
Abstract
Study Design:
Systematic review.
Objectives:
Allogeneic blood transfusion-related immunomodulation may relatively suppress the immune system, heightening the risk of infection following spine surgery. This systematic review seeks to determine whether allogeneic blood transfusion increases the risk of postoperative infection and whether there are any factors that modify this association.
Methods:
PubMed, Cochrane Central Register of Controlled Trials, and reference lists from included studies were searched from inception to April 20, 2017 to identify studies examining the risk of infection following allogeneic blood transfusion in adult patients receiving surgery for degenerative spine disease.
Results:
Eleven retrospective cohort or case-control studies, involving 8428 transfusion patients and 43 242 nontransfusion patients, were identified as meeting the inclusion criteria. Regarding surgical site infection (SSI), the results were mixed with roughly half reporting a significant association. There was an association between allogeneic transfusion and urinary tract infection (UTI) and any infection, but not respiratory tract infection. There was no statistical modifying effect of lumbar versus thoracic surgery on the association of allogeneic transfusion and SSI, though subgroup analyses in 3 of 4 studies reported a statistical association between transfusion and postoperative infections, including SSI, UTI, and any infection within the lumbar spine.
Conclusions:
This systematic review failed to find a consistent association between allogeneic transfusion and postoperative infection in spine surgery patients. However, these studies were all retrospective with a high or moderately high risk of bias. To properly examine this association an observational prospective study of sufficient power, estimated as 2400 patients, is required.
Introduction
The United States has seen a growing rate of allogeneic blood transfusion in the context of spine surgery. 1,2 Intraoperative blood loss necessitates the transfusion of allogeneic blood to avoid perioperative anemia, itself identified as an independent risk factor in perioperative morbidity and mortality. 3,4 However, there exist consequential trade-offs between the risks and benefits of allogeneic blood transfusion versus anemia in terms of their effects on perioperative outcomes. 3,4
Although the adverse effects of allogeneic blood transfusion on postoperative infection in the context of spine surgery have been demonstrated, the low power and uncontrolled potential confounds of many of these studies has limited the interpretation of their data. The aim of this systematic review is to evaluate the association between allogeneic transfusion and postoperative infection in spine surgery patients, as well as the many modifying risk factors. We sought to answer the following key questions: (1) Does allogeneic blood transfusion increased the risk of postoperative infection in patients undergoing spine surgery compared with no blood transfusion? (2) Are there any factors that modify the risk of infection associated with allogeneic blood transfusion?
Materials and Methods
Study Design: Systematic Review
Information Sources and Search
PubMed, Cochrane Central Register of Controlled Trials, and reference lists from included studies were searched from inception to April 20, 2017. Search strategy can be found in the Supplemental Online Material.
Eligibility Criteria
Inclusion criteria
(1) Adult patients receiving surgery for degenerative spine disease and (2) comparative studies comparing the risk of infection in those with allogeneic blood transfusion versus no blood transfusion.
Exclusion criteria
(1) More than or equal to 20% of patients who received spine surgery for trauma or cancer, (2) ≥20% of patients who received autologous blood instead of allogeneic blood, (3) outcomes other than infection, and (4) case series.
Data Identification and Extraction
Articles were selected for inclusion and data was extracted by 2 investigators (CF, JRD). Discrepancies were resolved through discussion. The following data items were recorded: study author, study design, study demographics (sample size, age, sex), data source, spine segment treated, timing of transfusion, covariates analyzed, odds ratio from both univariate and multivariate models comparing infection in those receiving blood transfusion versus no transfusion.
Outcomes
Surgical site infection, urinary tract infection, respiratory tract infection, sepsis.
Analysis and Synthesis of Results
Qualitative synthesis and meta-analysis. Because of the likelihood of confounding, the primary analysis used adjusted versus crude odds ratios. For meta-analysis, we performed a logarithmic transformation of the adjusted odds ratios and confidence intervals. The corresponding standard errors were then computed. Next the studies were pooled and weighted according to the inverse of their respective variances, which were derived from the standard errors. A random effects model was assumed. Final values were exponentiated back to and presented in their original scale. Calculations and figures were done with RevMan v. 5.2.
Results
Study Selection and Characteristics
We identified 19 of 88 studies as potentially meeting inclusion criteria. After full-text review of the 19 studies, 8 were excluded (wrong population, n = 3; wrong comparison, n=2; wrong study design, n = 2; and wrong outcome, n = 1) (Figure 1). Citations and a comprehensive list of reasons for exclusion can be found in the Supplemental Online Material. The remaining 11 met inclusion criteria and were retained. These studies involved 8428 patients who received a transfusion and 43 242 who did not. They are composed of 6 retrospective cohort studies 5 –10 and 5 retrospective case-control studies. 11 –15 All studies have moderately high or high risk of bias, class of evidence (CoE) III or IV (see Supplemental Online Material for CoE evaluation). Characteristics of the included studies are summarized in Table 1.
