
Abstract
Study Design:
Retrospective cohort.
Objectives:
Parkinson’s disease (PD) is a neurodegenerative condition associated with significant morbidity and mortality. PD patients often develop spinal conditions and are known to have high complication rates following surgery. This study evaluated the outcomes of lumbar fusion surgery in patients with PD using a large, public, national database.
Methods:
The Healthcare Cost and Utilization Project (HCUP) Nationwide Inpatient Sample (NIS) was used to identify elective lumbar spinal fusion patients with and without PD for the years 2000 to 2012. PD patients were matched with non-PD controls for comorbidity and age using propensity score matching. Univariable and multivariable logistic regression were used to determine the relationship between PD and surgical outcomes in the matched cohort.
Results:
A total of 231 351 elective lumbar fusion patients were examined, of which 1332 had PD. Before matching, elective lumbar fusion patients with PD were significantly older (P < .001) and more likely male (P < .001) compared with non-PD patients. In the matched cohort, PD was associated with increased length of stay (6.91 vs 5.78 days) (P < .001) and total hospital charges ($129 212.40 vs $110 324.40) (P < .001). There was no significant difference in overall in-hospital complication rate between PD patients and matched non-PD patients (22.3% vs 21.4%) (P = .524).
Conclusions:
Analysis demonstrated significant increases in length and cost of hospitalization for elective lumbar spinal fusion in patients with PD. However, inpatient complication rates in PD patients were not significantly increased. As a growing number of PD patients undergo elective spine surgery, further studies are needed to optimize operative planning. Further study is needed to assess the long-term outcomes of lumbar spinal fusion in PD.
Introduction
Parkinson’s disease (PD) is a progressive neurological disease associated with bradykinesia, tremor, and postural instability. PD is the second most common neurodegenerative disease, affecting 1% of the population older than 65 years. 1 In particular, the postural instability and diminished bone quality in PD present important challenges to the spinal surgeon. 1,2 Furthermore, the increased risk of falls and osteoporotic fracture in this population is an important source of morbidity and mortality, especially following surgery. 1,3,4 While elective lumbar fusion has been used to correct degenerative spinal disease in patients with PD, there may be an increased complication rate, higher rates of revision surgery, and worse functional outcomes in the PD population. 2,5
The purpose of this study was to examine the Nationwide Impatient Sample (NIS) to determine whether patients with PD had inferior in-hospital outcomes after elective lumbar fusion compared to a matched cohort of non-PD control patients. Work from McClelland et al 5 showed an increase in specific complications in patients with PD, including acute respiratory distress syndrome, acute posthemorrhagic anemia, and device-related complications. We hypothesize that in contrary to these findings, overall complication rate is unchanged in PD patients when controlling patient age and comorbidity.
Materials and Methods
The Healthcare Cost and Utilization Project (HCUP) Nationwide Inpatient Sample (NIS) was used to collect US inpatient data from 2000 to 2012. The NIS is the largest publicly available, all-payer database, containing more than 7 million inpatient records annually from 46 participating states. 6 The NIS estimates a 20% stratified sample of national hospital discharges, allowing for results to be generalized to the national population. Lumbar spinal fusion patients were identified using International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9 CM) procedure codes (codes 81.04-81.07). Patients with PD were identified using ICD-9 CM diagnosis codes (332.0). Patients with traumatic spinal injury were excluded. Traumatic injury was identified using Clinical Classifications Software (CCS) multilevel diagnosis groups (16.2.5.1 Fracture of vertebral column without mention of spinal cord injury and 16.3 Spinal cord injury).
Quasi-experimental design was achieved using a propensity score matching procedure as described by Parsons et al 7 to match each PD patient with three non-PD control patients. The propensity score algorithm used a multivariable regression to match patients based on age, sex, Charlson comorbidity index (CCI), and year of admission. The CCI was developed to assess a patient’s risk for perioperative complication based on a validated set of medical comorbidities. 8 Univariable and multivariable logistic regression were used to determine the relationship between PD and surgical outcomes in the matched cohort.
