
Abstract
Study Design:
Systematic review.
Objectives:
To review the current literature on the treatment efficacy, clinical utility, and cost-effectiveness of multidisciplinary biopsychosocial rehabilitation (MBR) for patients suffering from persistent (nonspecific) lower back pain (LBP) in relation to pain intensity, disability, health-related quality of life, and work ability/sick leave.
Methods:
We carried out a systematic search of Web of Science, Cochrane Library, PubMed Central, EMBASE, and PsycINFO for English- and German-language literature published between January 2010 and July 2017. Study selection consisted of exclusion and inclusion phases. After screening for duplication, studies were excluded on the basis of criteria covering study design, number of participants, language of publication, and provision of information about the intervention. All the remaining articles dealing with the efficacy, utility, or cost-effectiveness of intensive (more than 25 hours per week) MBR encompassing at least 3 health domains and cognitive behavioral therapy–based psychological education were included.
Results:
The search retrieved 1199 publications of which 1116 were duplicates or met the exclusion criteria. Seventy of the remaining 83 articles did not meet the inclusion criteria; thus 13 studies were reviewed. All studies reporting changes in pain intensity or disability over 12 months after MBR reported moderate effect sizes and/or p-values for both outcomes. The effects on health-related quality of life were mixed, but MBR substantially reduced costs. Overall MBR produced an enduring improvement in work ability despite controversy and variable results.
Conclusions:
MBR is an effective treatment for nonspecific LBP, but there is room for improvement in cost-effectiveness and impact on sick leave, where the evidence was less compelling.
Keywords
Introduction
Nonspecific lower back pain (NSLBP), and in particular persistent (ie, of at least 12 weeks’ duration 1 ), NSLBP without structural origin, results in a considerable global socioeconomic burden 2 and disability. 3 Although NSLBP is very common, with lifetime and point prevalences of up to 84% and 40%, respectively, 4,5 the literature does not differentiate consistently between LBP and NSLBP, or persistent LBP and persistent NSLBP, forcing us to consider both terms in this article. LBP 6 reduces quality of life and work performance 6 and the proportion of people affected is projected to increase as society ages, 7 thus the condition is a real cause of concern and requires new and innovative management strategies. 8 The personal and societal costs of managing LBP are high, below only cardiovascular disease and diabetes in the United States 9 and although treatment uptake and the range of treatments available have increased dramatically, 9,10 treatment results are less convincing, leading to enormous economic and health care costs every year. 3,11 All parties with an interest in the management of LBP or NSLBP—patients, health care providers, and health care systems—need better knowledge about the efficacy, clinical utility, and cost-effectiveness of current treatments.
Efficacy, Clinical Utility, and Cost Effectiveness of Treatments for Persistent LBP or Persistent NSLBP
Several factors determine the quality of an intervention. A medical treatment is considered effective if there is evidence that it eliminates or reduces a given health problem. 12 If a treatment is feasible, useful and can be applied in a range of settings it is considered to have clinical utility. 12 A treatment is cost-effective if it provides the best treatment alternative in economic terms. 13 In German-speaking countries, health insurers will cover the costs of a medical treatment if it has proven treatment efficacy, clinical utility, and cost-effectiveness 14 ; this is not true of all first-world countries. Health care insurers in the United States, for example, are permitted to focus on cost-containment and profitability and, therefore, will not reimburse patients for services or drugs. 15
In recent years, only a few articles have reviewed the efficacy, clinical utility and cost-effectiveness of treatments for persistent LBP or persistent NSLBP. 16 –22 This article reviews recent evidence, covering the period up to July 2017.
Multidimensionality of Persistent LBP or Persistent NSLBP
Persistent LBP or persistent NSLBP represents a complex interaction of physical, psychological, social and environmental components, including both genetic and cultural factors. 23,24 Potential treatments should take this into account and encompass a representative range of medical disciplines and disciplines allied to medicine, combined so as to offer maximum benefit to patients. In their Cochrane systematic review, Kamper et al 19 confirmed the efficacy of multidisciplinary biopsychosocial rehabilitation (MBR) but were not completely able to proof its cost-effectiveness. 19
Definition of Inter- or Multidisciplinary Treatment
MBR is based on Engel’s 1977 biopsychosocial (BPS) model, according to which biological, psychological, and social factors influence the course of a disease. 25 To date, however, there is no consensus on terminology for describing such treatments. In their latest Cochrane review Kamper et al 19 describe MBR as an integrated intervention that involves at least 2 of the following: physical, psychological, social, and work-related factors. They also note that the therapeutic team should comprise a minimum of 2 different health care professionals, for example, a medical doctor (physician or psychiatrist) and a clinical psychologist or physical therapist, who communicate extensively about the management of patients. Additional team members, such as an occupational therapist, exercise therapist, or social worker, can be integrated when necessary. 19 Gatchel et al 24 differentiate between multidisciplinary interventions, involving several health care professions and interdisciplinary interventions in which the team has a common understanding of rehabilitation and is in constant communication, and the patient is actively involved in treatment planning. Although there is no universally accepted definition of MBR, the primary aim of MBR appears to be reduction of pain-maintaining factors. 19,24,26,27 For the purposes of this review, we have used Kamper et al’s definition and required MBR to involve weekly meetings of the therapeutic team at which individuals’ treatment is discussed. 24 Furthermore, we followed the recommendation of Guzman et al 17 to employ MBRs with a high treatment intensity of at least 25 hours per week. MBR also typically involves cognitive behavioral therapy (CBT) to help the individual identify and replace maladaptive thoughts, emotions and behaviors. 24 Thus CBT is often integrated into MBR, generally in the form of group therapy as this is considered to represent the most cost-effective use of resources. 1,28 Using this definition, we reviewed the literature between 2010 and 2017 in order to identify studies reporting on CBT-based MBR interventions of any design, provided they comprised at least 25 hours of treatment per week and involved at least 3 health professions. We examined the efficacy, clinical utility, and cost-effectiveness of these MBR interventions as treatments for persistent LBP or persistent NSLBP.
Material and Methods
Data Sources
An electronic and manual search of the English- and German-language literature was performed. The electronic search covered November 2016 to July 2017 in the databases Web of Science, Cochrane Library, PubMed Central, EMBASE and PsycINFO (January 2010 to July 2017). The search string entered was (efficacy OR effectiveness OR efficiency OR therapeutic effects OR utility OR cost effectiveness) AND (multidisciplinary treatment OR interdisciplinary treatment OR multidisciplinary rehabilitation OR functional restoration OR cognitive-behavioral pain management program OR functional centered rehabilitation) AND (low back pain OR non-specific low back pain OR persistent low back pain OR persistent non-specific low back pain). This search was supplemented with a manual check of references in articles included in recent reviews and work by authors known to publish in this area. The cutoff date for the retrieval of articles from libraries was July 31, 2017. The selected studies were compiled into an electronic list that formed the basis of the second step in the selection process, which is described below.
Literature Screening
Studies were selected through a systematic 2-step screening process. In spring 2017, the first rater (SS, junior psychologist, conversational bilingual German and English expertise) screened all titles, authors, and abstracts, and removed duplicates. Next the articles were reviewed by 2 independent raters (SS; CRS, senior psychologist, advanced bilingual German and English expertise) in order to exclude publications that were abstract only, case reports, letters, comments, or reviews; studies based on fewer than 15 patients (due to reduced generalizability of results); publications in languages other than English or German; publications where there was insufficient information to determine whether the intervention met our criteria for MBR. The full texts of all remaining articles were obtained in digital format. In the third phase, both raters (SS and CRS) selected all articles that examined the efficacy, clinical utility, or cost-effectiveness of MBR, where the MBR consisted of more than 25 hours of treatment per week delivered by at least 3 different health professions as well as CBT-based psychological education.