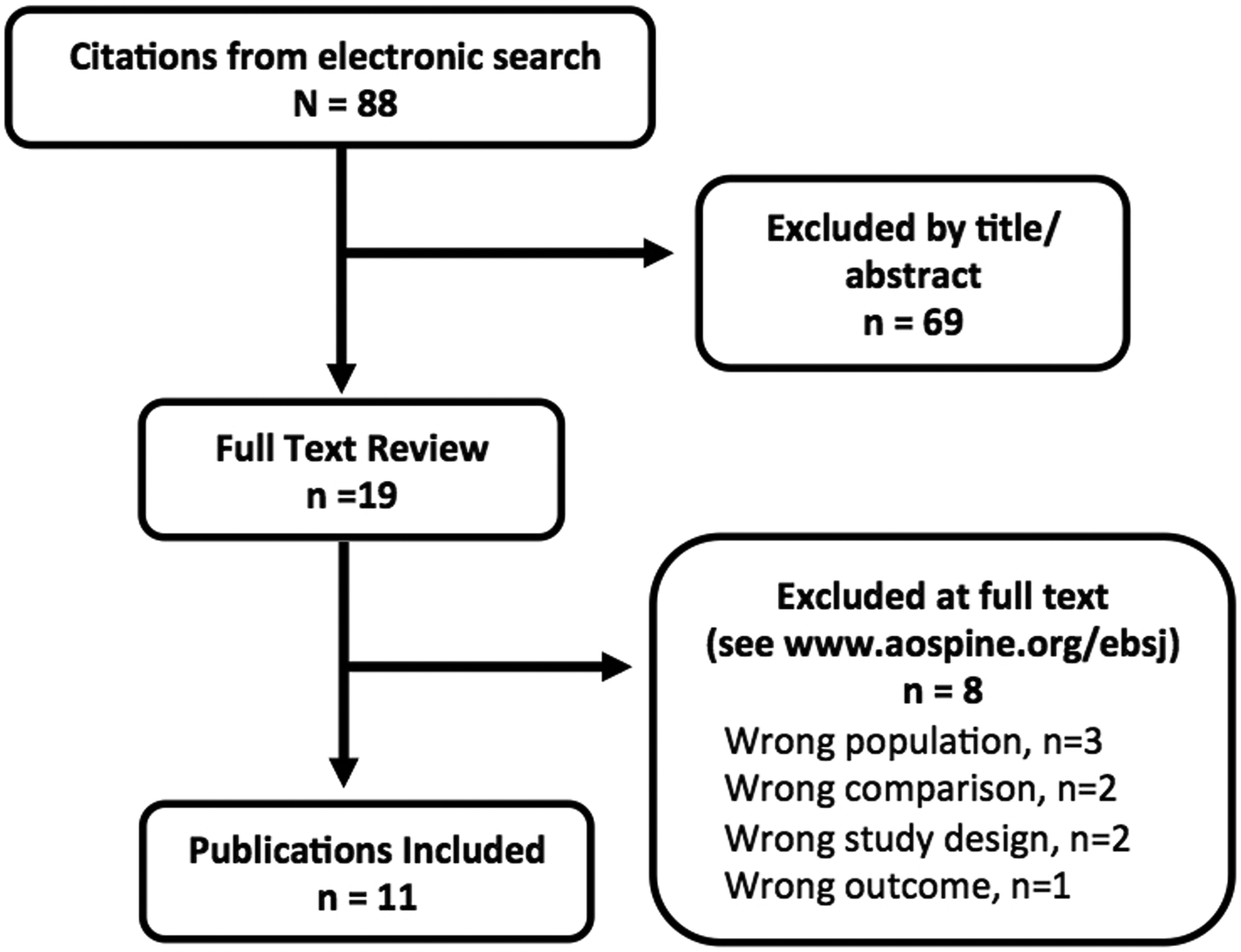
Study selection.
Study Characteristics.
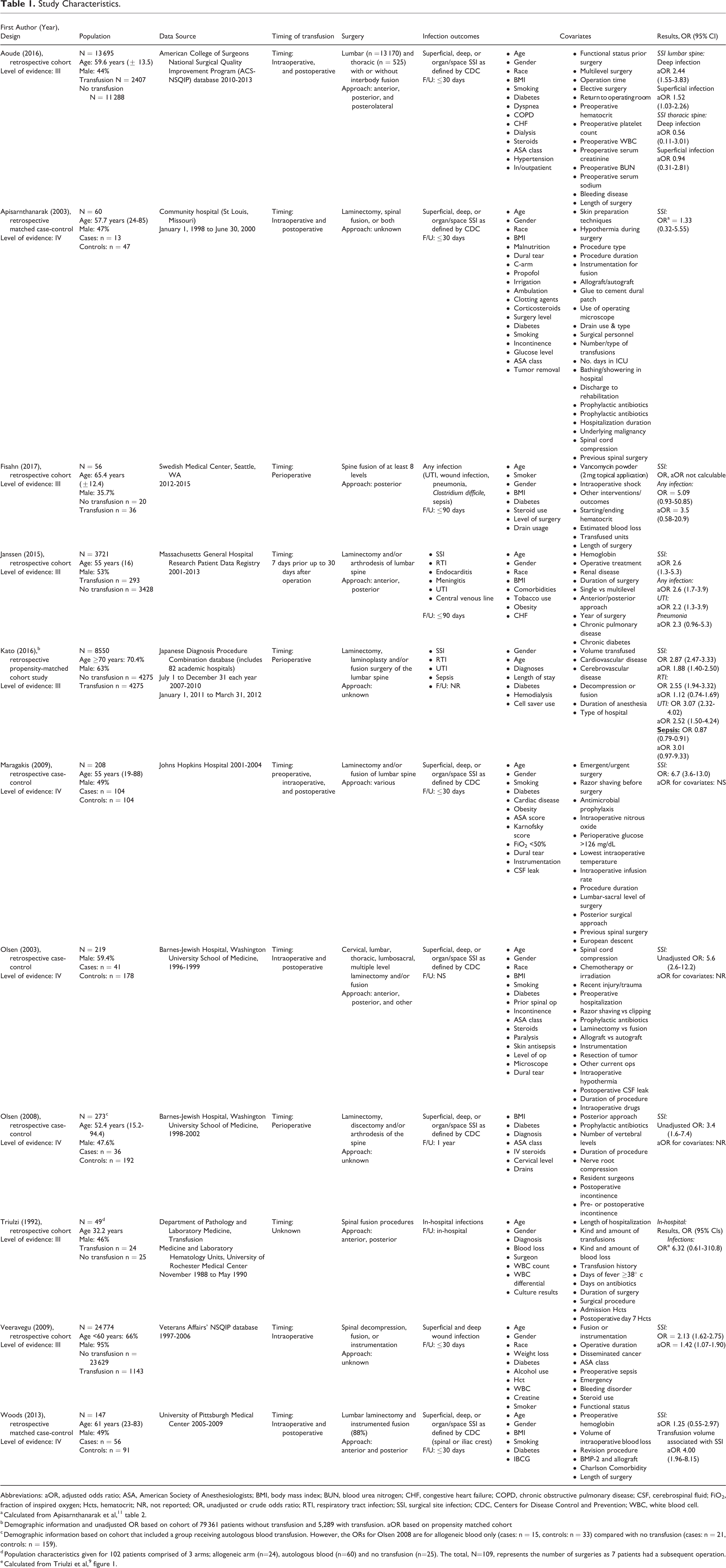
Abbreviations: aOR, adjusted odds ratio; ASA, American Society of Anesthesiologists; BMI, body mass index; BUN, blood urea nitrogen; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CSF, cerebrospinal fluid; FiO2, fraction of inspired oxygen; Hcts, hematocrit; NR, not reported; OR, unadjusted or crude odds ratio; RTI, respiratory tract infection; SSI, surgical site infection; CDC, Centers for Disease Control and Prevention; WBC, white blood cell.
b Demographic information and unadjusted OR based on cohort of 79 361 patients without transfusion and 5,289 with transfusion. aOR based on propensity matched cohort
c Demographic information based on cohort that included a group receiving autologous blood transfusion. However, the ORs for Olsen 2008 are for allogeneic blood only (cases: n = 15, controls: n = 33) compared with no transfusion (cases: n = 21, controls: n = 159).
