
Abstract
Study Design:
Retrospective cohort.
Objectives:
To evaluate the long-term effect of convex growth arrest (CGA) on coronal deformity correction in congenital scoliosis.
Methods:
Twenty-two patients with congenital scoliosis operated by 1-staged double approach hemiephysiodesis by bone grafting of the convex side without instrumentation are included. Eighteen curves had an isolated hemivertebra while 4 curves had congenital bar. Subgroup analysis was performed according to age at surgery (3 years cutoff), type of malformation (hemivertebra vs congenital bar), and severity of curve (35° cutoff).
Results:
Patients’ mean age at surgery was 3 years (range 0.5-8 years), with a mean frontal Cobb angle of 40.59°. Mean follow-up is 10.7 years (range 5.5-25 years). Overall results showed mean frontal Cobb angle reduction of 35.47% (40.59° to 27.41°). Detailed analysis showed that 15 curves had a mean correction of 51.8%, 5 stabilized and 2 had a mean aggravation of 25.11%. Subgroup analysis revealed that patients operated ≤3 years of age had mean cobb angle correction of 43.1% versus 21.49% in patients operated >3 years (P = .140). Mean correction of 44.5% was gained in curves with isolated hemivertebra compared with 1.3% in curves with congenital bar (P = .004). A 58.17% mean correction was reached in curves ≤35° versus 23.68% in curves >35° (P = .032).
Conclusions:
A limited convex hemiepiphysiodesis still has a place in congenital scoliosis care when it is performed in patients ≤3 years old, with curves ≤35°, and with isolated hemivertebra. It spares patients the risks of vertebral resection and instrumentation, while fusing the same number of levels.
Introduction
Convex anterior and posterior hemiepiphysiodesis, also known as convex growth arrest (CGA) is a growth modulating procedure that was regularly used to treat congenital progressive spine deformity in children. 1 –3 Congenital spine deformities in children result from abnormal vertebral segmentation (hemivertebra, congenital bar malformation, more complex malformations) leading to a progressive longitudinal deformity. 4,5 This deformity is due to an imbalance in the spine curve where convexity outweighs the growth at the level of the concavity. The compressive side of the deformity sustains supraphysiological loads that suppress the growth at the physis. 6 –8 CGA aims at controlling the spine deformity by inhibiting growth, anteriorly and posteriorly, on the convex side of the curve, allowing the concave side to grow and compensate the deformity in the following years. 2,4,9
Some special indications for CGA have been discussed, including a progressive pure scoliotic curve without major kyphosis or lordosis, patients aged less than 5 years, without unilateral segmental bar, with no cervical spine involvement. 10 –12 Other studies recommended that CGA is a possible and safe procedure in patients aged younger than 5 years regardless of other curve specifications 4 .
After being, for many years, the treatment of choice of congenital spine deformity, CGA progressively fell out of favor during the past years. 1,8 An unacceptably high rate of failure, the need of an anterior approach to the spine, the absence of immediate postoperative result and the uncontrollable and unpredictable results of the technique were CGA’s major drawbacks. 4,12,13 Hemivertebra resection followed by posterior fusion seems to be nowadays the treatment of choice permitting immediate correction of the deformity, and a more predictable outcome in the aftermath of this intervention. 4,5,14 However, hemivertebra resection is associated with higher blood loss, longer operative time, and more neurologic incidents and complications. 5,15
Keeping in mind that correction of deformity after hemiepiphysiodesis is a chronic and slowly progressive phenomenon, long-term follow-up is needed before definitive outcome is fixed. Little is known about this subject since no recent series with long-term follow-up were reported in the medical literature. To our knowledge, this is the first report in the medical literature to comment on very long follow up series of congenital scoliosis treated with CGA, discussing the place of anterior posterior hemiepiphysiodesis in the treatment of congenital scoliosis.
Material and Methods
This is a retrospective study that was approved by the ethics committee of our institution. Involved individuals are patients with progressive congenital scoliosis with hemivertebra or congenital bar, operated on with CGA in the same center, by 2 senior spine surgeons (KK and GK) between 1990 and 2010. All patients operated on during this period, whose records and radiographs are available are included in the study. Patients operated on of instrumented vertebral fusion, and those with associated syndromes and malformations (including medullary malformations) were excluded. During this period, CGA was the only surgical technique performed in all patients with progressive congenital scoliosis with hemivertebra or congenital bar.
