
Abstract
Study Design:
Systematic review of literature.
Objectives:
This systematic review was conducted to investigate the accuracy of radiostereometric analysis (RSA), its assessment of spinal motion and disorders, and to investigate the limitations of this technique in spine assessment.
Methods:
Systematic review in all current literature to invesigate the role of RSA in spine.
Results:
The results of this review concluded that RSA is a very powerful tool to detect small changes between 2 rigid bodies such as a vertebral segment. The technique is described for animal and human studies for cervical and lumbar spine and can be used to analyze range of motion, inducible displacement, and fusion of segments. However, there are a few disadvantages with the technique; RSA percutaneous procedure needs to be performed to implant the markers (and cannot be used preoperatively), one needs a specific knowledge to handle data and interpret the results, and is relatively time consuming and expensive.
Conclusions:
RSA should be looked at as a very powerful research instrument and there are many questions suitable for RSA studies.
Introduction
Radiostereometric analysis (RSA) is an accurate radiographic technique of measuring 3-dimensional (3D) movements between 2 bodies in vivo. 1 –10
The principle of RSA is that when radio-opaque markers are inserted in the skeleton in 2 different bodies with the use of stereography and specialized computer software, the 3D position and any relative change in relation between these labelled bodies can be detected. 11 The relative change in distance between the markers reflects the relative movement between the 2 different marked bodies. 12 RSA was first developed by Goran Selvik, a Swedish mathematician in 1972 in Lund, Sweden. RSA remained in the laboratories as a research tool for many years before entering into the clinical study mainly in orthopedics and trauma. Spinal motion assessment was the first clinical application of RSA. 11 Joint arthroplasty is one of the main fields where RSA is established as the main method of assessment of implant migration and loosening. 13,14 Fracture, osteotomies, and knee joint assessment are the other RSA applications in orthopedics and trauma. 15 –19
Spinal fusion, scoliosis surgery, spondylolisthesis treatment, and intervertebral disc arthroplasty are the main spinal conditions where RSA is used. Hindmarsh reported the first scoliosis treatment assessment by RSA in 1973, followed by Olsson and colleagues reporting, in 1976, the first analysis of lumbosacral spine fusion studied with RSA. 11,20
This systematic review was conducted to investigate the accuracy of RSA, its assessment of spinal motion and disorders, and to investigate the cause of why RSA still not commonly used in the clinical assessment of spine after about 30 years since its first use in spine.
Materials and Methods
To establish the evidence that supports the use of RSA in the assessment of spinal motion, we conducted a systemic search in the literature. The literatures were reviewed by searching through the most common available databases: PubMed (to December 2015) Medline (1966 to December 2015) Embase (1980 to December 2015) Cochrane database (to December 2015)
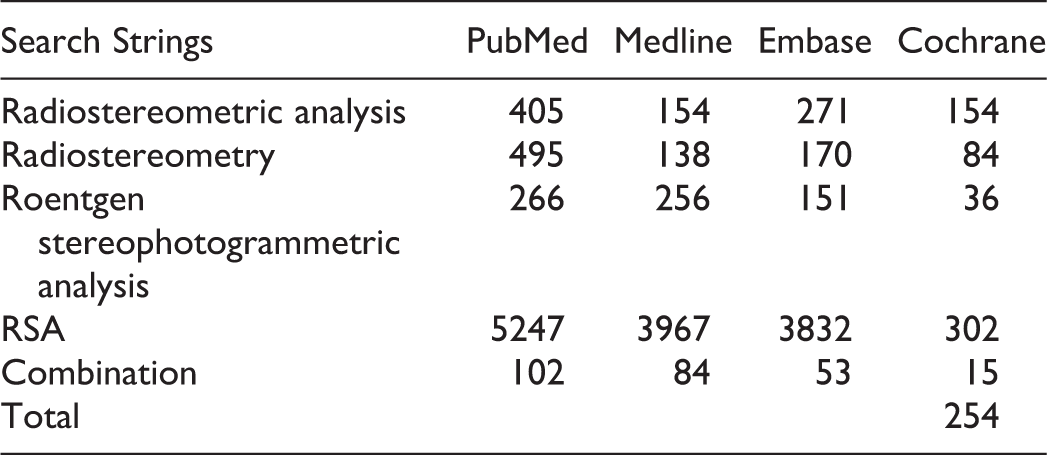
The search strings were the same in all databases (“radiostereometric analysis,” “radiostereometry,” “roentgen stereophotogrammetric analysis,” “RSA”) and are shown in the following table.
