
Abstract
Study Design:
Review of literature.
Objectives:
This review of literature investigates the application of mesenchymal stem cells (MSCs) in spinal fusion, highlights potential uses in the development of bone grafts, and discusses limitations based on both preclinical and clinical models.
Methods:
A review of literature was conducted looking at current studies using stem cells for augmentation of spinal fusion in both animal and human models.
Results:
Eleven preclinical studies were found that used various animal models. Average fusion rates across studies were 59.8% for autograft and 73.7% for stem cell–based grafts. Outcomes included manual palpation and stressing of the fusion, radiography, micro–computed tomography (μCT), and histological analysis. Fifteen clinical studies, 7 prospective and 8 retrospective, were found. Fusion rates ranged from 60% to 100%, averaging 87.1% in experimental groups and 87.2% in autograft control groups.
Conclusions:
It appears that there is minimal clinical difference between commercially available stem cells and bone marrow aspirates indicating that MSCs may be a good choice in a patient with poor marrow quality. Overcoming morbidity and limitations of autograft for spinal fusion, remains a significant problem for spinal surgeons and further studies are needed to determine the efficacy of stem cells in augmenting spinal fusion.
Introduction
Spinal Fusion Surgery
If the structural integrity of the spine is compromised, pain, neurological impingement, or instability may result. Spinal fusion surgery is the most definitive treatment performed to restore structural stability to the spinal column and enhance its ability to support the body and protect the spinal cord. It is currently one of the most common and costly procedures performed in the United States, with nearly 465 000 cases performed annually (Figure 1). 1 All age groups from young children to elderly are treated with spinal fusions, with an average cost of $120 000 per hospitalization and a total expense of $12.8 billion each year in nonfederal community hospitals alone. 1,2 The goal of spinal fusion surgery is to achieve bony stability for the diseased spine. However, a pseudarthrosis, or nonunion, occurs in roughly 25% to 35% of spinal fusion surgery, and success is dependent on the procedure, approach, and patient bone quality. 3,4 Unsuccessful fusion leads to instability, pain, instrumentation failure, and results in an enormous burden to both patients and the health care system (Figure 2). 5 A tremendous amount of research by basic scientists and clinicians has focused on the use of stem cells to increase the rate of spinal fusion. We will review the role of stem cells in spinal fusion surgeries from bench to bedside, highlighting both their potential and limitations in current applications.

(A) Patient radiograph displaying scoliosis of the spine. (B) Initial surgical correction and fixation of scoliosis.
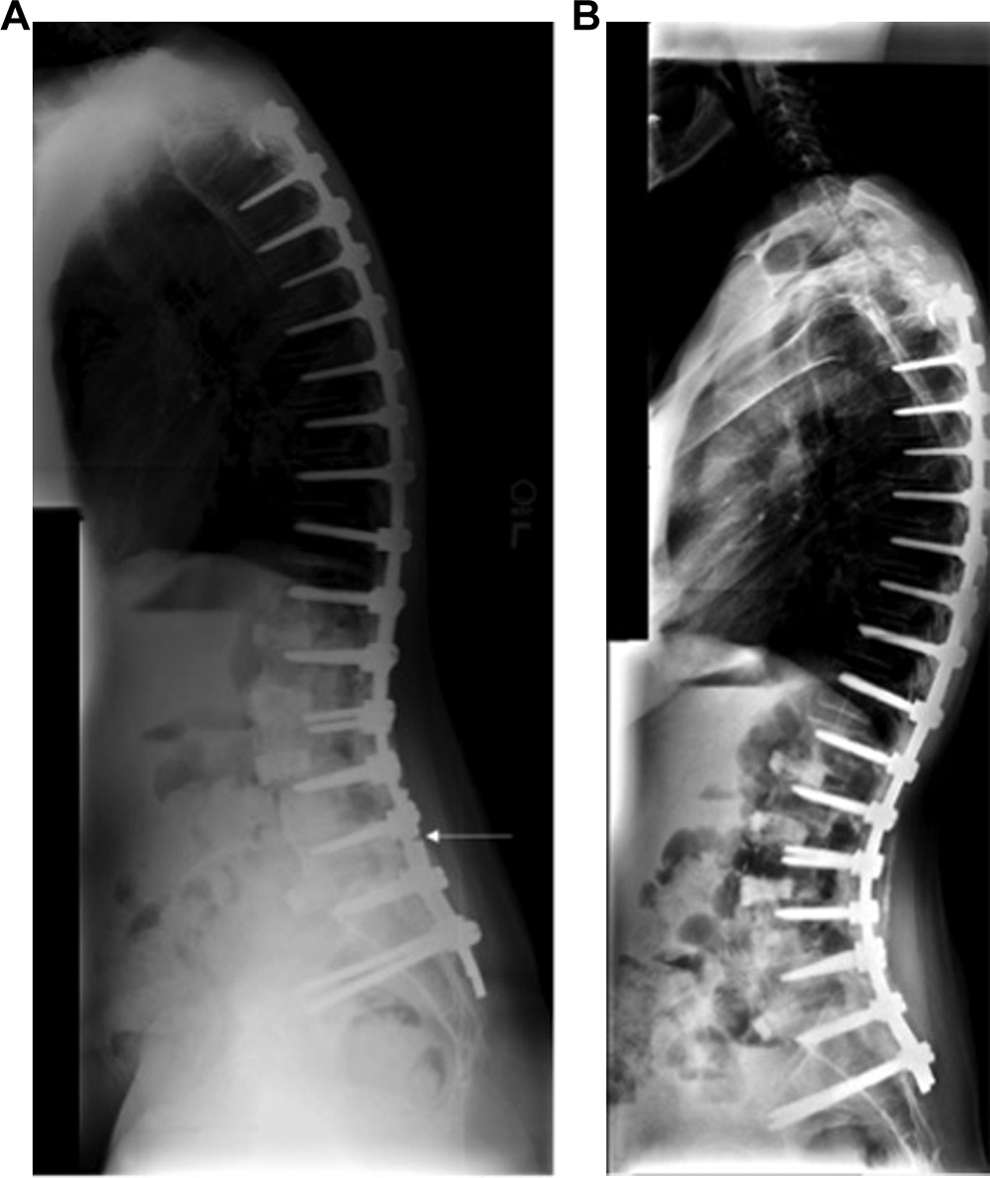
(A) Scoliosis patient from Figure 1 returning with pseudarthrosis and rod fracture requiring revision. White arrow points to rod fracture (B). Revisional fixation after pseudarthrosis.