d Population characteristics given for 102 patients comprised of 3 arms; allogeneic arm (n=24), autologous blood (n=60) and no transfusion (n=25). The total, N=109, represents the number of surgeries as 7 patients had a subsequent operation.
Does allogeneic blood transfusion increase the risk of postoperative infection in patients undergoing spine surgery compared with no blood transfusion?
Surgical Site Infection
With regard to surgical site infection (SSI), results from 10 low-quality studies are mixed; 3 studies report a significant association between allogeneic blood transfusion and infection, 7,8,10 4 report no significant association, 12 –15 1 study describes an association within certain patient subgroups but not in others 5 and 2 do not report multivarariate analysis 6,11 (Table 2).
Association (Crude and Adjusted Odds Ratio and 95% Confidence Interval) Between Allogeneic Blood Transfusion and Infection in Spine Surgery (P Value for Adjusted Odds Ratio Only).
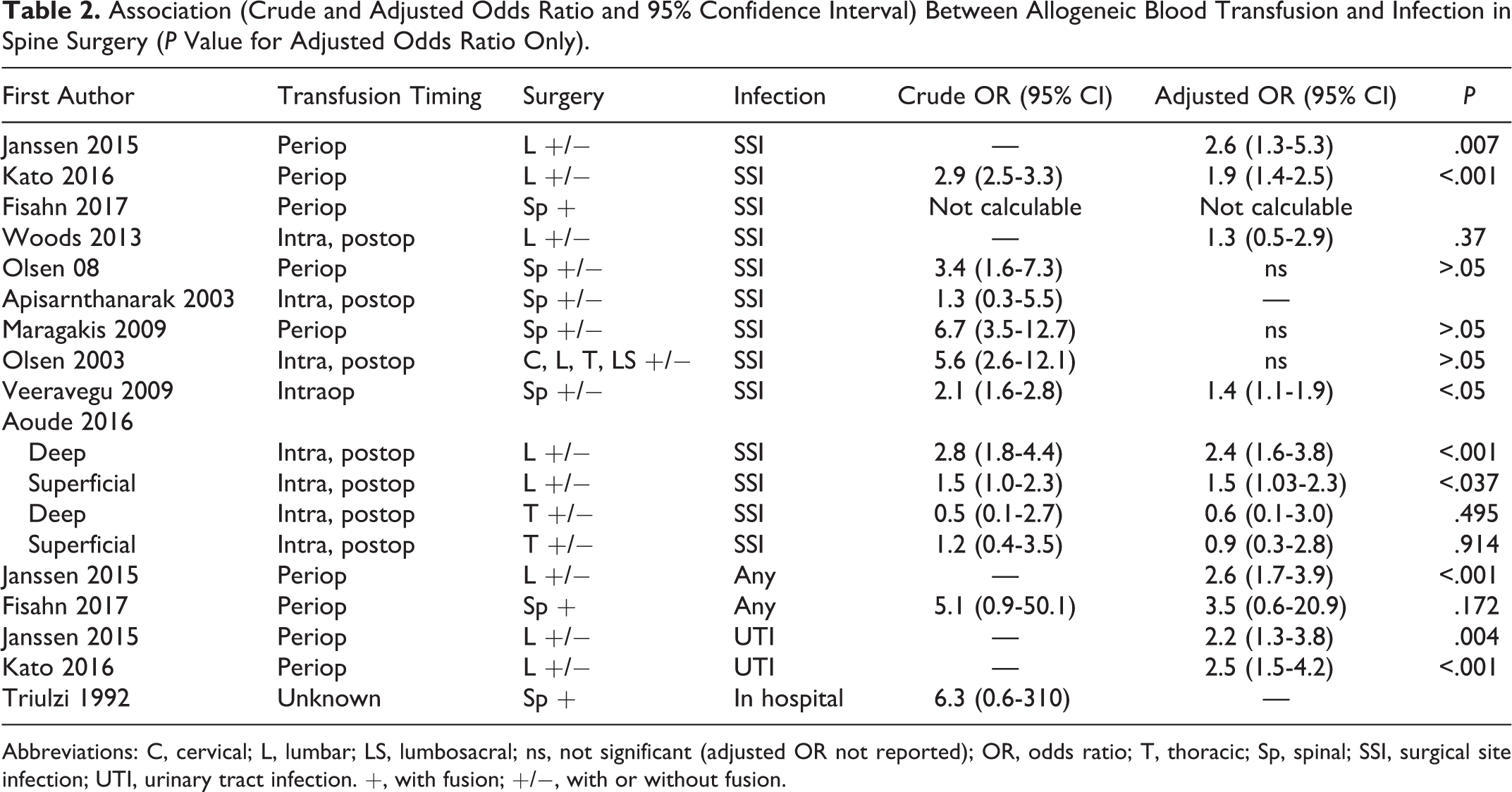
Abbreviations: C, cervical; L, lumbar; LS, lumbosacral; ns, not significant (adjusted OR not reported); OR, odds ratio; T, thoracic; Sp, spinal; SSI, surgical site infection; UTI, urinary tract infection. +, with fusion; +/−, with or without fusion.
Urinary Tract Infection
Two low-quality studies 7,8 found a significant association between allogeneic transfusion and urinary tract infection (UTI), pooled odds ratio 2.4 (95% CI, 1.6-3.5) (Figure 2).
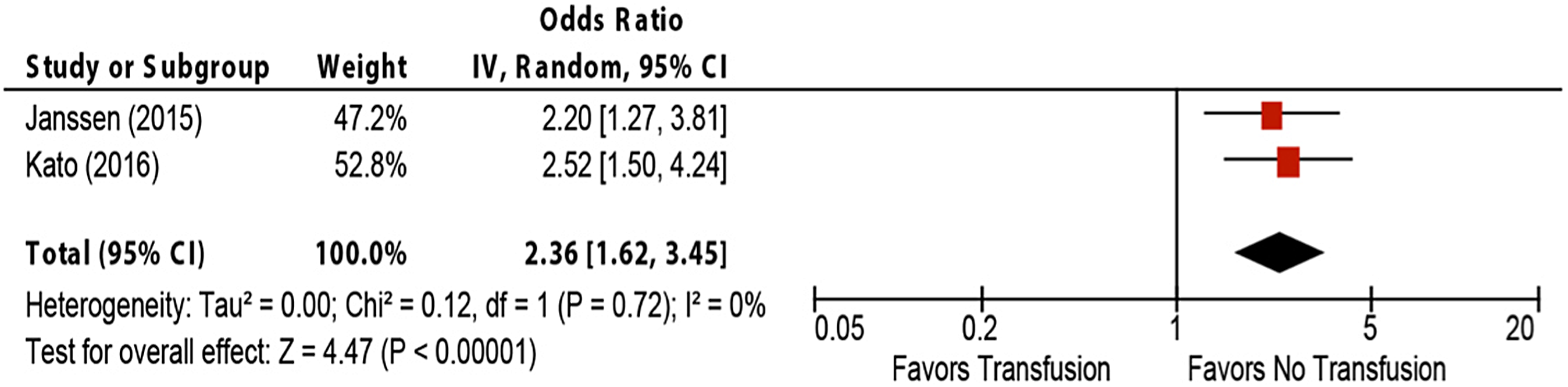
The association of allogeneic blood transfusion and urinary tract infection in spine surgery.
Respiratory Tract Infection
Two low quality studies 7,8 failed to find an association between allogeneic transfusion and respiratory tract infection (RTI), pooled odds ratio 1.5 (95% CI, 1.7-2.9) (Figure 3).
