
Abstract
Our health care system is an evidenced-based quality-centric environment. Pursuit of quality is a process that encompasses knowledge development and care advancements through collaboration and expertise. Depicted here is the foundational knowledge, process, and contributions that hallmark successful clinical quality programs. Beginning with methodology, followed by process and form, we create the foundational knowledge and exemplars demonstrating framework and continuum of process in pursuit and attainment of successful clinical quality and care development for patients. Although our protocol has been devised for complex spine care, this could be implemented across all health care specialties to provide individualized and high-quality care for all current and future patients, all while creating a culture of accountability for physicians.
Extraordinary claims require extraordinary evidence. Quality is the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.
1(p21)
Domains of Quality
Safe—avoiding harm
Effective—based on scientific knowledge, care provided to those who may benefit
Patient centered—respectful, responsive, and guided by patient values
Timely—reduction of harmful delay
Efficient—avoid waste, including ideas and energy
Equitable—does not vary based on personal characteristics
Individual and System Efforts
In improvement of care, traditionally a main focus has been placed on individual practitioner responsibility by emphasizing each and everyone’s duty to minimize error and maximize outcomes. The influence of health systems is commonly perceived to be a supervisory and regulatory function rather than serve as a prime participant in efforts to transform care. Creation of a collaborative and trouble-shooting atmosphere can foster practitioner and health system partnership and prevent an “us versus them” mind-set. Development of collaborative processes are essential when seeking to understand and resolve adverse patient events in a collective, facilitated fashion, as is the goal of root cause analyses. Though, the amount of positive impact from a root cause analysis can vary. 3 Results, in fact, may obscure meaningful advancements if imbalances are created by a lack of trust or lack of true collaboration and problem solving of individual practitioners and the health system they operate in.
