
Abstract
Study Design:
Retrospective cohort study.
Objective:
To determine the effects of operative time on postoperative complications in patients age 65 and older undergoing posterior lumbar fusion.
Methods:
All patients age 65 and older undergoing posterior lumbar fusion were identified in the 2012 to 2015 American College of Surgeons National Surgical Quality Improvement Program database. The primary outcome measures were complications occurring up to 30 days postoperatively, including death, any complication, and complication subtypes. The primary independent variable was operative duration. Both bivariate and multivariate analyses utilized logistic regression and analyzed operative duration as a continuous variable. Statistical significance was considered P < .05.
Results:
A total of 4947 patients age 65 and older undergoing posterior lumbar fusion were identified. The mean operative time was 3.3 hours (SD 1.7). The overall complication rate was 13.4% (n = 665). In multivariate analysis, each incremental hour of operative time was associated with increased risk of postoperative thromboembolism (odds ratio [OR] = 1.23; 95% confidence interval [CI] = 1.10-1.37), transfusion (OR= 1.25; 95% CI = 1.18-1.32), urinary tract infection (OR = 1.21; 95% CI = 1.10-1.32), and total postoperative complications (OR = 1.22; 95% CI = 1.16-1.27).
Conclusion:
For patients age 65 and older undergoing posterior lumbar fusion, longer operative time is associated with greater risk for thromboembolism, transfusion, intubation, kidney injury, urinary tract infection, surgical site infection, and overall postoperative complications. This data highlights several specific complications that are influenced by operative time in older patients, and further supports the need for future protocols that seek to safely minimize operative time for posterior lumbar fusion.
Introduction
Patients age 65 and older represent the fastest growing cohort in the United States, which is estimated to double by 2050. 1 In addition, the prevalence of chronic low back pain in patients age 65 and older has been increasing over time, which has been mirrored by increasing number of spinal fusions. 2 -5 However, the growing population of older patients undergoing spinal procedures is also exhibiting an increasing rate of comorbidities, contributing to a disproportionately higher risk of complications. 6 -12
Studies have shown that increasing operative time remains a risk factor for postoperative complications among other specialties, including plastic surgery, 13 breast reconstruction, 14 gynecology, 15 and general surgery. 16,17 For spinal cases, previous studies have focused on all patients undergoing specific procedures, such as fusion for adult spinal deformity, 18 lumbar fusion, 19 and instrumented spinal fusion. 20 Age has also been found to be an independent risk factor for postoperative complications among lumbar spine patients, 20 -23 as well as among other specialties. 10,24 -26 However, there is a need for investigation for the implications of operative time among the growing population of elderly lumbar spine patients.
The current study aims to determine the critical operative duration at which more complications occur, as well as which complications increase as operative time increases in patients over the age of 65 undergoing posterior lumbar fusion. By identifying specific ages, time points, and complications, physicians can not only be more aware of the risks of operative time but also prepared for complications that are most likely to occur.
Methods
Data Source
Data was obtained from the American College of Surgeons National Quality Improvement Program (ACS NSQIP) dataset, years 2012 to 2015. The NSQIP collects data from member hospitals for surgical procedures, including patient characteristics (eg, age, sex, weight, height, American Society of Anesthesiologists [ASA] Classification), procedure characteristics (eg, operative duration, procedure codes), and 30-day complications. As the NSQIP is both publicly available and deidentified, this study was not considered human subjects research and was therefore deemed exempt from institutional review board consideration.
Patient Selection
Patients were preliminarily included in the study based on presence of a primary listed Current Procedural Terminology (CPT) code for posterior/posterolateral lumbar fusion (22612). Patients were subsequently excluded if they exhibited any of the following characteristics: age <65, nonelective surgery, revision surgery, emergent surgery, and outpatient surgery, as well as preoperative ventilator dependency, ascites, congestive heart failure within 30 days preoperatively, renal failure, dialysis, disseminated cancer, preoperative open/infected wound, pathologic weight loss, sepsis, and totally dependent functional health status. Patients were also excluded if they underwent spinal fusion at nonlumbar levels or with technique other than posterior/posterolateral, as evidenced by presence of CPT codes 22554, 22585, 22558, 22556, 22551, 22552, 22533, 22532, 22534, 22634, 22633, 22632, 22630, 22600, or 22610. Characteristics of excluded patients are detailed in Supplemental Table S1 (available in the online version of the article); select patients were excluded on multiple criteria.