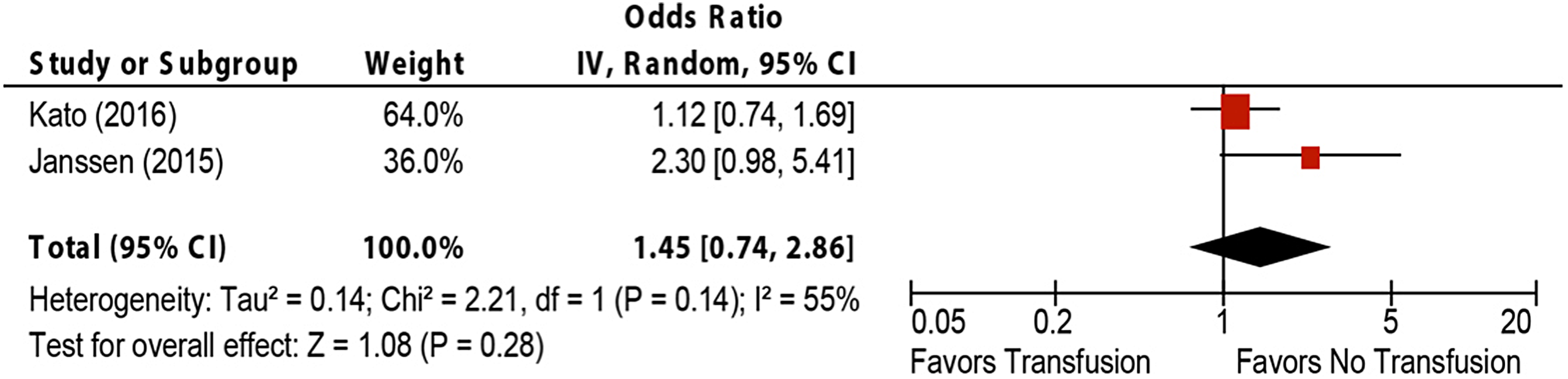
The association of allogeneic blood transfusion and respiratory tract infection.
Any Infection
Two low-quality studies assessed the association between allogeneic blood transfusion and any infection. Any infection is defined as an SSI, RTI, UTI, sepsis, and Clostridium difficile in one study by Fisahn et al, 6 and SSI, RTI, UTI, endocarditis, meningitis, and central venous line infection in a second study by Janssen et al. 7 Pooling the studies result in a significant association, pooled odds ratio 2.6 (95% CI, 1.8-4.0) (Figure 4).
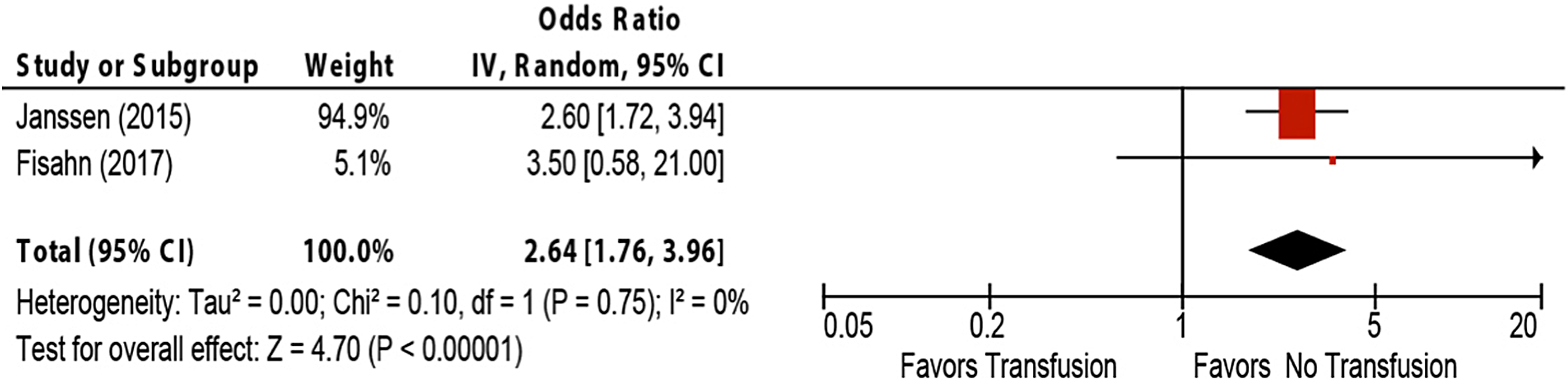
The association of allogeneic blood transfusion and any infection in spine surgery.
In-Hospital Infection
One small low-quality study did not find an association between allogeneic blood transfusion and in-hospital infection, crude odds ratio, 6.3 (95% CI, 0.6-310).
Are There Any Factors That Modify the Risk of Infection Associated With Allogeneic Blood Transfusion?