Twenty-two patients (11 girls and 11 boys) formed the cohort of this study. Eighteen patients had an isolated hemivertebra, and 4 patients had an associated congenital bar. One staged, double approach, hemiepiphysiodesis is done by bone grafting of the convex side of the curve, without instrumentation (Figure 1). Only the convex side of the curve was exposed and autologous bone graft (rib if thoracic or thoracolumbar CGA, iliac bone graft if lumbar CGA) was solely used. Limited fusion is defined as the fusion centered over the hemivertebra, including the 2 adjacent levels (Figure 2). Extensive fusion is the one carried on more than one adjacent vertebra to the hemivertebra, proximally and/or distally, expanding fusion to the most tilted vertebra (Figure 2). Technically, CGA was performed as previously described and a postoperative cast was worn 1 week after the surgical intervention for a mean period of 12 weeks for maintenance. No braces were used thereafter.
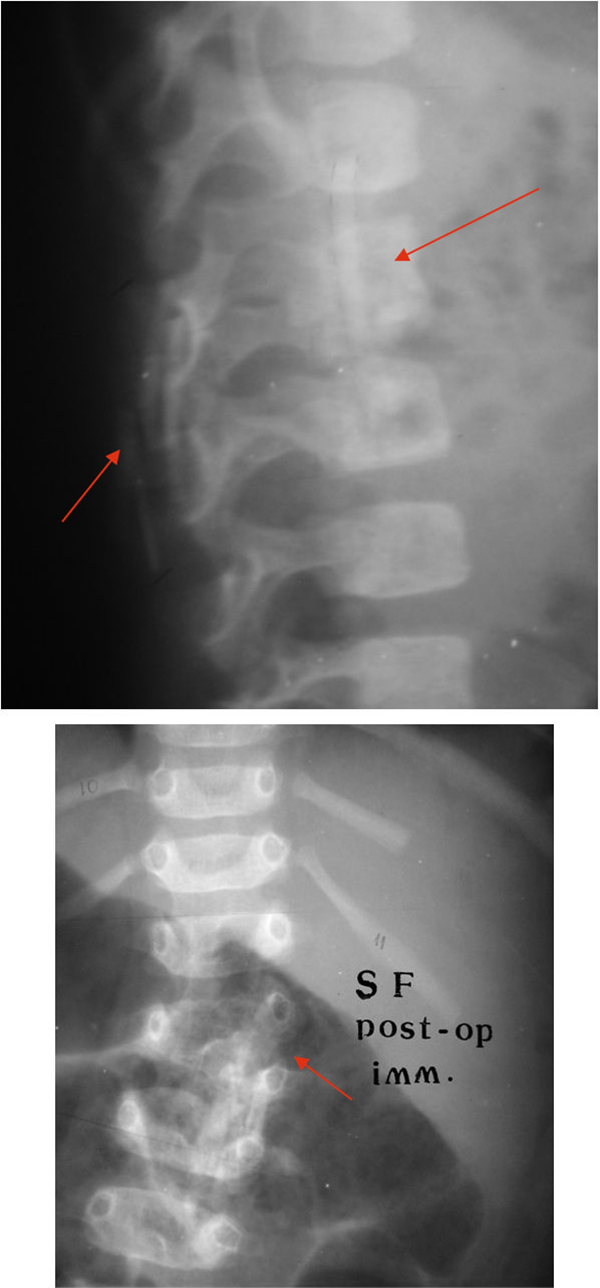
Anteroposterior and lateral dorsolumbar X-rays showing the immediate postoperative changes in a patient with L3 hemivertebra operated of anterior and posterior convex hemiepiphysiodesis. Red arrows point to the bone graft.
