
Abstract
Study Design:
Case series and literature review.
Objective:
There is a growing body of literature supporting that osteochondroma of the spine may not be as rare as previously documented. The purpose of this study was to perform an updated review and present our experience with 4 cases of solitary osteochondroma of the spine, including surgical treatment and subsequent outcomes.
Methods:
A review of 4 cases and an updated literature review.
Results:
All 4 cases were diagnosed as solitary osteochondroma of the spine based on clinical and histopathologic findings. Majority of the lesions arose from the posterior column with one case showing extension into the middle column with clinical neurologic sequelae. Treatment strategies for all cases included complete marginal excision of the lesions using a posterior approach. All 4 cases showed no radiographic evidence of recurrence. The literature review yielded 132 cases of solitary osteochondroma and 17 case associated with multiple hereditary exostosis. Out of the 132 cases, 36 presented with myelopathic symptoms.
Conclusion:
Osteochondroma of the spine may not be as rare as previously reported. The best approach to treatment in almost all symptomatic cases include wide surgical excision of the tumor. This should include complete resection of the cartilaginous cap of the tumor in an effort to prevent recurrence. When excision is performed properly, the outcomes are excellent with very low recurrence of the tumor.
Introduction
Osteochondroma (exostosis) is the most common benign bone tumor, accounting for 36% of benign bone tumors. 1 Most often found in long bones, reports suggest osteochondroma of the spine to be relatively rare, accounting for only 4% to 7% of primary benign spinal tumors 1 -3 and less than 3% of all osteochondromas. 3,4 Osteochondroma can arise as a solitary lesion or as part of an inherited condition known as multiple hereditary exostosis (MHE). 