
Abstract
Study Design:
Systematic review.
Objectives:
The objective of this systematic review was to answer 2 key questions: (1) What is the clinical presentation and probability of symptomatic improvement following treatment for patients with renal cell carcinoma (RCC) of the spine? (2) What is the overall survival of patients diagnosed with spinal metastases from RCC?
Methods:
A literature review was performed to identify articles that reported on survival, clinical outcomes, and/or prognostic factors in the RCC population with spinal metastases from 1986 to 2016.
Results:
Forty-eight articles (807 patients) were included. The Fuhrman Nuclear Grade has been significantly associated with survival in previous studies but was underpowered in the current study. The Memorial Sloan-Kettering Cancer Center Score (MSKCC/Motzer) was also underpowered in the current study. From the time of spinal metastasis, the mean and median survival for patients with previously diagnosed primary RCC was 8.75 and 11.7 months, respectively, whereas synchronously diagnosed patients (primary RCC and spinal metastasis) had a mean and median survival of 6.75 and 11 months, respectively. Patients with a “low” (0-8), “intermediate” (9-11), or “high” (12-15) revised Tokuhashi score at initial presentation had a median survival of 5.4, 11.7, and 32.9 months, respectively.
Conclusion:
Patients with either a synchronous or latent diagnosis of RCC survived greater than 6 months from the time of presentation. Initial Furhman grade, Tokuhashi score, and MSKCC/Motzer can be useful tools in informing patient-specific prognosis for those with metastatic RCC of the spine.
Keywords
Introduction
Renal cell carcinoma (RCC) is the seventh most common cancer in the United States, 1 and annually, one fifth of new cases of RCC result in death. 2 –5 The heterogeneity of the malignancies arising from the kidney presents particular diagnostic and therapeutic challenges. RCC subtypes differ in their prevalence, aggressiveness, metastatic potential, life expectancy, and therapeutic sensitivities. Clear cell carcinoma is the most common of 8 RCC subtypes, accounting for approximately 70% of all renal tumors. 3,4 Local RCC is treated with cytoreductive nephrectomy with curative intent. Metastatic disease, because of the aforementioned heterogeneity, poses challenges around the appropriate systemic therapy, radiotherapy, and/or surgery treatment. 2,4,5
As many as one third of patients with RCC are diagnosed with metastatic disease at presentation. 2 Even following nephrectomy, 25% of RCC recur locally or as metastatic disease. 3 After metastases to the lungs, osseous metastatic disease is the second most frequent, with the vertebral column being the most common site. 5 Spinal metastasis remains an indicator of poor prognosis; however, some patients with oligometastatic spine disease can have prolonged survival. Furthermore, advances in surgical treatment, systemic therapy, and radiotherapy have improved overall survival and functional status. 2 –6
Emerging therapies, such as multitargeted receptor tyrosine kinase inhibitors, mTOR inhibitors, concurrent VEGF monoclonal antibodies, and interferon-α have have improved survival in these patients. 2,6,7 Moreover, RCC was considered radio-resistant to conventional radiotherapy, 8,9 but the use of stereotactic radiotherapy (stereotactic body radiotherapy [SBRT], stereotactic radiosurgery [SRS]) has shown significant promise in the treatment of pain and local disease control. 10 –13 The significant dilemma for spine surgeons is when to be surgically aggressive, such as en bloc resection of oligo spine metastasis? In long-term survivors the risk benefit ratio would make sense, given the challenges of local recurrence. In limited life expectancy it would not.
Given the advent of newer treatment modalities, the current knowledge of outcomes and prognosis for patients with metastatic RCC to the spine is still insufficient. To address this knowledge gap, this systematic review focuses on 2 key questions: What is the clinical presentation and probability of symptomatic improvement following treatment for patients with RCC of the spine? What is the overall survival of patients diagnosed with spinal metastases from RCC?
Methods
Electronic Literature Search
A systematic review of the literature using CINAHL, Embase, PubMed, and Web of Science databases and review of the bibliographies of eligible articles was performed with searches run on July 29, 2016. The search query was designed to include the RCC patient population with spinal metastases reported in the literature over the past 30 years, since 1986. Additionally, a search specific to prognostic variables for renal cell spinal metastases patients was conducted with emphasis on the duration between diagnosis of primary disease and survival. This was performed to supplement the limited prognostic variables available in the studies reviewed. A summary of the inclusion and exclusion criteria is provided in Supplemental Information 1 and Table 1 (available in the online version of the article).
Inclusion Criteria
Our inclusion criteria included the following: fully published, peer-reviewed, retrospective or prospective studies, including randomized controlled trials, nonrandomized trials, cohort studies, case-control studies, case series, and case reports in the English language or a complete English translation; human patients from age 18 to 85; articles describing patients diagnosed with metastatic RCC to the spine origin and/or with known primary; articles describing interventions (radiation therapy [RT], SBRT, SRS, surgery, vertebroplasty/kyphoplasty/cement-augmentation, chemotherapy, embolization) used to treat spinal metastases in RCC patients; and clinical studies assessing prognostic and therapeutic factors for RCC related to life expectancy or local control. The PRISMA tool was used as applicable to assess the methodological quality of the included studies. 14
Exclusion Criteria
Our criteria for exclusion included articles that did not provide clinical outcomes and statistics specific to patients with spinal metastases from RCC, articles that included outcomes for patients with varying primary tumor types where data for RCC-specific patients was indistinguishable, articles on nonhumans, and review articles.
