moreover, compared with normal population with normal gait performance (GDI of 100), our DLS study group clearly exhibited a level of gait abnormality with average values around 88 (P < .001), which is over a standard deviation below normal gait function. 19 Significant changes in sagittal joint ROM included increased knee flexion (right P = .002) and hip flexion (left P = .006, right P = .037). The relatively unchanged postoperative GDI values may indicate that continual neuromuscular adaptation is necessary to achieve maximal recovery beyond the early postoperative recovery period. Ankle (P < .030) and pelvic (P < .001) ROM in the sagittal plane, and ankle (P < .013) and knee (P < .005) in the coronal plane, and GDI score (P < .001) were still different between postsurgical DLS patients compared with controls (Table 3).
Summary of Joint Range-of-Motion (ROM) Results of Degenerative Lumbar Spondylolisthesis Patients 1 Month Before (Pre), and 3 Months After (Post) Surgical Treatment.a
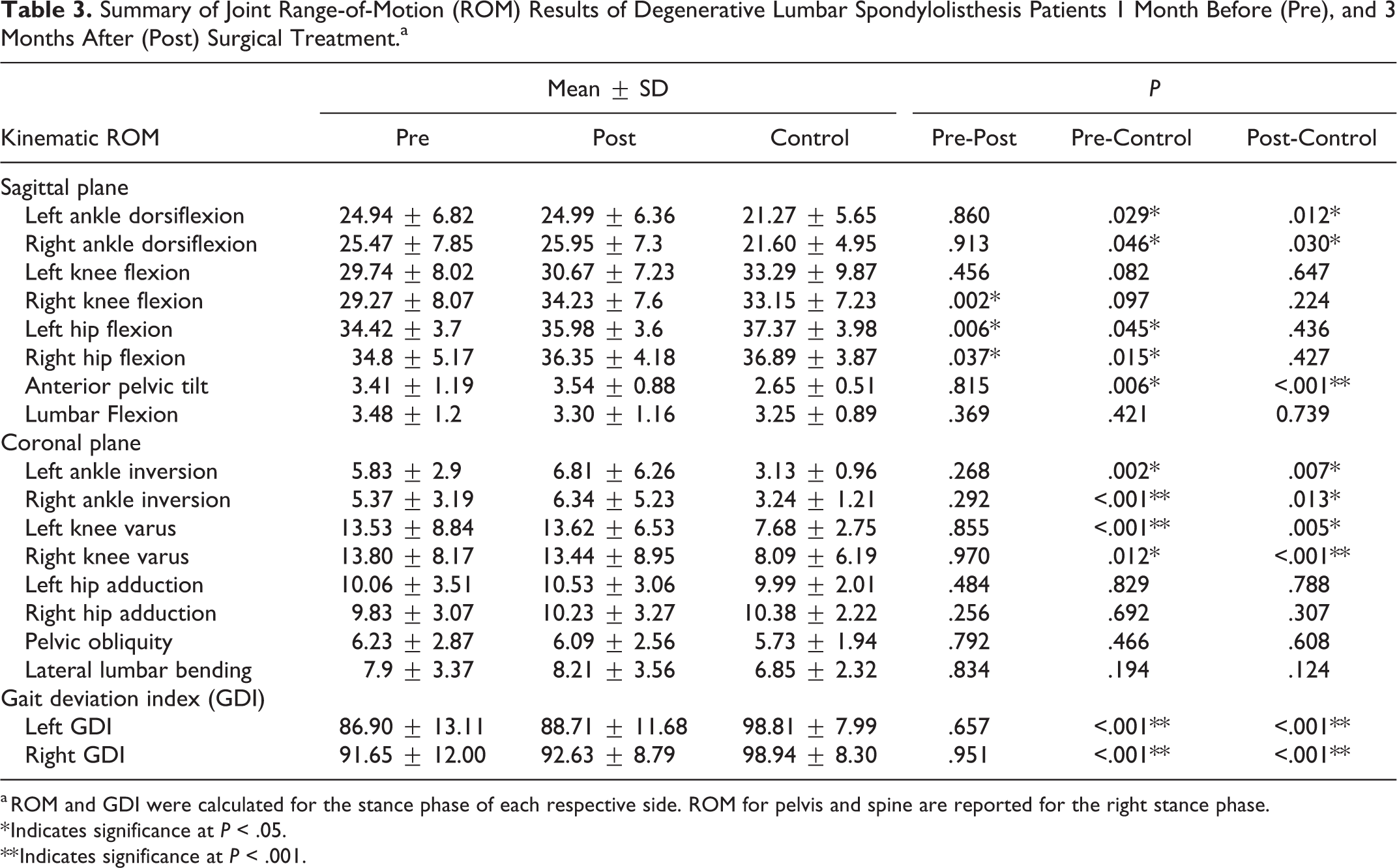
a ROM and GDI were calculated for the stance phase of each respective side. ROM for pelvis and spine are reported for the right stance phase.