Study Selection for Data Extraction
At least one out of several outcomes should be reported in the selected studies 29 : pain intensity (eg, visual analogue scale, VAS 30 ; Numeric rating Scale, NRS 31 ), disability (eg, Oswestry Disability Index, ODI 32 ; Roland Morris Disability Questionnaire, RMDQ 33 ), health-related quality of life (HRQoL; eg, Short Form–36, SF-36 35 ), and work ability/sick leave (eg, length of absence from work). We also extracted the following study characteristics and demographic variables: study location, and outcomes; treatment duration; specific information about the treatment; nature of the control and treatment groups; the disciplined incorporated into treatment; measurement times; sample size; gender distribution and mean age of sample. 29
To ensure a transparent and complete reporting of the review, this study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. 35,36 Furthermore, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was chosen to rate the quality of evidence. 37 GRADE was developed by a widely representative group of international guideline developers with the aim to clearly separate between the quality of evidence and the strengths of recommendations. Explicit, simple, transparent, and comprehensive criteria for down- or upgrading quality-of-evidence ratings are described for the study design, study limitations, inconsistency of results, indirectness of evidence, imprecision, and publication bias of a publication—finally offering 4 quality-of-evidence classifications (high, moderate, low, and very low). 37
Statistics
Where available, effect sizes (ESs) and P values are reported. An ES is a quantitative measure of the strength of an outcome. It represents the difference between pre- and postmeasurements divided by a pooled standard deviation. ESs can be categorized as follows: ES ≥0.20 = small effect, ES ≥0.50 = moderate effect and ES ≥0.80 = large effect. 38 P value has been defined as “[…] the probability under a specified statistical model that a statistical summary of the data (e.g., the sample mean difference between two compared groups) would be equal to or more extreme than its observed value.” 39(p131) Although P values indicate the level of compatibility with a specified statistical model (null hypothesis, H0), they must be understood as a statement about data in relation to a specified hypothesis. A P value is a measure of statistical significance, but it does not indicate the size of an effect or the clinical importance of a result. 39(p132) In this study, the smaller the P value, the greater the statistical incompatibility of the data with H0 (pre- and posttreatment measurements are similar).
Results
Data Retrieval
The initial literature review identified 1199 publications of which 1116 were rejected as duplicates (n = 784) or because they met exclusion criteria (n = 332). Seventy of the remaining 83 articles did not meet the inclusion criteria, leaving a sample of 13 primary studies for review (Figure 1). 40 –54 Twelve studies examined the efficacy of MBR, 3 investigated cost-effectiveness, and 1 examined clinical utility. Three of the 13 studies examined 2 or more of these variables.
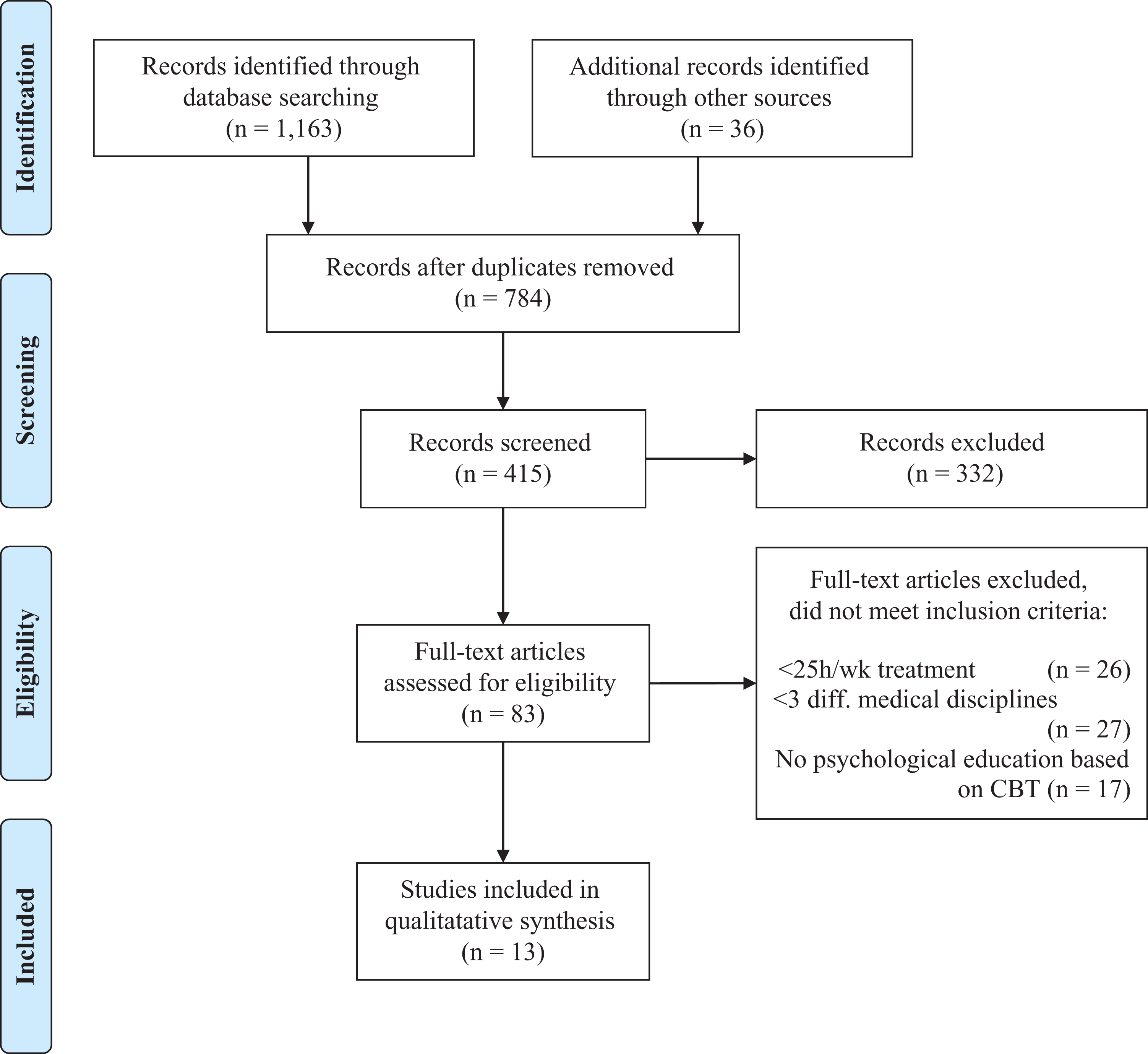
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) 2009 flow diagram.
Study Characteristics
All 13 extracted studies were longitudinal studies conducted in Europe; they comprised 4 randomized controlled trials, 6 prospective studies, 2 cost analyses, and 1 retrospective study (Table 1). The number of hours of therapy per week ranged from 25 to 50 and the total for the intervention from 97.5 to 150. According to the GRADE 37 criteria, 1 study provided high-quality evidence and 1 moderate-quality evidence, but the rest had limitations (Table 2).
Characteristics of Extracted Original Studies.