1 Several studies have reported that solitary osteochondromas are more common in the spine when compared with osteochondroma associated with MHE. 2,4,5 There is a growing body of evidence suggesting osteochondroma of the spine may not be as rare as previously reported. 6 -8 In this article, we describe our experience with the diagnosis, treatment, and natural history of osteochondroma of the spine of 4 cases, and the most up-to-date literature review of this topic since 2003.
Case Series
The authors have obtained the patients’ informed written consent for print and electronic publication of the case report.
Case 1
A 6-year-old female was brought to the emergency department for nonradiating neck pain that was localized to her left posterior neck. The patient had no neurological signs or symptoms. Radiographs demonstrated an osseous neck mass arising from the posterior cervical elements (Figure 1). Advanced imaging (magnetic resonance imaging and computed tomography scans) demonstrated an osseous lesion with a medullary cavity contiguous with the left C6 lamina. No signs of cord or root compression were seen. The patient has no known significant medical or family history of similar lesions.
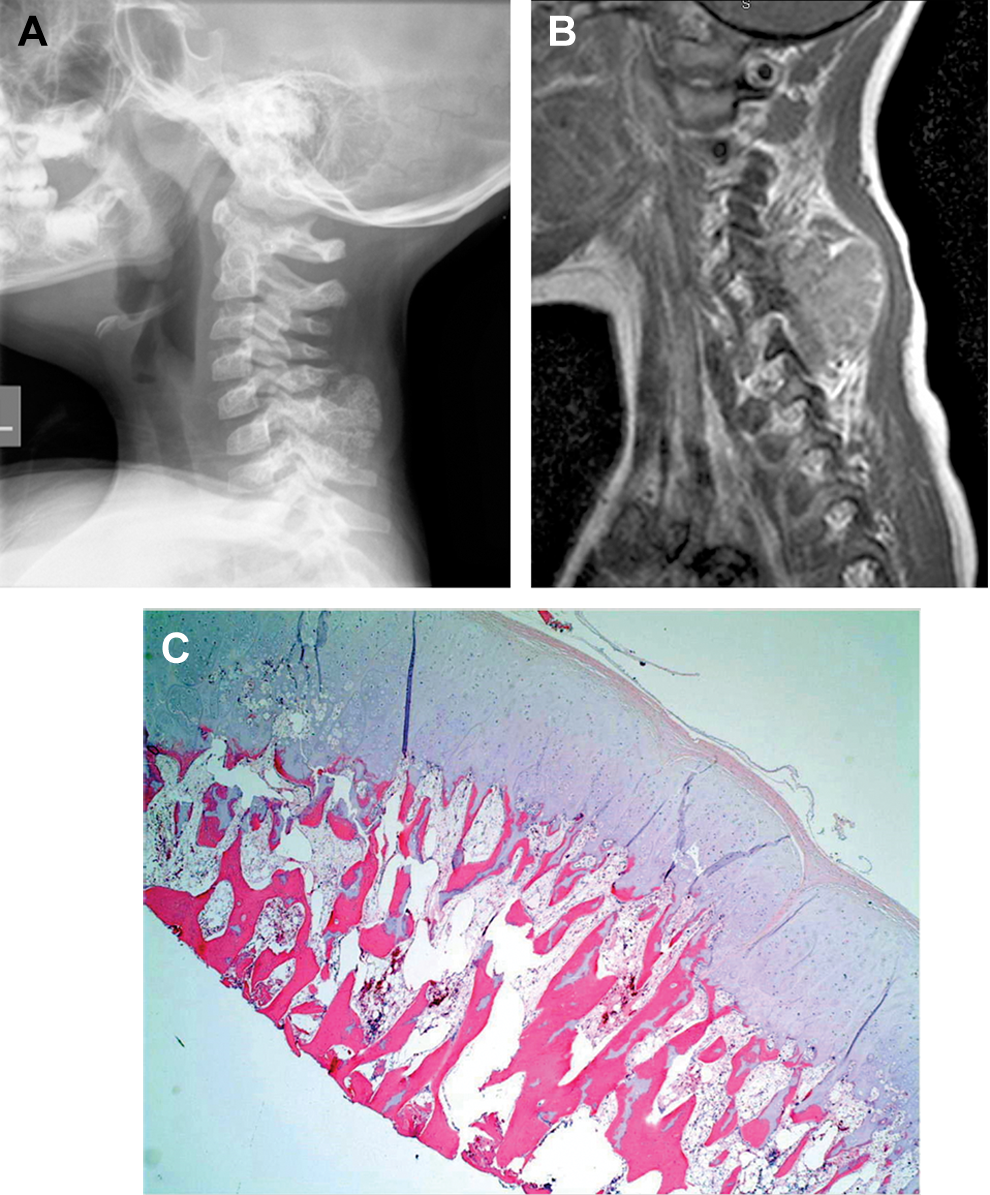
A 6-year-old female referred for a nonpainful mass in her neck noticed by her family. (A) Lateral radiograph showing ossified mass involving the C6 vertebrae and (B) sagittal magnetic resonance imaging showing the extent of the soft tissue involvement and the mass arising from the posterior cervical elements. (C) Hematoxylin and eosin slide of the cervical mass demonstrating a benign cartilage cap with subchondral bone, findings typical of an osteochondroma.
Case 2
A healthy 35-year-old male complained of 2 weeks of persistent mid-back pain after riding a go-cart. The patient denied any neurological symptoms during this time and was neurologically intact on physical examination. Imaging studies showed an osseous lesion about the low thoracic and thoracolumbar junction (Figure 2) without neurological involvement. The patient denies any medical or family history of similar lesions.