In the field of spine surgery, many entities are now bound by governmental and third-party payors to quantify quality of care. The key is to employ adequate measures to allow for objective assessment of results and derive appropriate countermeasures as needed. Spine care continues to be a befuddling—and expensive—health undertaking due to its complexity and variability, both in types of patient disease as well as interventions. Finding solutions to operationalize quality of spine care is of primary concern for the health care community globally with rising demand for spine services being predictable of older and sicker populations worldwide. 4
Do Measurements Matter?
Measurements provide opportunity to determine a current state and explore mechanisms to identify if change results in actual clinical improvement. Measurements shed light on strengths as well as vulnerabilities and provide decision support for directing resources based on risk. Without measurements what is left is conjecture. Measurements matter in improving clinical care through the provision of evidence of the degree to which services increase likelihood of desired outcome and are consistent with current professional knowledge. Competency in interpretation of common measures, as well as basic definitions, is essential to understanding context of quality and in turn apply assessment of quality to clinical practice. Some common measures are illustrated in Table 1.
Illustration of Common Definitions and Application in Outcome Measures in a Complex Spine Practice.
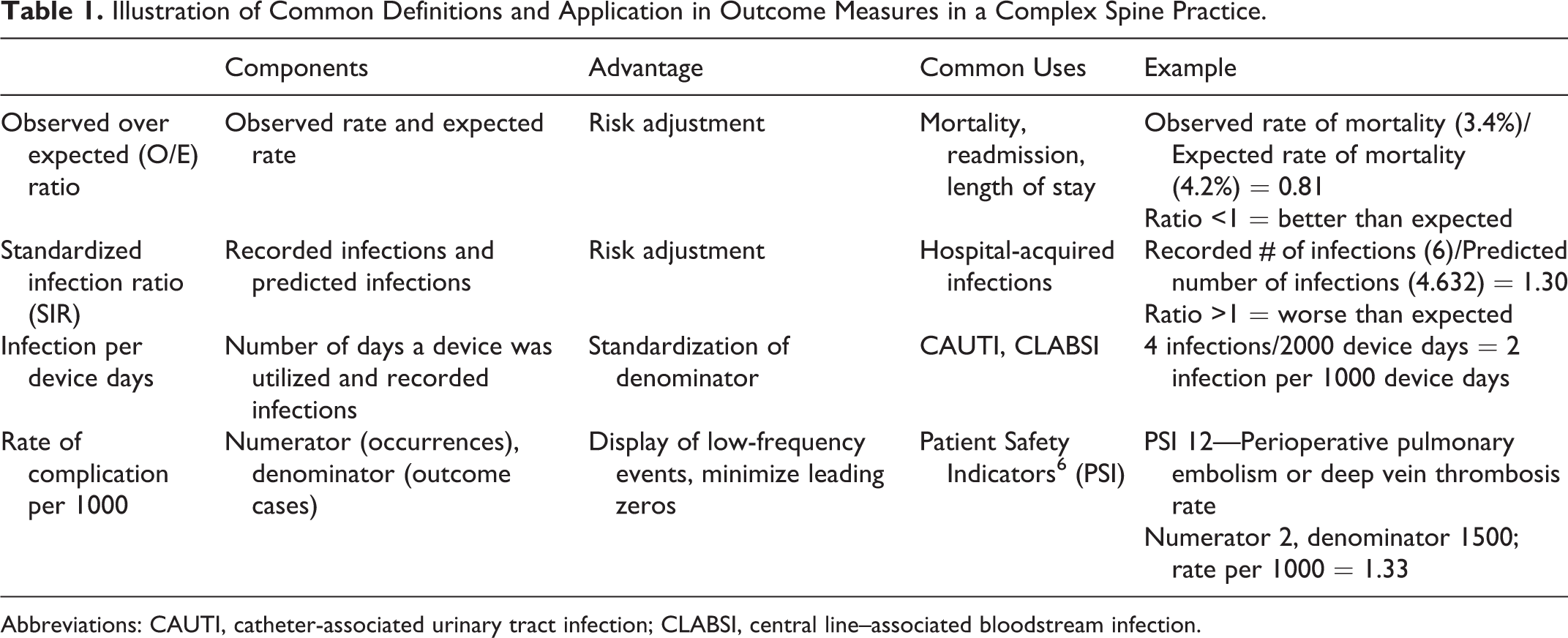
Abbreviations: CAUTI, catheter-associated urinary tract infection; CLABSI, central line–associated bloodstream infection.
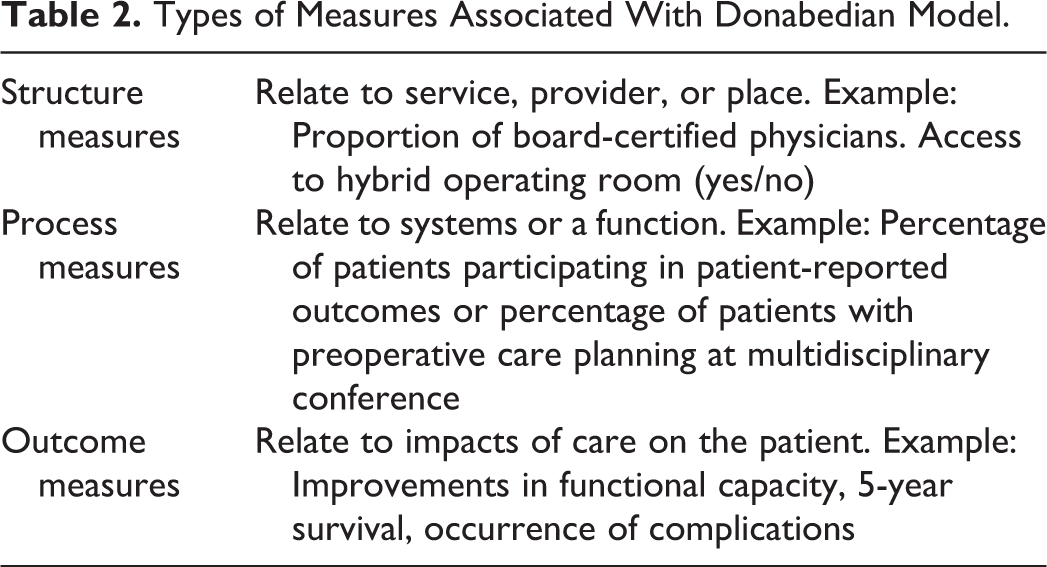
Measurements can be categorized by type. A common framework for categorizing by type is descried by the Donabedian model. 5 This model groups measurements into 3 categories: structure, process, and outcome (Table 2).
Types of Measures Associated With Donabedian Model.
Data Selection Considerations
When selecting resources for developing measures, establishing baseline, and crafting surveillance, it is helpful to ask the very fundamental question: Is the data meaningful?