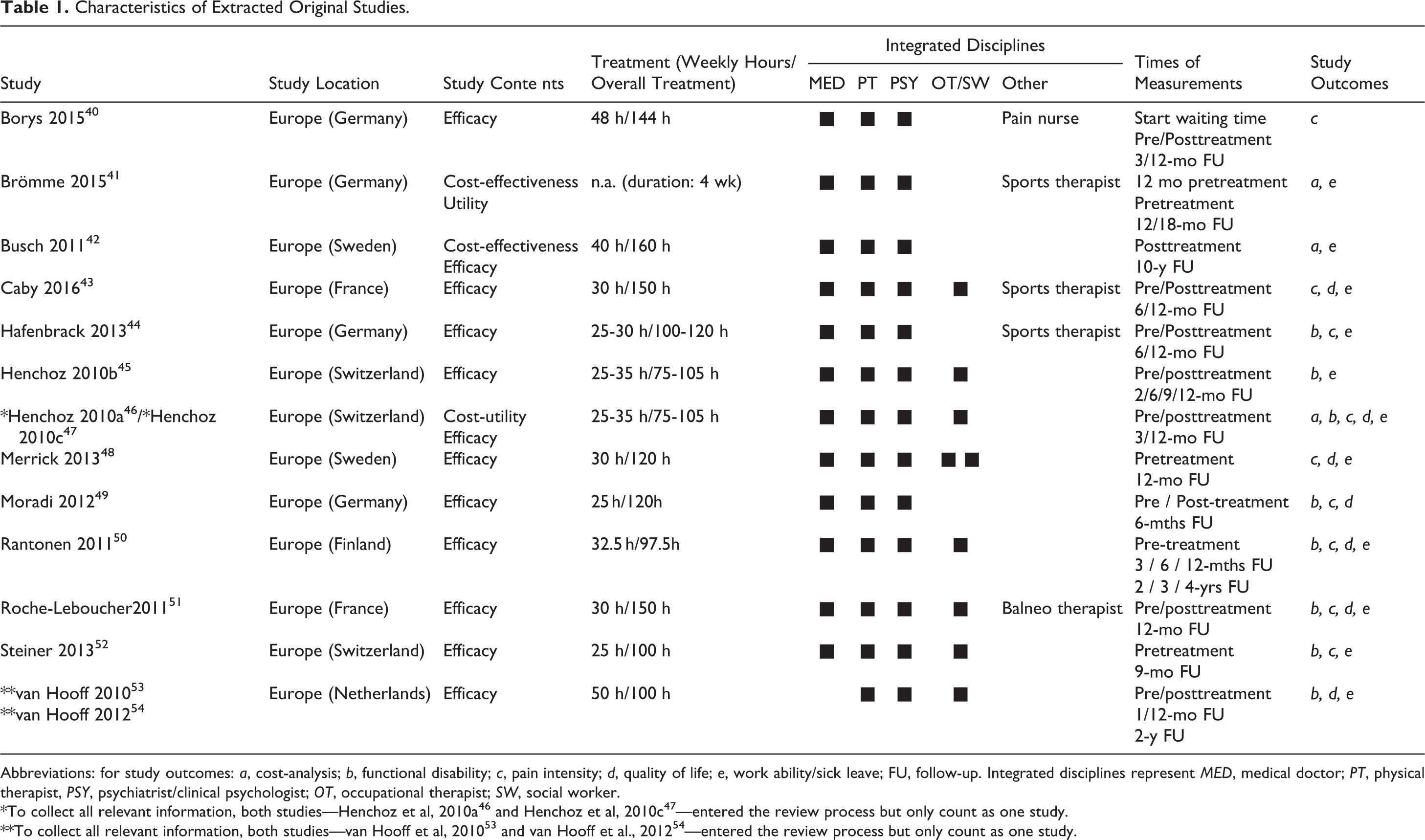
Abbreviations: for study outcomes: a, cost-analysis; b, functional disability; c, pain intensity; d, quality of life; e, work ability/sick leave; FU, follow-up. Integrated disciplines represent MED, medical doctor; PT, physical therapist, PSY, psychiatrist/clinical psychologist; OT, occupational therapist; SW, social worker.
Evidence Profile for the Extracted Studies (GRADE Approach).
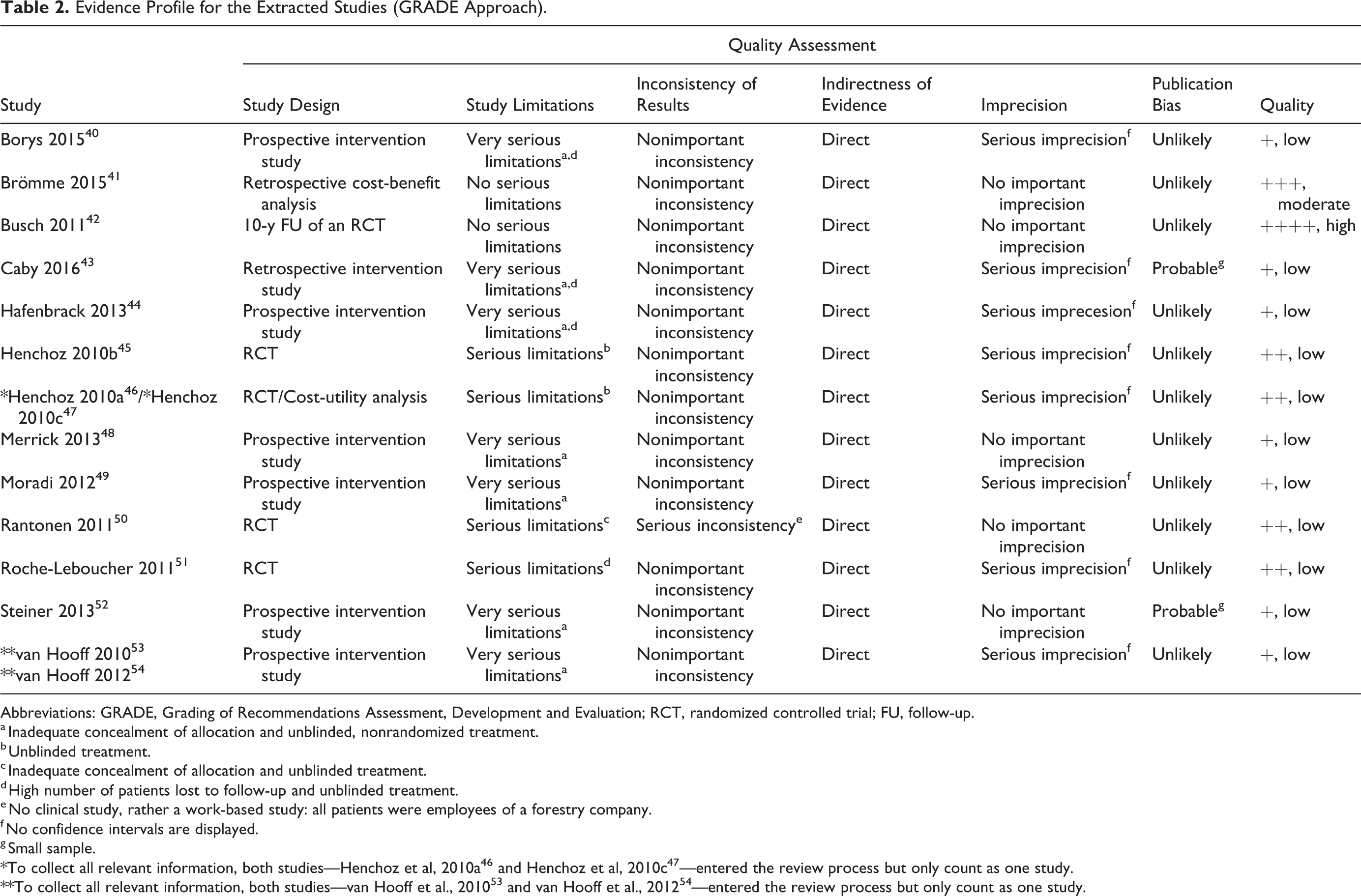
Abbreviations: GRADE, Grading of Recommendations Assessment, Development and Evaluation; RCT, randomized controlled trial; FU, follow-up.
a Inadequate concealment of allocation and unblinded, nonrandomized treatment.
b Unblinded treatment.
c Inadequate concealment of allocation and unblinded treatment.
d High number of patients lost to follow-up and unblinded treatment.
e No clinical study, rather a work-based study: all patients were employees of a forestry company.
f No confidence intervals are displayed.
g Small sample.