Data Extraction
Demographic information including age, gender, spinal level treated, radiation use, chemotherapy and/or other adjuvant therapy, presentation of symptoms, histologic tumor grade, and type of clinical study was extracted. Any information on functional status was extracted when possible, such as American Spine Injury Association (ASIA) Impairment Scale, Revised Tokuhashi Score, and Frankel Grade. Based on the available literature, outcomes on pain, neurologic deficit, and survival time were extracted. The Fuhrman Grade, which characterizes nuclear atypia 14 to predict prognosis, was recorded when available. The Memorial Sloan Kettering Cancer Center (MSKCC/Motzer) 15 score combines clinical and laboratory data to calculate a total number of points, which corresponds to median survival. This was also included in the data extraction where available.
Study Eligibility
All potentially eligible studies, meeting the inclusion criteria, were determined by 3 reviewers (AKA, NAB, and CB). All discrepancies were resolved by a fourth reviewer (CRG). Articles that met predetermined criteria for exclusion were not included in the study.
Similar to previous publications, 16,17 the assessment of individual study quality was performed using the following grading system: high, low, or insufficient. “High” was assigned to studies that were Class of Evidence (CoE) I or II, and the true effect could be confidently assumed to be close to the estimated effect. “Low” was assigned to studies that were Class III or IV, and the true effect may have been significantly different from the estimated effect. Case reports were assigned Class V. “Insufficient” was assigned if there was very little confidence in the estimated result, no evidence, or too little evidence to estimate an effect. The quality could be downgraded if the evidence was indirect, results were inconsistent, there were no a priori subgroup analyses, or the effect estimates were imprecise. Conversely, an overall estimation of quality could be upgraded if the magnitude of effect was large.
Statistical Methods
Survival statistics and Kaplan-Meier curves were calculated using GraphPad Prism 5.0 (GraphPad; La Jolla, CA). All cases from the literature were included as applicable. Patient demographics, presentation, treatment, and outcomes were calculated based on the cohort of patients with known status for each variable.
Results
Demographics and Presentation
The literature search identified 1440 unique results, where 47 articles met the inclusion criteria with a total of 807 patients included in the data analysis (Figure 1). 1,10,11,13,15,18 –60 Demographics, presenting features, treatment, and survival information were compiled for those patients with known status. The majority of patients were male (75.5%), and the mean age at diagnosis of RCC spine metastasis was 56.7 years. The most common presenting symptom was pain (79.9%), and a majority of patients had systemic/visceral disease (58.9%) at the time of diagnosis of spine metastasis. The most common location was the thoracic spine (49%), followed by the lumbar spine (34.4%) and the cervical spine (11.6%). Most patients were neurologically nonfocal, presenting with either Frankel Grade E (66%) or ASIA E (89.6%; Table 1). Twenty-three percent of patients had a synchronous diagnosis of RCC with spine metastasis.
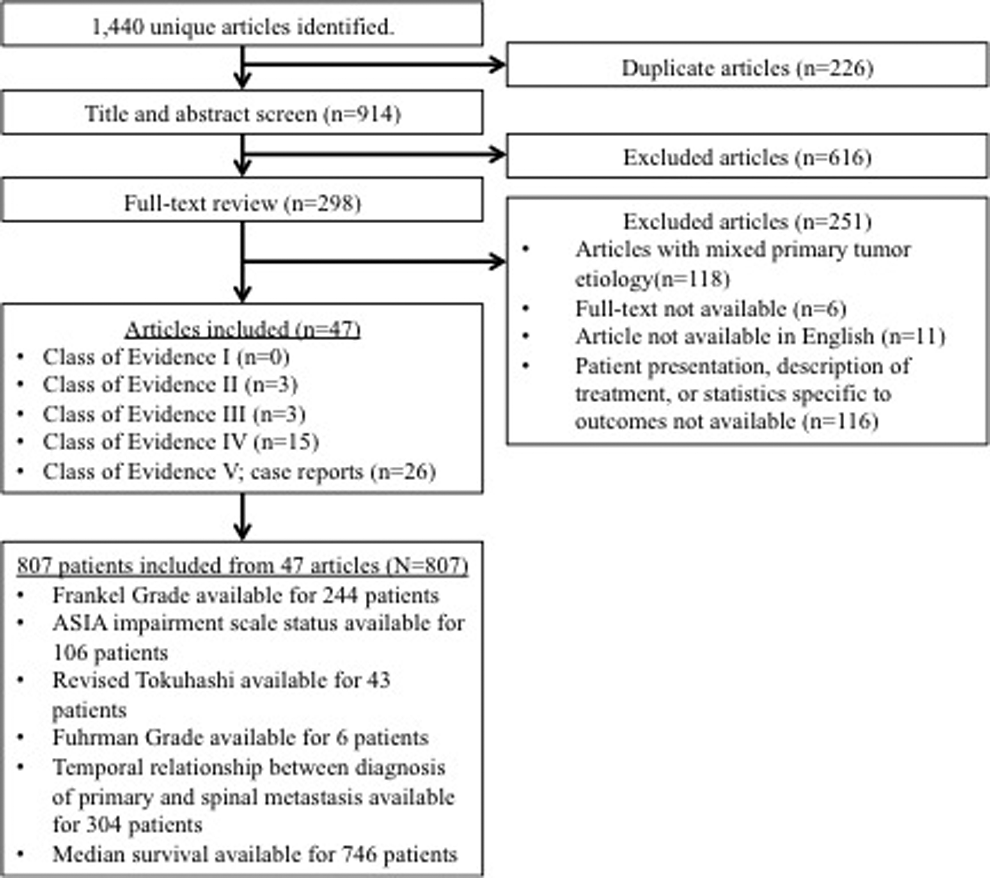
Consolidated standards of reporting trials diagram for article selection.
