
Abstract
Study Design:
Meta-analysis-based calculation.
Objectives:
Lumbar degenerative spine disease (DSD) is a common cause of disability, yet a reliable measure of its global burden does not exist. We sought to quantify the incidence of lumbar DSD to determine the overall worldwide burden of symptomatic lumbar DSD across World Health Organization regions and World Bank income groups.
Methods:
We used a meta-analysis to create a single proportion of cases of DSD in patients with low back pain (LBP). Using this information in conjunction with LBP incidence rates, we calculated the global incidence of individuals who have DSD and LBP (ie, their DSD has neurosurgical relevance) based on the Global Burden of Disease 2015 database.
Results:
We found that 266 million individuals (3.63%) worldwide have DSD and LBP each year; the highest and lowest estimated incidences were found in Europe (5.7%) and Africa (2.4%), respectively. Based on population sizes, low- and middle-income countries have 4 times as many cases as high-income countries. Thirty-nine million individuals (0.53%) worldwide were found to have spondylolisthesis, 403 million (5.5%) individuals worldwide with symptomatic disc degeneration, and 103 million (1.41%) individuals worldwide with spinal stenosis annually.
Conclusions:
A total of 266 million individuals (3.63%) worldwide were found to have DSD and LBP annually. Significantly, data quality is higher in high-income countries, making overall quantification in low- and middle-income countries less complete. A global effort to address degenerative conditions of the lumbar spine in regions with high demand is important to reduce disability.
Introduction
Degenerative disease of the lumbar spine is a significant cause of disability in the world; it encompasses conditions such as spondylolisthesis, disc degeneration, and lumbar spinal stenosis. Associated with a variety of clinical symptoms, including lower extremity pain, weakness, and low back pain (LBP) of varying levels of severity, lumbar degenerative spine disease (DSD) can lead to a reduction in the quality of life. Demonstrated geographic disparities for DSD 1 may be associated with disparities in socioeconomic status and access to medical care. In the 2010 Global Burden of Disease (GBD) Study, 1 LBP was ranked highest of the 291 conditions studied in terms of years lost to disability, with 83 million disability-adjusted life years lost in 2010. 1