Characteristics of Participants
There were 2002 patients enrolled in MBRs and 947 subjects in various control groups. Approximately 49% of all enrolled patients were female and the overall average age of patients was 43 years. All studies but one included participants with persistent NSLBP lasting at least 3 months. The exception was Rantonen et al, 50 who included participants with acute or recurrent LBP employed by a forestry company and unsurprisingly, the histories of this patient group are clearly different from the other, more typical histories of participants on sick leave due to persistent LBP or persistent NSLBP (Table 3).
Characteristics of Study Participants.
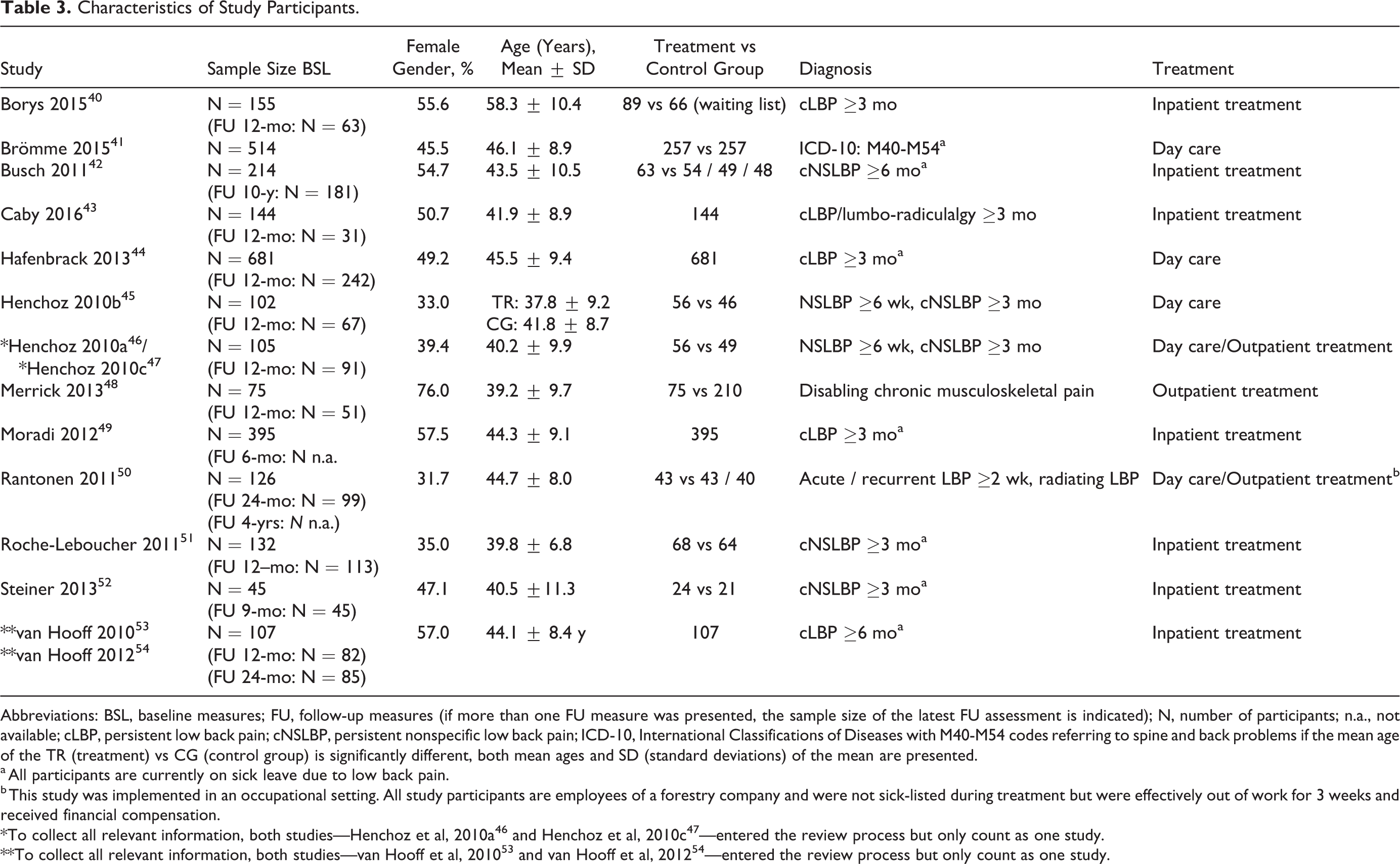
Abbreviations: BSL, baseline measures; FU, follow-up measures (if more than one FU measure was presented, the sample size of the latest FU assessment is indicated); N, number of participants; n.a., not available; cLBP, persistent low back pain; cNSLBP, persistent nonspecific low back pain; ICD-10, International Classifications of Diseases with M40-M54 codes referring to spine and back problems if the mean age of the TR (treatment) vs CG (control group) is significantly different, both mean ages and SD (standard deviations) of the mean are presented.
a All participants are currently on sick leave due to low back pain.
b This study was implemented in an occupational setting. All study participants are employees of a forestry company and were not sick-listed during treatment but were effectively out of work for 3 weeks and received financial compensation.
Outcome Measures
There were some differences between the outcome variables used in the studies included in this review; however, 11 of the 13 studies reported data on work ability and sick leave. Several studies investigated disability and HRQoL using various tools (Table 1) in addition to pain intensity. The following sections provide an overview of the various outcome measures.
Pain Intensity
Eight studies examined changes in pain intensity over the 12 months following MBR; most used similar tools (VAS 30 or NRS 31 ). Comparisons of pre- and posttreatment scores revealed moderate to large ESs or P values in pain reduction (ES −0.6 to −0.74; P = .003 to P < .001). In studies that assessed patients over a longer period, the reduction in pain intensity persisted for at least 24 months (P < .01; Table 4).
Summary of Findings Regarding Pain Intensity, Disability, and Quality of Life.