Outcome Measures
The primary outcome measures in this study were complications occurring up to 30 days postoperatively, including death, any complication, wound dehiscence, pneumonia, urinary tract infection (UTI), stroke/cerebrovascular accident (CVA), transfusion within 72 hours postoperatively, surgical site infection (SSI), sepsis, acute kidney injury (AKI), thromboembolism, major adverse cardiac event (includes cardiac arrest and myocardial infarction), and postoperative intubation.
Independent Variables
The primary independent variable was operative duration, expressed in hours. Variables considered as potential confounders included age group, sex, body mass index (BMI) category, and number of levels fused. Levels fused was calculated as the total number of CPT codes corresponding to single or additional levels of posterior/posterolateral lumbar fusion (22612 and 22614).
Statistical Analysis
Descriptive statistics for both independent variables and postoperative complications were generated. Both bivariate and multivariate analyses utilized logistic regression and analyzed operative duration as a continuous variable. Model discrimination and fit were assessed with the c-statistic and Hosmer and Lemeshow goodness-of-fit (HF GOF) test, respectively. The analyses of postoperative transfusion indicated initial poor GOF. The model was subsequently refined by the removal of ASA classification, yielding a model with HF GOF test P > .05 (ie, achieving a good fit). Analyses of stroke/CVA indicated initial overfitting, resolved via sequential removal of variables with the lowest Wald χ2 values (ASA classification, BMI category, and levels fused). All statistical analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC). Statistical significance was considered P < .05.
Results
Descriptive Statistics
In total, 4947 patients were analyzed. The mean operative duration was 3.3 hours (standard deviation [SD] 1.7). The majority of patients were aged 65 to 69 years (34.4%, n = 1700), followed by age 70 to 74 years (30.7%, n = 1519). Most patients were female (57.3%, n = 2836) and with ASA classification of 3 (59.9%, n = 2960). Most patients were of BMI category 25.0 to 29.9 kg/m2 (35.2%, n = 2074), followed by 30.0 to 34.9 kg/m2 (28.7%, n = 1693). The majority of procedures involved a single level (48.0%, n = 2373) or 2 levels (40.6%, n = 2009; Table 1). Complications occurred in 13.4% (n = 665) of patients overall. The most common complication was blood transfusion (6.3% of patients, n = 313; Table 2).
Patient Characteristics.
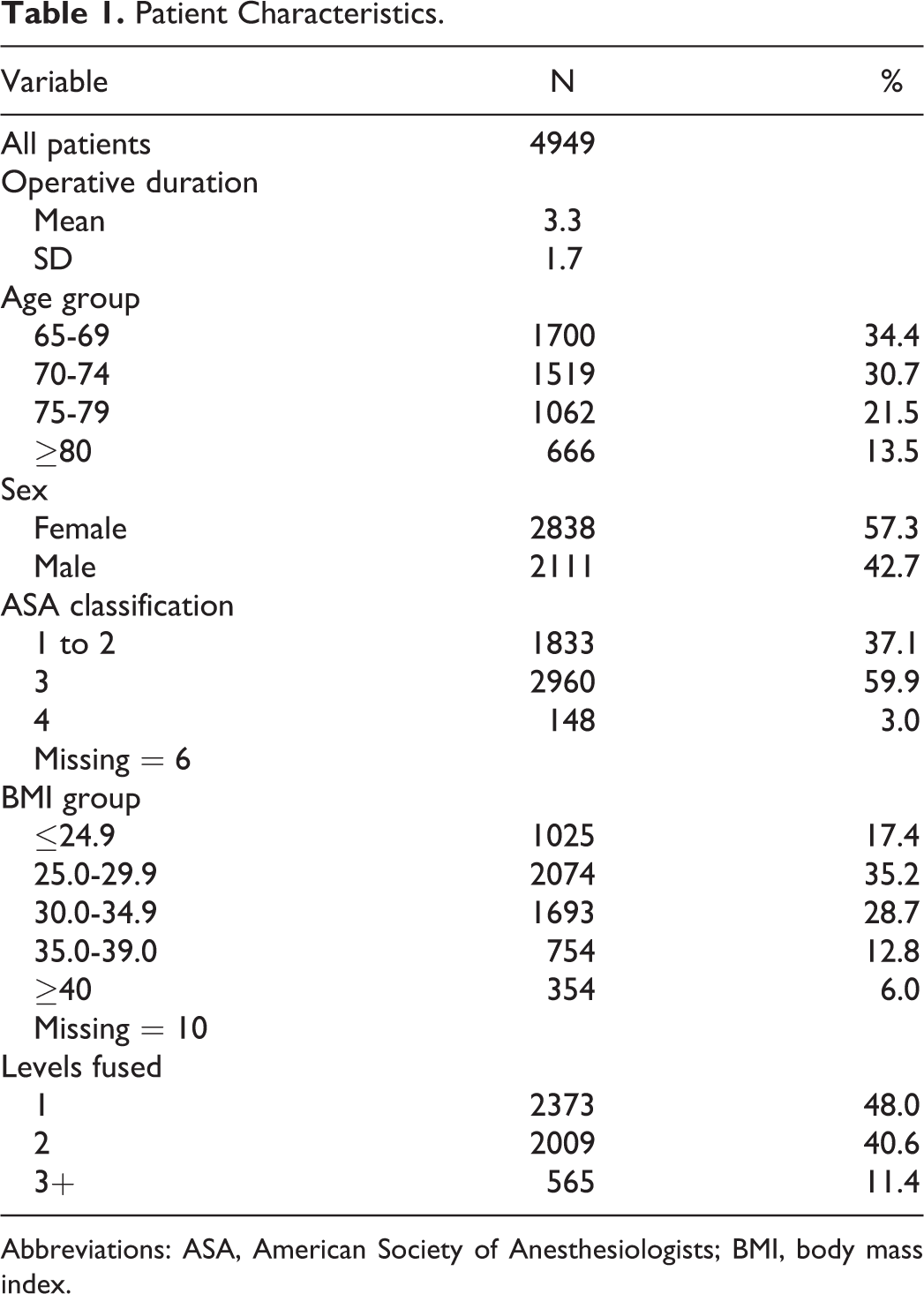
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index.
Complication Frequency.
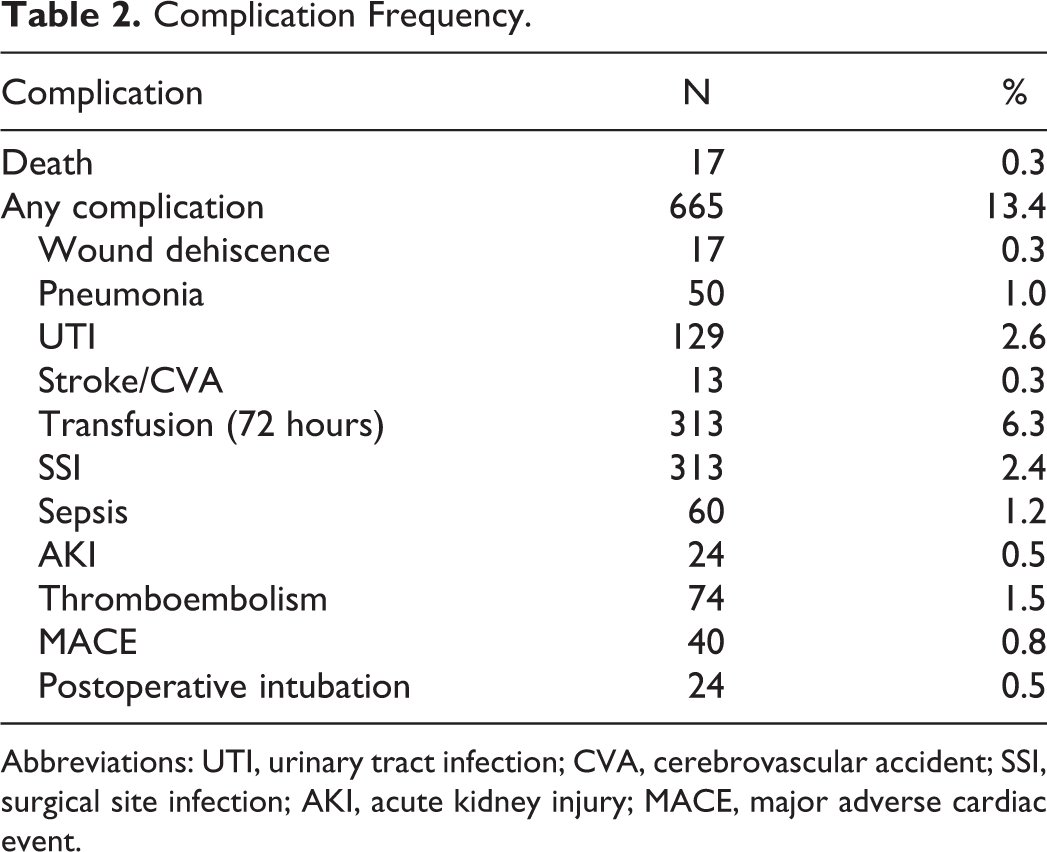
Abbreviations: UTI, urinary tract infection; CVA, cerebrovascular accident; SSI, surgical site infection; AKI, acute kidney injury; MACE, major adverse cardiac event.