Requirements for Fusion
A successful posterolateral spinal fusion consists of new bone developing and structurally connecting transverse processes to form a bridge across 2 or more adjacent vertebrae. As such, the surgical site requires immediate structural support, while osteogenic material, local biological signals, scaffolds, and vasculature act together to activate a complex cascade of cytokines and inflammatory factors to induce a bone-healing response or in this case, bone formation. 4,6 –9 The gold standard stimulus to achieve fusion is autologous bone (autograft), which is commonly harvested from the iliac crest or is local bone obtained from the primary surgical site. Autograft contains osteoconductive materials (bone supporting scaffold) such as collagens and bone minerals that provide structural support, osteoinductive factors (bone promoting signals) such as cytokines and growth factors in the transforming growth factor–β (TGF-β) family, and osteogenic components (bone forming cells) such as osteoblastic/preosteoblastic cells or bone marrow stem cells. 10 Autologous bone is the ultimate bone graft because it contains osteogenic, osteoinductive, and osteoconductive abilities.
Although the success rate of spinal fusions with autograft is high (up to 95%), autograft material is limited in quantity and quality varies depending on the patient. There is also significant morbidity of bone harvesting, including surgical site pain, infections, fractures, and cost. 4,11 Therefore, a synthetic graft that replicates the properties of autograft would decrease the need for its use and overall morbidity. Many currently available alternatives contain isolated subsets of the components of autograft such as osteoinduction or osteoconduction, but do not address osteogenic abilities. Examples include demineralized bone matrix, collagen sponges, synthetic grafts that mimic bony substances, or biologics like recombinant human bone morphogenetic protein–2 (rhBMP-2). Advances in the field of regenerative medicine have led to investigation of the osteogenic properties of bone marrow–derived mesenchymal stem cells (MSCs) in spinal fusion. The use of MSCs is attractive since they can be harvested from the host with minimal morbidity, potentially even modified to secrete osteoinductive factors, and implanted on an osteoconductive scaffold providing the 3 key components of osteogenesis to optimize fusion. 12
While MSCs hold great therapeutic promise, their use in spinal fusion surgery has been met with variable success, with some reports indicating great benefits of MSCs and others showing little or no benefit. 13 It is not yet clear whether the primary contribution of MSCs is truly osteogenic or osteoinductive (ie, contributing directly to new bone formation versus secreting trophic factors to induce bone formation from host cells). From here we will discuss the current knowledge of MSCs and their use in spinal fusion therapy by providing a brief comparison with acellular grafts and scaffolds and summarizing current preclinical and clinical studies using MSCs or bone marrow aspirates (BMA) in spinal fusion. By identifying key areas that need further inquiry, we hope to better focus tissue engineering strategies toward enhancing the success rate of spinal fusion surgery without autograft.
Stem Cells
Definitions and Use of Stem Cells
MSCs are a renewable population of undifferentiated cells, resident within their niche in most adult tissues, which can give rise to the various types of mature cells of that tissue (Figure 3). First described by Freidenstein 14 in 1970, they are defined as multipotent cells that adhere to plastic in culture media, display a number of cell specific markers (Table 1), and are capable of differentiation into muscle, bone, tendons, fat, and other stromal tissues 15 –20 They have also been isolated and cultured from these tissues. 21 Some researchers believe they derive from pericytes, which surround blood vessels within each distinct tissue. 22 MSC applications are a significant area of research in modern regenerative medicine due to their ability to form many types of mature differentiated cells. Their utility has been explored in a wide range of clinical settings, including bone marrow transplantation, tissue engineering, cartilage regeneration, graft versus host disease, osteogenesis imperfecta, multiple sclerosis, wound healing, degenerative disc disease, spinal cord injuries, and other pathologies. 21,23 –27 Bone is derived from mesenchymal tissues, and therefore MSCs are clinically useful in the context of bone healing and bone formation.