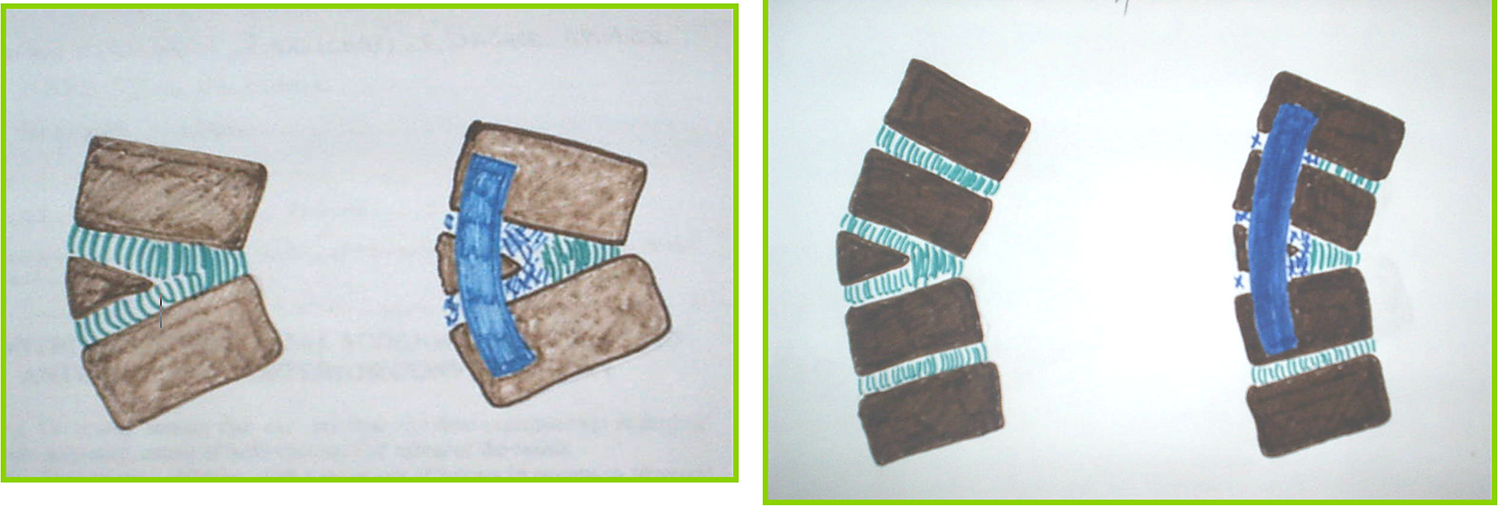
Schematic representation showing limited fusion to the left and extensive fusion to the right.
Evaluated variables were Cobb angles of the scoliotic curves preoperatively and at the last follow-up. Primary endpoint is degree of variation (reduction or increase) of the frontal Cobb angle between the preoperative setting and the last follow-up (
Statistical analysis comparing variation of frontal Cobb angle between the preoperative setting and the last follow-up was performed between the 2 subgroups in each of the 3 categories (age at surgery, type of malformation, and severity of the curve). It was performed using SPSS for Windows, version 23.0, and P values less than .05 were considered statistically significant. Independent Student t test was used to compare means. χ2 test was used to compare binary variables.
Results
The minimum follow-up was 66 months (5.5 years) and the mean follow-up was 128.5 months (10.7 years; range 66-300 months). Mean age at surgery was 3 years (range 0.5-8 years). Mean frontal Cobb angle was 40.6°. Deformity was dorsal in 4 patients, dorsolumbar (D10-L2) in 9 patients and lumbar in 9 patients. Limited fusion was performed on 16 patients (mean curve of 37.2°) while extensive fusion was performed on 6 patients (mean curve of 50.3°). Surgeons generally opted for extensive fusion in the majority of cases where there was a congenital bar, a severe curve, and in older patients. Blood loss averaged 80 mL per patient, and mean operative time was 135.7 minutes.
When all 22 curves were taken together, there was a mean frontal Cobb angle reduction from 40.6° pre-operatively to 27.4° (reduction of 32%) at last follow-up. Fifteen curves (approximatively two-thirds of curves) had a mean frontal Cobb angle reduction of 20.5° (51.8%). Five curves (22.72%) stabilized, with a mean Cobb angle of 39.8°. Two curves (9.09%) had an aggravation of their frontal Cobb angle of 11.5° (25.11%) at last follow-up. The 16 curves where limited fusion was adopted had a mean Cobb angle of 37.2° had a mean correction of 44.8%. The remaining 6 curves (mean Cobb angle of 50.3°) that were extensively fused had a mean correction of 11.3%. Table 1 shows the detailed data for all included 22 patients.
Detailed Individual Data for the 22 Patients Including Age at Surgery, Type of Malformation (HV or CB), Pre- and Postoperative Cobb Angles of the Involved Spinal Curve and the Follow-up.