Bivariate Analyses
On bivariate analyses, operative duration was associated with significantly higher rates of any complication (P < .0001), UTI (P < .0001), transfusion (P < .0001), AKI (P = .0428), thromboembolism (P < .0001), and postoperative intubation (P = .0323; Table 3).
Bivariate Analyses.
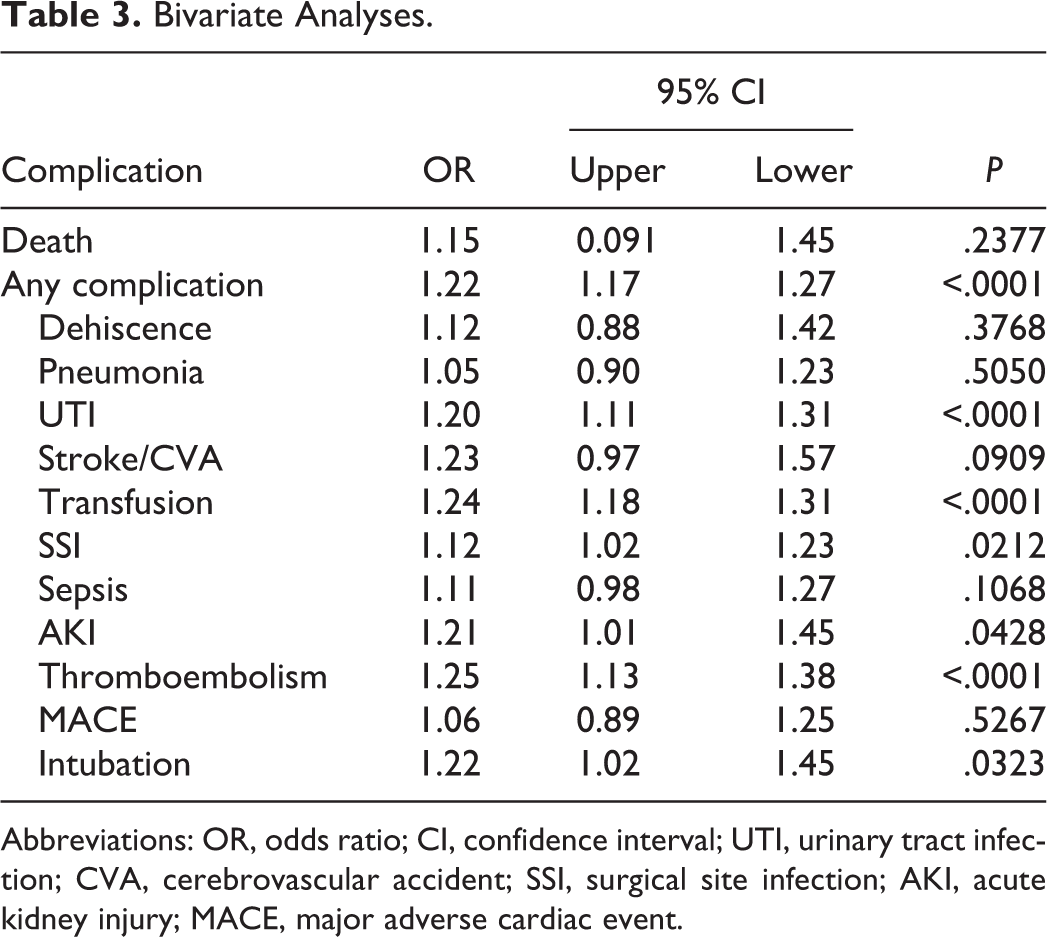
Abbreviations: OR, odds ratio; CI, confidence interval; UTI, urinary tract infection; CVA, cerebrovascular accident; SSI, surgical site infection; AKI, acute kidney injury; MACE, major adverse cardiac event.