Selection Criteria for Systematic Review of Metastatic Renal Cell Carcinoma of the Spinea.
aPubMed and Embase searches were limited to humans. No other limitations were placed on any searches. All searches were run on July 29, 2016, yielding a total of 1440 unique results.
Clinical Outcomes
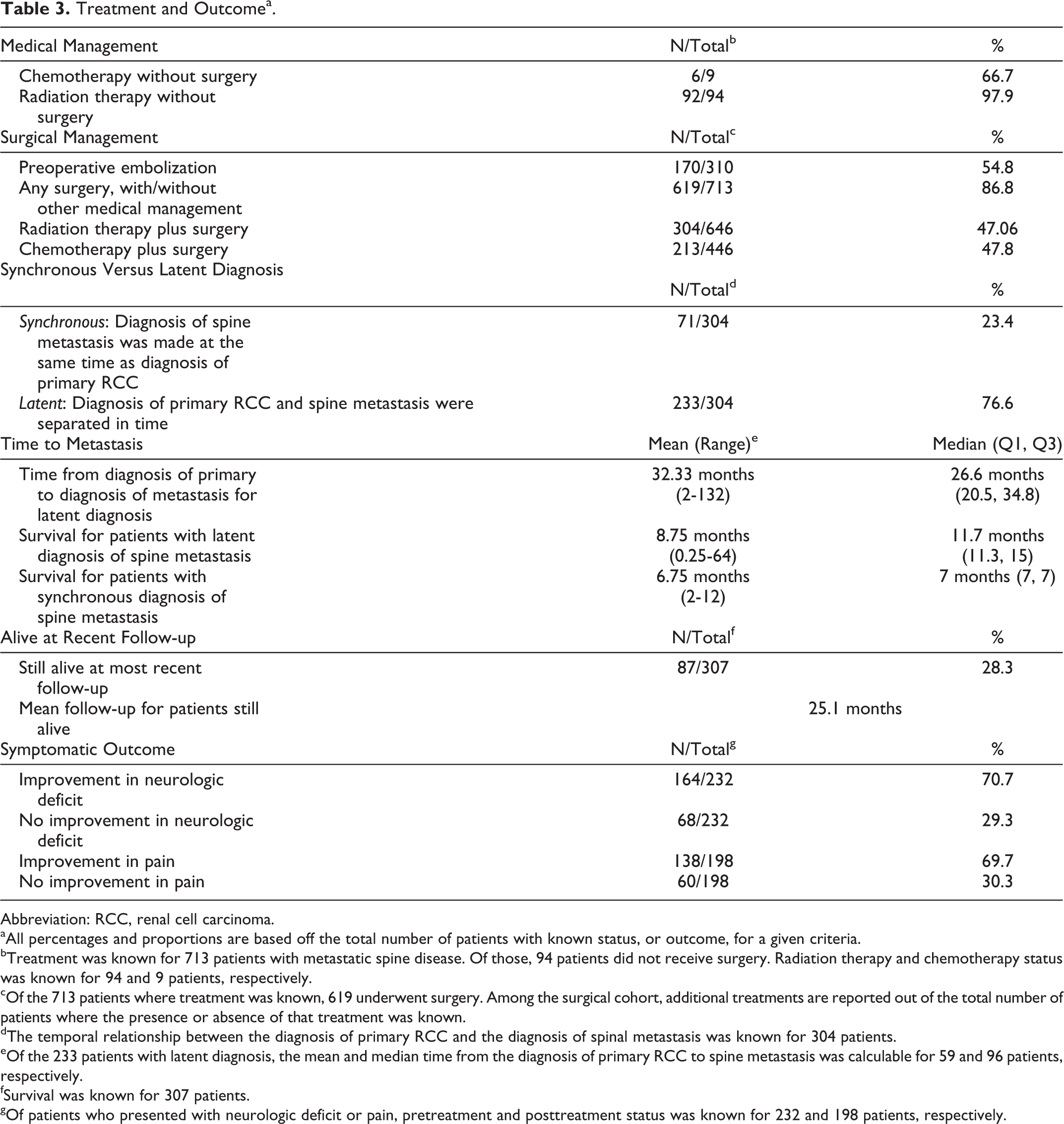
Data regarding treatment status of patients was frequently unavailable, omitted in the literature, or combined with other treatments. Thus, use of treatment modalities could only be analyzed within patient subgroups for whom the data was available. Available data was insufficient to distinguish patients treated with single or combinations of treatment modalities; thus, there is an overlap of patients between the categories, unless otherwise stated. The presence or absence of surgical treatment was known for 713 patients. Ninety-four (13.2%, 94/713) patients did not receive any surgical intervention for metastatic spine disease from RCC. Spinal surgery, whether alone or as part of a combined treatment strategy, was performed in 619 (86.8%, 619/713) patients. For those patients with known treatment, radiation was performed with surgery in 47.1% (304/646) of cases, and chemotherapy was performed with surgery in 47.8% (213/446) of cases. Of the surgical cases where it was known, preoperative embolization occurred in 54.8% (170/310) of surgical cases. Of the 94 nonsurgical cases, 92 (97.9%) underwent some form of radiation (RT/SRS/SBRT), and of the nonsurgical cases with known status, 66.7% (6/9) received chemotherapy/immunotherapy.