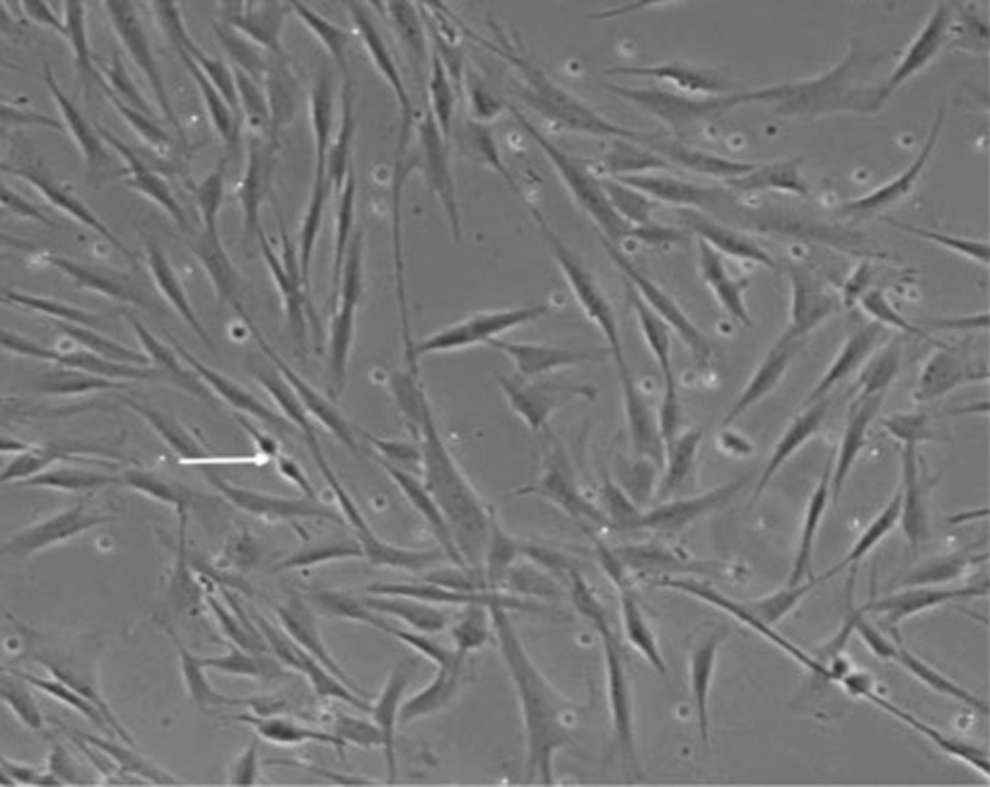
Mesenchymal stem cells growing in vitro. White arrow indicates healthy dividing cells.
Stem Cell–Specific Markers.
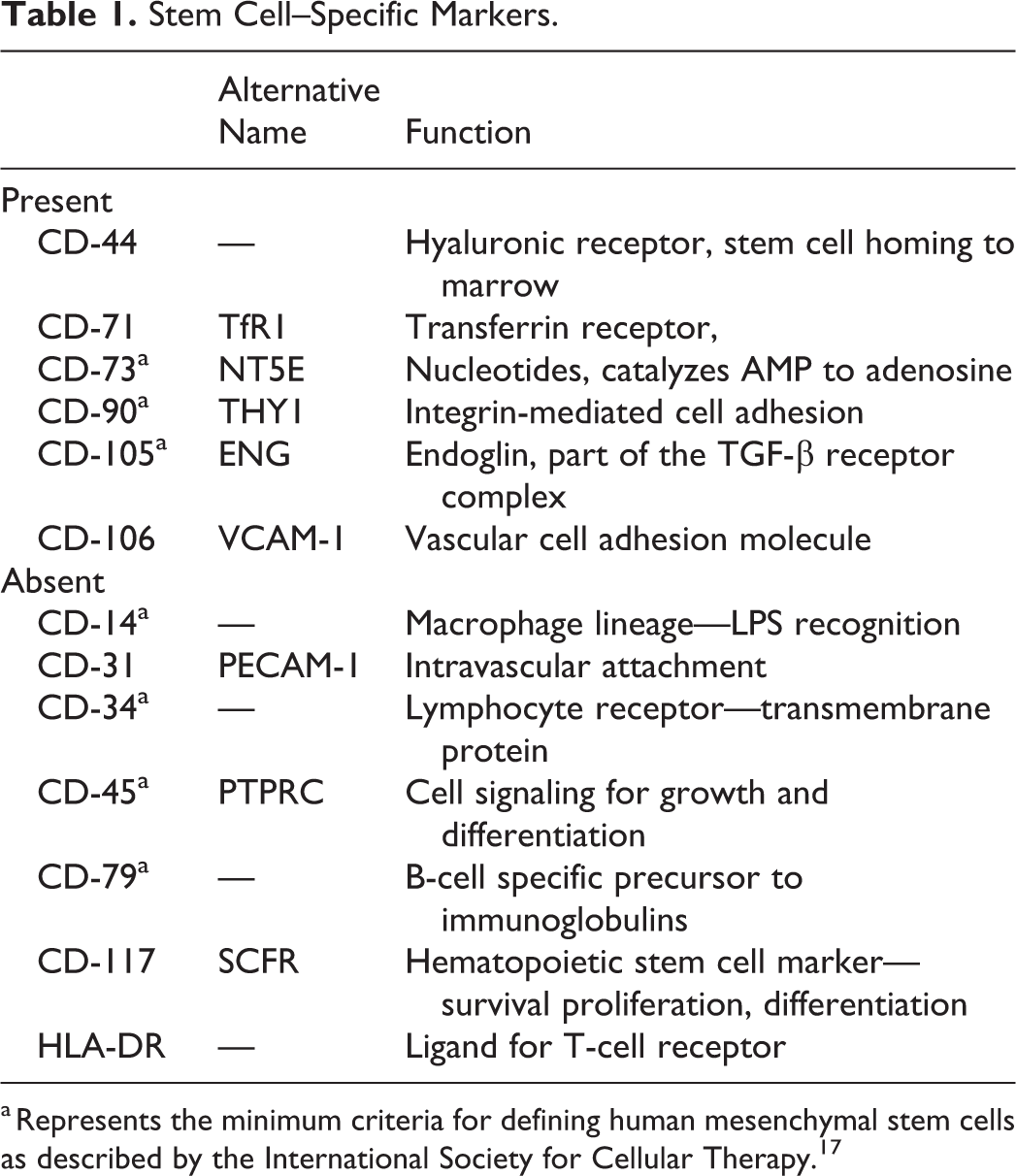
a Represents the minimum criteria for defining human mesenchymal stem cells as described by the International Society for Cellular Therapy. 17
Osteogenesis
Perhaps the most common source of MSCs is BMA. MSCs represent under 0.01% of the aspirate, and it is thought that an in vitro expansion phase is necessary to obtain sufficient stem cell numbers before implantation. 21 Once the MSCs are isolated and expanded, they can be stored frozen until utilized. Although bone marrow aspiration is not a completely painless process for the patient, adding some local morbidity, it represents a significant improvement when compared with harvesting autologous bone grafts from a secondary surgical site. 17,18
It is believed that stem cells contribute to the fusion process and improve union. They have the potential to exhibit both osteogenic and osteoinductive properties within the fusion bed. Both local bone and distant site autologous bone grafts can serve as a source of stem cells at the fusion site, and many researchers and clinicians have begun incorporating MSCs directly into grafting material in hopes of improving fusion rates. Although stem cells contain both osteogenic and osteoinductive properties, when implanted without additional growth factors, they do not produce the same fusion rates as autograft. 28 The decreased fusion rates without additional osteoinductive factors highlights the need for all 3 components of a bone graft to be present for successful fusion.
Osteoinduction
Recently, osteoinductive factors have been used to improve fusion success rates. 29 Bone morphogenetic protein (BMP) is the most commonly used osteoinductive factor. Many studies demonstrate between 65% and 99% fusion with the addition of these BMPs; however, there are also concerns over its current use. 30 –32 BMP is a highly osteoinductive member of the TGF-β protein family and many different isoforms of BMP exist. 