Multivariate Analyses
After adjusting for confounding factors, each incremental hour of operative duration was associated with higher odds of any complication (odds ratio [OR] = 1.22, 95% confidence interval [CI][ = 1.16-1.27, P < .0001; Figure 1), UTI (OR = 1.21, 95% CI = 1.10-1.32, P < .0001), transfusion (OR = 1.25, 95% CI = 1.18-1.32, P < .0001), and thromboembolism (OR = 1.23, 95% CI = 1.10-1.37, P < .0001; Table 4 and Figure 2).
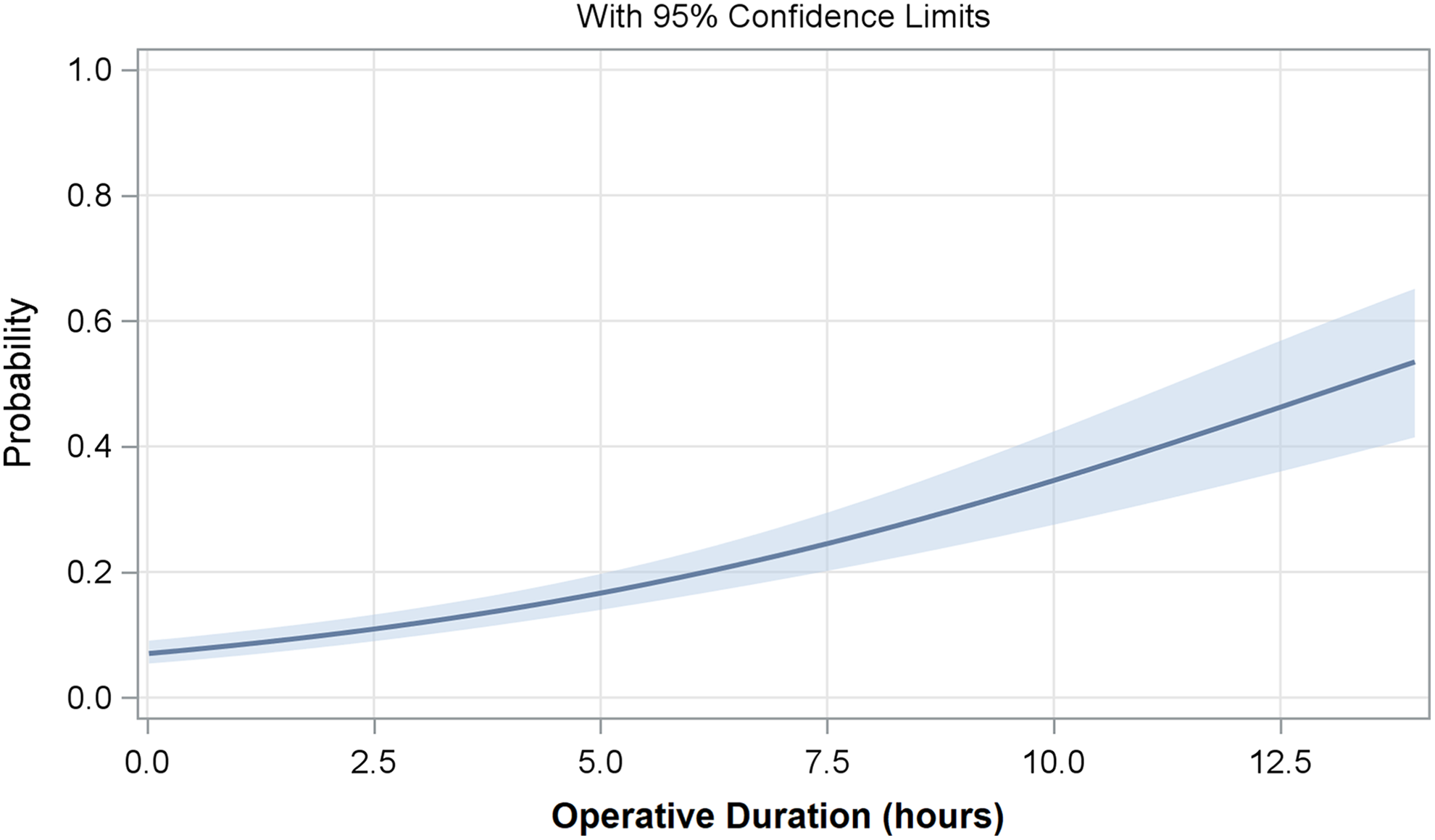
Predicted probability of any postoperative complications as a function of operative duration.