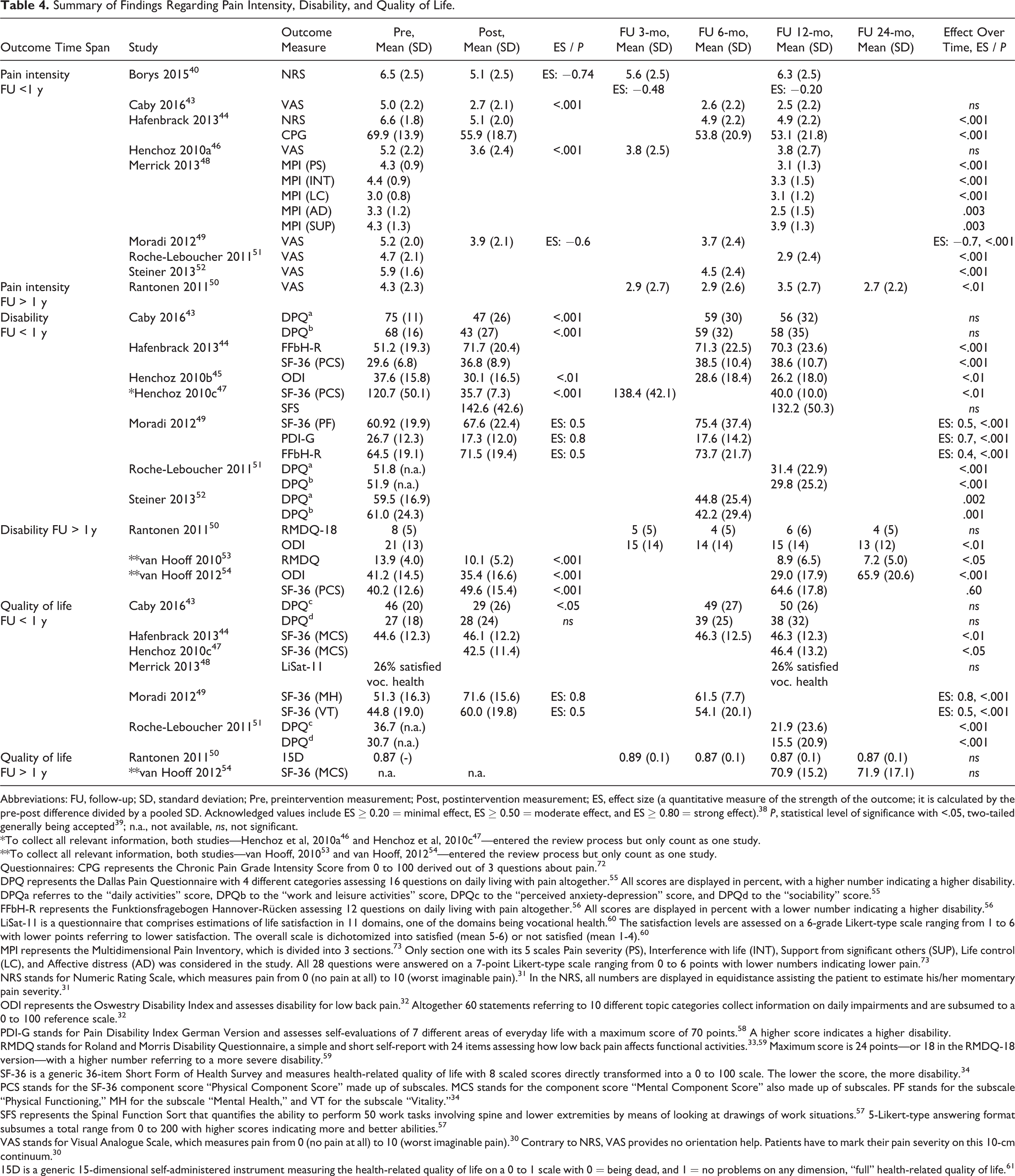
Abbreviations: FU, follow-up; SD, standard deviation; Pre, preintervention measurement; Post, postintervention measurement; ES, effect size (a quantitative measure of the strength of the outcome; it is calculated by the pre-post difference divided by a pooled SD. Acknowledged values include ES ≥ 0.20 = minimal effect, ES ≥ 0.50 = moderate effect, and ES ≥ 0.80 = strong effect). 38 P, statistical level of significance with <.05, two-tailed generally being accepted 39 ; n.a., not available, ns, not significant.
*To collect all relevant information, both studies—Henchoz et al, 2010a 46 and Henchoz et al, 2010c 47 —entered the review process but only count as one study.
**To collect all relevant information, both studies—van Hooff, 2010 53 and van Hooff, 2012 54 —entered the review process but only count as one study.
Questionnaires: CPG represents the Chronic Pain Grade Intensity Score from 0 to 100 derived out of 3 questions about pain. 72
DPQ represents the Dallas Pain Questionnaire with 4 different categories assessing 16 questions on daily living with pain altogether. 55 All scores are displayed in percent, with a higher number indicating a higher disability. DPQa referres to the “daily activities” score, DPQb to the “work and leisure activities” score, DPQc to the “perceived anxiety-depression” score, and DPQd to the “sociability” score. 55
FFbH-R represents the Funktionsfragebogen Hannover-Rücken assessing 12 questions on daily living with pain altogether. 56 All scores are displayed in percent with a lower number indicating a higher disability. 56
LiSat-11 is a questionnaire that comprises estimations of life satisfaction in 11 domains, one of the domains being vocational health. 60 The satisfaction levels are assessed on a 6-grade Likert-type scale ranging from 1 to 6 with lower points referring to lower satisfaction. The overall scale is dichotomized into satisfied (mean 5-6) or not satisfied (mean 1-4). 60
MPI represents the Multidimensional Pain Inventory, which is divided into 3 sections. 73 Only section one with its 5 scales Pain severity (PS), Interference with life (INT), Support from significant others (SUP), Life control (LC), and Affective distress (AD) was considered in the study. All 28 questions were answered on a 7-point Likert-type scale ranging from 0 to 6 points with lower numbers indicating lower pain. 73
NRS stands for Numeric Rating Scale, which measures pain from 0 (no pain at all) to 10 (worst imaginable pain). 31 In the NRS, all numbers are displayed in equidistance assisting the patient to estimate his/her momentary pain severity. 31
ODI represents the Oswestry Disability Index and assesses disability for low back pain. 32 Altogether 60 statements referring to 10 different topic categories collect information on daily impairments and are subsumed to a 0 to 100 reference scale. 32
PDI-G stands for Pain Disability Index German Version and assesses self-evaluations of 7 different areas of everyday life with a maximum score of 70 points. 58 A higher score indicates a higher disability.
RMDQ stands for Roland and Morris Disability Questionnaire, a simple and short self-report with 24 items assessing how low back pain affects functional activities. 33,59 Maximum score is 24 points—or 18 in the RMDQ-18 version—with a higher number referring to a more severe disability. 59
SF-36 is a generic 36-item Short Form of Health Survey and measures health-related quality of life with 8 scaled scores directly transformed into a 0 to 100 scale. The lower the score, the more disability. 34
PCS stands for the SF-36 component score “Physical Component Score” made up of subscales. MCS stands for the component score “Mental Component Score” also made up of subscales. PF stands for the subscale “Physical Functioning,” MH for the subscale “Mental Health,” and VT for the subscale “Vitality.” 34
SFS represents the Spinal Function Sort that quantifies the ability to perform 50 work tasks involving spine and lower extremities by means of looking at drawings of work situations. 57 5-Likert-type answering format subsumes a total range from 0 to 200 with higher scores indicating more and better abilities. 57
VAS stands for Visual Analogue Scale, which measures pain from 0 (no pain at all) to 10 (worst imaginable pain). 30 Contrary to NRS, VAS provides no orientation help. Patients have to mark their pain severity on this 10-cm continuum. 30
15D is a generic 15-dimensional self-administered instrument measuring the health-related quality of life on a 0 to 1 scale with 0 = being dead, and 1 = no problems on any dimension, “full” health-related quality of life. 61
Disability
The 8 studies reporting disability used 7 different instruments (Dallas Pain Questionnaire, DPQ 55 ; Funktionsfragebogen Hannover, FFbH-R 56 ; ODI 32 ; SF-36 34 ; Spinal Function Sort, SFS 57 ; Pain Disability Index–German Version, PDI-G 58 ; 18-item version of the Roland Morris Disability Questionnaire, RMDQ-18 59 ), rendering direct comparisons difficult. Nevertheless, all comparisons between pre- and posttreatment scores revealed moderate to large ESs or P values for reduction in functional disability (ES 0.4 to 0.8; P < .01 to P < .001; Table 4). Reduction in pain-related disability persisted for 24 months in the studies that examined a longer time frame (P < .05 to P < .001). Rantonen et al, 50 who included non-sick-listed employees, reported neither short- nor long-term changes in disability (Table 4).