18 rhBMP-2 is Food and Drug Administration (FDA)–approved for clinical use in single level anterior interbody lumbar fusion. 33,34 The clinical use of BMP has increased drastically over the past 10 years, and now BMP is most often used off-label in posterolateral spinal fusion. 35,36
BMP is effective in inducing spinal fusion, but there are recent concerns over its safety. Adverse effects include antibody formation to the foreign protein, ectopic bone formation, retrograde ejaculation, postoperative radiculopathy, cardiac arrhythmias, and potentially cancer (Figure 4). 37,38 BMP is also expensive, causing some to question the necessity of its routine use. 39 Many institutions and organizations, including the Yale University Open Database Project, Medtronic internal reports, and the FDA have investigated the impact of rhBMP-2 in spinal fusion and found adverse events correlated with its use. 39 However, this data has been challenged by recent studies. Prospective trials and retrospective reviews of 55 000, 16 000 800, and 500 patients found no or minimally increased statistical significance in adverse events with the use of BMP. 32,33,36,40,41 As highlighted by one of these studies; the negative correlations nearly disappear once the data is controlled for patient age and operation status (primary vs reoperation), and the overall complications related to BMP use are low. 33,42 A major weakness of these studies is a short average follow-up of only 2 to 5 years. Each of these short-term studies certainly requires longer follow-up to monitor for any future side effects. Despite the current debate over the safety of BMP, it is a powerful osteoinducer and is clinically useful in promoting osteogenesis in spinal fusion.
Large callous formation after surgical correction and fixation of patient with scoliosis. White arrows point to borders of callous extending from the spine.