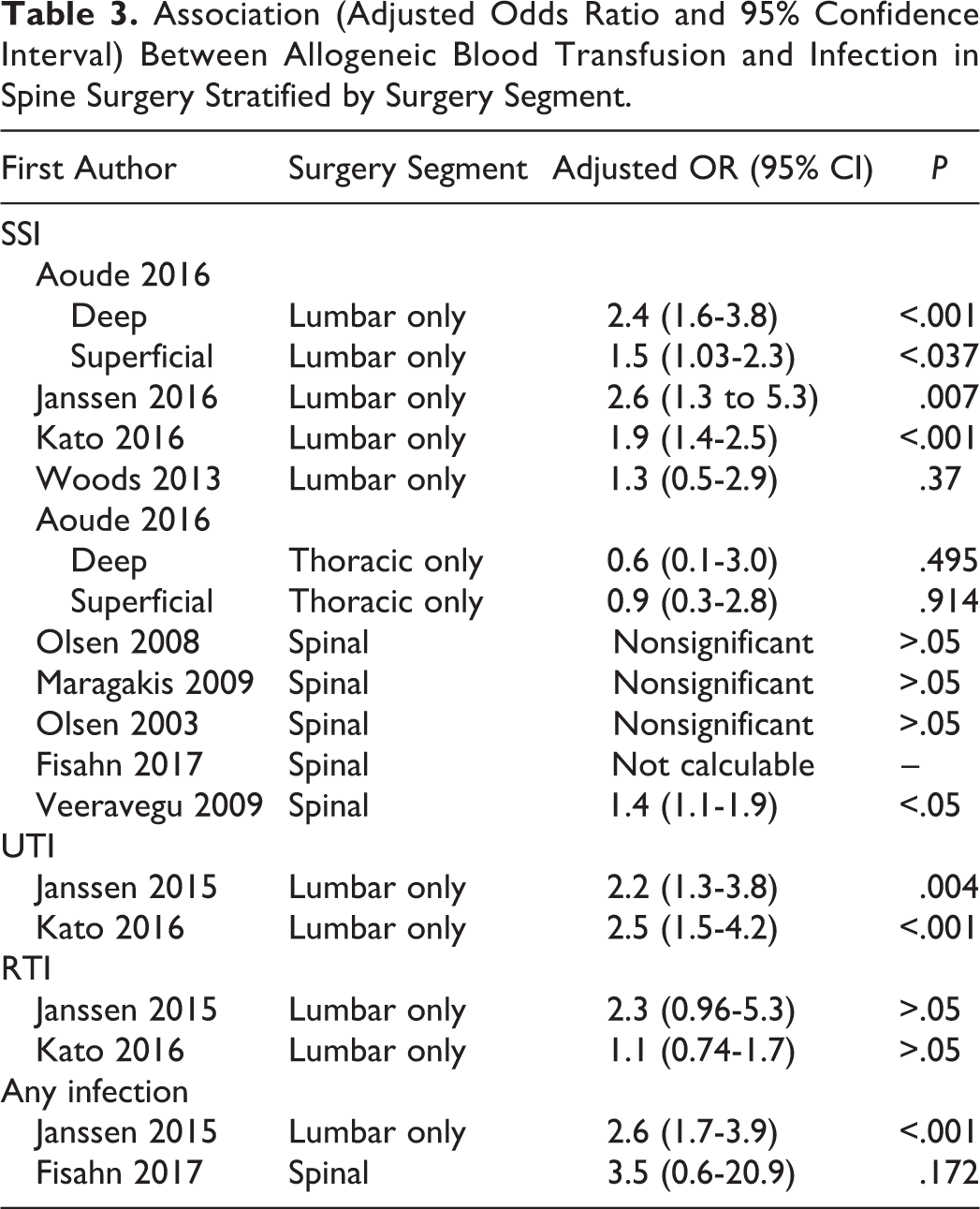
One study stratified SSI results by spine segment, lumbar and thoracic. There was no statistical difference between the subgroups, P = .10, possibly due to the small sample size and variability in the thoracic spine (Figure 5). Stratifying the results of all studies reporting SSI by spinal segment reveals that allogeneic blood transfusion is significantly associated with SSI in 3 of 4 studies in surgeries restricted to the lumbar spine. This is in contrast to only 1 of 5 studies reporting a significant association in studies of only the thoracic spine or in studies that likely include several segments (Table 3). The pattern is similar for UTI and any infection.