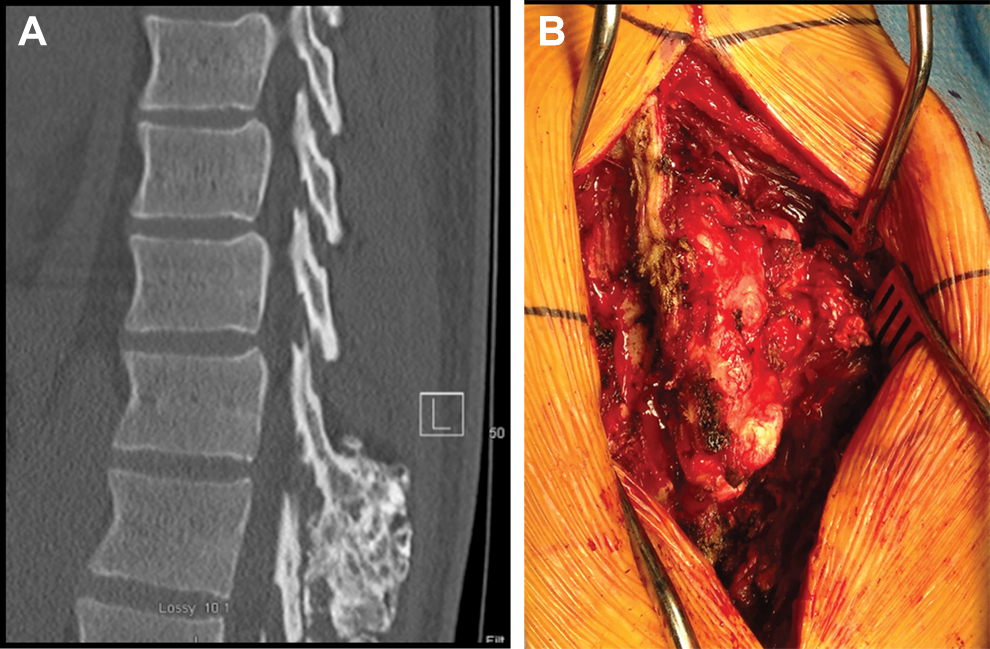
A 35-year-old male with mid-back pain following a minor injury. Plain radiographs demonstrated a mass arising from the posterior elements of T12. (A) Mid-Sagittal computed tomography scan of the thoracic spine demonstrating an osseous mass at the thoracolumbar junction. (B) Intraoperative clinical photograph of well-encapsulated thoracic mass.
Case 3
An 11-year-old male had progressive right posterior neck swelling for the past 10 months. A cervical computed tomography scan showed a mass at the C6 vertebrae with medullary continuity with the right lamina and spinous process. There was no evidence of cord or nerve root compression or vascular compromise. There was no significant medical or family history of similar lesions.
Case 4
A 36-year-old female had neck pain and progressive myelopathy (bowel and bladder dysfunction, gait abnormality, and progressive upper and lower extremity weakness). No history of antecedent trauma was reported. Plain radiographs showed an osseous lesion arising from the posterior column with significant canal compromise at the level of the C3 and C4 vertebrae (Figure 3). The patient had no medical or family history of similar lesions.
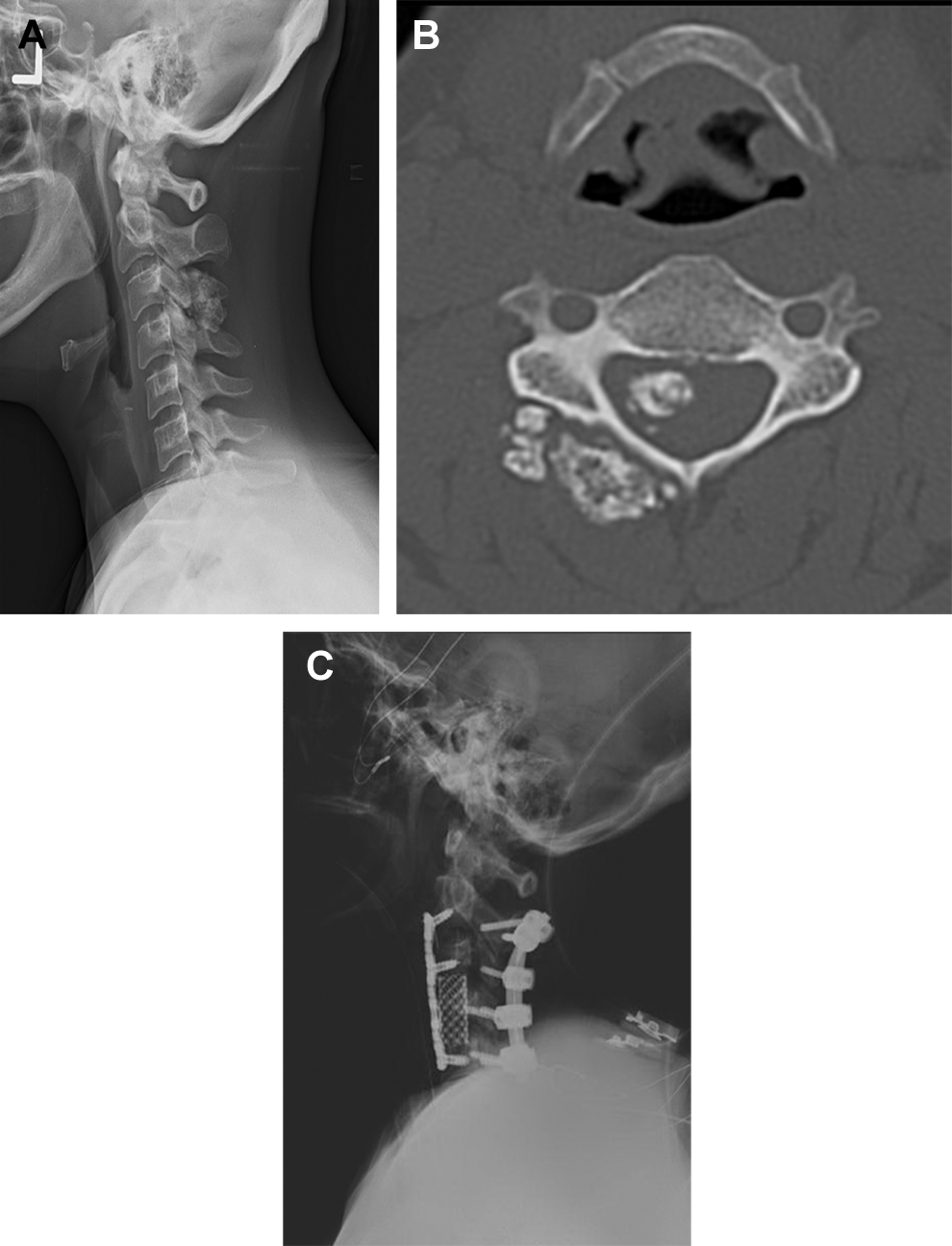
(A) Lateral radiograph and (B) axial computed tomography scan showing osseous mass arising from the right C3 lamina and invading the spinal canal causing cord compression. Biopsy revealed an osteochondroma. (C) Postoperative lateral radiograph showing C3 vertebrectomy, anterior reconstruction with a titanium cage and plate, and a posterior instrumented fusion from C2 to C5 required to stabilize the spine following a wide resection of the osteochondroma.
Literature Review
Ovid MEDLINE and other nonindexed citations database search engines were used with the assistance of a medical librarian. The terms “osteochondroma” and “spine” and/or proxy descriptors were used to query PubMed. No limit in publication year, country, or language of publication was used. This yielded a list of all reported cases of osteochondroma of the