Osteoconduction
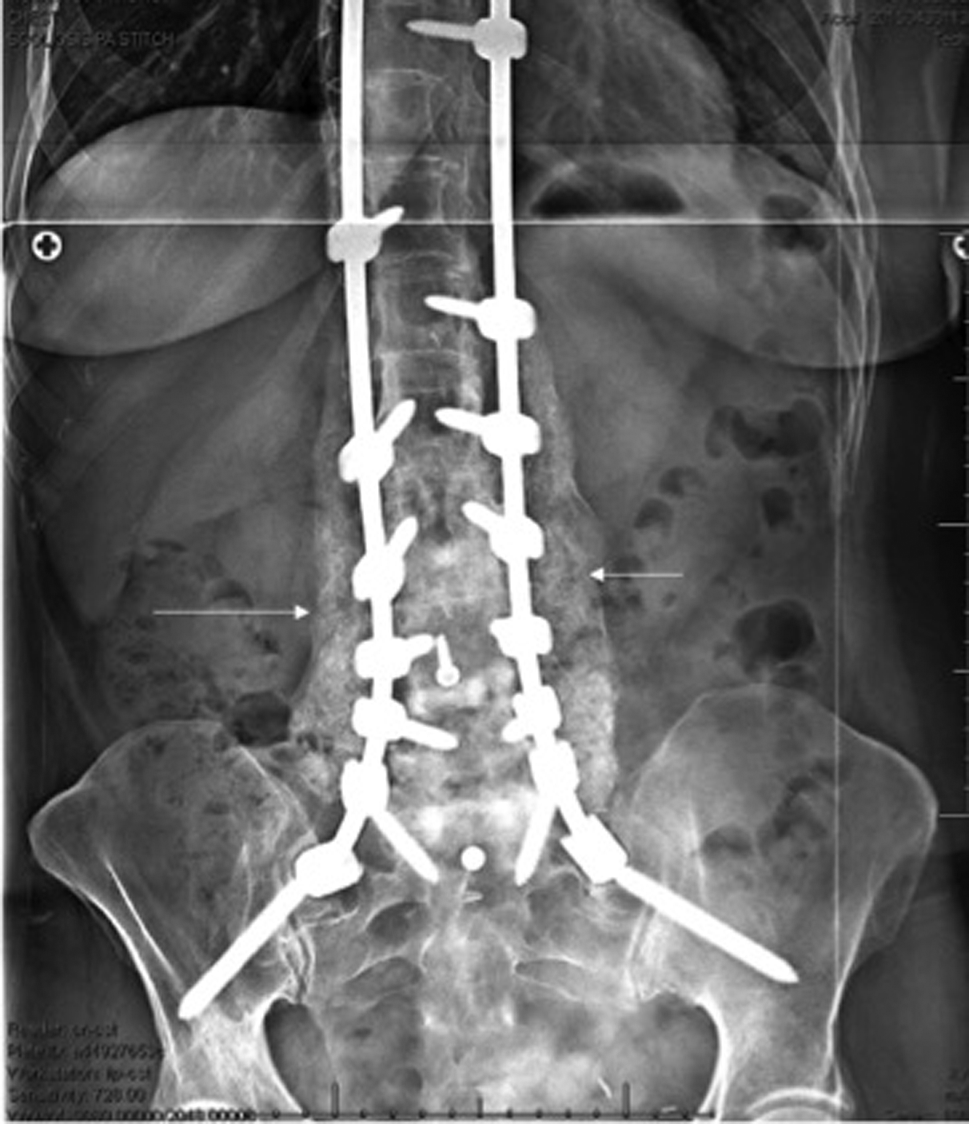
A major function of bone graft is to provide an osteoconductive scaffold on which cells may proliferate to fill structural defects caused by tumor, infection, surgical removal, or trauma. 17 Limits to the more widespread clinical use of bone grafts include insufficient or poor quality of autograft (from the host), and increased risks of disease transmission or rejection from allograft (donor/cadaver) or xenograft (animal). 17 An ideal osteoconductive scaffold would be biocompatible and integrate rapidly into native tissues. 8 Synthetic bioscaffolds such as demineralized bone matrix (DBM) are used to encourage bone growth and can be effective, but lack inherent osteogenic ability. 10 The amount of osteogenesis induced by DBM is highly variable depending on the host, and may be insufficient to fill every defect, since the host cells provide the osteogenic material (Figure 5). 43 Lack of cellular adherence to the material and rate of resorption are the most common obstacles to overcome with synthetic grafts. Absorption rate of graft material should parallel endogenous osseous remodeling replacing the scaffold with newly formed bone. 44

Image showing spinal fusion with mixed autograft and demineralized bone matrix (DBM) material to provide scaffold for bone growth.
Native bone is composed primarily of type I collagen and a carbonated form of hydroxyapatite (HA) called bone mineral. Synthetic HA is similar to native bone making it an appealing substrate in the development of bone grafts. It is immunologically inert and more stable than collagen. 45 However, HA is brittle and resorbed over a long period of time. β-Tricalcium phosphate has similar properties to bone, including porosity, protein binding affinity, and has more rapid resorption than HA, making it a favorable osteoconductive platform for native tissues to grow. 46 The microporosity of β-tricalcium phosphate can be engineered to enhance osteoconduction via blood vessel incorporation, improving bone formation. 45
Scaffolds in isolation do not result in fusion, and many studies use a scaffold alone as their negative control. 7,30,47 –50 Current scaffold materials available for clinical use are listed in Table 2. 28 A recent review article of the current scaffolds used for bone defects outlined the types of grafts currently employed in long bone fusion. 30 They described 23 different preclinical and clinical studies and found that MSCs implanted on a biologic or synthetic scaffold are effective in promoting bony union in long bone defects and are superior to scaffolds alone. The most common graft material used in these studies was β-tricalcium phosphate. Each of these studies also found that the addition of MSCs is effective, but grafts alone were not sufficient to promote fusion.
Currently Described Scaffolds and Growth Factors Shown in Animal Models.

Preclinical Results
Given the current interest in regenerative medicine, studies involving stem cells for bony fusion are emerging more frequently. Preclinical trials investigating the efficacy of stem cells in animal spinal fusion models include rats, rabbits, sheep, and monkey models. 51 –54 Recent systematic reviews have looked at the use of stem cells for osseous repair. 47,55 Many studies look at applications outside of spinal fusion and will not be discussed in this article. On close inspection of the preclinical spinal fusion studies found in those reviews, there is significant variability in fusion rates (Table 3). 31,49 –51,54,56 –61 Inconsistencies are evident when comparing fusion rates of autograft constructs compared to stem cell-based grafts, although comparing across studies is difficult because of the wide range of variables related to each study design. Average fusion rates across studies of 59.8% for autograft and 73.7% for stem cell–based grafts. Some studies have found the addition of stem cells achieved fusion rates superior to autograft and yet other studies have found significantly inferior fusion rates with the use of cell-based grafts. Interestingly some of the more recent studies report worse fusion rates with MSCs than with autograft. 54,57,61 Overall, the majority of these studies are able to at least replicate the fusion rates of autograft with synthetic materials and cells. Current evidence seems to indicate that the addition of either growth factors or stem cells to an appropriate scaffold leads to improved fusion results.