The time to metastasis was known for 304 patients. Seventy-one patients (23.4%, 71/304) were diagnosed with spinal metastasis on initial presentation, also known as a “synchronous diagnosis.” The remaining 233 (76.6%, 233/304) of patients were diagnosed with spine metastasis after a period of time where primary RCC had been previously diagnosed, also known as “latent metastasis.” For those with a latent diagnosis, the mean and median time between the diagnosis of primary RCC and spine metastasis was 32.33 and 26.6 months, respectively (N = 307; Table 2). Moreover, the mean and median survival for those with a latent diagnosis of spine metastasis from RCC was 8.75 months (range = 0.25-64) and 11.7 months (Q1, Q3: 11.3, 15), respectively. The mean and median survival for those with a synchronous diagnosis of spine metastasis was 6.75 (2-12) and 7 (7, 7) months (Figure 2).
Patient Demographics and Presentationa.
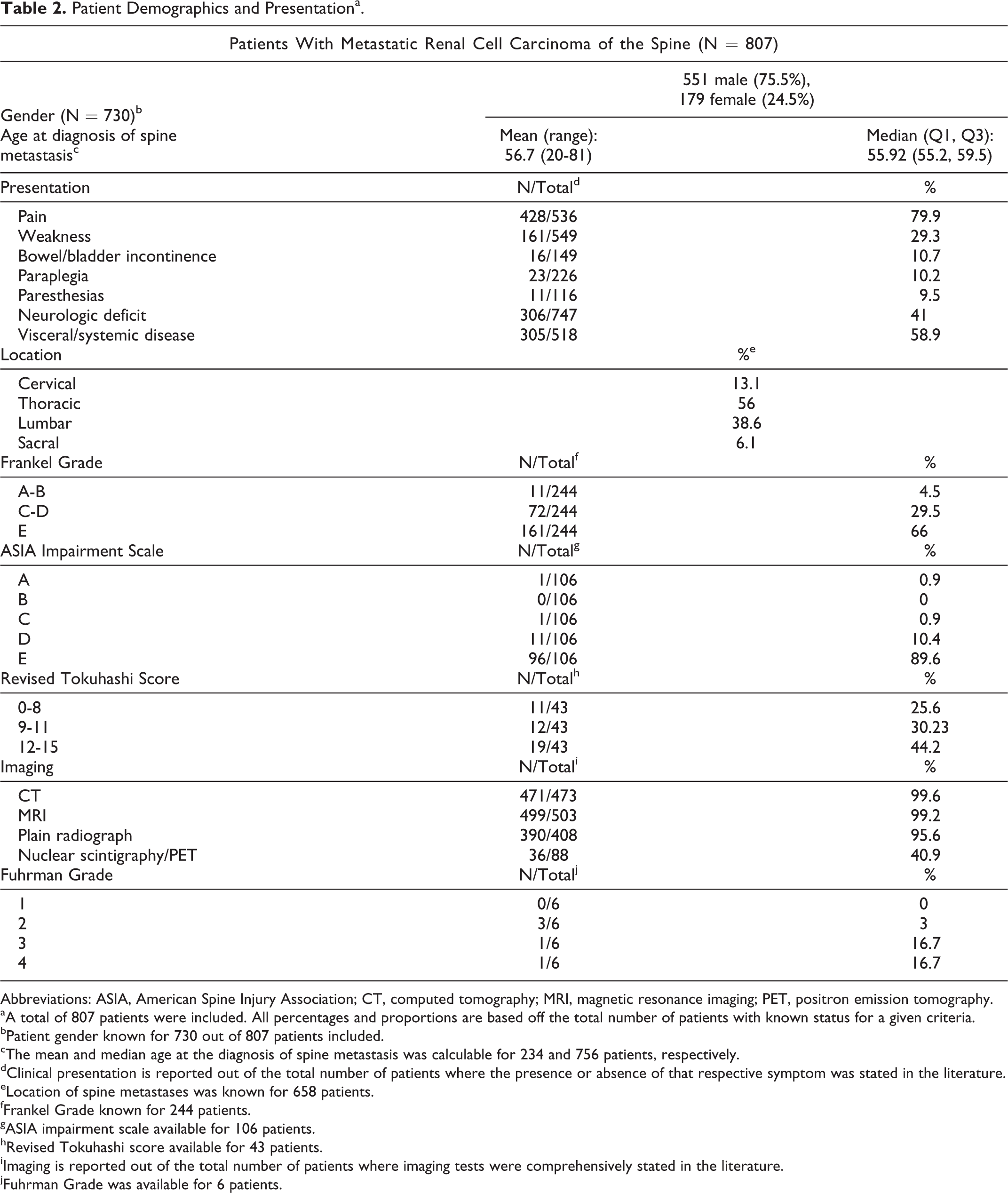
Abbreviations: ASIA, American Spine Injury Association; CT, computed tomography; MRI, magnetic resonance imaging; PET, positron emission tomography.