Results
The total number of articles in the combined searches was 254. PubMed combined search resulted in 102 references, which was the highest number, while Medline, Embase, and Cochrane gave 84, 53, and 13, respectively.
The inclusion criteria were the following: Published article in which spinal motion was assessed by RSA Clear documentation of the accuracy of RSA An article in English
The exclusion criteria were the following: Nonspinal RSA study No clear documentation about the accuracy of RSA Not an article in English Review papers
A total of 213 references were excluded because they were irrelevant or not fitting the inclusion criteria. The remaining 41 studies were included in this review study (Table 1).
Summary of All the Studies Included in This Review.
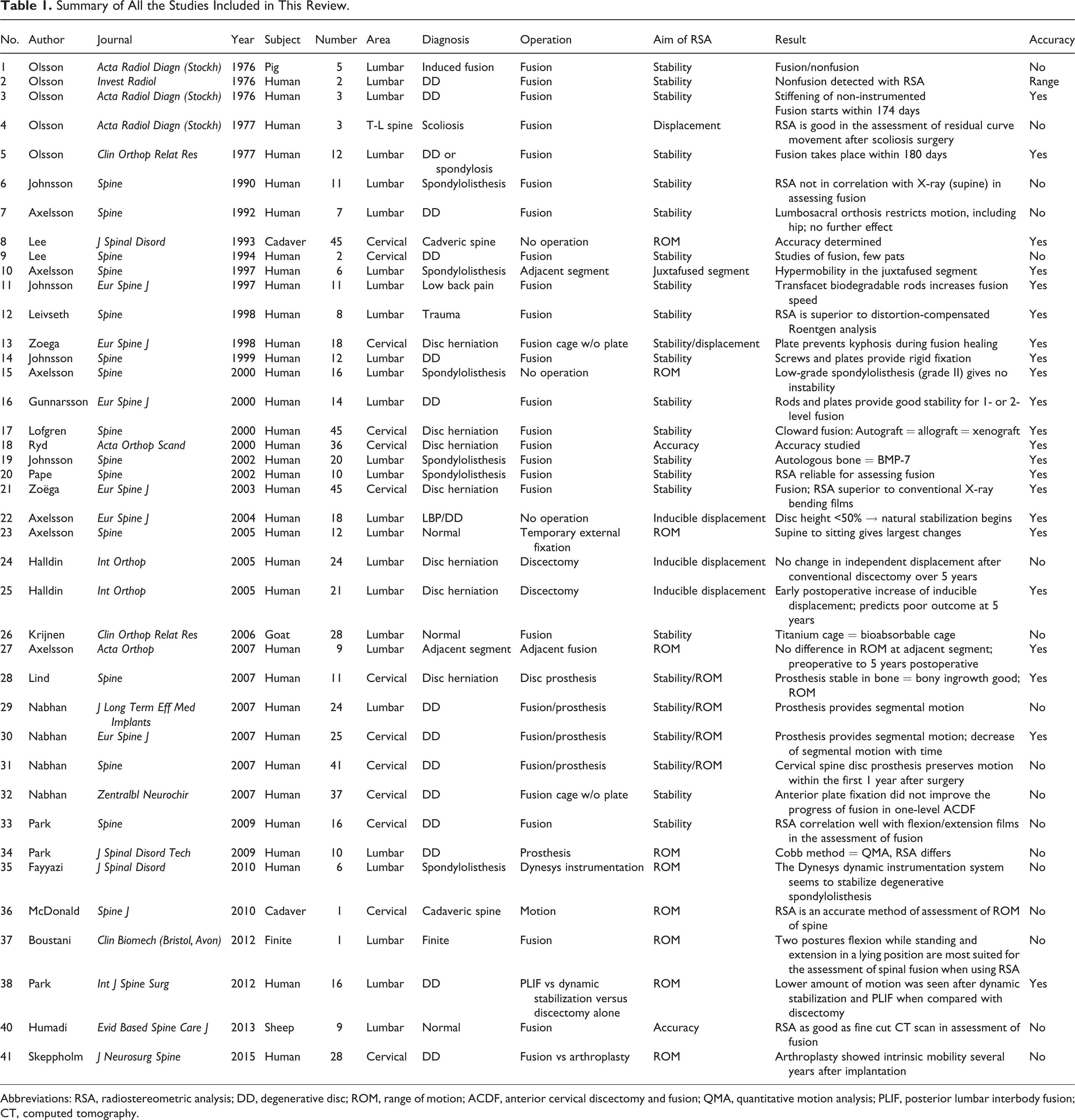
Abbreviations: RSA, radiostereometric analysis; DD, degenerative disc; ROM, range of motion; ACDF, anterior cervical discectomy and fusion; QMA, quantitative motion analysis; PLIF, posterior lumbar interbody fusion; CT, computed tomography.