Multivariate Analyses.
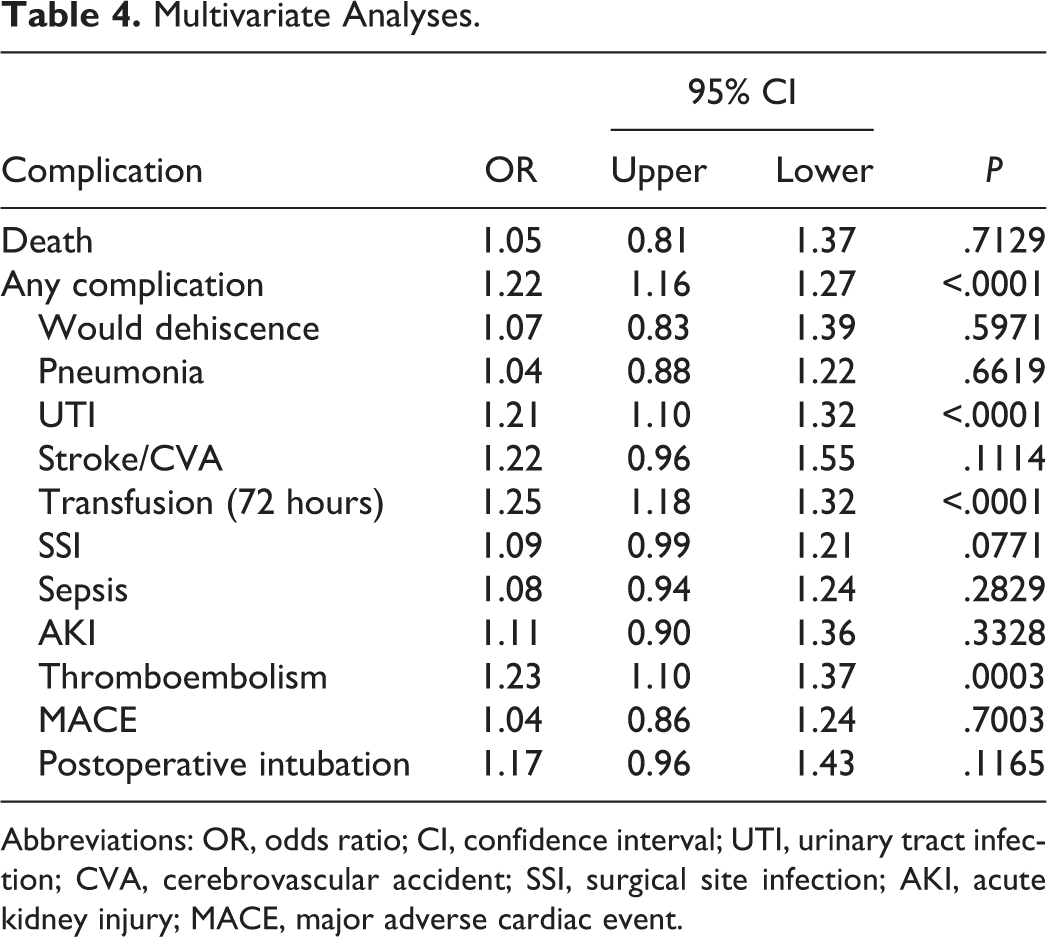
Abbreviations: OR, odds ratio; CI, confidence interval; UTI, urinary tract infection; CVA, cerebrovascular accident; SSI, surgical site infection; AKI, acute kidney injury; MACE, major adverse cardiac event.