aA total of 807 patients were included. All percentages and proportions are based off the total number of patients with known status for a given criteria.
bPatient gender known for 730 out of 807 patients included.
cThe mean and median age at the diagnosis of spine metastasis was calculable for 234 and 756 patients, respectively.
dClinical presentation is reported out of the total number of patients where the presence or absence of that respective symptom was stated in the literature.
eLocation of spine metastases was known for 658 patients.
fFrankel Grade known for 244 patients.
gASIA impairment scale available for 106 patients.
hRevised Tokuhashi score available for 43 patients.
iImaging is reported out of the total number of patients where imaging tests were comprehensively stated in the literature.
jFuhrman Grade was available for 6 patients.
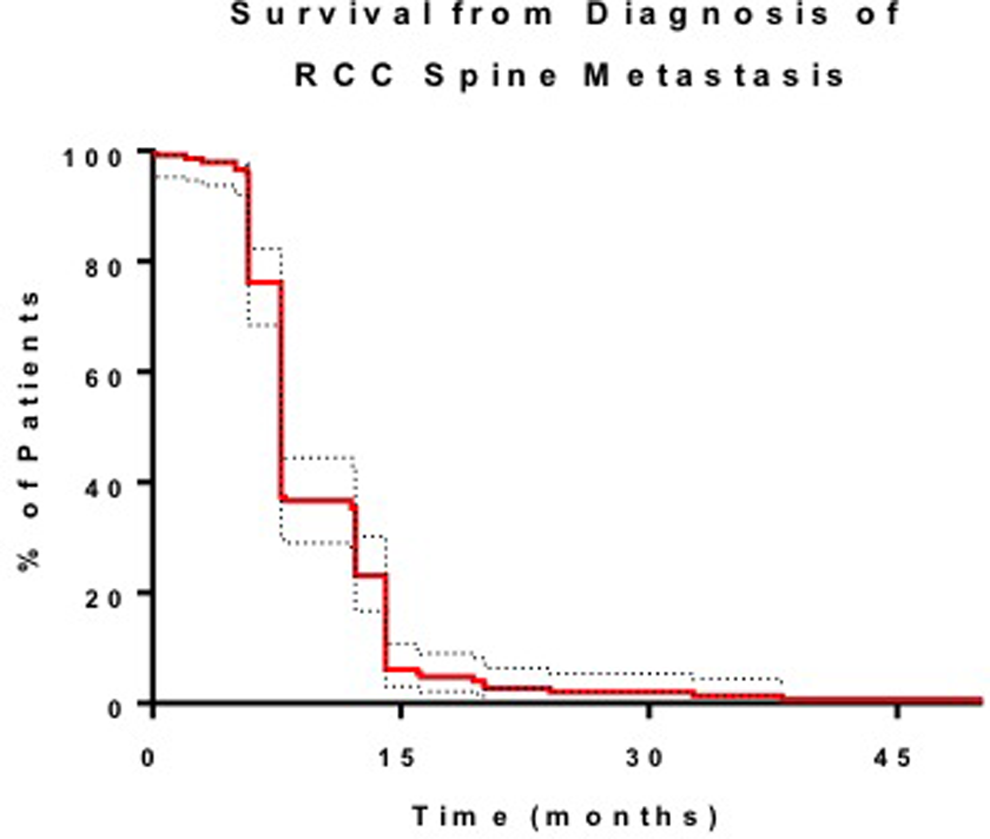
Kaplan-Meier survival curve after diagnosis of RCC spine metastasis. Dotted lines represent confidence intervals.
The mean survival was known for 307 patients. Of those, 87 (28.3%) were still alive at most recent follow-up for a mean follow-up time of 25.1 months. Of patients with preexisting neurologic deficit or pain where posttreatment outcomes were known, 70.7% had improvement in neurologic deficit (N = 232) and 69.7% had improvement in pain (N = 198).
The earliest article included in the calculation of survival was from 1990. 53 Of articles published from 1990 to 1999, the mean and median survival was 5.8 months and 7 months from the time of spinal metastasis, respectively (N = 29 and N = 106). For articles published from 2000 to 2009, the mean and median survival was 8.7 months and 12.3 months, respectively (N = 60 and N = 57). For articles published from 2010 to 2016, the mean and median survival was 15.4 months and 13.5 months, respectively (N = 218 and N = 563). Of note, the mean survival from diagnosis of spinal metastases was statistically significant between each decade assessed (P < .05).