The Precision and Accuracy of RSA in the Reviewed Articles
The accuracy of RSA varies in the literatures and it depends on several factors. The accuracy is the closeness of the measurements obtained to the actual movement. 44 The stability and security of beads fixation, the number of the beads inserted, and the distribution of the beads in each rigid body are the most important factors in determining the precision of the RSA setup and assessment (Figure 1). 29,45 The accuracy can be adversely affected by the instability of the beads in the rigid body. 44 This can be improved by using a very tight hole in the bone and avoiding oversized drilling, which keeps the beads loose or by delaying the assessment for 14 days, especially in metabolically active bone (children) to allow for initial instability to settle. 45 The alternative way to improve the instability is by using glue materials such as bone wax to provide temporary stabilization. The higher the number and the wider the distribution of the beads, the better the accuracy of the RSA assessment. 11,45 The precision of RSA is the closeness of the measurements obtained from repeated examination to that of the first examination usually measured by testing and retesting of all of the sample of patients and defined as the standard deviation from the repeated measurements. 32,33,45,46
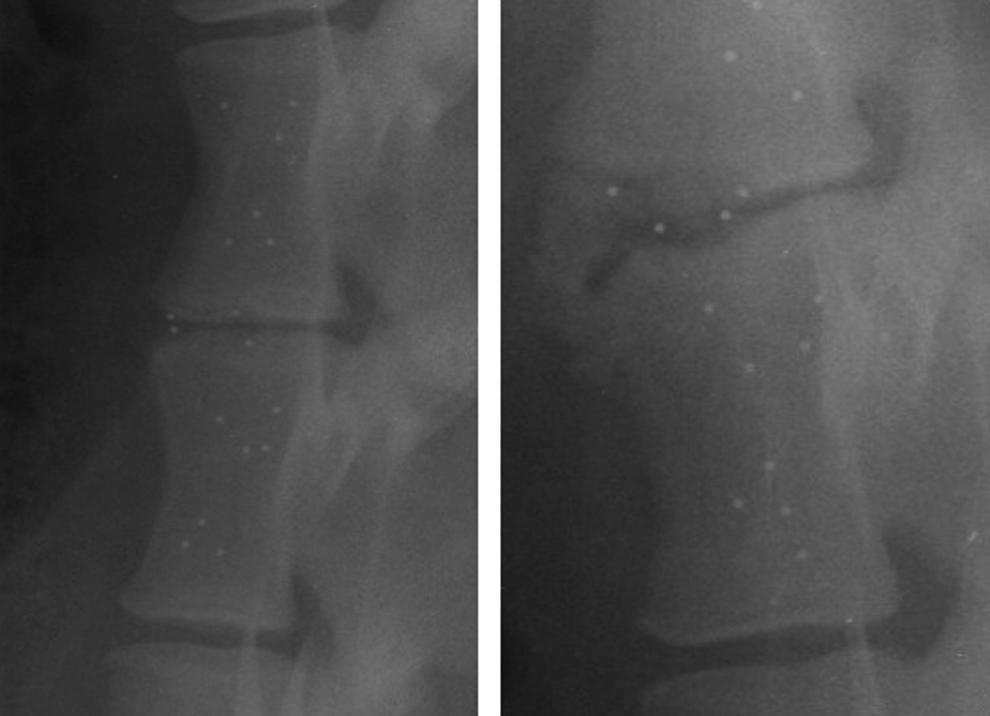
X-rays of lumbar spine in sheep showing the widely distributed RSA beads.