The primary outcome studied was in-hospital complication rate, defined using CCS multilevel diagnosis code 16.10: complications. Additional outcomes measured included mortality rate, length of stay, and total hospital charges. Results were stratified by patient age, sex, CCI, and year of admission. Univariable and multivariable logistic regression were used to determine the relationship between PD and surgical outcomes in the matched cohort, including overall complication rate, in-hospital mortality, length of stay, and total hospital charges. Chi-square test was used to compare demographic means between patients with and without PD in the overall lumbar fusion population and matched cohort. Adjusted odds ratios and 95% confidence intervals were calculated for surgical outcomes. National estimates were calculated using NIS national discharge weights. Statistical analyses were performed using SAS statistical software v.9.4 (SAS Institute, Inc, Cary, NC). Statistical significance was set at P < .05. This study was exempt from institutional review board approval, as all data used was publicly available, and subjects could not be identified, either directly or through identifiers linked to the subjects.
Results
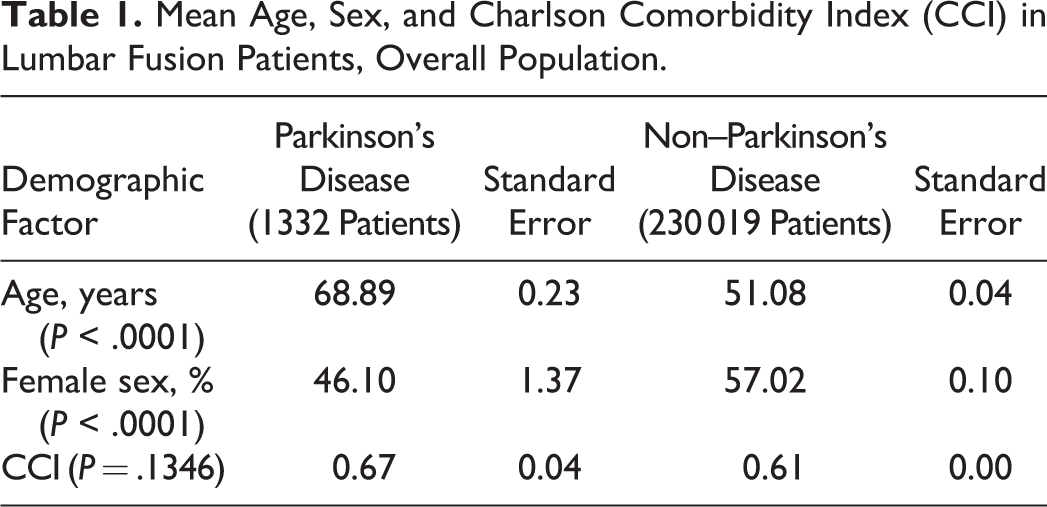
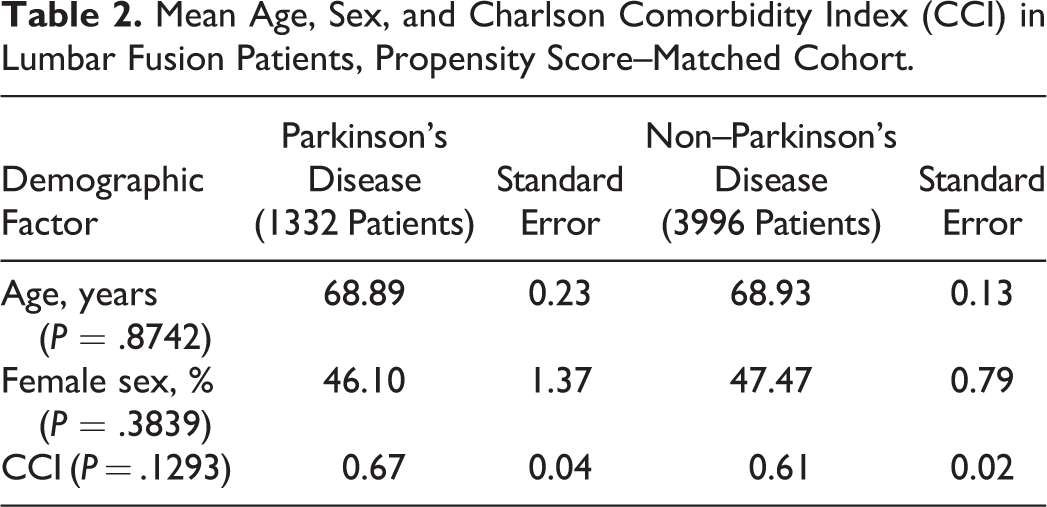
A total of 231 341 elective lumbar fusions were performed between 2000 to 2012 in NIS. Of these patients, an estimated 1332 (0.58%) had comorbid PD. From 2000 to 2012, the percentage of lumbar fusion patients with PD increased from 0.46% in 2000 to 0.74% in 2012 (P < .001), representing a 1.6-fold increase (Figure 1). Before matching, elective lumbar fusion patients with PD were significantly older (68.9 vs 51.1 years old, P < .0001) and more male (53.9% vs 43%, P < .0001), compared with non-PD patients (Table 1). CCI was not significantly different among lumbar fusion patients with PD (0.67 vs 0.61, P = .1346), indicating that PD patients were not significantly more likely to have medical comorbidities. After the propensity score matching procedure was applied, the demographics of lumbar fusion patients with and without PD were no longer different based on age (68.9 vs 68.9, P = .8742), sex (53.9% vs 52.5%, P = .3839), and CCI (0.67 vs 0.61, P = .1293) (Table 2).
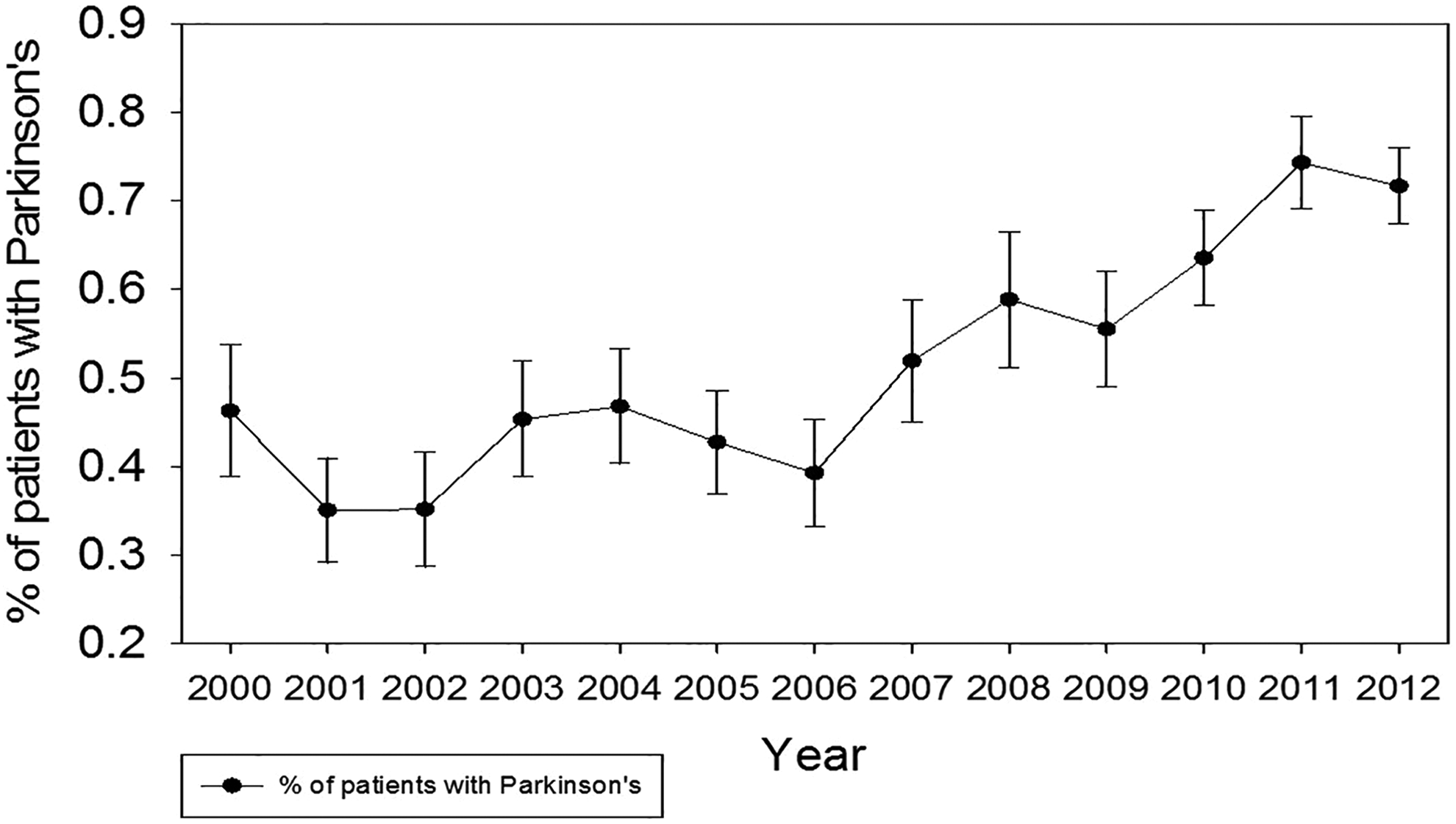
Percentage of elective lumbar fusion patients with Parkinson’s disease, 2000-2012.
Mean Age, Sex, and Charlson Comorbidity Index (CCI) in Lumbar Fusion Patients, Overall Population.
Mean Age, Sex, and Charlson Comorbidity Index (CCI) in Lumbar Fusion Patients, Propensity Score–Matched Cohort.
In the matched cohort, in-hospital complication rate among patients with PD was not significantly increased compared with non-PD control patients (22.3% vs 21.4%, P = .524) (Table 3). After adjusting for age, sex, and comorbidity burden, the odds ratio of complication in patients with PD was 1.05 (95% CI 0.904-1.219). Similarly, in-hospital mortality rate was not increased in patients with PD (6.1% vs 7.2%, P = .39). The odds ratio of mortality in patients with PD was 0.648:1 (95% CI 0.241-1.742).
Outcomes in the Matched Cohort.

Length of stay was significantly longer in patients with PD (6.4 vs 5.2 days, P < .0001). Older age (P = .0094) and increased CCI (P < .0001) were also associated with longer length of stay. Patients with PD averaged total hospital charges of $129 212.40, while matched non-PD patients averaged $110 324.41 (P < .0001).
Discussion
PD has been associated with poor postoperative outcomes in surgical patients. 3,9,10 The literature describing the effect of PD on spine surgery is conflicting. Case series have highlighted rates of complications that ranged from 60% to 80%. 3,9,10 Schroeder et al 1 reviewed 96 cases of PD patients undergoing fusion surgery. They observed a higher rate of complications among PD patients than in the general population. Babat et al 9 described that PD patients more often need revision surgeries due to instability and hardware failure.