Anything can be measured, including the meaningfulness of a measure. The National Quality Forum recognize a structure for measuring usefulness and appropriateness of data and sources. 7 A few key considerations in evaluation of sources and metrics are the following:
Standardization—Is the measure standardized at the national level?
Comparability—Will the measure be comparable for the population (CMI [case mix index], severity of illness)?
Stability—Is the source for measure stable, what is the longevity of the source?
Availability—Will the measure be available spanning the intended population?
Timeliness—What is the lag time, will the measure be relevant when received?
Validity—Is the measure adequately tested for consistency and accuracy?
Distinguishable—Does the user have experience to know if the measures reflect performance and not shortcoming of information systems?
Credibility—Are the measures audited or do not require audit?
Risk Adjustment ≠ Benchmarking
Risk adjustment can be confused with benchmarking. Risk adjustment and benchmarking complement each other but are not the same. Risk adjustment considers how the patient or health system performed, factoring in severity of illness, present on admission conditions, and demographics for an assessment of outcome. Benchmarking is comparing this performance to other groups performing same measurement. Table 3 offers illustration of a group of health systems utilizing the common measurement of unexpected readmissions within 30 days. Benchmarking compares between the groups. Benchmarking can be performed taking into account similarities and differences of health systems in review of comparative performance. The different disease severities of health systems are expressed by the CMI that help influence the observed to expected ratio of readmissions relative to the size and setting of a hospital.
Benchmarking Example, Measurement With Ability to Compare Between Health Systems.
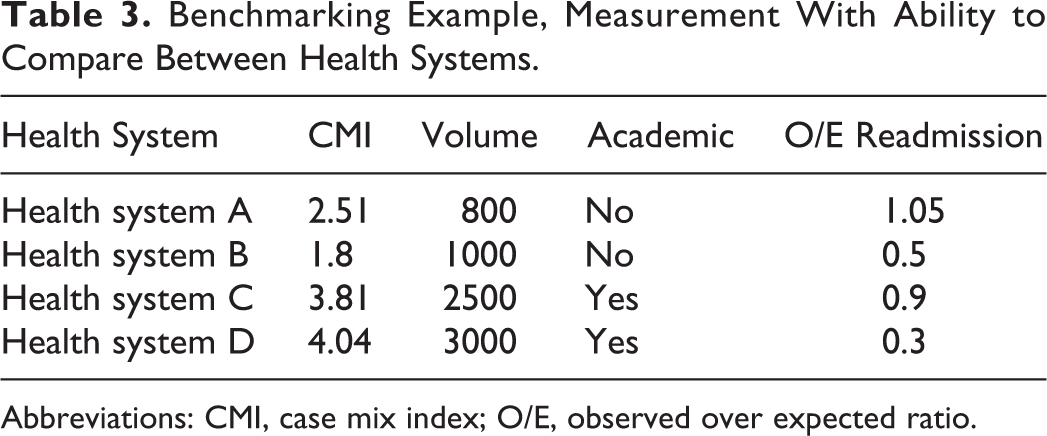
Abbreviations: CMI, case mix index; O/E, observed over expected ratio.
Data…Now What?
The acquisition of data feels like the journey, when rather it is the starting place. Data must be analyzed and utilized in a regular and ongoing fashion. A good starting point is the question: Does it make sense? Next, organize the data, display it, and discuss it among knowledgeable peers. Compare the data to the “expected,” to benchmarks, and to literature. Can variations be identified? Identify differences and research outliers both positive and negative on the spectrum. Act to course correct around clear gaps such as in care planning, communication, or competencies. Develop hypotheses around subtle findings such as would standardizing closure in spine surgery reduce rate of dehiscence? Would implementing nutrition protocol in spine surgery reduce wound dehiscence?
Model for Health Care Improvement
It is inevitable, on making data actionable, that opportunities will surface to practitioners involved in such a quality process. The Institute for Healthcare Improvement offers a model for improvement. 8 The model begins with asking, “What are we trying to improve?” Followed by, “How will we know if the change is an improvement?” and “What change can we make that will result in improvement?” This provides process for clarifying aim, defining improvement, and to hone in on what changes could be made to accomplish. This is followed by testing if a proposed change will meet the intended goal. The framework for testing a proposed change is known as “Plan-Do-Study-Act”:
Develop plan to test a change (Plan)
Carry out the process being tested (Do)
Observe and gather the results (Study)
Determine modifications, make recommendations for further study or implement process, that is, plan for next step: modify, adopt, or abandon (Act)
Model for Organizational Change
Change can be difficult to achieve let alone sustain. Utilizing a model for structuring organizational change is helpful for assuring support for success. One model is Lewin’s model of change theory. 9 In the Lewin model of change theory, change is grouped into phases beginning with “unfreezing,” followed by “change,” and lastly “refreeze.”