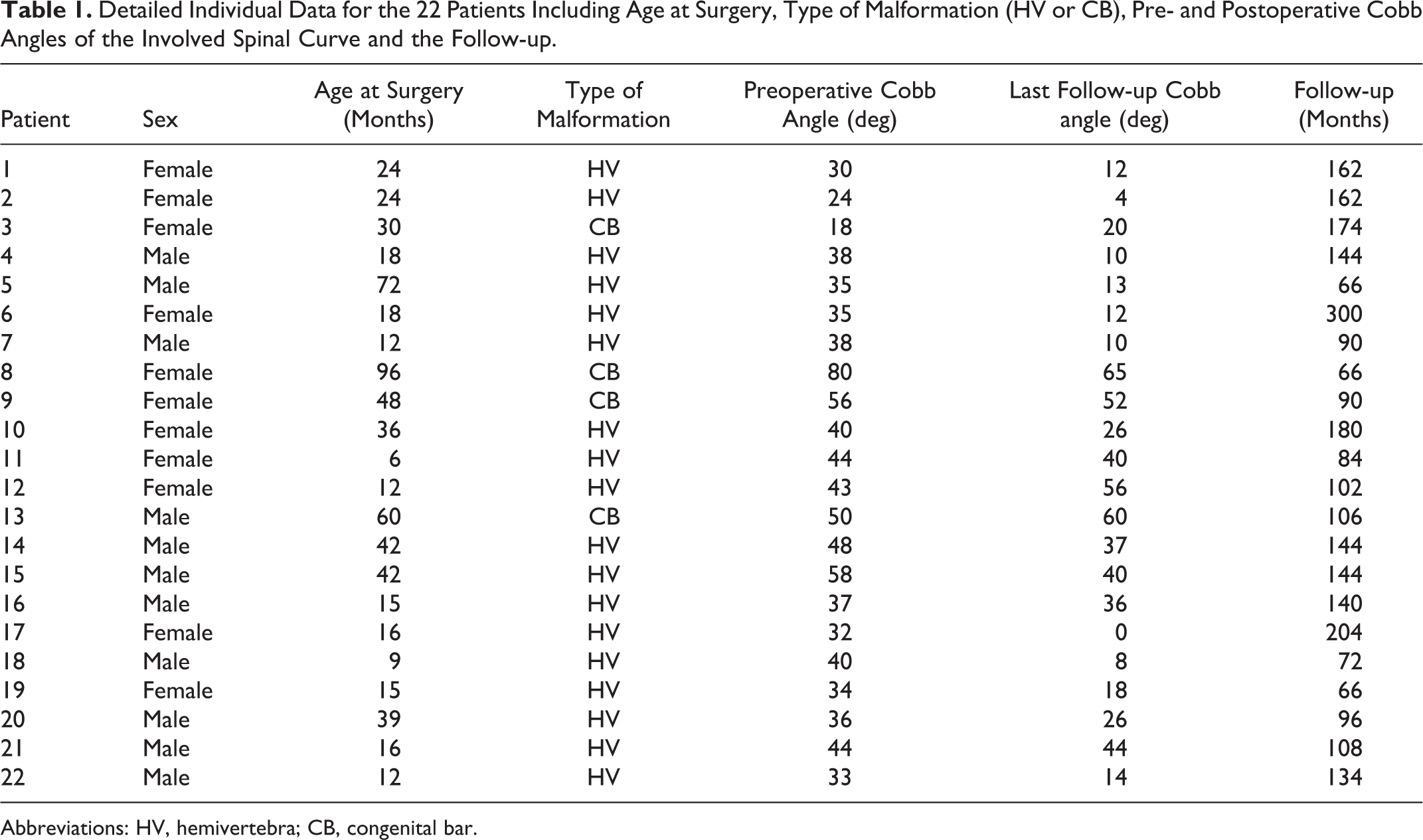
Abbreviations: HV, hemivertebra; CB, congenital bar.
Subgroup Analysis
Age
The subgroup analysis (Table 2) revealed that patients operated on at or before the age of 3 years (15 patients) had a mean correction of 43.1% in their curves compared with a mean 21.5% of correction in patients operated after the age of 3 years (7 patients) (P = .140).