spine since 1951. The list of articles was screened using the inclusion criterion—all reported cases from 2016 to 2004—and the following exclusion criteria: literature reviews, cases of primary tumor not arising from spine, non–case report accounts of cases, and nontumor processes (infection). Each case was reviewed for each parameter of clinical history and radiographic description whenever available in the case reports. Demographics, anatomic location of tumor, symptoms, treatment, and recurrence rates of tumor were almost always available and reported. A custom-built Excel database was used to organize and analyze the data. Descriptive statistics were used to summarize the results of the data.
Results
All 4 cases were diagnosed as solitary osteochondroma of the spine based on clinical findings and histopathologic features. All cases except for “Case 4” had no neurological symptoms—Case 4 was associated with cord compression and progressive myelopathy. Three of the 4 cases involved the cervical spine (includes case with cord compression) and 1 of 4 from the thoracolumbar region. All cases of osteochondroma in this series appeared to arise from the posterior column, with one case showing extension into the middle column and clinical neurologic sequelae. Treatment strategies for all cases included complete marginal excision of osteochondroma lesions using a posterior approach. Additionally, Case 4 (osteochondroma with cervical retrovertebral lesion and cord compression) required anterior corpectomy with placement of an interbody cage, followed by posterior decompression and instrumented fusion. All patients had complete symptomatic relief at their latest follow-up (up to 2 years) and showed no radiographic evidence of recurrence.
The review literature yielded a total of 223 articles, 2 -92 of which 110 were from the 2016 to 2004 period. Twenty-six articles were excluded, leaving 84 articles in the final analysis. The 84 articles yielded 149 reported cases. One hundred and thirty-two (88.6%) were solitary osteochondromas and 17 (11.4%) were associated with MHE.