Factors Associated With Survival
Due largely to the limited sample sizes available where these factors were reported in the literature, patient presenting factors, symptoms, location of spinal lesion, Frankel Grade, ASIA Impairment Scale, and Fuhrman Grade were not significantly associated with survival. The Furman Grade and MSKCC score are important clinical factors in treating patients with metastatic RCC but were underpowered in the current study to find significance with regards to prognosis.
Patients with a “low” revised Tokuhashi Score (0-8) at presentation and known survival were alive for a mean of 1.63 months and a median of 5.4 months from the time of diagnosis of spine metastasis. Patients with an “intermediate” revised Tokuhashi Score (9-11) lived for a mean of 13.27 months and a median of 11.7 months, and patients with a “high” revised Tokuhashi Score (12-15) survived for a mean of 32.67 months and a median of 32.9 months. Patients that did not receive surgery had a mean and median survival of 8.33 and 3 months, respectively. Patients that received surgery had a mean and median survival of 16.2 and 14.1 months, respectively. Of those that received surgery, patients who received preoperative embolization had a mean and median survival of 15.6 and 14.1 months, respectively (Tables 3 and 4). Due to the limited number of patients in the groups where treatment and survival were known, the prognostic factors did not achieve statistical significance from one another.
Treatment and Outcomea.
Abbreviation: RCC, renal cell carcinoma.
aAll percentages and proportions are based off the total number of patients with known status, or outcome, for a given criteria.
bTreatment was known for 713 patients with metastatic spine disease. Of those, 94 patients did not receive surgery. Radiation therapy and chemotherapy status was known for 94 and 9 patients, respectively.
cOf the 713 patients where treatment was known, 619 underwent surgery. Among the surgical cohort, additional treatments are reported out of the total number of patients where the presence or absence of that treatment was known.
dThe temporal relationship between the diagnosis of primary RCC and the diagnosis of spinal metastasis was known for 304 patients.
eOf the 233 patients with latent diagnosis, the mean and median time from the diagnosis of primary RCC to spine metastasis was calculable for 59 and 96 patients, respectively.
fSurvival was known for 307 patients.
gOf patients who presented with neurologic deficit or pain, pretreatment and posttreatment status was known for 232 and 198 patients, respectively.
Factors Affecting Survival.
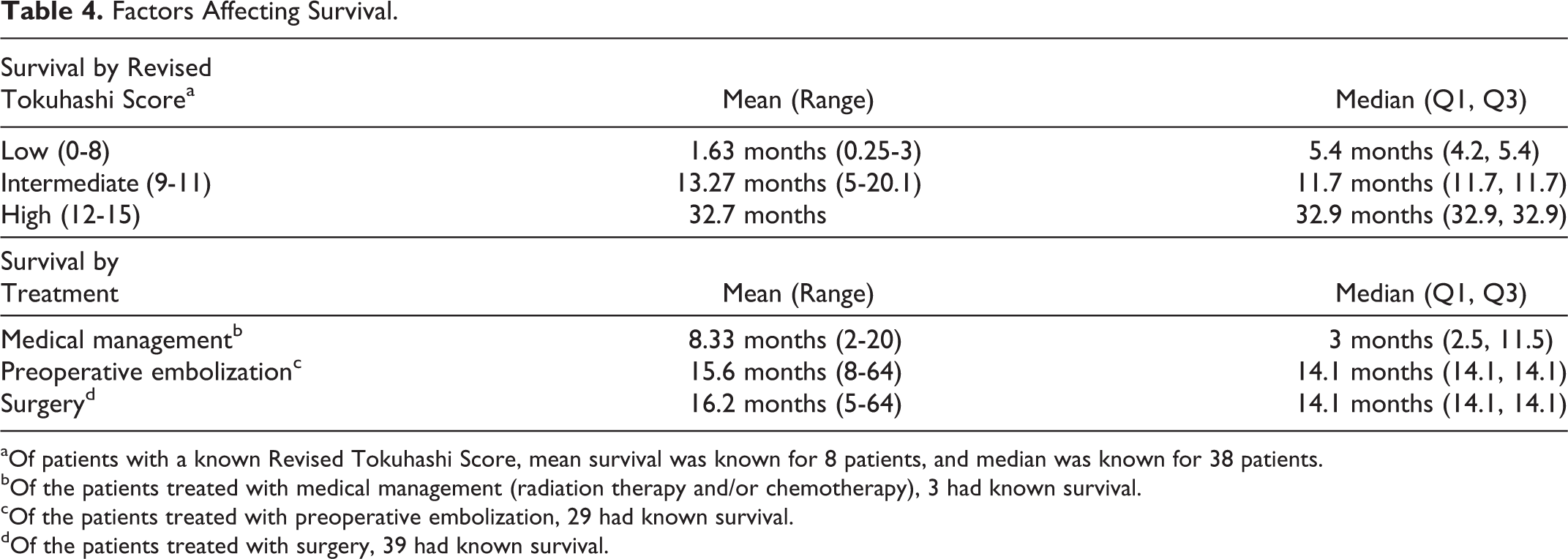
aOf patients with a known Revised Tokuhashi Score, mean survival was known for 8 patients, and median was known for 38 patients.
bOf the patients treated with medical management (radiation therapy and/or chemotherapy), 3 had known survival.
cOf the patients treated with preoperative embolization, 29 had known survival.
dOf the patients treated with surgery, 39 had known survival.