Numerous studies 2 –44 have quantified (incidence or prevalence) DSD; however, the combination of sparse high-quality population-based data, competing disease definitions, and specific population samples, coupled with limited literature resulting from underdiagnosis and underreporting of lumbar DSD in resource-poor settings, have hindered the ability to produce a global estimate. Understanding the burden of lumbar DSD is essential to begin formulating a coordinated, multinational public health effort. In this report, we aggregate data through a systematic review of the literature to generate an approximation of region-specific incidence via a meta-analysis, ultimately culminating in a global estimation of lumbar DSD within the context of LBP.
Methods
Literature Search
A literature search was performed using PubMed and EMBASE in January 2016, following guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 45 The aim of our search was to identify English-language studies with large sample size (both population and hospital based) that reported the epidemiology of DSD within populations having back or neck pain. Including patients with back or neck pain enabled us to focus on neurologically relevant (ie, not strictly age-related) DSD. MeSH and title/abstract keywords were included to maximize the inclusion of any article that related to the volume or the burden (disability-adjusted life years [DALY], years of life lost [YLL], or years lost due to disease [YLD]) of DSD. The full list of search terms can be found in the appendix. Studies without abstracts and those with inappropriate study designs were excluded (Figure 1).
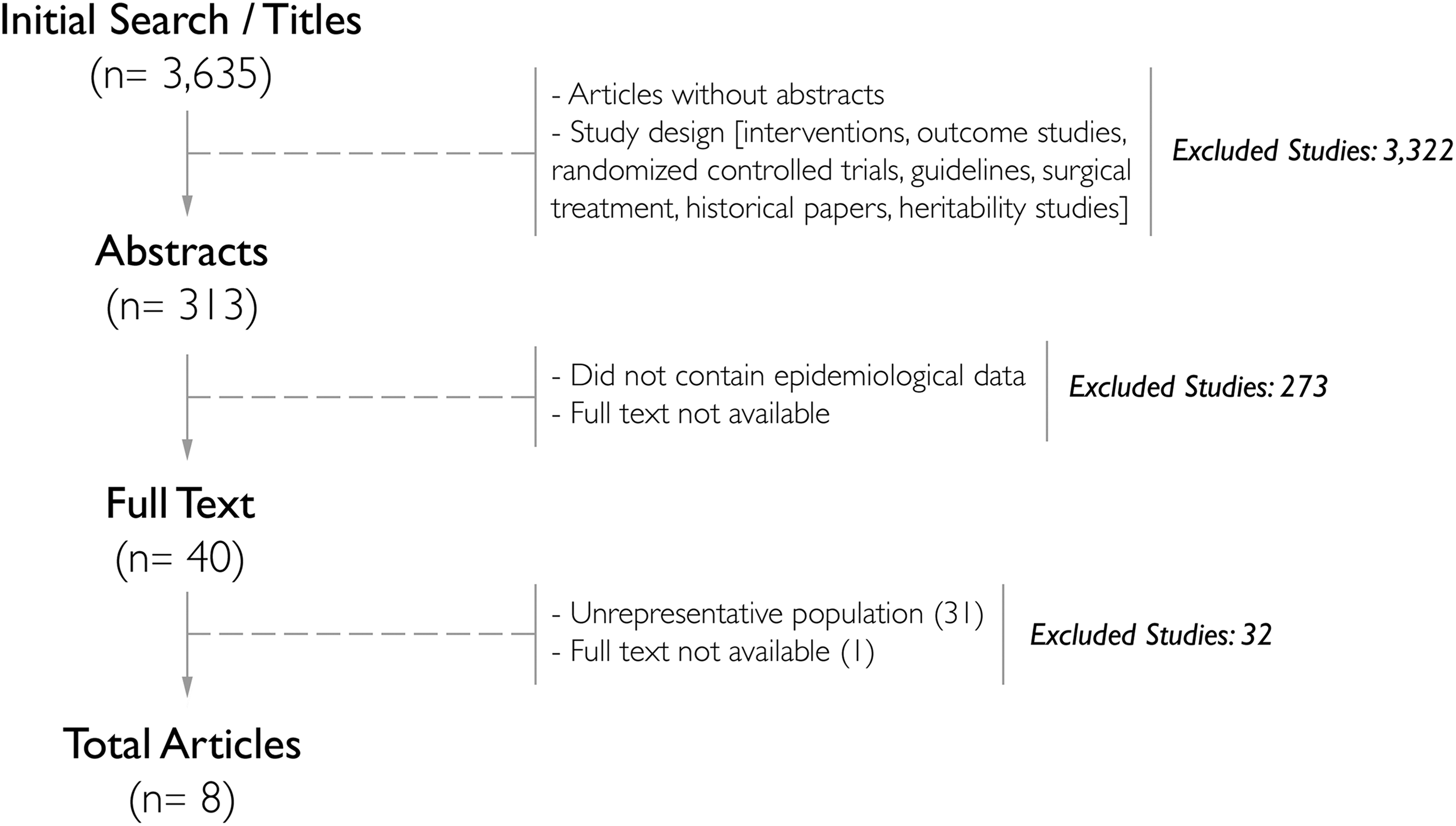
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart: PubMed literature search on degenerative spine disease and back or neck pain.
Two authors (VMR, SSS) screened the titles and abstracts of the resulting articles. Articles that contained epidemiological data and met the DSD pathological inclusion criteria (ie, spondylosis, disc degeneration, disc narrowing, degenerative scoliosis, disc herniation, spondylolisthesis, and spinal stenosis) were included. Pathological criteria were determined prior to article screening; we excluded pathologies