Results of the Statistical Analysis According to the Subgroups Repartitions of Patients.a
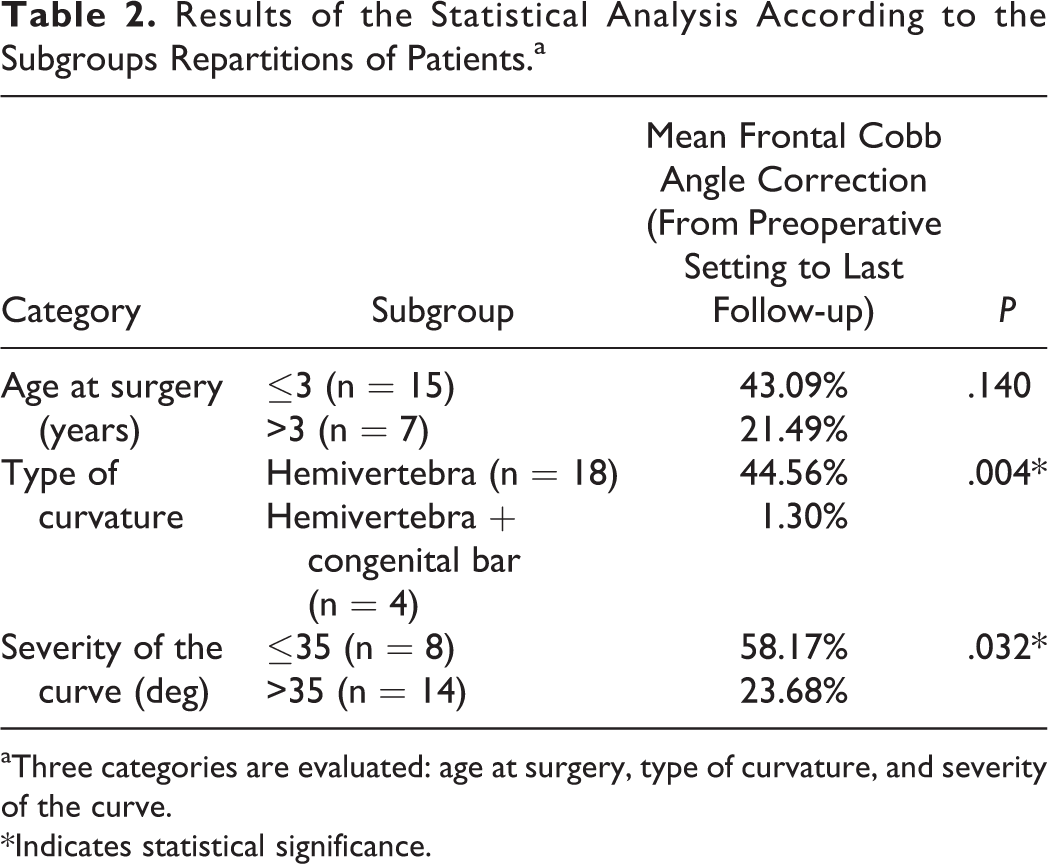
aThree categories are evaluated: age at surgery, type of curvature, and severity of the curve.
*Indicates statistical significance.
Type of Malformation
A mean frontal Cobb angle correction of 44.6% was gained in curves with isolated hemivertebra (18 curves) compared with 1.3% of correction in curves with hemivertebra and congenital bar (P = .004).
Severity of the Curve
A 58.2% mean frontal Cobb angle correction was reached in curves ≤35° (8 patients) matched to 23.7% of mean correction in curves >35° (P = .032).
In the subset of patients (4 patients) with curves greater than 35°, having a congenital bar and an hemivertebra, and operated on after the age of 3 years, limited fusion performed in 1 case led to a progression of the curve, and extended fusion performed in 3 patients led to stabilization in 2 curves and to reduction of Cobb angle in 1 curve at the last follow-up.
No intraoperative nor perioperative neurologic or hemodynamic complications, were reported in this series. No respiratory complications were recorded after the anterior approach, even in patients with thoracic CGA. No cases of pseudarthrosis or chronic pain were noted. One case of superficial infection of the posterior approach wound was reported treated with oral antibiotic therapy and local wound care. No revision surgery was performed on any of the patients.
Discussion
CGA used to be one of the most used techniques in the treatment of congenital scoliosis in children. 2,10,11,13 It was popularized because of its simplicity, efficacy, low morbidity, and low cost when compared with other alternatives. 4,16 However, the high rate of curve progression observed with some series (reaching 21% with Keller et al 16 ) led spine surgeons to look for alternatives. However, knowing that the results cannot be judged in the immediate postoperative setting, long-term follow-up is a necessity.