Stage 1—Unfreeze: Organize participation and support (buy in). Groups prepare for acceptance and plan for change.
Stage 2—Change: Change is accepted, and new paths adopted. There is alignment around change.
Stage 3—Refreeze: Change becomes the new norm, processes are evaluated for adherence (process measures) and recognized (positive or resulting in course correction) ensuring new ways are anchored into culture.
Initial planning for each area of change, including supports to sustain, is key to successful implementation and sustainment of organizational change.
Applying the Principles to Complex Spine Surgery
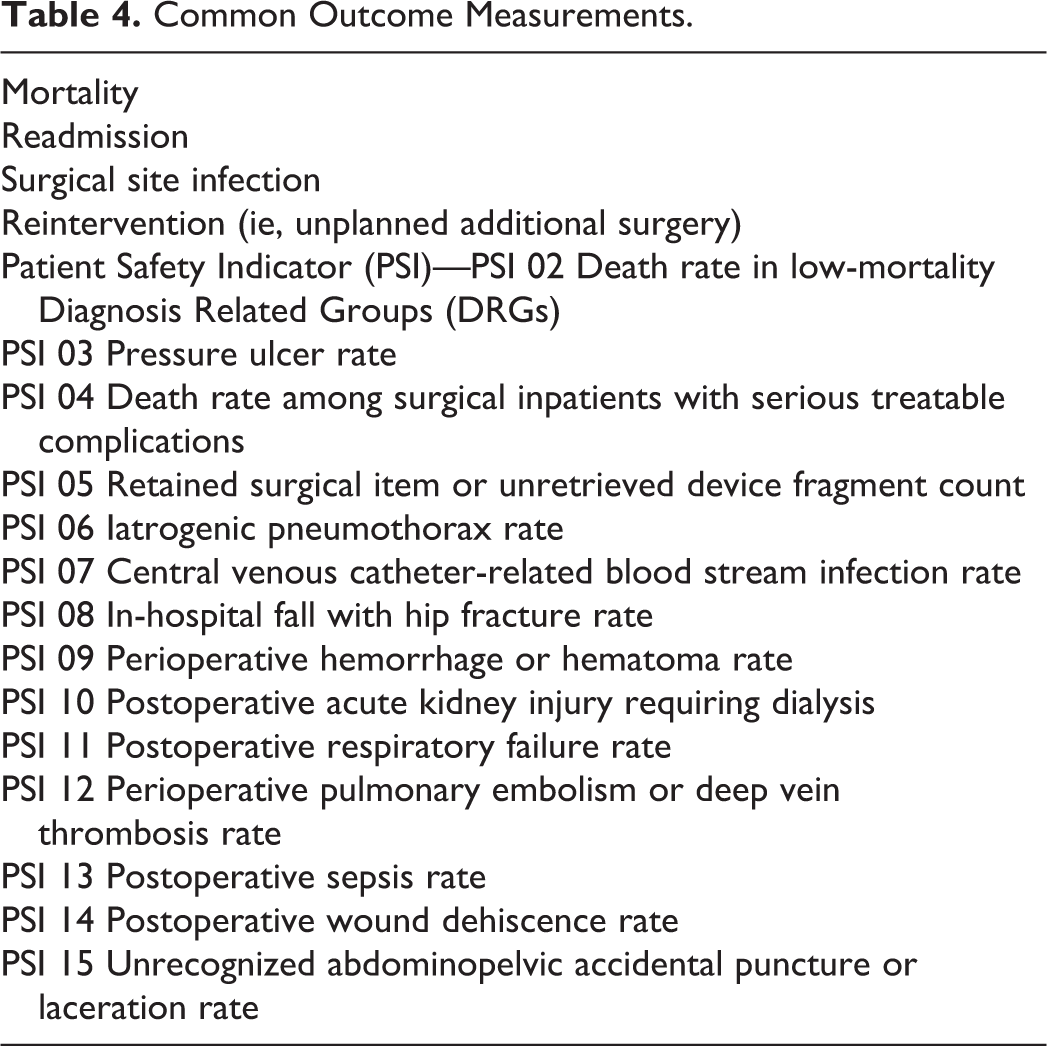
Complex spine surgery has evolved to an increasingly commonplace procedure category and in such has become a major focal point of quality improvement initiatives. Nationally, a number of measurements have come to life beyond the usual mortality and deep surgical site infections that are increasingly governing how we practice. Examples of these are shown in Table 4. 10
Common Outcome Measurements.