relating to aging (eg, osteoporosis), autoimmune disease (eg, rheumatoid arthritis), and congenital disorders (eg, juvenile idiopathic scoliosis). The term degenerative disease has been previously described as ambiguous, 46 which created complications when attempting to define DSD. Our selection criteria aimed to include pathologies that are commonly classified as DSD. 47 Throughout the abstract and full-text review process, reviewers evaluated articles separately. To ensure selection accuracy and to avoid misrepresentation of populations and pathologies, a subset of articles was jointly reviewed as a form of an interrater reliability test. Discrepancies between article inclusion and exclusion were resolved by a third author (AR or MCD).
Full-text papers were acquired, and data extraction was performed. If necessary, additional articles were excluded based on the exclusion criteria noted in Figure 1. Articles were only included if the epidemiological data defined specific lumbar DSD pathologies presenting in subjects with LBP. Articles that presented epidemiological data on just LBP or just lumbar DSD were excluded. Other exclusion criteria are indicated in Figure 1. Data extraction was performed and results were pooled using MedCalc software version 15.1 (MedCalc Software, Ostend, Belgium) to conduct the meta-analysis.
Meta-Analysis and Calculations
To calculate the overall incidence of lumbar DSD within LBP, a model was designed that exploited multiple sources, including literature reviews, the GBD initiative, and the World Bank (WB) population database (https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups). First, data on the incidence (per 100 000) of LBP was obtained from the Institute of Health Metrics and Evaluation (IHME) GBD 2015 database. 48 The database did not account for countries not recognized by the WB and World Health Organization (WHO) regions. Reported data was representative of both sexes and all ages. Incidence values were adjusted based on 2015 WB population metadata and then reported as a proportion, p(LBP).
Next, the epidemiological data obtained from the second systematic review was pooled with random-effects inverse probability weight to estimate the probability of lumbar DSD among those presenting with LBP: p(DSD|LBP). To determine joint proportion of lumbar DSD and LBP, p(DSD∩LBP), the proportion of LBP—p(LBP)—was multiplied by the proportion of lumbar DSD within LBP populations, p(DSD|LBP). The methodology for calculations is presented in Figure 2 with calculations as follows:

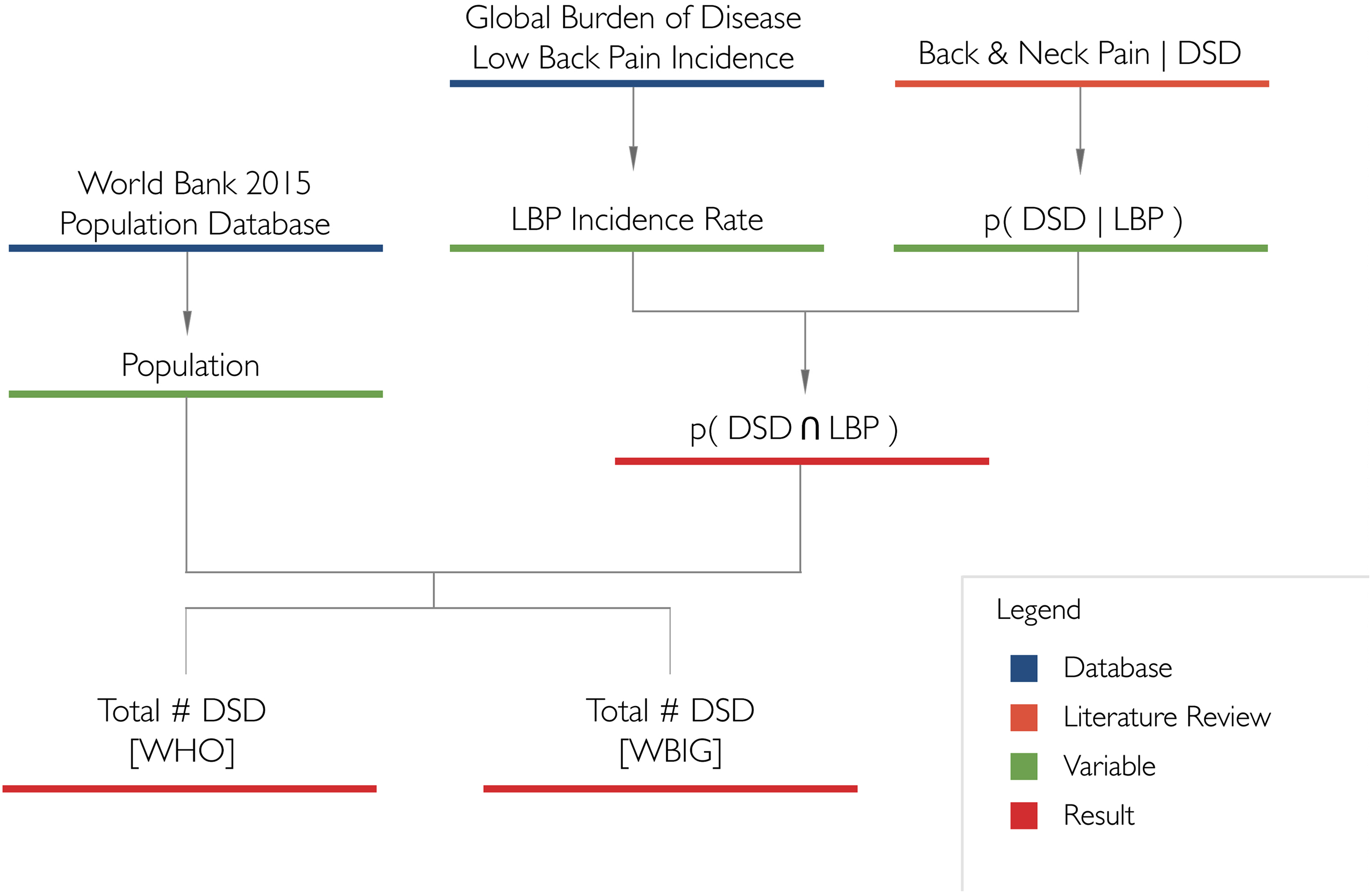
Degenerative spine disease incidence calculations.
The incidence of lumbar DSD and LBP was calculated by multiplying p(DSD∩LBP) by the total population of each country obtained from the 2015 WB population metadata. To deliver a simplified geographic breakdown, total incidence results were organized by country into their respective WHO regions (Figure 3). 49 The Region of Americas was further divided into United States and Canada (AMR-US/Can) and Latin America (AMR-L). Results were also presented by income group (low, middle, high) using categorizations of the World Bank gross national income per capita. To create a global and regional incidence, the number of lumbar DSD and LBP cases for each country in a given region was totaled prior to dividing it by a region’s total population for countries represented by the GBD data. This proportion was then multiplied by more accurate regional population figures. This approach weighed countries with larger populations more heavily, and error propagation was addressed to generate accurate 95% confidence intervals.
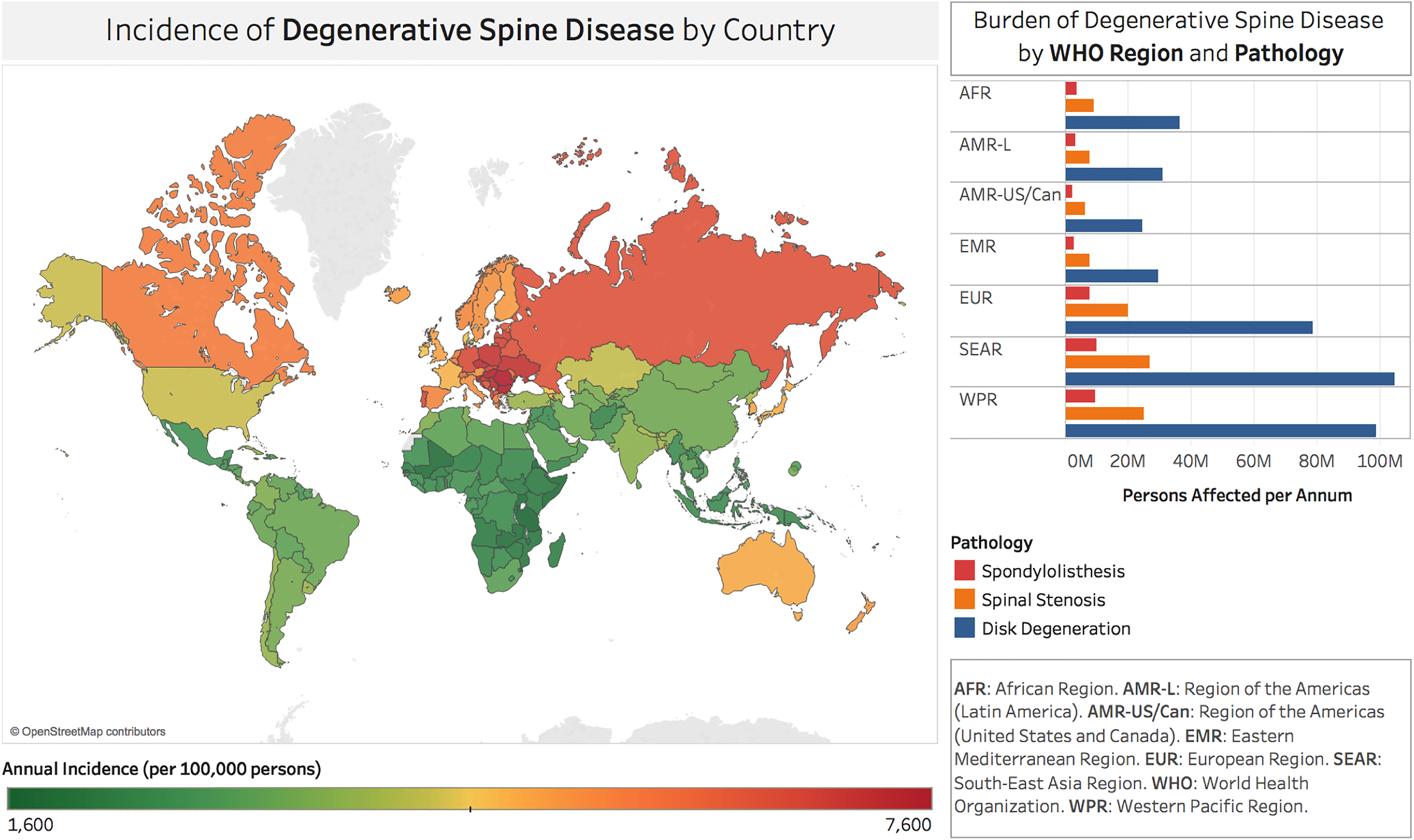
Incidence rates of degenerative spine disease/low back pain in World Bank and World Health Organization recognized countries.
Finally, within the studies analyzed, spondylolisthesis, spinal stenosis, and disc degeneration were the most prevalent lumbar DSD pathologies. Therefore, a proportion was created—p(DX|LBP)—with DX referring to each of the aforementioned pathologies, to obtain their global incidence. Studies used for proportion calculations are presented in Table 1.
Overview of Studies Used to Calculate Proportions.
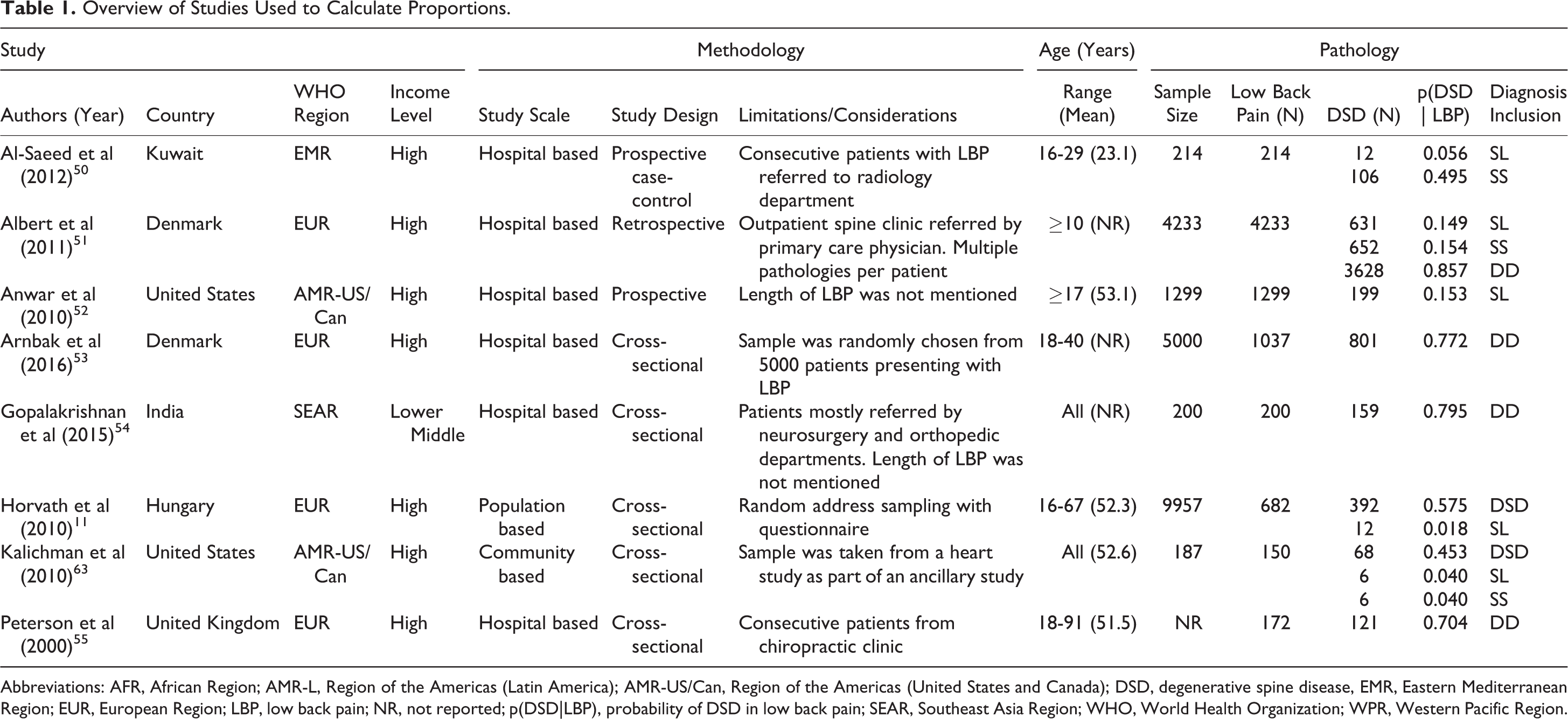
Abbreviations: AFR, African Region; AMR-L, Region of the Americas (Latin America); AMR-US/Can, Region of the Americas (United States and Canada); DSD, degenerative spine disease, EMR, Eastern Mediterranean Region; EUR, European Region; LBP, low back pain; NR, not reported; p(DSD|LBP), probability of DSD in low back pain; SEAR, Southeast Asia Region; WHO, World Health Organization; WPR, Western Pacific Region.