Preclinical Studies of Spinal Fusion Surgeries Comparing Fusion Rates Between Cell-Containing Constructs With Allograft.
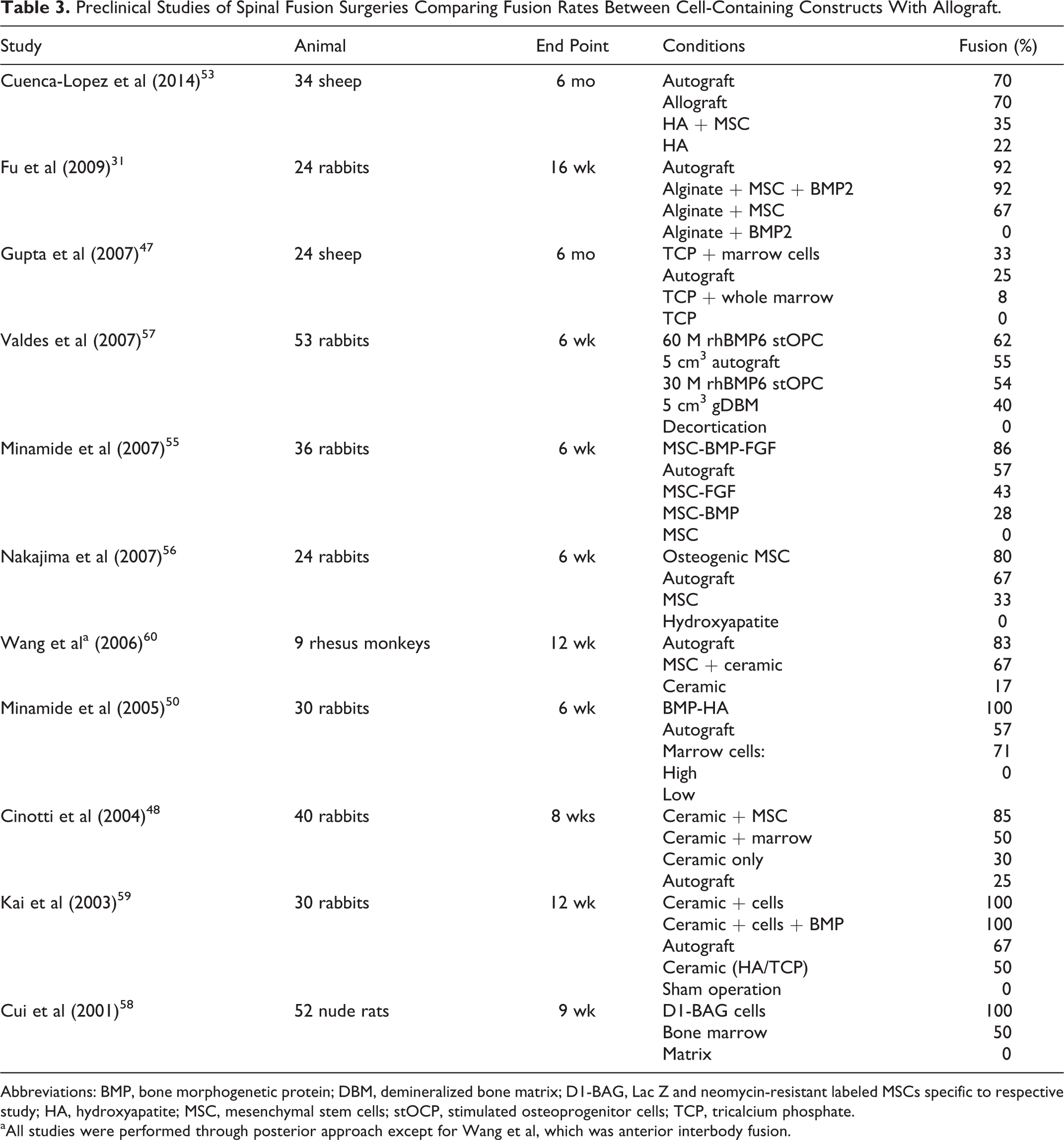
Abbreviations: BMP, bone morphogenetic protein; DBM, demineralized bone matrix; D1-BAG, Lac Z and neomycin-resistant labeled MSCs specific to respective study; HA, hydroxyapatite; MSC, mesenchymal stem cells; stOCP, stimulated osteoprogenitor cells; TCP, tricalcium phosphate.
aAll studies were performed through posterior approach except for Wang et al, which was anterior interbody fusion.
In summary, preclinical trials demonstrate that MSCs together with an appropriate scaffold and growth factors aid in new bone formation and approach or match fusion outcomes achieved with autograft. However, the question of whether the use of these cells will translate to clinical spinal fusions requires further exploration.
While there is substantial information regarding preclinical use of stem cells in bony fusion and some specific to spinal fusion, current clinical trials are few in number. The animal models show promising results without short-term complications from the use of MSCs. Given the apparent safety of their use, more clinical trials involving stem cells in spinal fusion are occurring, but results are still pending.