Study Quality and Overall Strength of Literature
All 47 studies were case reports, case series, or cohort: 26 were case reports of Class V, 15 were Class IV, 3 were Class III, and 3 were Class II. The majority of patients included were from articles of Class III or IV. Class V studies made up 3.22% of the patient population (26/807). Based on the CoE and the quality and consistency of data, the overall strength of findings is “low” to “insufficient.”
As described by Wan et al, 58 combining ordinal data is a limitation in many systematic reviews. To avoid this error, only mean values with known standard deviation was performed and medians were pooled and compared independently in a parametric distribution for studies where either (1) mean, sample size, and standard deviation or (2) median, first interquartile, and third interquartile were known values.
Discussion
RCC is an aggressive malignancy that frequently metastasizes, exhibiting a predilection for the bony spine. With the advent of targeted chemotherapies, precise radiotherapy, and newer surgical approaches, better outcomes can be achieved. Despite these advances in patient care, there is inadequate information on prognosis and survival for patients with RCC of the spine. We conducted a systematic review of the literature and analyzed available data from 807 patients with metastatic spine disease from RCC—treated from 1986 to 2016—the largest sample size to date. Key outcomes were those that relate to life span and quality of life, including overall survival and symptom relief (pain and neurologic). 1. What is the clinical presentation and probability of symptomatic improvement following treatment for patients with RCC of the spine?
Consistent with metastatic spine disease of other primary tumor types, pain was the most common presenting symptom, followed by neurologic deficit. In this review, 69.7% and 70.7% of patients presenting with pain or neurologic deficit had improvement following treatment, respectively. Although pain or neurologic deficit did not affect survival in the current analysis, Sellin et al 51 presented a retrospective review of 37 patients with metastatic RCC to the spine, wherein the median survival for patients presenting with neurologic deficit was 7.4 months and those presenting without neurologic deficit was 32 months. All patients were treated with SRS, and 5 went on to receive surgery. Tatsui et al 55 demonstrated a similar result, out of 267 patients surgically treated for spinal RCC, where the median survival for those patients presenting with neurologic deficit was 5.9 months, compared to 13.5 months for those presenting without neurologic deficit.
2. What is the overall survival of patients diagnosed with spinal metastases from RCC?
In the current review, the mean and median survival for patients with a “synchronous” diagnosis (spine metastasis and primary tumor site diagnosed at the same time) was 6.75 and 7 months, respectively, whereas for patients with a latent diagnosis (previous diagnosis of primary RCC prior to spine metastasis), the mean and median survival was 8.75 and 11.7 months, respectively. As the armamentarium of multitargeted receptor tyrosine kinase inhibitors, immunotherapeutic agents, and other therapies continue to improve, and the ability to diagnose and molecularly classify affected patients to provide more personalized treatments is realized, it is expected that these survival times will improve and potentially alter the role each treatment modality plays in the management of metastatic RCC to the spine. 2,6 Unfortunately, given the paucity of data on prognostic factors associated with distinct treatment modalities for RCC spinal metastases, it is difficult to assess whether specific factors are associated with increased overall survival than other groups.
In the literature, many of the large studies present cohorts of patients treated with a combination of radiation, chemotherapy, and surgery. Moreover, survival is often presented in medians where the systematic review of multiple cohorts is not feasible. As such, it was not possible to yield meaningful data on the effect of individual treatment modalities for survival. The mean survival for patients receiving medical treatment, surgical treatment, and surgical treatment with embolization was 8.3, 16.2, and 15.6 months, respectively. The survival difference was not significant between treatment groups, due to the small sample size of the groups where survival was known and where treatment methods did not overlap. Therefore, we summarize the results of a few key clinical studies by treatment modality. Sohn et al 13 published 26 patients—13 treated with SRS and 13 treated with RT. The median survival for patients treated with SRS was 15 months, compared with 7 months for those treated with RT. In a series by Sundaresan et al 54 of 43 patients, 32 patients treated with surgery had a median survival of 13 months, compared with 3 months for the 11 patients treated with RT alone. In the largest known series by Tatsui et al, 55 all 267 patients received surgery, with 108 receiving immunotherapy/chemotherapy, and 99 receiving RT prior to surgery. The median overall survival was 11.3 months. In the series of 37 patients by Thibault et al, 57 all patients received SBRT, with an indiscernible number undergoing surgery prior to SBRT and following SBRT. The median overall survival in this series was 26.6 months.
Histologic grade can play a key role in the prognosis of a metastatic spine lesion. The presenting Fuhrman Nuclear Grade was available for 6 patients, none of whom had known survival. However, Tatsui et al 55 demonstrated Fuhrman Grade as an independent predictor for prognosis in metastatic RCC of the spine. Of 267 patients, those who presented with spinal RCC that was Grade 3 or lower had a median survival of 14.3 months, compared with Grade 4 RCC that had a median survival of 6.1 months, regardless of other factors or treatments.