Health-Related Quality of Life
Four different instruments were used to assess HRQoL (DPQ 55 ; Life Satisfaction Questionnaire 11; LiSat-11 60 ; SF-36 34 ; generic 15-dimensional self-administered 15D instrument 61 ), which probably contributed to the conflicting results. Three studies found no long-term increase in the HRQoL after MBR: Caby et al 43 found a short-term reduction in one HRQoL variable 43 and neither Rantonen et al 50 nor Merrick et al 48 detected any change in HRQoL (Table 4). The other 4 studies reported moderate to large increases in HRQoL that persisted for at least 12 months (ES 0.5 to 0.8; P < .05 to P < .001).
Cost-Effectiveness
Three of the 12 studies examined economic parameters of MBR and all demonstrated that indirect costs substantially exceed direct costs and that MBR produced a substantial reduction in direct and indirect costs (Table 5). Henchoz et al 46 found that direct and indirect monthly costs were, respectively, 94% and 84% lower 12 months after treatment (P = .004) while quality-adjusted life years (QALYs) remained stable over the 12 months following treatment. Brömme et al 41 reported a reduction of costs per person over the 12 months following treatment but found that this was not maintained beyond 12 months, they suggested that this was because people gradually returned to their preintervention habits. In contrast, Busch et al 42 demonstrated an overall cost reduction of €3583 per subject 12 months after MBR 42 ; taking into account the costs of the intervention, disability pension, and incremental costs of sick leave they projected the intervention would result in a reduction of €53 382 per subject over 10 years (Table 5). 42
Summary of Findings Regarding Cost-Effectiveness.
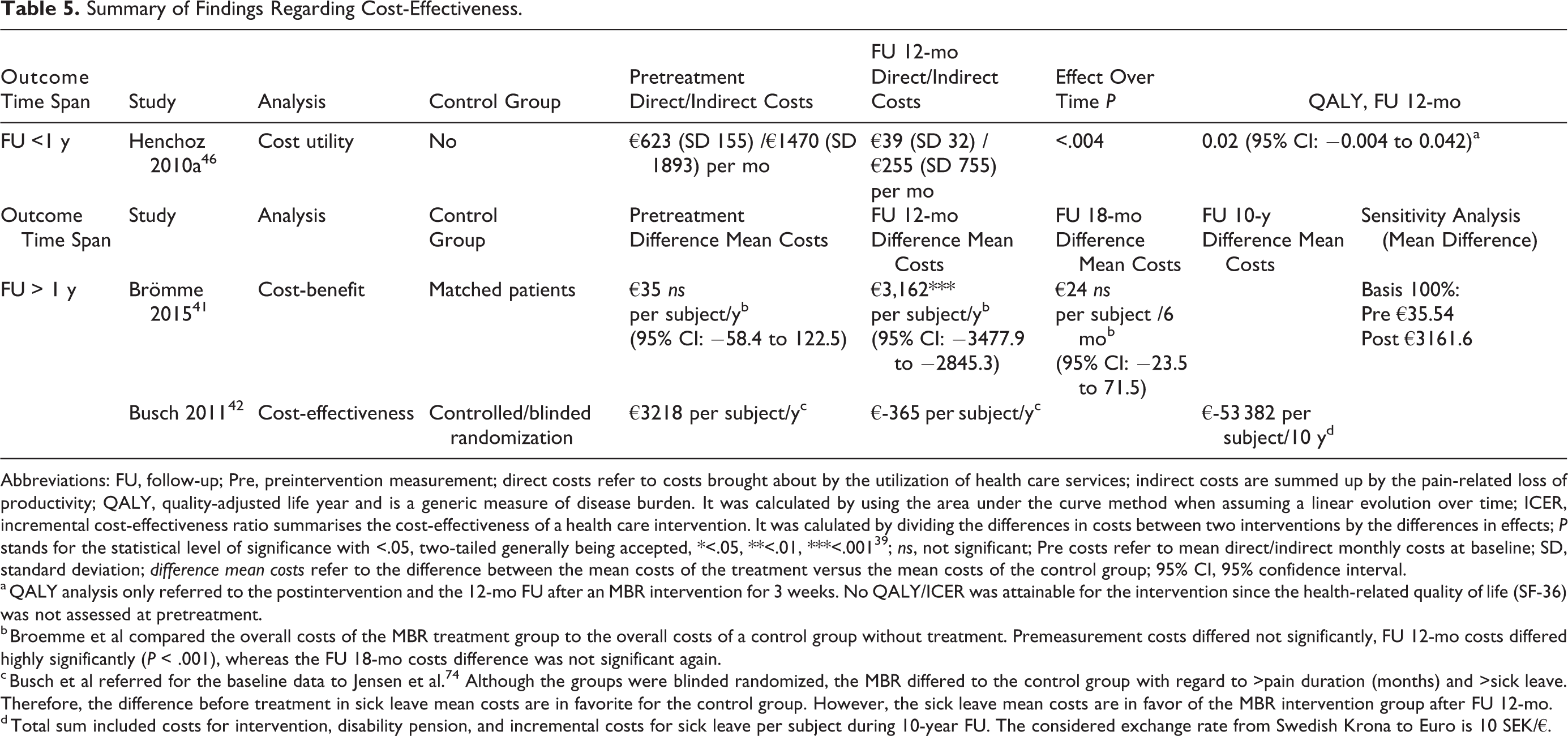
Abbreviations: FU, follow-up; Pre, preintervention measurement; direct costs refer to costs brought about by the utilization of health care services; indirect costs are summed up by the pain-related loss of productivity; QALY, quality-adjusted life year and is a generic measure of disease burden. It was calculated by using the area under the curve method when assuming a linear evolution over time; ICER, incremental cost-effectiveness ratio summarises the cost-effectiveness of a health care intervention. It was calulated by dividing the differences in costs between two interventions by the differences in effects; P stands for the statistical level of significance with <.05, two-tailed generally being accepted, *<.05, **<.01, ***<.001 39 ; ns, not significant; Pre costs refer to mean direct/indirect monthly costs at baseline; SD, standard deviation; difference mean costs refer to the difference between the mean costs of the treatment versus the mean costs of the control group; 95% CI, 95% confidence interval.
a QALY analysis only referred to the postintervention and the 12-mo FU after an MBR intervention for 3 weeks. No QALY/ICER was attainable for the intervention since the health-related quality of life (SF-36) was not assessed at pretreatment.
b Broemme et al compared the overall costs of the MBR treatment group to the overall costs of a control group without treatment. Premeasurement costs differed not significantly, FU 12-mo costs differed highly significantly (P < .001), whereas the FU 18-mo costs difference was not significant again.
c Busch et al referred for the baseline data to Jensen et al. 74 Although the groups were blinded randomized, the MBR differed to the control group with regard to >pain duration (months) and >sick leave. Therefore, the difference before treatment in sick leave mean costs are in favorite for the control group. However, the sick leave mean costs are in favor of the MBR intervention group after FU 12-mo.
d Total sum included costs for intervention, disability pension, and incremental costs for sick leave per subject during 10-year FU. The considered exchange rate from Swedish Krona to Euro is 10 SEK/€.