Clinical Results
At present, there are few published clinical studies using stem cells, and many use proprietary constructs of commercial grade stem cells on a matrix. Most studies evaluating cellular augmentation of bone grafts in spinal fusion use BMA as the primary source of stem cells 62 –66 BMA is harvested from the iliac crest intraoperatively and transplanted to the fusion site. Studies using BMA have found fusion rates similar to autologous bone. 62 Some have explored different BMA harvest sites to determine the highest yield of cells and found vertebral bodies to be a robust location for aspirate. If the findings were reproducible, it would allow for convenient and superior intraoperative isolation of cells with similar number of cells in the vertebral body aspirate as in the iliac crest. 67 This could potentially obviate the need for an additional puncture site for aspiration. Studies utilizing BMA intraoperatively as a source for MSCs show fusion results ranging from 87% to 92.3% in a total of 297 patients (Table 4). 62 –65,67 –71 Importantly, only 1/10 000 cells per BMA are mesenchymal stem cells in a young healthy patient, with significantly lower yields with increasing age. Given the variable quality of a patient’s stem cells due to age, health, smoking status, and other factors, a BMA may not consistently yield cells to support fusion. 72 Fusion results in elderly or otherwise compromised patients may improve if MSCs are first isolated and expanded prior to implantation or derived allogeneically. 15
Clinical Studies in Spinal Fusion Displaying Fusion Rates Across Studies.
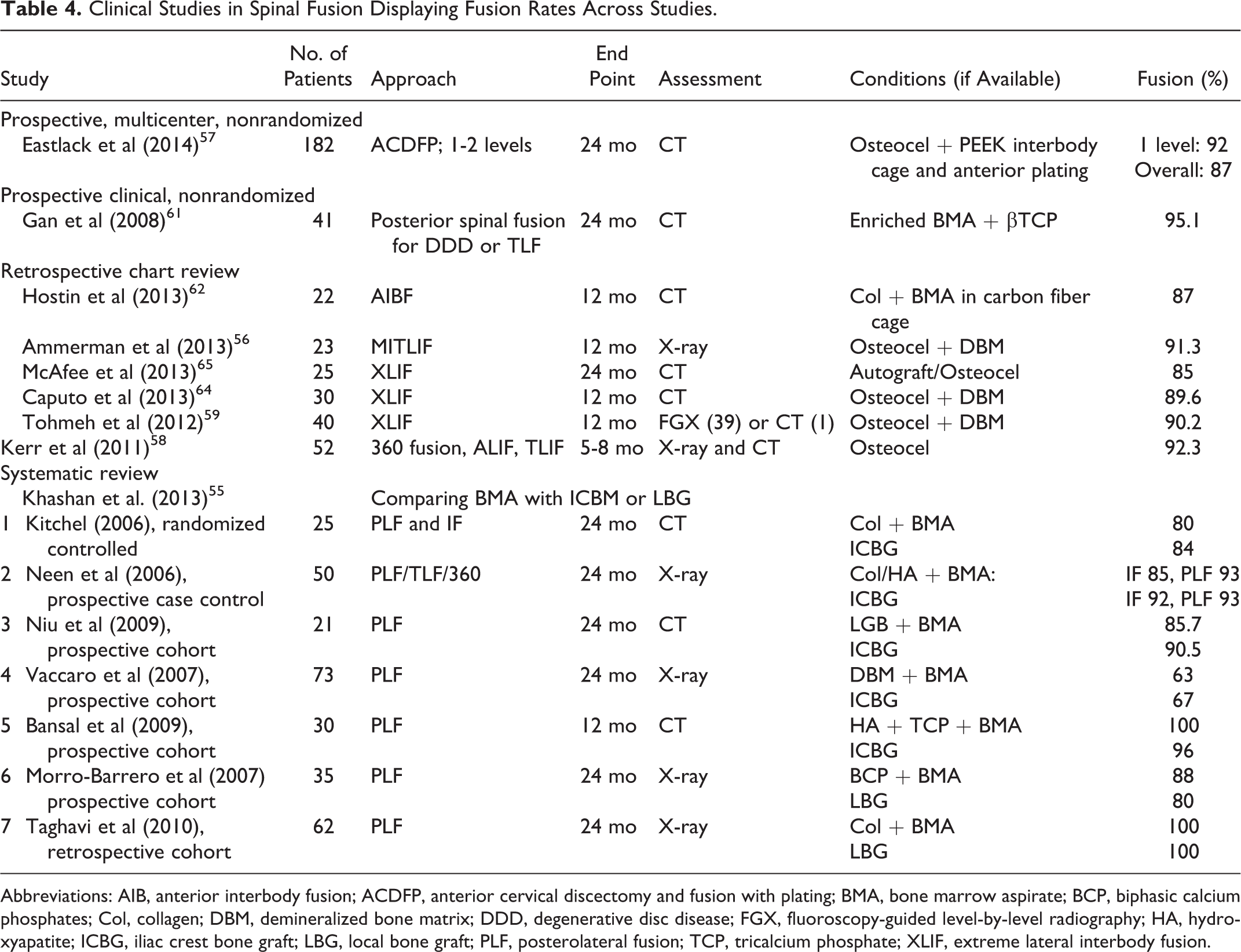
Abbreviations: AIB, anterior interbody fusion; ACDFP, anterior cervical discectomy and fusion with plating; BMA, bone marrow aspirate; BCP, biphasic calcium phosphates; Col, collagen; DBM, demineralized bone matrix; DDD, degenerative disc disease; FGX, fluoroscopy-guided level-by-level radiography; HA, hydroxyapatite; ICBG, iliac crest bone graft; LBG, local bone graft; PLF, posterolateral fusion; TCP, tricalcium phosphate; XLIF, extreme lateral interbody fusion.