* Indicates significance at P < .05.
** Indicates significance at P < .001.
Patient-Reported Outcome Measures
Table 4 provides a summary of PROMs. Significant improvements were found in reduced pain scores for VAS middle back, low back, and leg and ODI (all P < .001). Psychological measures for fear avoidance (FABQ Physical Activity P < .001), kinesiophobia (TSK P < .001), and demoralization (DS P = .040) all showed significant improvements as well.
Summary of Patient-Reported Outcome Measures (PROMs) of Degenerative Lumbar Spondylolisthesis Patients 1 Month Before (Pre), and 3 Months After (Post) Surgical Treatment.
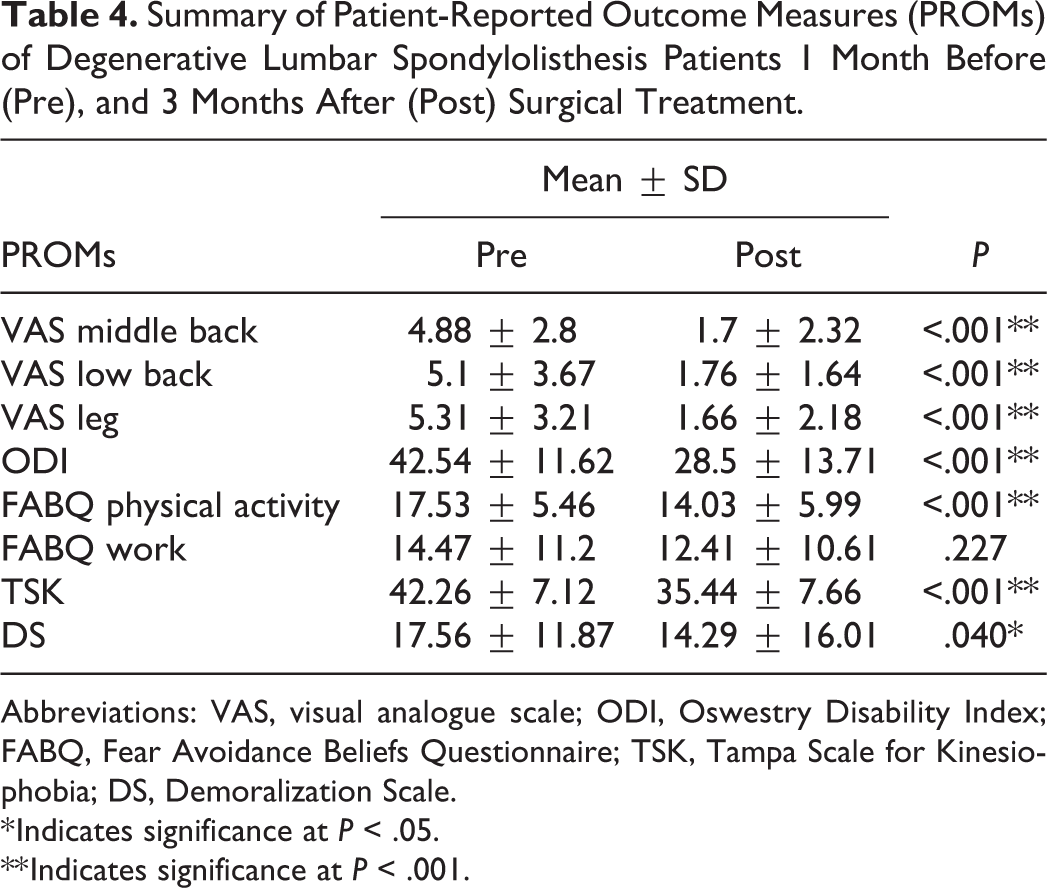
Abbreviations: VAS, visual analogue scale; ODI, Oswestry Disability Index; FABQ, Fear Avoidance Beliefs Questionnaire; TSK, Tampa Scale for Kinesiophobia; DS, Demoralization Scale.
* Indicates significance at P < .05.