Predictive analytics and prognostic factor analysis is becoming a mainstay of spinal oncology. One of the most widely used prognostic factors is Tokuhashi Score, where a higher score is predictive of a favorable prognosis. Of the 8 patients where Tokuhashi Score and survival was known, those with a “low” score (0-8) had a mean survival of 1.63 months, those with an “intermediate” score (9-11) had a mean survival of 13.27 months, and those with a “high” score (12-15) had a mean survival of 32.7 months. This is comparable to the series by Petteys et al, 44 where 30 patients were surgically treated for spinal RCC. Of the 30, 15 patients with a “high” score (12-15) had a median survival of 32.9 months, the 7 patients with an “intermediate” score had a median survival of 11.7 months, and 8 patients with a “low” (0-8) score had a median survival of 5.4 months. The MSKCC/Motzer Score for Metastatic Renal Cell Carcinoma is a similar form of predictive analytics, which takes into consideration the time from diagnosis to systemic treatment, hemoglobin, calcium, lactate dehydrogenase, and Karnofsky Performance Scale score. In a series by Bakker et al, 15 where 21 patients were surgically treated for spinal RCC, those with a “favorable risk” had a median survival of 25 months, those with an “intermediate risk” had a median survival of 6 months, and those with a “poor risk” had a median survival of 2 months.
Time to diagnosis, presenting symptoms, treatment modality, and prognostic scores all play an essential role in predicting survival and outcome for patients with metastatic RCC of the spine. Although the current review does not achieve statistical significance regarding several factors, limiting the conclusions that may be drawn, it is the largest known systematic review of RCC of the spine and may prove useful in guiding treatment decisions, compiling the major literature in this field, and informing expected outcomes. Despite the large number of patients and articles encompassed in this review, there are several limitations. Data from major articles that are provided in median amounts limits the analysis of larger cohorts and systematic reviews. Given the heterogeneity of reported outcomes in metastatic RCC, future clinical studies would benefit by reporting the mean, median, standard deviation, range, Q1 and Q3 of a cohort. It would also be preferable to report the number of patients, spinal location, and the total amount of affected spinal levels in the cohort. There are also limitations that are inherent to systematic reviews, including publication bias, consisting of articles with varying numbers of subjects and CoE.
Conclusion
The mean and median time to spine metastasis for patients previously diagnosed with RCC is 32.33 and 26.6 months, respectively. Of patients previously diagnosed with RCC, the mean and median survival is 8.75 and 11.7 months, respectively, from the time of diagnosis of spine metastasis. For patients who initially present with metastatic spine disease from RCC, the mean and median survival is 6.75 and 7 months, respectively, from the time of presentation. For articles published from 2010 to 2016, the mean and median survival was 15.4 months and 13.5 months, respectively (N = 218 and N = 563). In this review, presenting factors, patient characteristics, and treatment modalities were not associated with better or worse outcomes. However, initial Furhman Grade, Tokuhashi Score, and MSKCC/Motzer Score for Metastatic Renal Cell Carcinoma as well as more contemporary predictive analytics may more accurately inform patient-specific prognosis for those with metastatic RCC of the spine.
Supplemental Material
Supplemental Material, RCC_Supp_tables - The Challenges of Renal Cell Carcinoma Metastatic to the Spine: A Systematic Review of Survival and Treatment
Supplemental Material, RCC_Supp_tables for The Challenges of Renal Cell Carcinoma Metastatic to the Spine: A Systematic Review of Survival and Treatment by C. Rory Goodwin, A. Karim Ahmed, Christine Boone, Nancy Abu-Bonsrah, Risheng Xu, Niccole Germscheid, Daryl R. Fourney, Michelle Clarke, Ilya Laufer, Charles G. Fisher, Chetan Bettegowda, and Daniel M. Sciubba in Global Spine Journal
Footnotes
Acknowledgments
Carrie Price, MLS, for technical assistance with search criteria. This work received support from the AOSpine Knowledge Forum Tumor. AOSpine is a clinical division of the AO Foundation—an independent medically guided nonprofit organization. The AOSpine Knowledge Forums are pathology-focused working groups acting on behalf of AOSpine in their domain of scientific expertise. Each forum consists of a steering committee of up to 10 international spine experts who meet on a regular basis to discuss research, assess the best evidence for current practices, and formulate clinical studies to advance spine care worldwide. Study support is provided directly through AOSpine’s Research department.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C. Rory Goodwin: UNCF Merck Postdoctoral Fellow and has received an award from the Burroughs Wellcome Fund and the Johns Hopkins Neurosurgery Pain Research Institute. A. Karim Ahmed: has received an award from the NREF Medical Student Summer Research Fellowship. Ilya Laufer: Globus, SpineWave, Depuy/Synthes, Medtronic, BrainLab. Charles G. Fisher: Royalties from Medtronic, consulting for Medtronic and Nuvasive, and research support from OREF, AOSpine, and Medtronic. Daniel M. Sciubba: consultant for Medtronic, Globus, DePuy, and Stryker. The remaining authors have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.