The literature shows multiple series with variable follow-ups ranging from 2 years 4 months to 8 years 10 months. 4,10 This is the first study in the medical literature with a mean follow-up of more than 10 years (range 5.5-25 years); 15 patients (66.67%) of the 22 included patients reached skeletal maturity at time of last follow-up. This study showed that 68.2% of curves had an epiphysiodesis effect, 22.72% had a fusion effect, and 9% of patients had no or minimal effect, and their curve progressed. This rate of deterioration is comparable to that of the majority of series reported in the medical literature. 2 –4 However, this long-term study was in favor of the preponderance of epiphysiodesis effect over fusion effect; a finding that was presented in only 2 of the series reported in the literature. 10,13 In the majority of cases, fusion effect was the most common finding.
The heterogeneous results obtained from different series in the medical literature could not be solely attributed to lack of long-term follow-up. Many attempts were made in the past to diffuse specific indications limiting the utilization of CGA to certain subgroup of patients. 10,12 Uzumcugil et al 4 concluded that this procedure can be performed in patients with cosmetic congenital curves, younger than 5 years, regardless of the remaining associated characteristics. 4
Our subgroup analysis divided patients by age. A cutoff below the age of 5 years was previously chosen as it is known that the fastest growth in spine occurs in the first years of age. In our study, age 3 years was chosen being the median age of our included patients. Statistical analysis showed a greater, improvement in correction of curves in patients operated at or before the age of 3 years, tending into being significant. Patients were also divided into subgroups depending on the curves type. A statistically significant difference in mean correction was found between curves with isolated hemivertebra and those with hemivertebra and congenital bar, in favor of the first group. Finally, patients were divided according to the severity of their curve. The cutoff was chosen as a mid-value between the Cobb angle defining scoliosis (10°) and the Cobb angle traditionally known to be the upper limit of CGA indication (50°). 4 Therefore, 35° was chosen, and curves ≤35° had a statistically significant better correction when compared with curves ≥35°.Hence, patients having an isolated hemivertebra with a curve of 35° and less were those who would benefit the most from CGA. Patients younger than 3 years would probably benefit from this intervention also.
Extensive fusion was used in older patients presenting with congenital bar and severe deformity. It yielded in these cases 2 fusion effects and 1 progression. However, when limited fusion was carried on older patients, those with congenital bar, and in those with severe curves, the outcome was a stabilization of the curve and also possibility of progression when all these factors were combined together. Consequently, it is advised to reserve limited fusion to patients aged 3 years or less, having an isolated hemivertebra with a curve of ≤35° (Figure 3). In the cases where the patient was older, having a congenital bar or a severe curve, other surgical alternatives should be sought for (growing rods, expandable rib procedures, hemivertebra resection, spinal osteotomies with fusion.) considering the lack of correction witnessed after the long-term follow-up when extensive fusion was used in these patients.