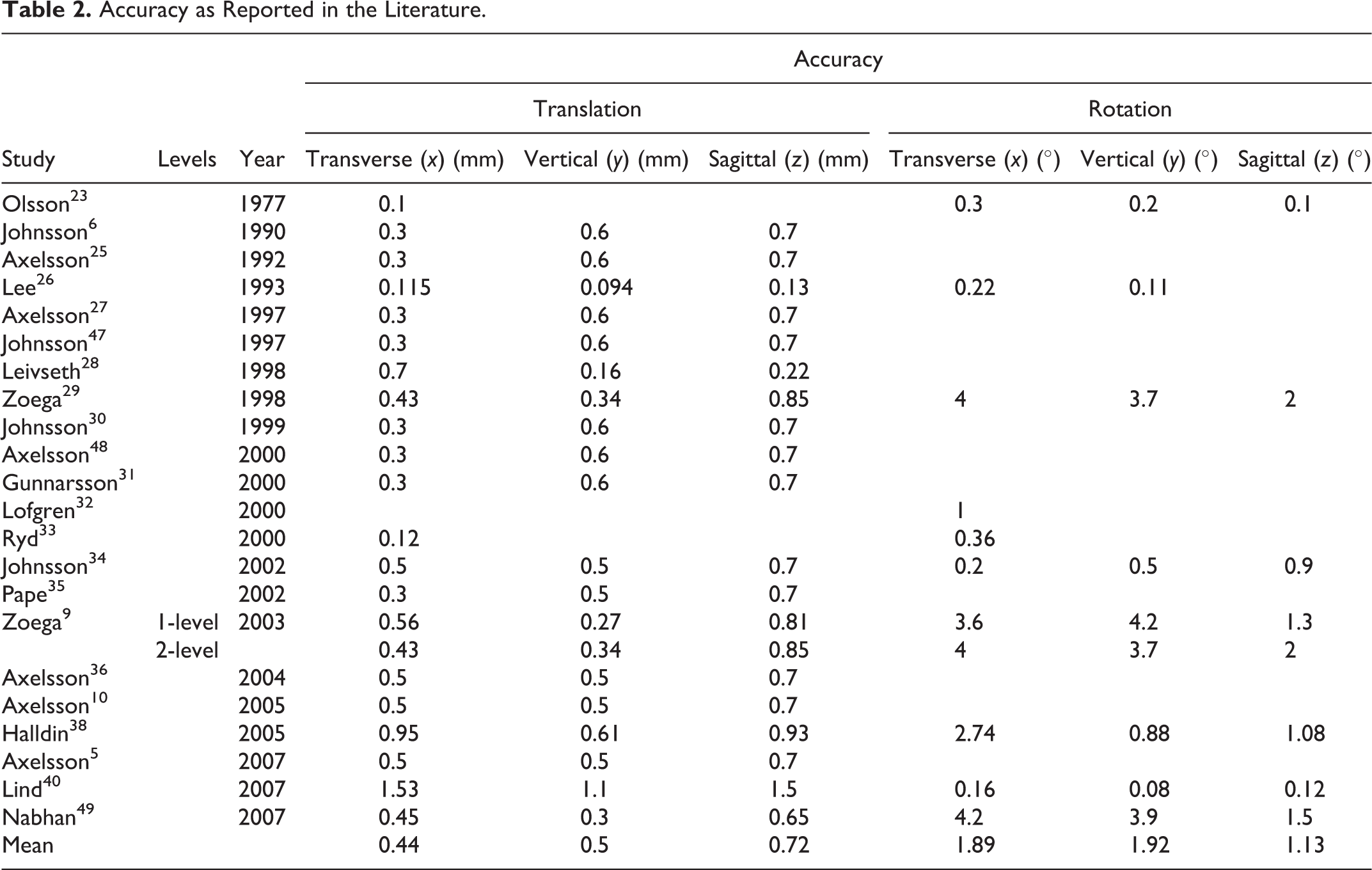
The accuracy is often expressed as a value and any movement above this value is considered significant. A movement below this value is considered insignificant as it is within the RSA setup error range. Table 2 shows summary of the reported precision figures of the RSA setup in the reviewed articles. Articles with unclear documentations of the accuracy and precision or using range of accuracy were excluded from this table. The mean translational accuracy in millimeters was (0.44, 0.5, 0.72) in the (x, y, and z axes), respectively, and rotational accuracy in degrees was (1.89, 1.92, and 1.13) in the (x, y, and z axes), respectively. This may suggest that we should aim for accuracy figures close to these values.