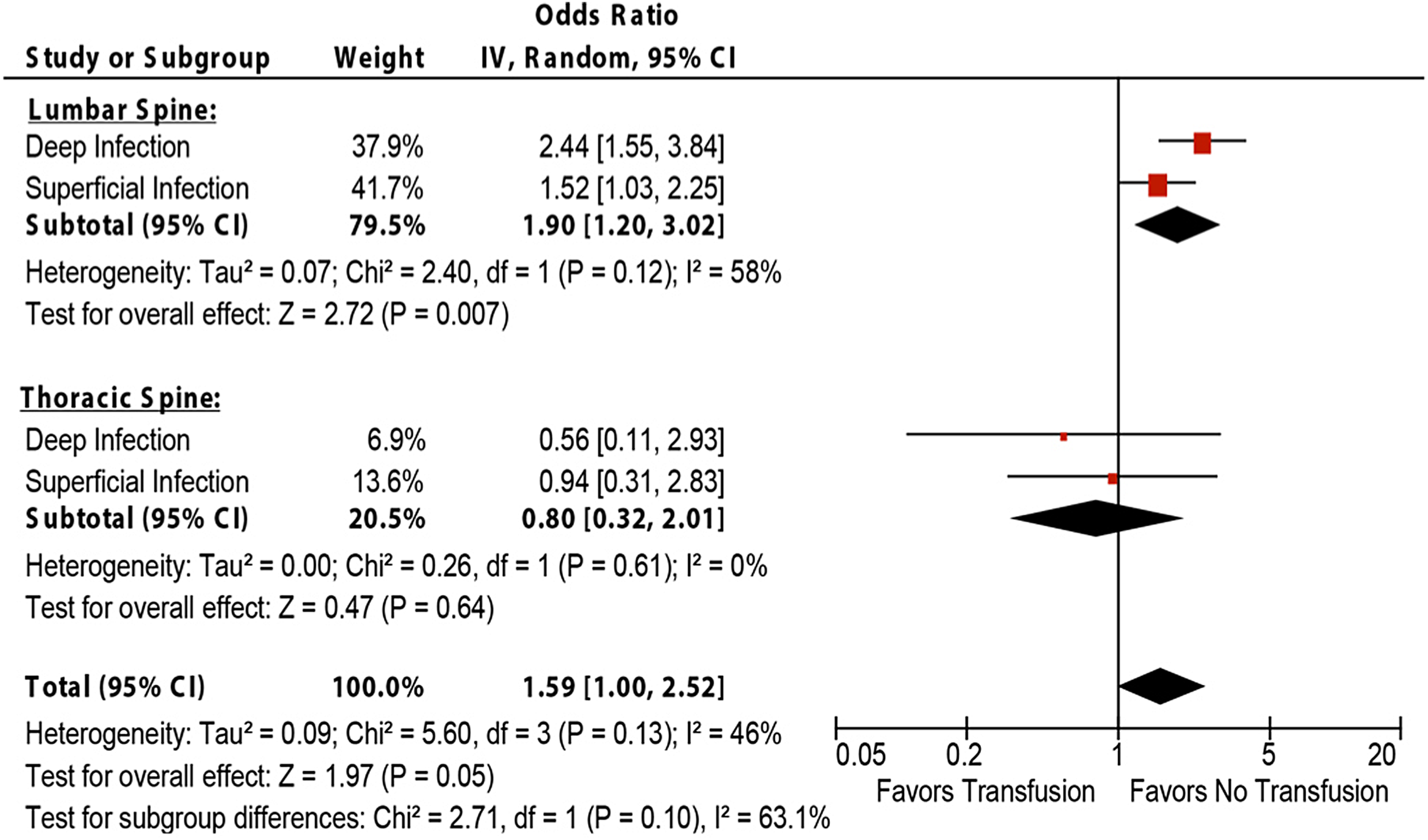
Subgroup analysis comparing the association of allogeneic blood transfusion and surgical site infection (SSI) between spine surgery of the lumbar and thoracic spines.
Association (Adjusted Odds Ratio and 95% Confidence Interval) Between Allogeneic Blood Transfusion and Infection in Spine Surgery Stratified by Surgery Segment.
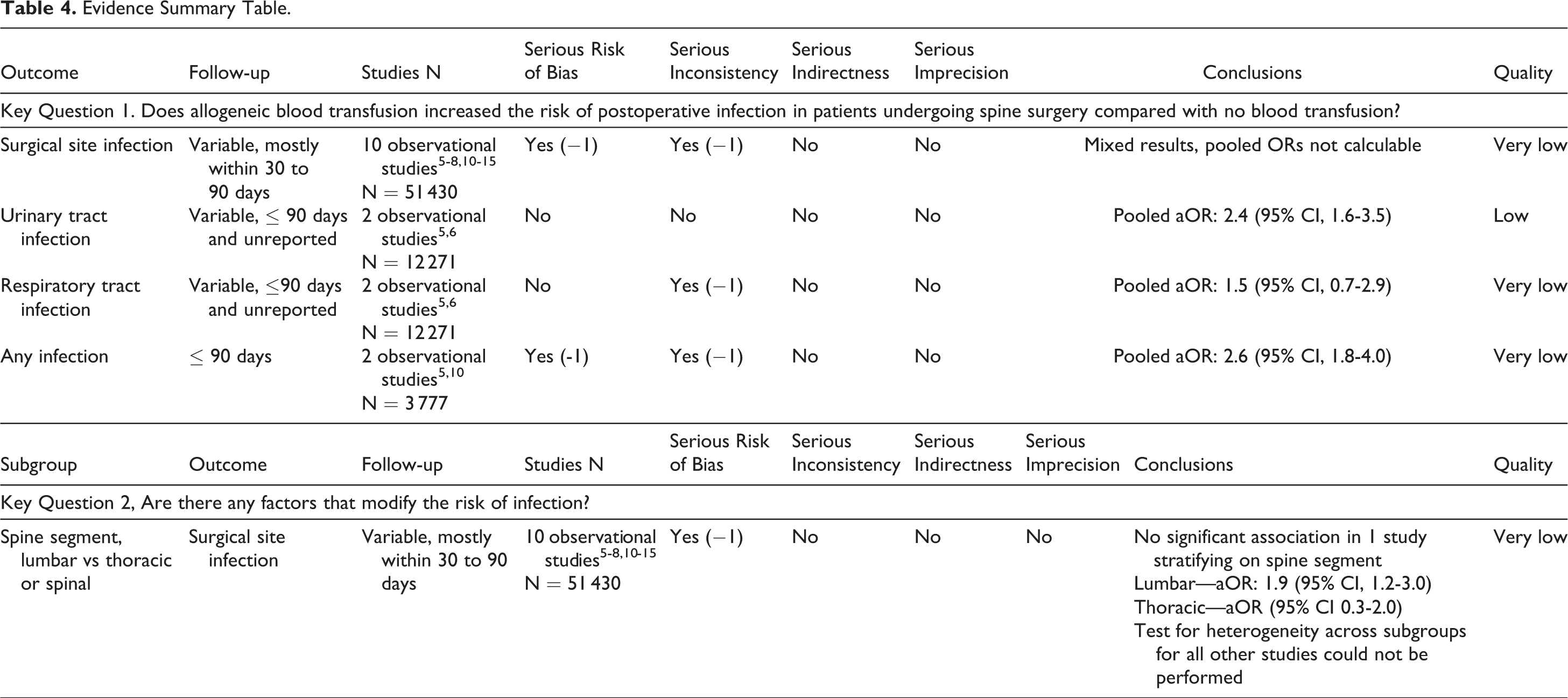
Evidence Summary (Table 4)
Mixed results as to whether allogeneic blood transfusion is associated with SSI in spine surgery patients, strength of evidence very low.