Work Ability
Sick leave and return to work (RTW) were the 2 main indicators of work ability (Table 6). Sick leave is defined as absence from work due to illness, whereas RTW relates to the number of workers who returned to work after a defined period of sick leave. Three out of 5 studies reported a moderate to strong P value with regard to RTW in the 12 months after MBR (P < .01 to P < .001). Of the remaining 2 studies, one did not report work-related follow-up data 44 and the other mentioned RTW only in passing. 54 The 1-year follow-up data on sick leave present a similar picture. All 3 studies demonstrated moderate to large ESs in sick-leave duration over time, however, some conflicting results must be mentioned. Roche-Leboucher et al, 51 who compared MBR with active physical therapy (PT), found a highly significant reduction in sick leave days over a 12-month MBR follow-up but over the same period there was no group difference in RTW.
Work-Ability: Sick Leave and Return to Work.
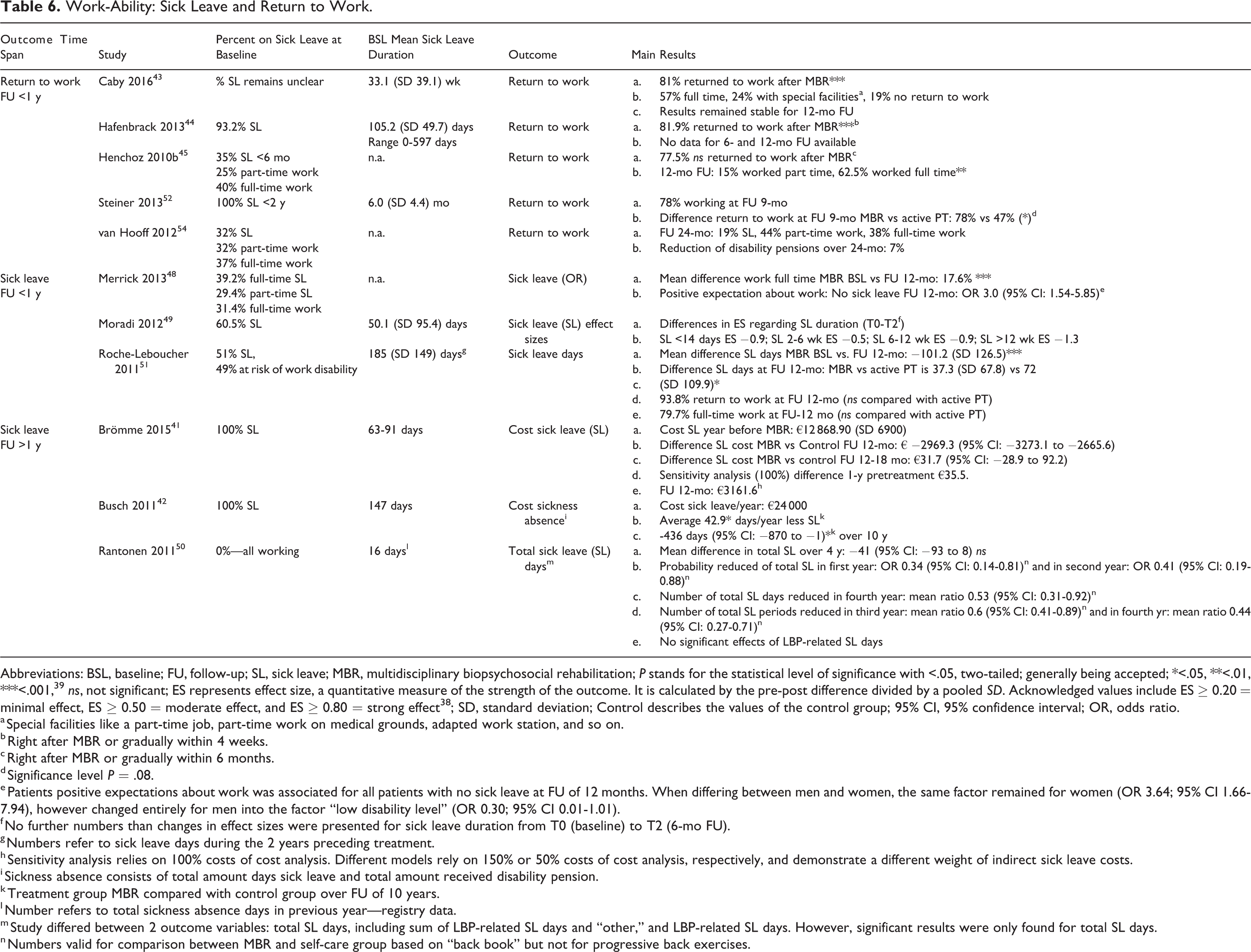
Abbreviations: BSL, baseline; FU, follow-up; SL, sick leave; MBR, multidisciplinary biopsychosocial rehabilitation; P stands for the statistical level of significance with <.05, two-tailed; generally being accepted; *<.05, **<.01, ***<.001, 39 ns, not significant; ES represents effect size, a quantitative measure of the strength of the outcome. It is calculated by the pre-post difference divided by a pooled SD. Acknowledged values include ES ≥ 0.20 = minimal effect, ES ≥ 0.50 = moderate effect, and ES ≥ 0.80 = strong effect 38 ; SD, standard deviation; Control describes the values of the control group; 95% CI, 95% confidence interval; OR, odds ratio.
a Special facilities like a part-time job, part-time work on medical grounds, adapted work station, and so on.
b Right after MBR or gradually within 4 weeks.
c Right after MBR or gradually within 6 months.
d Significance level P = .08.
e Patients positive expectations about work was associated for all patients with no sick leave at FU of 12 months. When differing between men and women, the same factor remained for women (OR 3.64; 95% CI 1.66-7.94), however changed entirely for men into the factor “low disability level” (OR 0.30; 95% CI 0.01-1.01).
f No further numbers than changes in effect sizes were presented for sick leave duration from T0 (baseline) to T2 (6-mo FU).
g Numbers refer to sick leave days during the 2 years preceding treatment.
h Sensitivity analysis relies on 100% costs of cost analysis. Different models rely on 150% or 50% costs of cost analysis, respectively, and demonstrate a different weight of indirect sick leave costs.
i Sickness absence consists of total amount days sick leave and total amount received disability pension.
k Treatment group MBR compared with control group over FU of 10 years.
l Number refers to total sickness absence days in previous year—registry data.
m Study differed between 2 outcome variables: total SL days, including sum of LBP-related SL days and “other,” and LBP-related SL days. However, significant results were only found for total SL days.
n Numbers valid for comparison between MBR and self-care group based on “back book” but not for progressive back exercises.