Results
Search Results
The literature search produced 3635 results. After thorough review (Figure 1), 40 articles underwent full-text review. Thirty-one studies were excluded from our systematic review because the study population was unrepresentative. One study was excluded because full text was unavailable and the abstract did not contain enough information to include in our incidence equation. Eight studies 11,50 –55,63 were analyzed to formulate proportions and ultimately estimate the global incidence of lumbar DSD. A majority of these studies were hospital-based (6/8; 75%) 50 –55 and the remaining 2 were population and community based. Most of these studies were derived from high-income countries (HICs) (88%) and most were from the European region (EUR; 4/8, 50%). 11,51,53,55 This was followed by the North American region (AMR US/Can; 2/8, 25%). The last 2 studies were from the Southeast Asia region (SEAR) and the Eastern Mediterranean region (EMR). In studies where the population was defined, the age range was from 10 to 91 years, with 2 studies describing the age as all inclusive. Of the 8 studies in total, 5 were cross-sectional analyses (5/8, 62.5%), 2 were prospective (2/8, 25%), and 1 was retrospective (1/8, 12.5%). An overview of studies used to create the proportions is found in Table 1, which indicates which studies were used in each calculation.
Epidemiological Findings
We found that 266 million individuals (3.63%) worldwide are diagnosed with lumbar DSD yearly; the highest estimated incidence was in Europe (5.7%; 5668 per 100 000) and the lowest estimated incidence was in Africa (2.4%). In total, low- and middle-income countries (LMICs) had nearly 4 times as many cases as HICs of DSD and LBP (Table 2). Thirty-nine million individuals (0.53%) worldwide were found to be diagnosed with spondylolisthesis yearly, with the highest estimated incidence in Europe (0.83%) and lowest in Africa (0.36%). According