** Indicates significance at P < .001.
Discussion
The North American Spine Society (NASS) Evidence-Based Clinical Guidelines for Multidisciplinary Spine Care guidelines report that surgical decompression with fusion for the treatment for DLS results in significant improvements in pain, disability, functional ability, and walking confidence. 3 At the 3-month follow-up, our findings further illustrate an improved spatiotemporal performance, chiefly in a faster and more efficient gait cycle demonstrated by significant improvements in walking speed, stride time, step time, and single-support time. Significant changes in joint ROM were found primarily for increased sagittal hip and knee ROM. Increased knee and hip flexion are often associated with a more stable, confident level of gait function. 7,20 When combined with the strong improvements in reduced pain, reduced disability, and improved psychological factors, the findings of our study indicate that surgical decompression and fusion for DLS leads to improved gait function as early as 3 months following surgical treatment.
The improved spatiotemporal performance among our DLS patients is similar to those found in previous studies of patients surgically treated for lumbar stenosis. Loske et al 10 studied gait and function of patients after surgical intervention for symptomatic lumbar spinal stenosis. Their study group consisted of 29 patients with lumbar spinal stenosis, 40% of which included degenerative spondylolisthesis. They reported postoperative improvements in walking function reflected in faster walking speed, shorter strides, and higher cadence. Moreover, a stepwise linear regression model revealed that a greater improvement in the ODI score was associated with a greater increase in stride length after surgical intervention at the 12-month follow-up when compared with the preoperative baseline. 10 Our results show a similar relationship with a significantly improved ODI score from 43 to 29 and mild improvement in stride length at the 3-month follow-up. While we did see an increase in mean stride length from Pre to Post, the difference was not significant. This may be due to the difference of 9 months between our study and Loske et al’s 12-month follow-up and suggests that improved pain and disability may precede similar improvements in stride length. In a similar study of stenosis patients, Suda et al 15 also observed gait improvements at a 7- to 8-month follow-up with a significant increase in walking speed that was maintained at 12 months after surgical intervention. In the present study, we found a similar significant increase but at a much earlier follow-up.
The results of our study, along with those reported by Loske et al 10 and Suda et al, 15 suggest that some spatiotemporal parameters improve relatively early in the postoperative period while other measures, like joint ROM, may require a more prolonged recovery to elicit significant changes. The findings of our study did show significant improvements in hip and knee ROM; however, these improvements were not consistent side to side and were not reflected in addition changes in lower leg kinematics. A “relearning” period may be necessary to reestablish neuromuscular control and coordination to return to a more balanced and normal level of gait function.
Previous studies have shown significant correlations between fear avoidance and gait dysfunction in adult degenerative scoliosis. 21,22 The findings of the present study indicate that similar patterns are present among DLS patients treated with spinal fusion. Furthermore, based on data from longer follow-up studies such as Suda et al, 15 it can be inferred that early postoperative gait improvements can be maintained long term. Thus, it seems appropriate to initiate postoperative rehabilitation protocols that emphasize improving strength, muscular endurance, neuromuscular control, and spinal stabilization for patients that undergo surgical intervention for DLS. It is evident that recovery of patients undergoing surgical management for symptomatic DLS follows a continuum that involves an early improvement in pain that allows early participation in functional rehabilitation programs aimed at improving neuromuscular control and the resultant dysfunctional gait patterns.
It is important to note the limitations of this study. As with any gait study, the data collected will have large intersubject variability. Additionally, we acknowledge the limitations associated with kinematic modeling using the selected marker set, including skin movement, errors in the anthropometric model, system tracking errors, and data smoothing errors. We also acknowledge the relatively short follow-up time, which likely limits our ability to follow patients to their maximal clinical recovery however the present study provides data at a new time point not previously investigated for gait function. Last, a limitation specific to DLS is the heterogeneity in surgical management, further introducing variability in the study population.
Conclusion
Surgical treatment of patients with DLS produces improvement in gait parameters, pain scores, psychosocial factors, and functional outcome measures that significantly improves walking tolerance. These beneficial changes that we identified early in the postoperative period indicate that patients return to the quality of life they seek early on. This study not only provided a richer understanding of the gait pathology in lumbar spondylolisthesis but uniquely showed that DLS patients enter the gait cycle with abnormal spinal parameters and consequently have altered lower extremity biomechanics. This data can be a valuable contribution to further validate specific surgical interventions and can also be utilized to monitor and adjust rehabilitation protocols and for improved long-term evaluation of patient progress. With utilization of modern techniques in 3D gait analysis along with the incorporation of novel parameters, spine surgeons can further improve the preoperative assessment of disability, which can potentially help guide surgical planning. Furthermore, once patients reach maximal, long-term recovery, we can also gain a better understanding of the surgical outcomes and the applicability of specific techniques to the preoperative pathology identified.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Western Institutional Review Board for the Protection of Human Subjects (IRB#: 20152881).