To effect change, a number of concepts hold promise to connect the power of a healthcare system with each of its providers toward the mutual goal of creating a fact based collaborative and continuous learning environment intent on continuous self-improvement. Relatively simple program implementations for a complex spine service have afforded beneficial results. The following are a number of such measures the authors have found to be helpful in their practices.
Quality and Outcomes Conferences
Most hospitals around the world feature some form of regular morbidity and mortality reviews, some more formal than others. The morbidity and mortality reviews usually rely on a more or less voluntary self-reporting system or extracted complications from a hospital data bank. 11 Such conferences are a desirable foundation for inter- and intradisciplinary communication and provide a hopefully blame-free learning opportunity for all in attendance. As such conferences are established, the goal is to develop input and reporting systems, remain current with peer review and analysis of adverse events. Reliance on individualized self-reporting or hospital registries may lead to significant underreporting of actual adverse events. Use of a dedicated reporting system and a resource professional such as a “Quality Nurse” at the intersection of care providers and hospital administration has been described as a desirable resource to professionalize, provide a clinical lens for surveillance process, and operationalize learnings from conference.
Beyond regular case conferences, routine and standardized outcome review is the cornerstone of clinical quality efforts. Outcome review is 2-fold: (1) publication of measurements and (2) review of cases for context and identification of opportunity for improvement. One can exist without the other; however, publication of measurements without review is of limited utility. Review of cases without measurements lacks evidence and context. Publication of measurements with case review context provides the foundation for evidence-based clinical improvements and ability to measure if a change results in improvement. Ideally, measurement review in conjunction with M&M case review provides context and stimulus promotes intervention.
The following is a case study of clinical care development in partnership with clinical quality program.
Case Study: Protocols in Complex Spine Surgery Aimed to Prevent Postoperative Complications
In an effort to address complications following complex spine procedures, the most common reasons for patient readmissions and return to the operating room were regularly reviewed and analyzed over a period of 2 years. Paired with outcome measurements, 4 areas of opportunity were identified and assessed for clinical opportunities in care planning: (1) postoperative respiratory complications; (2) postoperative wound complications; (3) intractable pain; and (4) DVT (deep vein thrombosis)/PE (pulmonary embolism). As a result, 5 initiatives were developed.
“Back to Basics” Protocol
Observation: Avoidable postoperative pulmonary complications. Elevated temperatures and fever work-ups with utilization of chest radiographs that identified “nonspecific atelectasis” were a relatively common occurrence.
Idea: Promote regular simple active breathing exercises by implementing incentive spirometry use (10 times per hour while awake) as well as specific deep breathing diaphragm mobilization exercises. Prior to implementation, advance practice nurses as well as nursing leadership provided education to staff and clinic nurses related to the significance and reasoning for use. This education was essential to ensure that nursing had an adequate understanding of the rationale and importance of this therapy and could, in turn, provide patient education in the clinics and on the units. This program was started before any elective surgery during preoperative education session and then continued for the acute phase hospitalization through home use until return to the hospital for a wound check at 3 weeks postoperatively. Compliance was tracked through daily rounding and electronic medical record data capture as part of a more active patient participation program in early recovery.
Multimodal Pain Management
Observation: Preventable readmission and delayed discharges related to inadequate pain management.
Idea: To install an effective preoperative, perioperative, and postoperative pharmacologic and nonpharmacologic regimen to be instituted on all elective complex spine patients. A dedicated comprehensive complex spine order set was generated in the electronic medical record to assure accurate and consistent use of desirable medication regimens outlined for consistent provider use. In addition, nursing was instructed how to utilize multitiered pain management orders and encourage the use of conservative, nonpharmacologic pain management tools. This is an ongoing effort and has been a challenge due to widely variable opiate tolerance of patients as well as their baseline health status. It is also affected by cost consideration for some helpful medications, such as intravenous acetaminophen and liposomal-based bupivacaine, which limit their regular availability in everyday practice. Nevertheless, creative application of a “multimodal” pain management program has become a culture of care focus with ongoing efforts to find optimal solutions for any and all patient and their various specific needs and challenges.