to the compiled studies, LMICs had nearly 3.5 times the incidence of spondylolisthesis and LBP than HICs (Table 3). This data indicates that nearly 400 million individuals are diagnosed with pathologic disc degeneration worldwide yearly (5.5%); the estimated incidence was highest in Europe (8.6%) and lowest in Africa (3.7%). LMICs had nearly 3.5 times the incidence of disc degeneration and LBP than HICs (Table 2). A total of 102 million individuals (1.4%) were found to be diagnosed with spinal stenosis worldwide yearly, with the highest estimated incidence in Europe (2.2%) and lowest in Africa (0.94%). LMICs had nearly 3.5 times greater incidence of spinal stenosis and LBP than HICs (Table 3). Figure 3 demonstrates a global burden of disease map depicting the incidence of lumbar DSD and LBP, that is, p(DSD∩LBP).
Incidence of Low Back Pain and Degenerative Spine Disease Worldwide by World Bank Income Group and WHO Region.
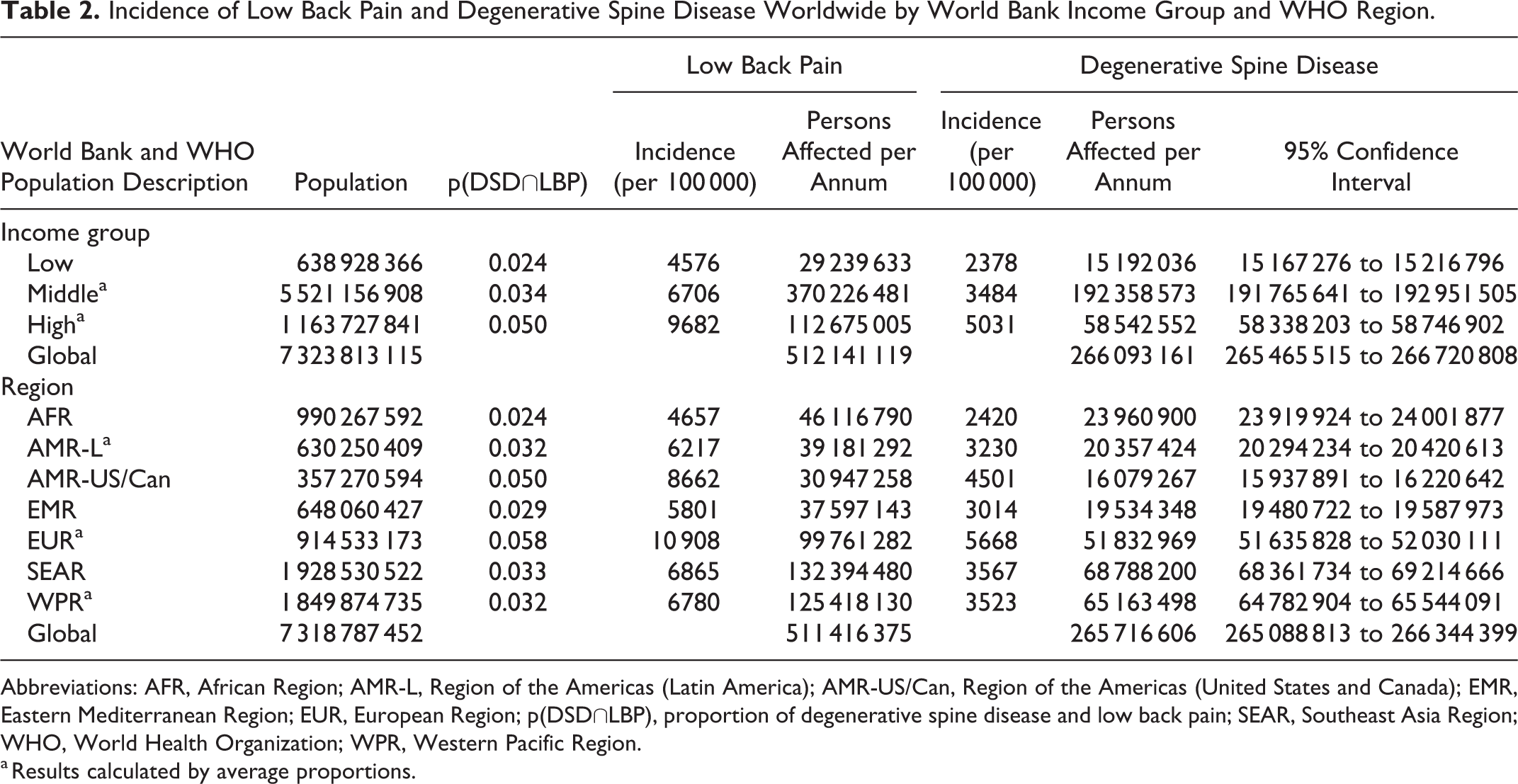
Abbreviations: AFR, African Region; AMR-L, Region of the Americas (Latin America); AMR-US/Can, Region of the Americas (United States and Canada); EMR, Eastern Mediterranean Region; EUR, European Region; p(DSD∩LBP), proportion of degenerative spine disease and low back pain; SEAR, Southeast Asia Region; WHO, World Health Organization; WPR, Western Pacific Region.
a Results calculated by average proportions.
Comparison of Incidence for Total Degenerative Spine Disease and Specific Degenerative Spine Disease Conditions by World Bank Income Group and WHO Region.
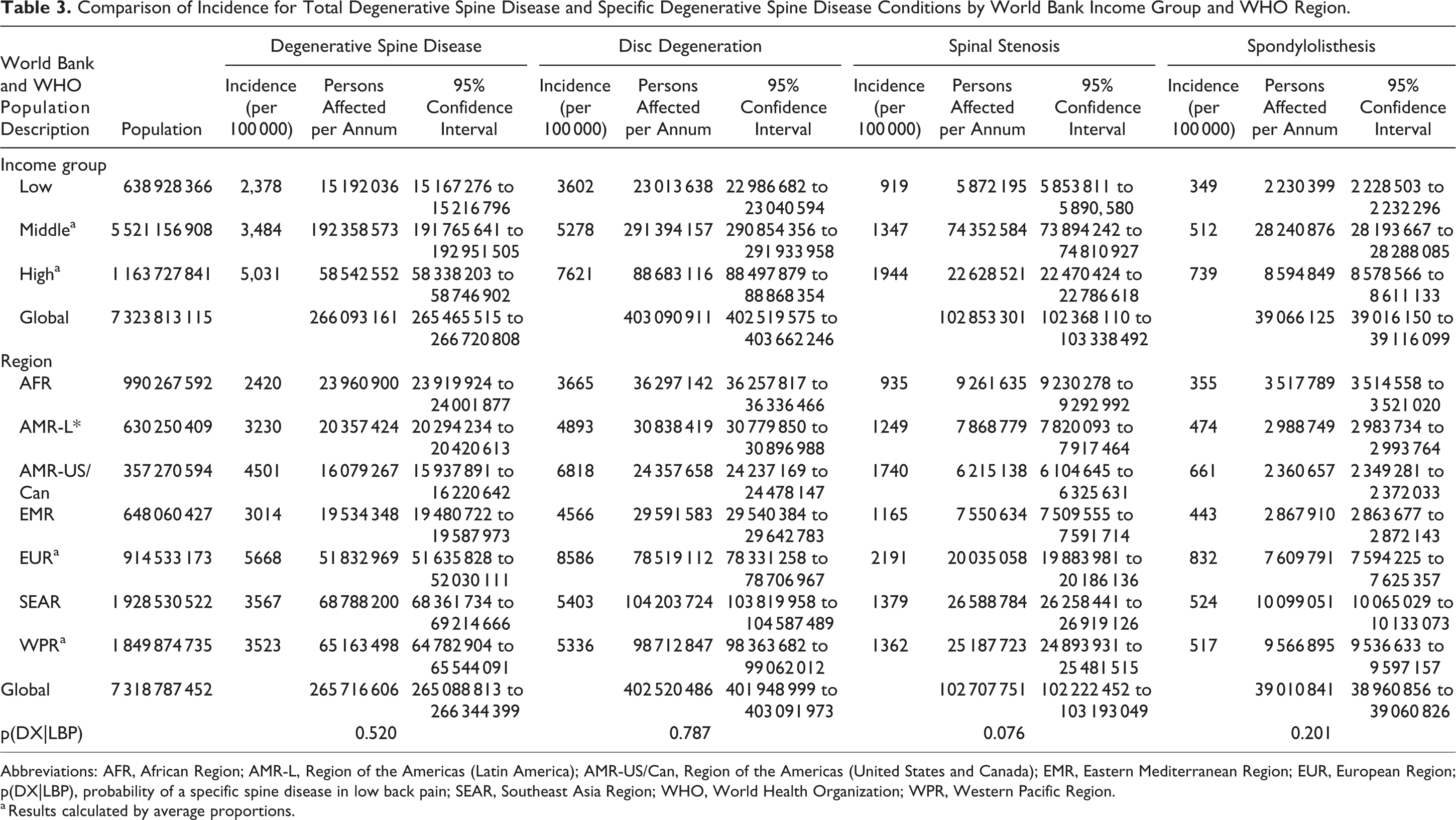
Abbreviations: AFR, African Region; AMR-L, Region of the Americas (Latin America); AMR-US/Can, Region of the Americas (United States and Canada); EMR, Eastern Mediterranean Region; EUR, European Region; p(DX|LBP), probability of a specific spine disease in low back pain; SEAR, Southeast Asia Region; WHO, World Health Organization; WPR, Western Pacific Region.