Accuracy as Reported in the Literature.
Application of RSA and Analysis of Reviewed Papers
RSA has been used for studying of (1) inducible displacement of vertebral segments and (2) spinal deformation over time. Inducible displacement should be understood as the positional difference between 2 vertebral bodies resulting from positional changes, such as supine to standing and also flexion/extension. These changes are ultimately described in translations and rotations in 3 dimensions. Areas studied are degenerative changes, 36 –38 spondylolisthesis, 27,34,35,48,50 pseudarthrosis, 22 fusion healing, 20 –23,28 –33,39,47,51 and disc replacement. 39 –43,49,52 Spinal deformation is the changes in segmental position over time, such as a segment that collapses into kyphosis during fusion healing 29 and scoliosis. 24 To fully study the fusion process, repeated provocations are needed (inducible displacement), which allows studies of both mobility (provocation) and deformation (comparison of repeated examinations).
Inducible Displacement
Cervical Spine
Lee et al performed a pioneering work in the cervical spine in a cadaveric setup in 1993. 26
In a study conducted by Nabhan et al, RSA was used to compare cervical disc arthroplasty and fusion. 49 Although the clinical outcome of both groups was the same, there was significant loss of intervertebral motion in the fusion group compared with disc replacement when looked at 3, 6, 12, and 24 weeks after surgery. However, the segmental motion decreased gradually in both groups over time, and further follow-up is recommended to verify the long-term outcome of this study.
Lumbar Spine
In the lumbar area, inducible displacement measured with RSA has been used to study the effect of lumbosacral orthosis, 25 stability in low-grade spondylolisthesis, 48 after discectomy, 37,38 in different stages of degenerative disc disease, 36 and motion over disc replacement segments. 40,42,49
In 1992, Axelsson et al found that lumbosacral orthosis inhibits trunk mobility rather than lumbar mobility. 25 Extension to the hip did not add further stability. In a later study, Axelsson et al could rule out instability in low-grade L5/S1 isthmic spondylolisthesis compared to radiologically normal segments. 48
In 2004, Axelsson et al used RSA to study the stages of progressive degenerative process in the lumbar spine. 36 The authors assessed the intervertebral mobility for the 2 most-distal lumbar disc levels in 18 adult patients with low back pain, different stages of radiological disc degeneration, and no prior spinal surgery. RSA was used to measure the relative inducible displacement through the disc segments by changing position from supine to sitting. They concluded that the inducible displacement through the studied discs changes throughout the degenerative process and the stage of natural stabilization begins when disc height is reduced by 50%. The same authors studied inducible displacement over segments adjacent to lumbar fusion and found no difference preoperatively compared to 5 years later. 5
The effect of lumbar discectomy on intervertebral motion over a period of 5 years was studied by Halldin et al. 38 Twenty-four patients with lumbar disc prolapse were treated by lumbar discectomy at the L4-L5 or L5-S1 level. The treated level was compared with the corresponding untreated level, which means that patients who had discectomy at L5-S1 were used as control for patients who had a discectomy at L4-L5 and vice versa. At the L4-L5 level they found no significant difference between the operated and control levels at discharge or 5 years postoperatively, whereas there at the L5-S1 level there was a statistically significant motion reduction in the sagittal plane compared to the controls. Furthermore, 21 L4-5 or L5-S1 discectomy patients were studied in a prospective cohort study. 37 RSA was done postoperatively and 5 years after surgery. The results suggested that increased vertebral displacement in the early postoperative phase after discectomy is associated with a high risk of recurrence of back pain in the future.
Nabhan et al conducted a prospective study using RSA to compare lumbar spine disc replacement versus fusion for single-level degenerative disc disease. 41 They divided the patients into 2 groups, 13 patients who underwent disc replacement and 11 patients who had fusion procedures. They followed-up their patients with serial RSAs up to 12 months after surgery and found significant segmental motion in the disc replacement group in comparison to the lumbar fusion group.