Over longer follow-up periods. the results are mixed. Busch et al 42 demonstrated a clear long-term improvement in sickness absence, reporting that the treatment group managed on average 436 more workdays than the control group over a 10-year period, whereas Brömme et al 41 found that the marked increase in costs relative to a control group over the first 12 months after MBR (€ −2969.3; 95% CI −3273.1 to −2665.6) was not maintained 41 : The costs of both groups were similar for the period between 12 and 18 months post-MBR. 41 Finally, Rantonen et al 50 found no changes in LBP-related sick leave days over the 4 years following MBR in their group of non-sick-listed employees although they did find that compared with self-treatment guided by a back book, MBR reduced total sick leave days in the first (odds ratio = 0.34, 95% CI 0.14 to 0.81) and second (odds ratio = 0.41, 95% CI 0.19 to 0.88) years after the intervention. They also found that the MBR group had fewer sick leave periods than the self-treatment group in the third and fourth years and fewer days of sick leave in the fourth year. 50 We conclude that overall there is some evidence suggestive of a long-term impact of MBR on work ability.
Discussion
Main Findings
This systematic review aimed to examine the literature on the efficacy, clinical utility, and cost-effectiveness of MBRs (>25 hours per week) including CBT approach, as treatments for persistent LBP or persistent NSLBP. Application of our exclusion and inclusion criteria resulted in the selection of 13 studies published between January 2010 and July 2017. In these studies pain, disability, HRQoL, and sick leave/RTW were used as indicators of effectiveness, clinical utility, and monthly costs and QALYs as measures of cost effectiveness. As expected, 19 all studies reported moderate to large reductions in short- and long-term pain and disability and, although the results were arguably less impressive, improvement in HRQoL. It seems reasonable therefore, to conclude that MBR has proven short- and long-term efficacy. A high-quality study demonstrated an impressive projected decrease in direct and indirect costs of €53 382 per subject over 10 years. 42 The other 2 studies that looked at cost-effectiveness also confirmed that over 12 months MBR was cost-effective. 41,46 Unfortunately, Henchoz et al 46 were not able to calculate incremental cost-effectiveness ratios of the increase in QALYs following MBR due to methodological shortcomings. In summary, the literature presented in this review generally suggests that MBR is both clinically effective and cost-effective for patients with persistent LBP or persistent NSLBP. Furthermore, the studies included in the review demonstrate that the feasibility and utility of MBR extends to a variety of settings. 12
Eleven of the 13 studies identified in the systematic literature search reported the work ability of patients treated by MBR. All found moderate to large effects on RTW and duration of sick leave that persisted for at least 12 months. There were, however, some conflicting results. Brömme et al 51 found that after more than 12 months MBR had no effect on sick leave. Taking into consideration the methodological quality of the selected studies we are unable to draw a conclusion about the long-term impact of MBR, although they hint at a tendency toward a long-lasting impact on work ability. This is crucial as work ability is a more sensitive indicator of work-related productivity losses than absenteeism or duration of sick leave. Norlund et al, 62 Hoefsmit et al, 63 and Øyeflaten et al 64 all reported that treatments similar to MBR had a positive impact on RTW and through this, reduced the long-term indirect costs. 41 However, evidence remains conflicting. 19,65 –67 Further high-quality investigations are needed.
Strengths and Limitations
This systematic review has several strengths, including methodological rigor as it complies with the PRISMA guidelines 35,36 and uses the GRADE approach to indicate the quality of the evidence reviewed. 37 We also used well-defined inclusion criteria and selected only original articles involving a clearly-defined MBR intervention including a CBT element 19 with a follow-up period of at least 12 months. Finally, our review examines studies using outcome measures relevant to the efficacy, clinical utility, and cost-effectiveness of MBR in people with persistent LBP or persistent NSLBP. 29
The main limitations include the low number of studies included and the lack of high-quality studies. Well-defined inclusion criteria clearly limit the number of eligible studies. Our sample of 13 studies represents 1.1% of the 1199 publications originally identified and is higher than the 0.7% inclusion rate Kamper et al 19 reported in their Cochrane review. The second main limitation of our review is the lack of high-quality studies. There is a need for high-quality studies of MBR, particularly with regard to its impact on work ability and sick leave.
In this review, we addressed the lack of high-quality studies by examining indicators of the economic success of MBR. The lack of standardization of outcome domains is one of the most urgent problems affecting reporting of MBR outcomes in cases of persistent pain. 68 In an attempt to offer a fresh perspective Wieser et al 69 reported the economic consequences of LBP or NSLBP from a societal perspective, distinguishing between 2 productivity losses: work absenteeism, a temporary absence from work due to LBP or NSLBP, and work presenteeism, the reduced productivity of employees working despite illness. Not surprisingly, presenteeism added much more to the costs than absenteeism. 69 It remains unclear, however, to which group patients returning to work after a period of sick leave should be assigned. Given the burgeoning personal and public costs of LBP further high-quality analyses of the temporal pattern of productivity losses are warranted. 9 Surprisingly, our selection criteria resulted in an exclusively European sample, which may limit the generalizability of the results to other regions; we speculate that our search terms and defined inclusion and exclusion criteria may be biased by our European perspective despite our international experience. However, with regard to Kamper et al, 19 who did not detect substantially different effects in treatments with a high intensity (>25 hours per week) compared with less intensive interventions, one could presume that less intensive interventions are to be favored. Furthermore, performing an intensive intervention with at least 25 hours of treatment per week might substantially reduce its clinical utility with regard to time needed and efficiency of the treatment. Further methodological limitations include the lack any measure of the heterogeneity (Q or I2) of outcome measures, although as this is a systematic review rather than a meta-analysis heterogeneity testing would not generally be expected.
Implications
The results presented here confirm that MBR is effective as a treatment for persistent LBP and persistent NSLBP, and that there is a tendency for MBR to be cost-effective in such cases, at least over the first 12 months after treatment. In summary, the evidence suggests that these multidisciplinary treatments have therapeutic benefits, but the next aim of international experts and experienced clinicians should be to agree on a core set of outcome variables. With regard to sick leave or RTW issues, different study approaches are needed, addressing disabling work characteristics or maladaptive beliefs, emotions and fears. For example, a recent study presented the Yellow Flag Questionnaire (YFQ), 70 a mixture of established yellow flag questions developed via a Delphi process. 70 Moreover, a recent systematic review underlined the effectiveness of psychologically informed physical therapy (PIPT) for patients with persistent LBP with regard to the outcomes pain, pain interference, disability, and pain self-efficacy. Further high-quality investigations, however, are needed to gain knowledge about the cost-effectiveness of PIPT. 71
Conclusion
Multidimensional treatments for patients with persistent LBP or persistent NSLBP are effective although there is room for improvement in cost-effectiveness and impact on sickness absence. A degree of tailoring of treatment to individual needs might improve the cost-effectiveness of such treatments or their impact on RTW.
Supplemental Material
GSJ765483_suppl_mat - Treatment Efficacy, Clinical Utility, and Cost-Effectiveness of Multidisciplinary Biopsychosocial Rehabilitation Treatments for Persistent Low Back Pain: A Systematic Review
GSJ765483_suppl_mat for Treatment Efficacy, Clinical Utility, and Cost-Effectiveness of Multidisciplinary Biopsychosocial Rehabilitation Treatments for Persistent Low Back Pain: A Systematic Review by Cornelia Rolli Salathé, Markus Melloh, Rebecca Crawford, Stephanie Scherrer, Norbert Boos, and Achim Elfering in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.