Allogeneic blood transfusion is associated with UTI; pooled odds ratio 2.4 (95% CI, 1.6-3.5), strength of evidence low.
No association between allogeneic blood transfusion and RTI; pooled odds ratio 1.5 (95% CI, 0.7-2.9), strength of evidence very low.
Allogeneic blood transfusion is associated with any infection; pooled odds ratio 2.6 (95% CI, 1.8-4.0), strength of evidence very low.
Allogeneic blood transfusion was not significantly associated with SSI in a direct comparison when the surgery was performed in the lumbar spine compared with thoracic spine, strength of evidence very low.
Evidence Summary Table.
Clinical Guidelines
American Association of Blood Banks’ (AABB) recommendations
16
: Recommendation 1: The AABB recommends a restrictive red blood cell (RBC) transfusion threshold in which the transfusion is not indicated until the hemoglobin level is 7 g/dL for hospitalized adult patients who are hemodynamically stable, including critically ill patients, rather than a liberal threshold when the hemoglobin level is 10 g/dL (strong recommendation, moderate quality evidence). For patients undergoing orthopedic surgery or cardiac surgery and those with preexisting cardiovascular disease, the AABB recommends a restrictive RBC transfusion threshold (hemoglobin level of 8 g/dL; strong recommendation, moderate quality evidence). The restrictive hemoglobin transfusion threshold of 7 g/dL is likely comparable to 8 g/dL, but randomized controlled trial (RCT) evidence is not available for all patient categories. These recommendations apply to all but the following conditions for which the evidence is insufficient for any recommendation: acute coronary syndrome, severe thrombocytopenia (patients treated for hematological or oncological disorders who at risk of bleeding), and chronic transfusion–dependent anemia. Recommendation 2: The AABB recommends that patients, including neonates, should receive RBC units selected at any point within their licensed dating period (standard issue) rather than limiting patients to transfusion of only fresh (storage length: <10 days) RBC units (strong recommendation, moderate quality evidence).
Discussion
We herein conducted a systematic review examining (a) whether allogeneic blood transfusion increases the risk of postoperative infection compared with no blood transfusion and (b) whether there are any factors that modify the risk of infection associated with allogeneic blood transfusion.
Addressing the first question, a body of very low strength evidence showed mixed results for an association between allogeneic blood transfusion and surgical site infection. This may be a result of confounding factors that are inherent to these different subgroups of patients, factors controlled for in some studies but not others. For example, 3 studies reporting no significant association controlled for American Society of Anesthesiologists (ASA) class 12 –14 while 2 studies reporting a significant association did not. 7,8 The posterior approach has been shown to be a risk factor for postoperative infection. 17 Three studies in our review adjusted for approach 7,12,14 whereas others did not. 5,8,10,13,15
Two low-strength studies found a significant association between allogeneic blood transfusion and UTI, yet no association was found between allogeneic blood transfusion and RTI. 7,8 The risk of any infection was significantly associated with allogeneic blood transfusions, but again with a very low strength of evidence. 6,7 The significant association between all infections and allogeneic blood transfusions found by Fisahn et al 6 was in a study population of only 56 patients, the smallest population to yield significant results in our series. When examining individual infection risks (eg, SSI, UTI) the association lost significance. However, the underlying assumption of the current clinical question is that allogeneic blood increases infection risk because of its systemic immunomodulatory effects. It is therefore appropriate to be pooling all postoperative infections to examine for an association with perioperative allogeneic transfusion.
Addressing the second question, a stratification of SSI data by spine segment, lumbar and thoracic, found allogeneic blood transfusion to be significantly associated with SSI in 3 of 4 studies in surgeries restricted to the lumbar spine. The increased potential for infection in the lumbar region may be due to its proximity to the perineal region, a significant potential source of infection.
Limitations
Studies included consisted only of low-quality retrospective studies with high or moderately high risk of bias. These studies are subject to confounding variables. In this review, every study reporting both univariate and multivariate analyses had important confounds as demonstrated by the large change in the odds ratio between the 2 analyses. Because of the retrospective designs, not all studies collected the same prognostic characteristics and potentially important information was omitted, such as volume of blood transfused. Prospective studies are needed, which identify and control for all important potential confounders for infection.
We estimate that 2400 patients will be needed in a prospective observational study to establish the relationship between autologous blood transfusions and the risk of SSI assuming an SSI risk of 2% in patients without transfusion, a power of 80%, and an effect size of 2.0.
Conclusion
This systematic review failed to find a consistent association between allogeneic transfusion and SSI in patients undergoing spinal surgery. However, the studies were all retrospective with a high or moderately high risk of bias. To understand the nature of the association between allogeneic blood transfusion and subsequent infection in spine surgery, appropriately designed and controlled prospective studies of sufficient power (n = 2400) are required.
Supplemental Material
Supplemental Material, Supplemental_digital_material_05-11-17 - Blood Transfusion and Postoperative Infection in Spine Surgery: A Systematic Review
Supplemental Material, Supplemental_digital_material_05-11-17 for Blood Transfusion and Postoperative Infection in Spine Surgery: A Systematic Review by Christian Fisahn, Cameron Schmidt, Josh E. Schroeder, Emiliano Vialle, Isador H. Lieberman, Joseph R. Dettori and Thomas A. Schildhauer in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.