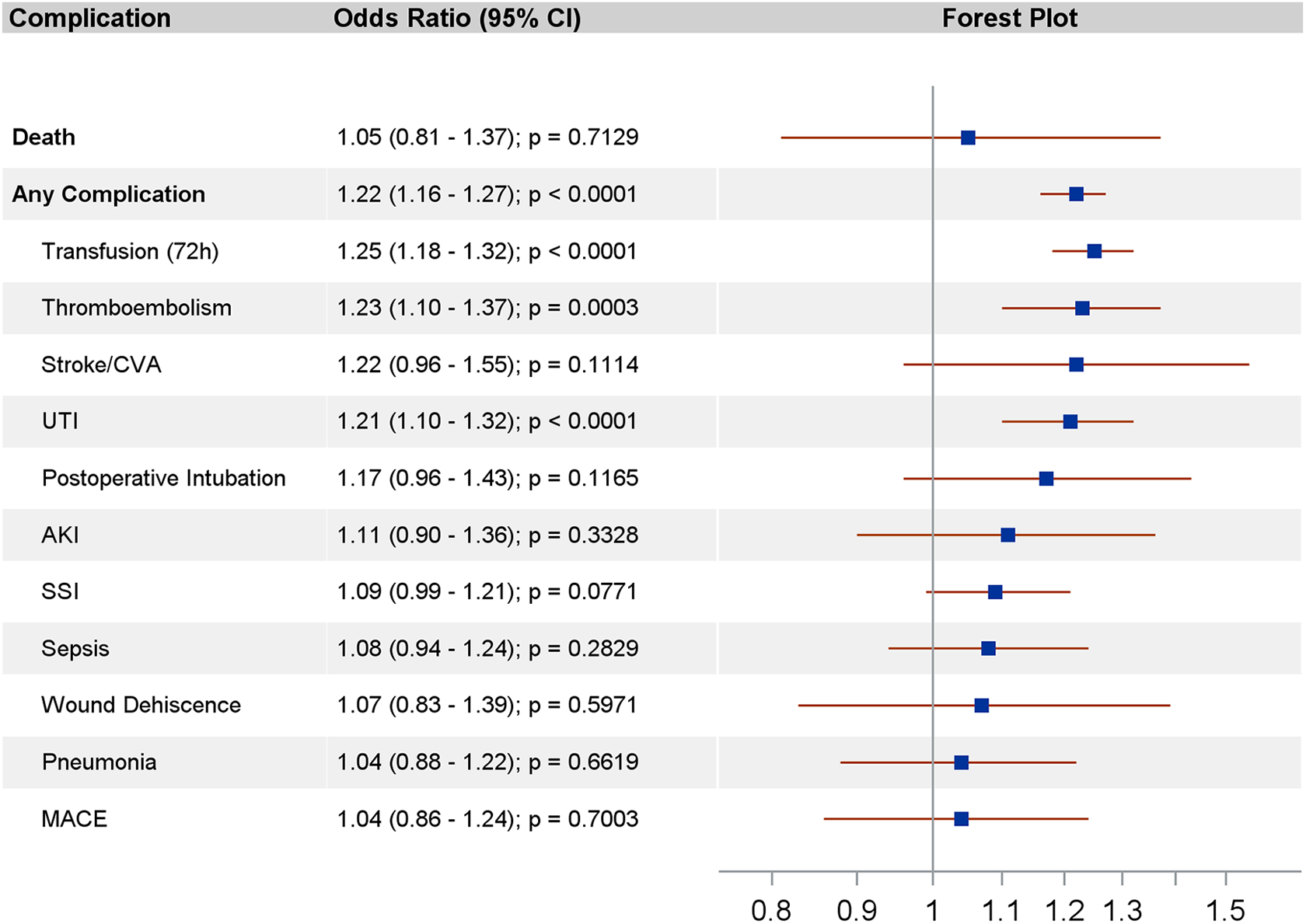
Adjusted association of operative duration and complications.
Discussion
This is the first large database analysis of the incremental effects of operative time on postoperative complications in elderly patient undergoing posterior lumbar fusion. In patients age 65 and older, each incremental hour in operative duration was independently associated with increased odds of postoperative thromboembolism, transfusion, UTI, and total complications. Patients with baseline preoperative risk of complications, such as patients with renal failure, preoperative infection, malignancy, or emergent surgeries, were excluded from analysis; this study therefore highlights the independent effects of operative time on postoperative complication in older, stable patients.