Mobilization Initiative
Observation: Avoidable postoperative complications such as DVT/PE.
Idea: Routine early mobilization of postoperative patients through implementation of a nurse-led initiative focused on avoidance of prolonged bedrest following complex spine surgery. Nursing education focused on the benefits of mobilization and troubleshooting for challenging patient situations and included routine preoperative patient and spouse education. Expectations included assisting patient out of bed to a chair by 0700
Nutrition Protocol
Observation: Avoidable postoperative nutrition-related complications such as wound breakdown.
Idea: Implementation of a nurse led initiative that focused on preoperative and postoperative nutrition guidance, management, and care. Nutrition screening using simple clinical and few serologic parameters was conducted in the preoperative setting to identify patients at risk for wound complications and to identify nutrition needs as well as supplying information and resources to patients regarding how to meet those needs (ie, nutritional supplementation, dietary changes, and referral for nutritional consult). The hospital system supported these measures in conjunction with a sponsoring industrial partner by making protein drinks available for 5 days preoperatively and 5 days postoperatively in identified “at-risk patients” and monitoring compliance.
Glycemic Control Initiative
Observation: Preventable postoperative complications for complex spine patients.
Idea: Focus on tighter blood glucose management in the preoperative, perioperative, and postoperative stages. Concerted preoperative efforts included clinic nursing staff screening patients for HgA1c higher than 7. These patients were provided education regarding possible complications associated with the surgical procedures as well as effective methods for avoidance. Referrals were made to Endocrinology for strategizing medication management as well as working with patients’ primary care physicians to optimize HgA1c prior to surgery for elective cases.
Methods
Ongoing deidentified summary data pertinent to selected quality metrics PSI 11 (postoperative respiratory failure), PSI 12 (postoperative venous thromboembolism VTE), and postoperative surgical site infections were pulled from the hospital database of a dedicated tertiary, quaternary dedicated neurosciences center over a 4-year period (2015-2018). Internal and external validity checks were performed through internal data auditors and a contracted commercial entity (Premier, Charlotte, NC).
Findings
Although undoubtedly multifactorial, the number of wound infections in spine surgery patients at the target institution decreased from the time of program implementation to the present as follows (Table 5).
Spine Fusion Surgical Site Infection Trenda.
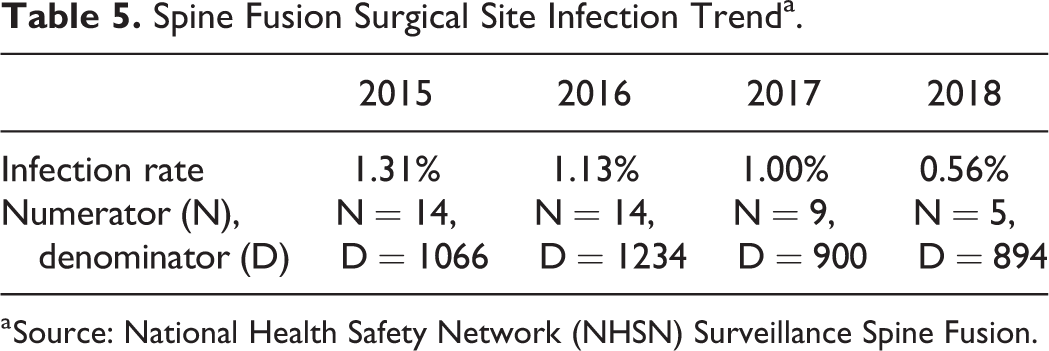
a Source: National Health Safety Network (NHSN) Surveillance Spine Fusion.
The efforts involved a coordination between the ambulatory clinics, pre-anesthesia departments, the operating room, post-anesthesia care unit, intensive care unit, and in-patient floors. In comparing pre-implementation year with full year following implementation: PSI 12, Perioperative DVT or PE, reduced 79%; PSI 11, postoperative respiratory failure reduced 45%; surgical site infection reduced 25% (Table 6).
Summary of Clinical Areas Overcome by Implementing Quality Improvement Strategies.