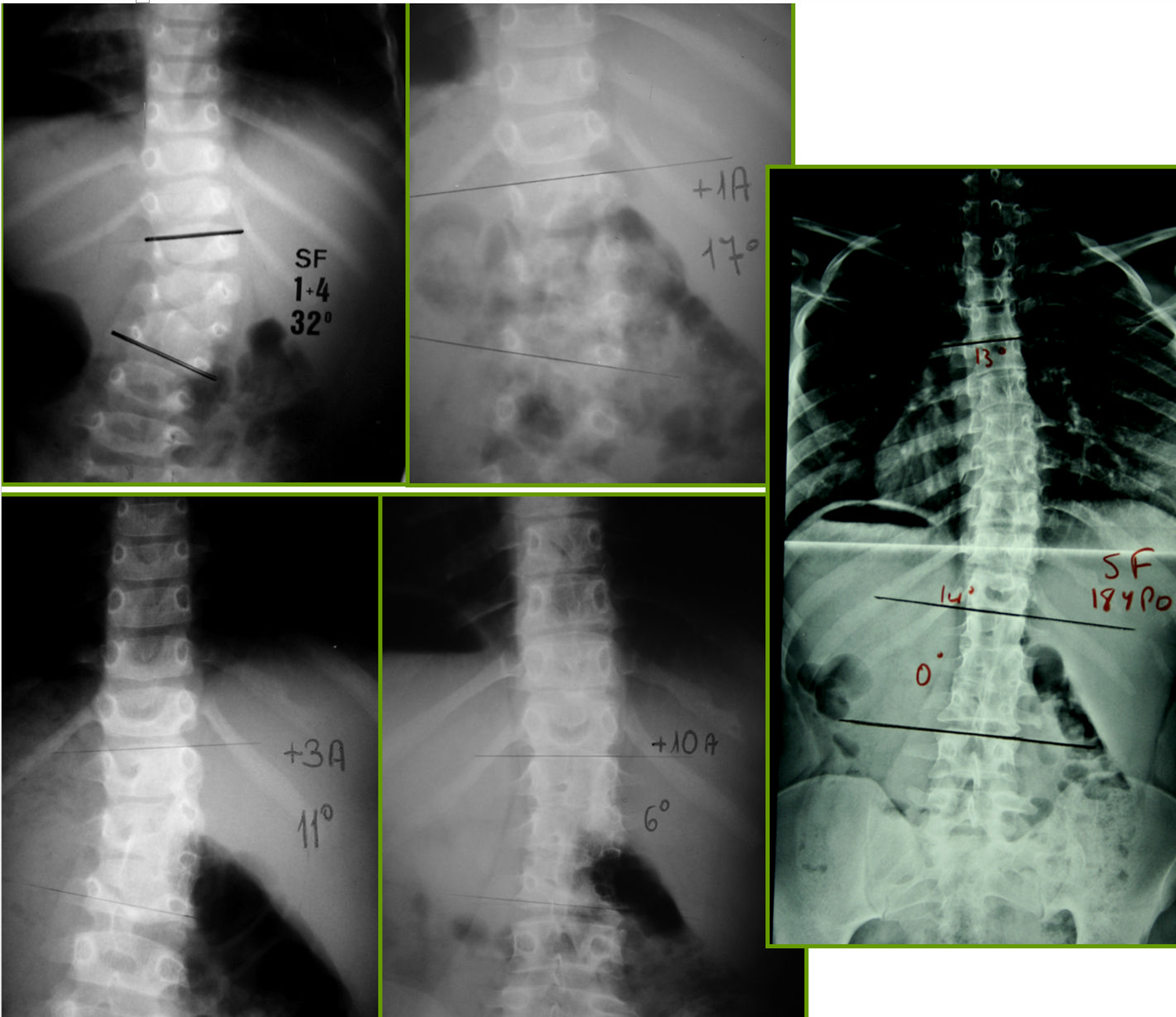
Anteroposterior dorsolumbar X-rays of a patient with L3 hemivertebra operated of anterior and posterior convex hemiepiphysiodesis in the preoperative setting, and at 1 year, 3 years, 10 years, and 18 years postoperatively.
Despite better correction and better final result reached in patients with congenital scoliosis operated of hemivertebra of congenital bar resection, 14,15,17 one should note the nonnegligible rate of complications, especially mechanical ones reported more and more leading to more instrumentation, higher costs, wider fusion, and more surgical reinterventions. 14,15,17
Despite being a census of all operated cases in a single center between 1990 and 2010, the main limitation of this study remains the limited size of the population. However, congenital scoliosis is an uncommon pathology and similar published studies had comparable population size. Another limitation is the retrospective design of this study. Knowing the long-term follow-up needed to judge the definitive result of this technique and the low incidence of this disease, prospective design is not feasible. More, this study is limited by the absence of the evaluation of the spinal deformity in the sagittal plane. The main aim of the study was to evaluate the effect of CGA on coronal deformity, and knowing that sagittal segmental abnormality does not have a negative effect on the control of scoliosis in the majority of patients with progressive congenital scoliosis with hemivertebra, sagittal profile was not analyzed in this cohort. 9 The lack of a comparator group may be considered as a limitation, however CGA was the only performed technique for all patients with progressive congenital scoliosis during the study period, and having a comparator group was impossible in this retrospective design. One last limitation to this study is the lack of stratification on the subtypes of hemivertebral segmentation. This was done on purpose to group patients with similar deformities together to have comparable groups due to the limited size of the population.
Conclusion
Single staged convex anterior and posterior hemiepiphysiodesis followed by maintenance cast for 3 months still have its place in congenital scoliosis care. It is advised to reserve limited fusion to patients aged 3 years or less, having an isolated hemivertebra with a curve of ≤35°. Good correction is expected in these patients as shown in this long-term follow-up series. This technique spares patients the risks and costs of vertebral resection and instrumentation, while fusing the same number of levels.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.