In a study similar to ours using the NIS, McClelland et al 10 found that PD was independently associated with higher in-hospital mortality and other individual complications. In contrast to the results of McClelland et al, 10 our analysis of the NIS found no significant increase in overall complication or mortality rate among patients with PD undergoing lumbar fusion. It is possible that, while PD patients may be at increased risk of specific complications, they are not at increased risk of complications overall. Information on both individual and aggregate complications is valuable to spine surgeons; the decision whether to operate on a patient with PD, however, may be better facilitated with gestalt complication risk. With regard to mortality risk, it is possible that selecting different patient demographic variables to develop the matched cohort explains the different findings in adjusted mortality risk among PD patients. MeClelland et al 10 adjusted for age, sex, and race, while the present investigation additionally controls comorbidity in addition to age and sex. The CCI was specifically validated as a metric predicting mortality from administrative data, supporting the hypothesis that its use in this study may have more robustly accounted for potential confounding. 11
In our analysis, from 2000 to 2012, the proportion of lumbar fusion patients with PD increased 1.6-fold from 0.46% in 2000 to 0.74% in 2012 (P < .001). This may be explained in part by an increase in the prevalence of PD, as well as greater comfort with surgery in this population. These effects have resulted in a greater number of PD patients undergoing lumbar fusion, creating a need for better information on the safety and efficacy in this population.