a Results calculated by average proportions.
Discussion
We have determined, using a global model, an estimate of the incidence of symptomatic adult lumbar DSD with LBP; we estimate that approximately 266 million cases of lumbar DSD and LBP occur worldwide each year. Although the incidence of DSD and LBP was estimated to be highest in Europe and North America, the greatest overall volume of DSD and LBP would be seen in Southeast Asia and the Western Pacific. Interestingly, this finding can be supported through the India-based study, which had the greatest calculated p(DSD|LBP). 54
This estimation is a stepping stone to outlining the global neurosurgical needs. Although surgical pathology is estimated to represent 30% of the global burden of disease, access to surgical care is outside the grasp of much of the global population, specifically those in LMICs. The WHO estimates that nearly 11% to 15% of the world’s disability is caused by surgically treatable disease. 56 In addition, there are nearly 5 billion people who lack access to basic surgical care, 57 a number that is much higher for those in need of neurosurgical care. 58 Neurosurgical diseases have significant impact on society, yet they have been largely ignored on the global stage. 59 The only neurosurgical procedure listed among the 44 essential surgical procedures in the Disease Control Priorities, third edition (Volume 1: Essential Surgery) is burr hole evacuation of subdural hematoma. 60 Access to neurosurgical care is limited by access to providers and cost-effective technology. 58 In an effort to address global neurosurgical needs, we must first attempt to characterize their global volume and epidemiology. It should be noted that primary and even secondary treatment of LBP, and the associated pathologies discussed, is nonoperative management, which may be lacking in LMICs. In these settings, especially, surgery is used for very select patients.
The estimates provided here are higher than those generated in previous efforts to quantify the volume of DSD worldwide. After carefully examining the results of an initial systematic review that included all reports of DSD, not just those associated with LBP, we formed a consensus that the data did not provide an accurate representation of the true volume of DSD. Although numerous studies were population based, many focused strictly on the aging population (65+ years old) and/or were of a small sample size. Also, a majority of the studies were from HICs (86%) and received a poor-quality rating. Because of these shortcomings in the collected studies, we modified our strategy and performed a second systematic review that reflects the current methodology. This method relied on incidence figures calculated from the IHME database, since reliable, population-based incidence figures for DSD in the majority of LMICs were unavailable in the literature. This provides greater confidence in the quality of the numbers from LMICs. The European incidence (5668 per 100 000) represents the highest volume of lumbar DSD. An important consideration is the presence of symptomatic DSD; however, a much larger percentage of the population has lumbar DSD, which may be clinically silent. The higher reported European incidence is also likely to be a product of large registries across European nations with high-level epidemiological data compared with the data available in LMICs. Similarly, the lower incidence in Africa is likely explained in part by lower quality data and lower access to diagnostic and treatment options for lumbar DSD from these area countries. An advantage to the methodology in this study is that the use of LBP as the denominator allows for assessment of symptomatic cases of DSD.
Since DSD is a broad term in the context of LBP, we chose to characterize spondylolisthesis (a common disease of the lumbar spine), disc degeneration, and spinal stenosis as subcategories to further delineate the types of pathology and the potential implications on surgical intervention. The estimated incidence of patients with spondylolisthesis in the setting of LBP was highest in Europe (832 per 100 000), with an estimated overall incidence worldwide of 0.20% (Table 3). Degenerative spondylolisthesis typically occurs in the setting of severe arthritis of the facet joints and intervertebral disk herniation. The use of spondylolisthesis in determining incidence of lumbar DSD may be limited by the potential inclusion of patients who have isthmic spondylolisthesis, which is not a degenerative condition, but is an osseous discontinuity of the vertebral arch at the isthmus—the pars interarticularis—and may occur in young adults, typically athletes, as a consequence of bilateral pars interarticularis stress fractures. 61,62
The finding that the incidence of disc degeneration (0.787) exceeds the overall incidence of lumbar DSD (0.520), at first glance, appears to be a contradiction but reflects the methodology of the review. The lumbar DSD papers reviewed 11,63 did not include disc degeneration as a subcategory. The varying inclusion and correspondence of subpathologies yielded varying proportions, thus contributing to the greater volume of disc degeneration compared with lumbar DSD. One could use disc degeneration as the denominator for this study; however, we decided that using LBP is a more methodologically sound method in further evaluating spondylolisthesis and spinal stenosis because these patients often present with back pain and may or may not have evidence of disc degeneration on imaging. It is worth noting that many cases of lumbar spine disease are often associated with lower extremity pain rather than low back pain; however, even fewer studies exist with proven findings of degeneration for the lower extremities. Thus, the decision was made to use LBP as the denominator.