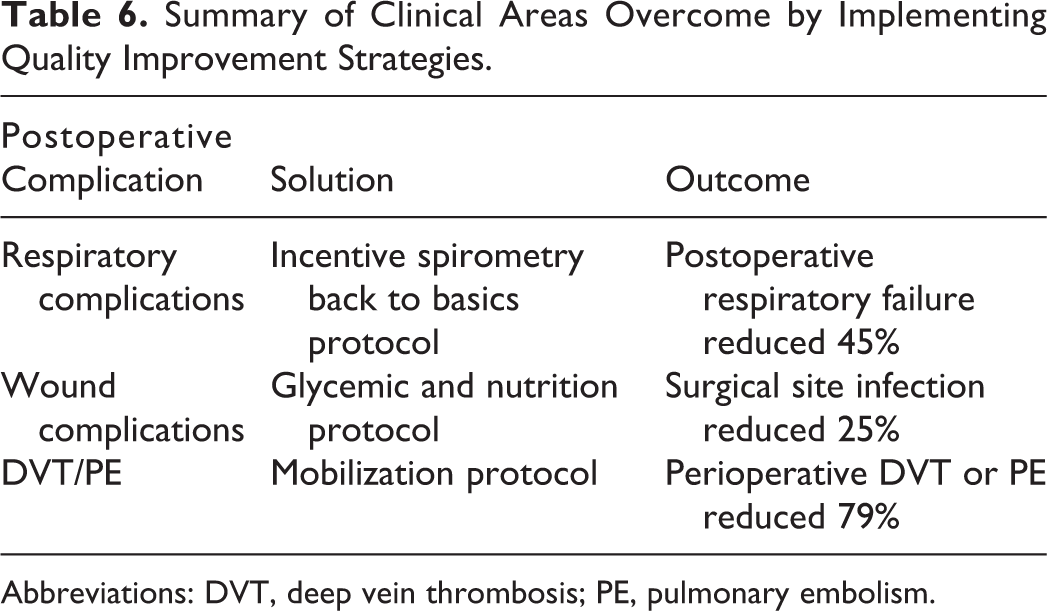
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism.
At year 2, these improvements led in removal of hospital acquired condition reimbursement penalty (CMS Hospital Acquired Conditions Reduction Program), to the financial amount of roughly US1 million annually. Additionally, CMS (Hospital Compare) star rating of facility increased by a full star. These initiatives were subsequently recognized by organizational annual quality award. Now in year 3, focus is on sustainment and anchoring the fundamentals of these initiatives into standard of care while continuously monitoring, reviewing, and adapting to meet unique needs of patients receiving complex spine care.
Summary
As previously discussed, utilizing a change model such as the Lewin model of change theory helps ensure the support necessary to maintain, sustain, and expand initiatives. The quality initiative described above met several impediments following the initial success. As part of a review process following this quality initiative we identified barriers of sustainability. Specifically,
Change in leadership and staffing
Scope of project
Disconnect between prioritization by ambulatory versus inpatient setting
Implementation of a multifaceted quality initiative requires the support of many individuals across settings. The above initiative was implemented over the course of a year, at a time when we saw turnover at many leadership levels as well as staffing at the RN level (the strongest driver of this initiative). With rapid turnover and use of temporary, agency, and per diem staffing, the commitment to the program slowed. In addition, the overall scope of this project was wide. With 5 separate initiatives woven into one larger all-encompassing initiative we found it difficult to perform the audits and continued education necessary to support the program. Last, despite a committed group of individuals in the ambulatory and inpatient setting, each location prioritized the initiative at various levels. For the clinic this initiative was a driving force in the work that RNs were performing. That being said, inpatient nurses were required to meet numerous metrics, only one of which was the above initiative.
Although our complication, readmission, and return to operating room rates remains at an admirable level we continue to find room for ongoing improvement. The challenge remains, how to embark on an ongoing process of course correction without loss of initiative and momentum, especially in times of ever-present cost-cutting efforts by hospital administrations. Recommendations include the development of an interdisciplinary group with representatives from each setting, identification of a champion(s) to support this effort, developing attainable auditing measurements to ensure compliance, and development of a standardized training for onboarding so the initiatives become part of the culture that new staff are presented with. In the big picture perspective having a regular reporting mechanism that is supported and recognized by the overall hospital system and then is duplicated in other facilities within the system can create a setting for ongoing quality initiatives and a sustained drive for improvement as part of the organizational culture—starting with each individual practitioner to the hospital and from there to its health care system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by funding from AO Spine North America.