The comorbidities associated with PD are well described. 12 Pneumonia, dementia, and thromboembolic disease are more prevalent in patients with PD. 13 –15 Additionally, sedentary patients can become osteoporotic, which may contribute to poor outcomes following fusion. 3,16 Kaspar et al 17 published a case series that identified aspiration pneumonia—a condition for which PD patients are at increased risk—as a major cause of mortality in the perioperative period. The authors concluded that if steps are taken to avoid such complications, symptoms are improved with surgery given adequate control of the PD itself.
In addition, Bourghli et al 18 reviewed a case series of 12 PD patients who underwent corrective spinal surgery. The authors describe improved balance in both coronal and sagittal planes and noted no loss of correction for the various radiologic parameters between 3 months and the end of the study. In this case series, there were no reported deaths, intraoperative neurological complications, or wound infections. The most common complication was postoperative delirium. Six patients required revision surgery, half due to hardware malfunction. Postoperatively, 11 of 12 patients were satisfied with the outcome. The results of this study suggest that corrective spinal fusion can produce successful outcomes in the PD population.
Using a national database in Japan, Oichi et al 19 compared 1423 patients with PD undergoing spinal fusion to 5498 age-matched controls. They found increased in-hospital mortality, and major complication rate in patients with PD. Similar to Bourghli et al, 18 increased rates of postoperative delirium was noted. However, this analysis did not control for patient comorbidity, while this was achievable using the NIS. This is of particular concern in the PD population, as PD patients have increased comorbidity compared with age- and sex-matched controls.
This study has several potential limitations. First, its retrospective nature makes it difficult to obtain definitive conclusions on the relative risks of lumbar fusion in PD patients. However, the high volume of surgeries accessible through the NIS database allows for a large, validated, and nationally representative population to be described. Given the multicenter nature of this database, our results and their interpretation are reliant on accurate documentation and is subject to data coding errors that may be present in this documentation. Additionally, we were unable to obtain long-term or functional outcome data because of the nature of the NIS itself, limiting the scope of our conclusions. Functional data is of particular interest in PD patients because of the likely difficulties in postsurgical rehabilitation and long-term degenerative nature of PD. While this analysis showed that perioperative outcomes are similar for PD patients, there may be increased risk of adverse outcomes over the long term. Diminished bone quality in PD patients, reduced mobility, and advanced disease are potential contributors to adverse long-term outcomes in PD patients. To date, these results have only been explored in small case series. Further study is needed to quantify the incidence of long-term surgical complication, reoperation, and functional status of PD patients after lumbar fusion.
The data, however, does support the perioperative safety of lumbar fusion in the setting of PD. The data also shows that cost of care and length of stay is greater in PD patients. Interestingly, this increased length of stay cannot be explained by older age or increased overall complication rate. Thus, it is possible that spine surgeons may be more cautious in management of PD patients, or that while complications are not increased, hospital recovery is slower. It is also possible that structural barriers lengthen hospital stay for PD patients, such as including caregivers in discharge planning, arranging safe transportation for patients who cannot drive, or the need for occupational therapy and physical therapy evaluation. While the NIS does not include this data, further study is necessary to determine the cause of increased length of hospitalization in PD patients, as this increases the cost and burden of lumbar fusion in this population.
Conclusions
This study provides the most current information to date regarding the trends and in-hospital outcomes of lumbar fusion in PD patients. We determined that overall complication burden and in-hospital mortality are not increased in PD patients. However, the matched cohort analysis also found increased length of stay and cost of care among PD patients. We also showed that the incidence of lumbar fusion in PD patients has steadily increased since 2000, demonstrating the importance of determining safety in this population. Further study is needed to determine the long-term outcomes of lumbar fusion among PD patients, as well as patient satisfaction and functional status. Based on the data in this study as well as the available body of literature, lumbar fusion may be safe to consider among PD patients in terms of in-hospital risk, though careful patient selection is still recommended given the increased cost of care and rehab difficulty in this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alan H. Daniels is a paid consultant for Stryker, Globus, Depuy, and Orthofix and receives research support from Orthofix.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.