Overall, the rates of postoperative complications in this patient cohort were low, with the most common being transfusion (6.3%), UTI (2.6%), and SSI (2.4%). The postoperative complications identified in this patient cohort are similar to those among previous identified in elderly spine patients, 27,28 and all patients undergoing spinal fusion. 20,29 Numerous studies have also demonstrated the association between operative duration and postoperative complications in orthopedic procedures. 20,22,30,31 However, previous analyses have categorized operative time by durational groups or have identified a threshold duration at which risk of complications are significantly higher. An analysis by Kim et al closely examined the effects of operative duration on postoperative complications in single-level lumbar fusion/instrumentation procedures. 19 Rates of overall, surgical, and medical complications were determined based on categorical operative durations of <2, 2 to 2.99, 3 to 3.99, 4 to 4.99, ≥5 hours. Most postoperative complications exhibited a nonlinear increase in risk across the increasing groups. Risk of organ/space SSI, sepsis, wound dehiscence, and deep vein thrombosis was significantly higher for operations ≥5 hours compared to <2 hours. Risk of overall complications, medical complications, and postoperative transfusions significantly increased in all operative duration groups compared to <2 hours.
Similar to the findings by Kim et al, the current analysis demonstrates a nonlinear increase in risk of complications with each incremental hour in operative time. However, treating operative time as a continuous variable, the current model demonstrates the overall significance of multiplicative increases in risk with increasing duration, as opposed to a threshold effect. For example, the risk of thromboembolism increased significantly with each hour, as indicated by the odds ratio of 1.23 (P < .0001). Compared with the findings by Kim et al, this highlights that the risk of thromboembolism may, in fact, increase across the spectrum of operative duration rather than exhibiting a threshold effect above 5 hours.
There are several limitations inherent to the use of the NSQIP database. First, elements of preoperative characteristics, including prior surgical history, and details of postoperative care are limited. The accuracy of the information that is, indeed, included in NSQIP is restricted by the CPT codes and input from individual institutions. NSQIP also includes complications occurring up to 30 days postoperatively and does not include an important outcome measure in postoperative care of elderly patient, that is, functional status. Of particular importance for our study, NSQIP is used for a variety of surgical procedures and therefore does not capture characteristics specific to spine surgery, such as technique, additional procedures related to implants such as cementation, surgeon experience, open versus minimally invasive procedures, or spine-specific complications such as durotomy, that may affect operative time.
This is the first study to investigate the incremental effects of operative time in elderly lumbar spine patients and holds important clinical implications. While previous studies of operative time have noted various cutoffs in duration that may increase risk of complications, the current study highlights that risk is continuous and multiplicative across the spectrum of operative durations. As the rate of spinal surgeries performed on a growing elderly population continues to expand, the impact of increasing operative time highlights a need for efficient and effective surgical techniques. Interestingly, studies have shown that minimally invasive technique does not confer significantly lower complication rates aside from significantly less blood loss. 32 -34 Therefore, other strategies of optimizing operative time in this cohort of patients is necessary to reduce the risk of other significant complications highlighted in this study. If prolonged operative time in older patients is unavoidable, our results provide a basis for the most pervasive complications that may be avoidable with perioperative interventions.
Conclusion
The current study provides evidence of the strong association between increasing operative time and specific complications in patients age 65 and older undergoing posterior lumbar fusion. This study has built on previous evidence highlighting the most pervasive complications in spinal procedures in the general population and elderly population alike, including blood transfusions, UTIs, SSIs, thromboembolism, and kidney injury. Our results further show that the odds of these complications increase significant with 1-hour increments in operative duration in this patient cohort. Further investigation is necessary to identify specific causality and effective techniques in safely reducing operative time.
Supplemental Material
Supplemental Material, GSJ789117_suppl_mat - Longer Operative Time in Elderly Patients Undergoing Posterior Lumbar Fusion Is Independently Associated With Increased Complication Rate
Supplemental Material, GSJ789117_suppl_mat for Longer Operative Time in Elderly Patients Undergoing Posterior Lumbar Fusion Is Independently Associated With Increased Complication Rate by Alicia E. Hersey, Wesley M. Durand, Adam E. M. Eltorai, J. Mason DePasse, and Alan H. Daniels in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alan H. Daniels received book royalties from LWW and Springer Grants, personal fees from Orthofix, personal fees from Stryker, personal fees from Spineart, and royalties from Springer. All other authors have no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.