RSA has been found to be very accurate and enables assessment of range of motion (ROM) in 3 dimensions both in terms of translation (AP and lateral directions) and rotations (around the x, y, and z axes). 5,8,10,26,27,48 This particular advantage of RSA over other radiological tools made RSA the preferred method of assessment of ROM of disc arthroplasty. 8,40 –42,49
Spinal Deformation
Scoliosis
Olsson et al studied spinal correction of scoliosis prospectively as early as 1977. They presented data on deformation of the residual curve up to 1 year postoperatively. 24
Cervical Spine
The first RSA randomized controlled trial on cervical spine by Zoega et al was a comparison of anterior cervical discectomy and fusion (ACDF) techniques where plate fixation added to crest graft prevented kyphosing during healing, which, however, did not affect the postoperative outcome. 29 Lofgren et al found similar fusion rates for ACDF regardless of the use of allograft, autograft, or xenograft. 32
Lumbar Fusion
Assessment of lumbar fusion healing was the first and is the most common topic for RSA in spine. RSA has the advantage of being dynamic and accurate. The disadvantage and limitations of other radiological methods like dynamic flexion extension plain X-ray films and computed tomography (CT) scan pushed researchers and surgeon to use RSA. Dynamic plain X-ray films are the most common method used in most clinical practice. There are several studies that showed this method as nonaccurate and that there is significant interobserver error. 9,53,54 CT scan has the disadvantage of being nondynamic and the risk of exposing the body to high X-ray radiation doses, which subsequently increase the risk of malignancies. 55 –61 Leivseth et al compared RSA to distortion compensation roentgen analysis (DCRA) in monitoring spinal motion. The authors found DCRA is inferior to RSA, with a higher measurement error. They describe 1° and 1 mm as limitation for DCRA to detect. If higher precision is important, as in spinal fusion assessment, RSA is recommended. In addition, RSA measures rotation and translation in 3 dimensions, while DCRA just measures rotation around the transverse axis and translation in the sagittal plane. 28,62 –64
Although there are many published studies about the clinical application of RSA in spinal surgery, there are several limitations to this investigation tool.
The main reason why RSA cannot be used in high numbers is because it consumes too much time and resources and demands an operation expertise and specific knowledge that is possessed only by a few people. It means that it needs to be performed at the university level with special facilities and economical resources for research. Quantitative motion analysis (QMA) and quantitative fluoroscopy (QF) are other techniques that use computer technology to assess the ROM across segments of the spine. 65 This technique is used more frequently in spine clinical and research practice compare to RSA. The accuracy of QF may not be the same as RSA, but the practicality and the noninvasiveness of this technique makes its future promising when compared with RSA. 66
There is no universally accepted figure (degree of rotation or millimeter of translation) below which the tested segment is considered fused and above which it is considered nonfused. Most of the studies considered any movement above the precision figure as significant because it is above the error limit of this tool. It is not clear whether there are still some movements across successfully fused discs due to the plasticity of the fusion mass, especially in the early stages of fusion. If we consider that there is no movement across successful fusion then any movement above the error limit of the RSA setup is consistent with pseudarthosis. For all of this RSA needs to be validated by the use of an animal model, which allows the comparison of RSA results to histopathology as the gold standard in the assessment of different stages of fusion. This type of study may be able to give us an idea about how accurate RSA is in the assessment of fusion and more importantly may quantify the diagnosis of fusion.
RSA may be considered an invasive procedure. The beads can be inserted via an open technique during the surgical exposure to perform the index surgery and this may require further dissection or exposure. The new development of bead insertion instruments and the insertion of the beads at the time of surgical operation where the spine is already exposed makes it less invasive. Percutaneous insertion of the beads has been described and used as separate procedure with potential risks. 48 As a result of this invasive nature of the procedure, human clinical study using RSA requires obtaining informed consent as an additional procedure.
The accuracy of RSA varies in the literatures and it depends on several factors. The accuracy means the closeness of the measured value to the true one. 44 The stability and security of beads fixation, the number of the beads inserted, and the distribution of the beads in each rigid body are the most important factors in determining the accuracy of the RSA setup and assessment. 29,45 The accuracy can be adversely affected by the instability of the beads in the rigid body. 44 This can be improved by using a very tight hole in the bone and avoiding oversize drilling, which keeps the beads loose, or by delaying the assessment for 14 days, especially in metabolically active bone (children) to allow for the initial instability to settle. 45 The alternative way to improve the instability is by using gluing materials like bone wax. The higher the number and the wider the distribution of the beads, the better the accuracy of the RSA assessment. 11,45 The accuracy of RSA is usually measured by testing and retesting of all of the sample of patients and is defined as the standard deviation from the repeated measurements. 32,33,45,46
The precision of RSA is the ability to achieve the same measurements by repeating the test. It can be measured only by repeating the test or by pair examination. Since RSA involves X-ray radiation, repeating the test exposes the patient to extra or double the radiation of a single testing. This is one of the disadvantages of RSA. The advantage of knowing the precision of the RSA testing usually overweighs the risk of radiation exposure, but careful explanation of the risk to the patient is mandatory.