The highest estimated incidence of spinal stenosis was seen in Europe (2191 per 100 000) with the lowest in Africa (935 per 100 000). Symptomatic degenerative lumbar spinal stenosis with clinical neurogenic claudication is a frequent source for spinal surgery consultation, which most commonly occurs beyond the fifth decade of life. It has been postulated that more than 2.4 million people in the United States alone will be affected by symptomatic lumbar spinal stenosis by the year 2021. 64
Our goal in undertaking this meta-analysis was to generate preliminary data to prompt further study into the epidemiology of degenerative lumbar spine disease with LBP as it might apply to surgical intervention (eg, surgeon availability, access to advanced care). Similarly, additional studies should be undertaken to examine the burden of cervical degenerative disease, degenerative scoliosis, spinal cord injury, spinal infection, and rheumatological diseases that affect the spine to obtain a more complete picture of the global burden of these diseases. The tremendous amount of data found within the literature cannot possibly be summarized in a single study, but the results are necessary if we are to begin to plan a global public health effort.
Limitations
Although this was a comprehensive, systematic review of the literature, there are shortcomings based on the quality of the evidence available for review. The literature reviews and meta-analyses conducted to obtain DSD and LBP relative ratios rely on studies with heterogeneous and often biased study designs. A topic this general inherently is reported in populations that are nonuniform, making direct comparisons challenging. Combining epidemiologic data across heterogeneous cohorts risks misrepresentation of disease volume.
As demonstrated by the methodology, there is a paucity of epidemiological information from LMICs, thus likely under-representing these areas in the overall volume of DSD and LBP. In addition, a large amount of the literature is focused on elderly, aging populations—this likely stems from the notion that degeneration implies an age relation, which is a misnomer that is highly prevalent in the literature.
An additional consideration is that the nomenclature used in the literature limited the number and quality of the studies analyzed. DSD can include loss of disc height, traction spurs, and annular osteophytes. 51 There are many publications with the term degenerative disc disease in the title, but this term does not have an explicit definition. 46 Degenerative disease of the spine (spondylosis) is defined as the finding of decreased disc height and fragmentation on magnetic resonance imaging. 51 Additionally, radiological diagnostics differed between studies. Although interrater reliability testing and specific protocols were used for diagnostic validity, the variability in imaging modality across studies may produce limitations. The differing, and arbitrary, use of terms may preclude adequate comparison with other studies in a review such as this. Stricter definitions could be used to improve global estimates of disease in the future.
Although the methodology used within this model has limitations, it has been previously used in similar studies to estimate national and global incidence rates of head injury, femoral fractures, and traumatic brain injury. 65 –67 Furthermore, its use can be justified through the use of sound scientific estimation because it is necessary to produce data for countries where research is limited, unreliable, or entirely unavailable. Our goal to estimate the volume of DSD on a global scale has been achieved—albeit with the aforementioned considerations. We estimated the volume of DSD with regional and income-level information. An important factor to the epidemiology and reporting of DSD in the setting of LBP may be from cultural bias and reporting. Back pain in western cultures is more prevalent because pain thresholds seem to be lower. 68 Secondary gain, which is more prevalent in HIC and Western culture, may also play a role; these 2 factors may affect reporting, and this represents a limitation of the study.
The results of our data must be considered within the context of the study. First, incidence values for LBP were obtained through the GBD data, which are modelled estimates. Also, only symptomatic cases were taken into account; DSD does not always present with LBP. For this reason, our results could be viewed as a minimum approximation. The studies that were used to calculate proportions may also present limitations, despite being the highest quality available within our search. First, studies used in our meta-analysis were weighted heavily on hospital-based studies, which was necessary in creating proportions. Second, our review excluded non-English literature, which may have provided more data from LMIC regions where literature was scarce and given a more accurate picture. Therefore, these estimates of DSD should be cautiously applied to the general global population. By nature of the available data from the literature, we assumed uniform disease susceptibility across age groups and sexes. We also assumed member countries of a particular WHO region or WB income group share the same injury incidence.
Ideally, to overcome the limitations presented in this study and increase the accuracy of a global estimation, a series of large, population-based studies will need to be performed and represent every type of population worldwide. It is important to acknowledge the value of these studies and the data they would produce, despite the vast cost and limited feasibility of such a project. Future studies would also benefit from an expert panel defining the criteria for spinal degeneration. Nevertheless, we believe that these estimations serve as a starting point in determining the global volume of spinal disease as it relates to neurosurgical awareness.
Conclusions
In our global model, the annual incidence of adult DSD is roughly estimated at 266 million individuals. Per capita, the highest annual incidence of DSD and back pain is estimated in Europe and North America (5668 and 4501 per 100 000 people, respectively); however, taking into account regional populations, the greatest volume of DSD is in Southeast Asia (69 million) and the Western Pacific (65 million). Thus, the health care systems in LMICs would encounter nearly 4 times as much total DSD as those in HICs. These estimates are limited by relatively low-quality data from LMICs and suggest the need for more robust and accurate reporting with uniform use of terminology. Uniform definitions of degenerative spine conditions requiring surgical intervention (such as ICD9 or ICD10 codes) will improve the efforts to characterize the global burden of disease and its impact on quality of life. A global effort to address degenerative conditions of the spine in regions with the greatest demand is imperative to decrease overall disparity and to decrease disease incidence and morbidity.
Footnotes
Appendix
Acknowledgments
The authors would like to thank Kristin Kraus, MSc, for editorial assistance in preparing this article and Ron Baticulon, MD for assistance in figure preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Vanderbilt Medical Scholars Program provided Abbas Rattani with support on this project. The other authors received no financial support for the research, authorship, and/or publication for this article.