Eight prospective clinical trials involving BMA for spinal fusion were found in the literature. One included 41 prospective patients over a 3-year period using enriched BMA on a β-tricalcium phosphate scaffold. 68 BMA was collected and enriched using a cell separator and centrifugation to concentrate MSCs perioperatively, then seeded onto a β-tricalcium phosphate graft using negative pressure. 68 Good incorporation of the graft as visualized with computed tomography scan was shown in all but 2 patients at 1 year and they reported a 95.1% fusion rate. Another prospective multicenter trial was, nonrandomized, unblinded, and included 182 patients. Overall fusion rates of 87% were reported in this article using computed tomography for fusion analysis. Another study compiled results from 7 different clinical studies, 6 of which were prospective, with 1 being a randomized controlled trial. Each study group had 20 to 70 patients totaling 317 subjects and compared BMA on a scaffold with iliac crest or local bone graft. 62 Fusion rates ranged from 60% to 100%, with an average fusion rate of 87.1% in the experimental group compared with 87.2% in the control group using a variety of fusion assessments.
When comparing BMA with commercially available stem cells, it appears that there is minimal clinical difference between BMA and stem cells. MSCs may be a good choice in a patient with poor marrow quality, but the data on its efficacy is limited. Six studies were found that utilized commercial MSCs to provide a reliable population of stem cells, having an average fusion rate of 89.3%. Most were retrospective reviews; however, there was 1 single-center prospective trial and 1 prospective multicenter trial. 63 –66,73,74 Unfortunately, this multicenter trial investigated anterior cervical decompression and fusion, a procedure with historical fusion rates of 95% to 97% using current techniques. 75 There are currently no studies involving spinal fusion where stem cells are isolated from the patient and expanded in vitro prior to implantation. Doing so would require knowledgeable and skilled staff with appropriate facilities in place, but may be an area of potential advancement under the theme of personalized medicine. A study investigating posterolateral spinal fusion rates with MSCs would provide more insight into their efficacy.
Clinical trials are continuing, and 18 studies involving stem cells and spinal fusion are listed on clinicaltrials.gov. 76 Three are active with 3 continuing to recruit patients. Of the remaining trials, 1 has been terminated, 1 withdrawn, 6 completed, and 4 are in unknown status. Five trials were completed from March 2010 to September 2013; however, no results have been published from any of these studies. We can only speculate as to why this is the case. Certainly, from a scientific standpoint, the results of these studies would be useful in advancing clinical knowledge and potential application of stem cells for spinal fusion.
Discussion
Overcoming the morbidity and limitations of autograft for spinal fusion remains a significant problem for spinal surgeons, and MSCs may be a good alternative and a potential choice for bone graft augmentation in a patient with poor marrow quality. There is a significant amount of preclinical data and some preliminary clinical data on the use of MSCs in spinal fusion; however, most studies use BMA and not isolated MSCs. An appropriate scaffold with the correct growth factors can induce bone formation and healing. This has been demonstrated on multiple animal models in spinal fusion and stem cells have proven to be necessary in the development of new bone in these preclinical models. MSCs exhibit both paracrine effects on their local environment and directly differentiate into osteogenic cells, but the degree to which they contribute to each of these pathways during spinal fusion is still unclear. In vivo characterization of stem cells may lead to improved fusion rates as grafts could be tailored to highlight their properties. The lack of information about the variety of scaffold materials available also makes it difficult to know which material is the most effective. MSC constructs with osteoconductive and osteoinductive factors appear to approach fusion rates similar to autograft based on the limited data. Further studies are needed to determine the exact role that MSCs play in the incorporation of graft materials into spinal fusion models as well as the safety of implanted cells that have been bioengineered to secrete osteoinductive factors. Studies directly comparing graft materials are also needed to identify the optimal material for application in these models. Optimizing the design of scaffolds to augment the activity of the transplanted stem cells may lead to improved outcomes after spinal fusion surgeries with improved fusion rates, decreased need for autograft, and therefore decreased morbidity to the patient.
Clearly, more information is needed and a more direct method of comparison is necessary. Additionally, the results of completed clinical trials will help guide future development of stem cell containing grafts for spinal fusion depending on their results.
Conclusion
While autograft is the gold standard with inherent osteogenic, osteoconductive, and osteoinductive properties, scaffolds with the addition of proteins and/or MSCs may be able to recreate the union potential of this gold standard. Scaffold and BMP have been shown to yield comparable fusion rates with autograft bone, but there are significant concerns and conflicting views regarding the routine use of BMPs. BMA on a scaffold appears to provide fusion outcomes similar to autograft and a BMA is significantly less morbid to the patient than an iliac crest bone graft, but may not be a viable option in all patients. To improve the variable results in current spinal fusion rates, there is a clinical need for material that replicates the properties of autograft without the morbidity, particularly in patients with poor bone quality. Autologous or allogeneic MSCs may be able to achieve union without these deleterious side effects in patients with poor bone marrow quality, indicating that MSCs have great potential for becoming the future gold standard in bone graft augmentation.
Footnotes
Acknowledgments
The data collection and analysis as well as the preparation of this article were conducted without contract or direct funding from any sponsor.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Michael A. Robbins is supported by the National Center for Advancing Translational Sciences, National Institute of Health through grant number UL1 TR000002 and linked award TL1 TR000133.