Risk of RSA beads migration into spinal canal, soft tissue, and blood vessel of distant sites is another concern of the clinical use of RSA, especially in patients with poor bone quality. Extraosseous beads migration into the soft tissue was studied by Lawrie et al in the setting of total hip replacement RSA study. 67
Unfortunately, the accuracy and precision of assessment were not mentioned properly in several studies included in this review, and this questions the reliability of these assessments. In some studies, the accuracy was calculated from only the instability of the markers in the rigid bodies, which is inadequate as the number and distribution of the markers play a very important role as discussed above. Most of the studies agreed that the precision of RSA can be detected by repeating the assessment. This has been not uniformly applied. Some studies repeated the RSA assessment in all of the patients included in the study. Other studies repeated the test in a sample of the patients. In a few studies included in this review, the authors used the precision of prior study conducted with the same RSA setup as a reference precision of their new study. The precision and accuracy of RSA need a uniform clear definition to avoid any mix up. Measuring the precision of the study by repeating the RSA in a small sample of patients or by using that of prior study is not without risk. This can result in misleading figures and my affect the overall results of the study.
Although this review gives us a rough figure about the average accuracy of RSA from previous works, which is translation accuracy in mm (0.45, 0.5, and 0.75) in the (x, y, and z axes), respectively, and rotational accuracy in degrees (1.89, 1.92, and 1.13) in the (x, y, and z axis), respectively, these figures are only rough and cannot be taken as exact due to various factors that could affect accuracy in RSA.
The accuracy of RSA did not improve with time as expected for any other radiological assessment tool and this may be because the earlier studies were animal studies, which makes it easier to justify putting a higher number of beads in a wider distribution. Although some recent studies are finite or cadaveric, 68 most are clinical human studies, which make it more difficult to widely distribute the RSA beads in the spine without causing unnecessary dissection and potential harm. 69
Despite all the above-mentioned limitations of RSA, it has been agreed by most researchers that RSA is an accurate method of assessment of spinal range of motion, inducible displacement, and spinal fusion. Humadi et al had tested the accuracy of RSA compared to fine-cut CT scan in an animal study using sheep as a model. They concluded that RSA is as accurate as CT scan with minimal radiation exposure. 63 They also suggested using a special awl in creating the holes for RSA beads and gluing the beads into the hole using bone wax to improve the stability of the beads and improve the accuracy of the assessment. 63
RSA can be used in assessment of scoliosis and in response to surgical correction in terms of derotation as RSA may be able to quantify the amount of derotation achieved postoperatively. RSA can also be used to follow-up traumatic injury of the spine and evaluate loss of position or progressive collapse of these injuries. Kyphoplasty is another area where RSA can be used to guide and follow-up the correction after this procedure. Assessment of ROM following the application of dynesys dynamic posterior stabilization system for treatment of degenerative lumbar spine has been reported using RSA. 70,71
Resorbable radio-opaque bioactive glass markers have shown adequate potential for RSA assessment due to their bone-bonding properties for marker stability and sufficient radio-opacity. 72 It is too early to decide whether this potential marker can replace tantalum beads for RSA assessment, and further preclinical comparison between the 2 markers is suggested be Madanat et al. 72
Conclusion
RSA is a very powerful tool to detect small changes between 2 rigid bodies such as a vertebral segment. The technique is described for animal and human studies for cervical and lumbar spine and can be used to analyze ROM, inducible displacement, and fusion of segments. The accuracy and precision of RSA is superior to other techniques of assessment of motion and inducible displacement like QMA and QF. However, there are a few disadvantages with this technique. RSA is an invasive technique and percutaneous surgical procedure is needed to implant the markers. It is a labor-intensive process requiring trained personnel with specific knowledge to handle data and interpret the results, and it is relatively time consuming and expensive. In conclusion, RSA should be looked at as a very powerful research instrument that can be applied in limited clinical spine work, and there are many clinical questions suitable for RSA studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.