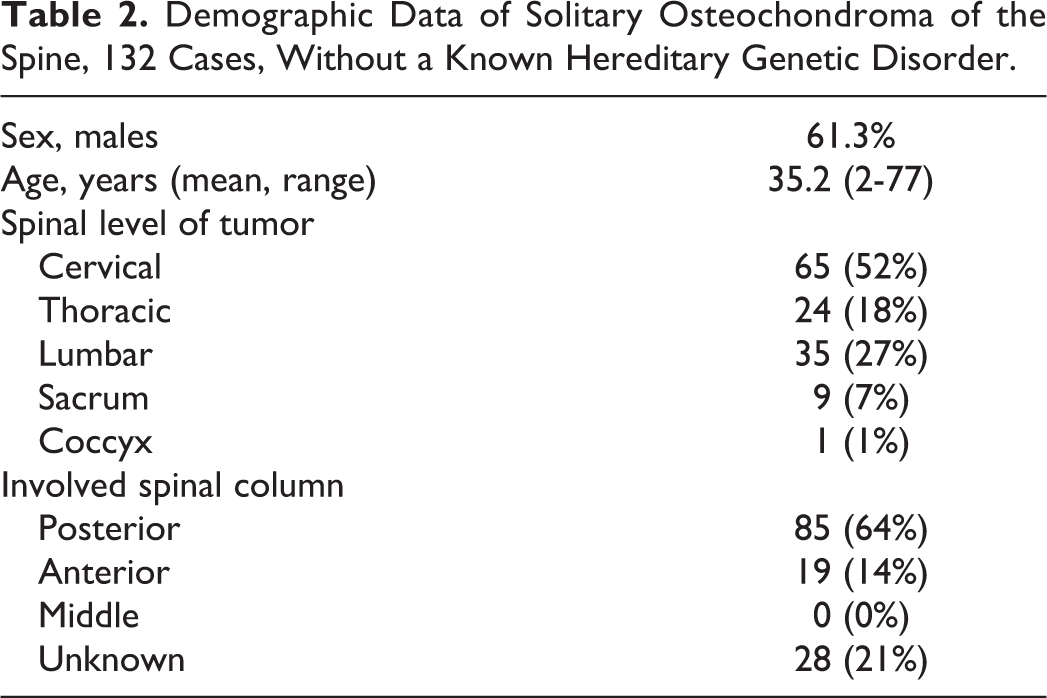
Table 1 lists all 132 cases of solitary osteochondroma of the spine from the literature. Table 1 highlights the interesting data from each case of solitary osteochondroma. The location, treatment, and outcome of the cases are shown, along with the demographic data. For solitary osteochondromas (Table 2), there was a female-to-male ratio of 1:1.6 and an average age of 35.2 years (range = 2-77). The most common spinal level involved was cervical, with 63 (52.2%) of the cases, followed by lumbar 35 (26.5%), thoracic 24 (18.2%), sacrum 9 (6.8%), and coccyx 1 (0.76%). The most frequent spinal anatomic column involved was the posterior column, with 85 cases (64.3%), followed by unknown 28 (21.2%), anterior column 19 (14.3%), and 0 in the middle column.
Reviewed Cases in Literature: Interesting Dataa.

aAll 132 cases reviewed from literature are presented. Age, sex of the patient, location of lesion, type of surgery, symptoms, and recurrence are shown. If symptomatic w/o myelopathic or radiculopathic symptoms, symptomatic due to pain. N/A, data unavailable in the literature.
Demographic Data of Solitary Osteochondroma of the Spine, 132 Cases, Without a Known Hereditary Genetic Disorder.
There were 36 (27.2%) cases that involved solitary osteochondroma with myelopathic symptoms (Table 3). This group had a female-to-male ratio of 1:2.6 and average age of 35.1 years (range = 8-77). The most common spinal level involved was cervical in 24 (66.6%) cases, followed by thoracic 8 (22.2%) and lumbar 4 (11.1%). The most frequent spinal anatomic column involved was posterior column, with 29 cases (80.5%), followed by anterior column 6 (16.6%), unknown 1 (2.7%), and middle column 0 (0%). The osteochondroma began in the posterior arch in 20 (55.5%) of the cases, followed by the lamina in 7 (19.4%), vertebral body in 5 (16.6%), spinous process in 2 (5.5%), and unknown location in 1 (2.7%) of the cases.
Demographic Data on Solitary Osteochondroma With Spinal Cord Compressiona.
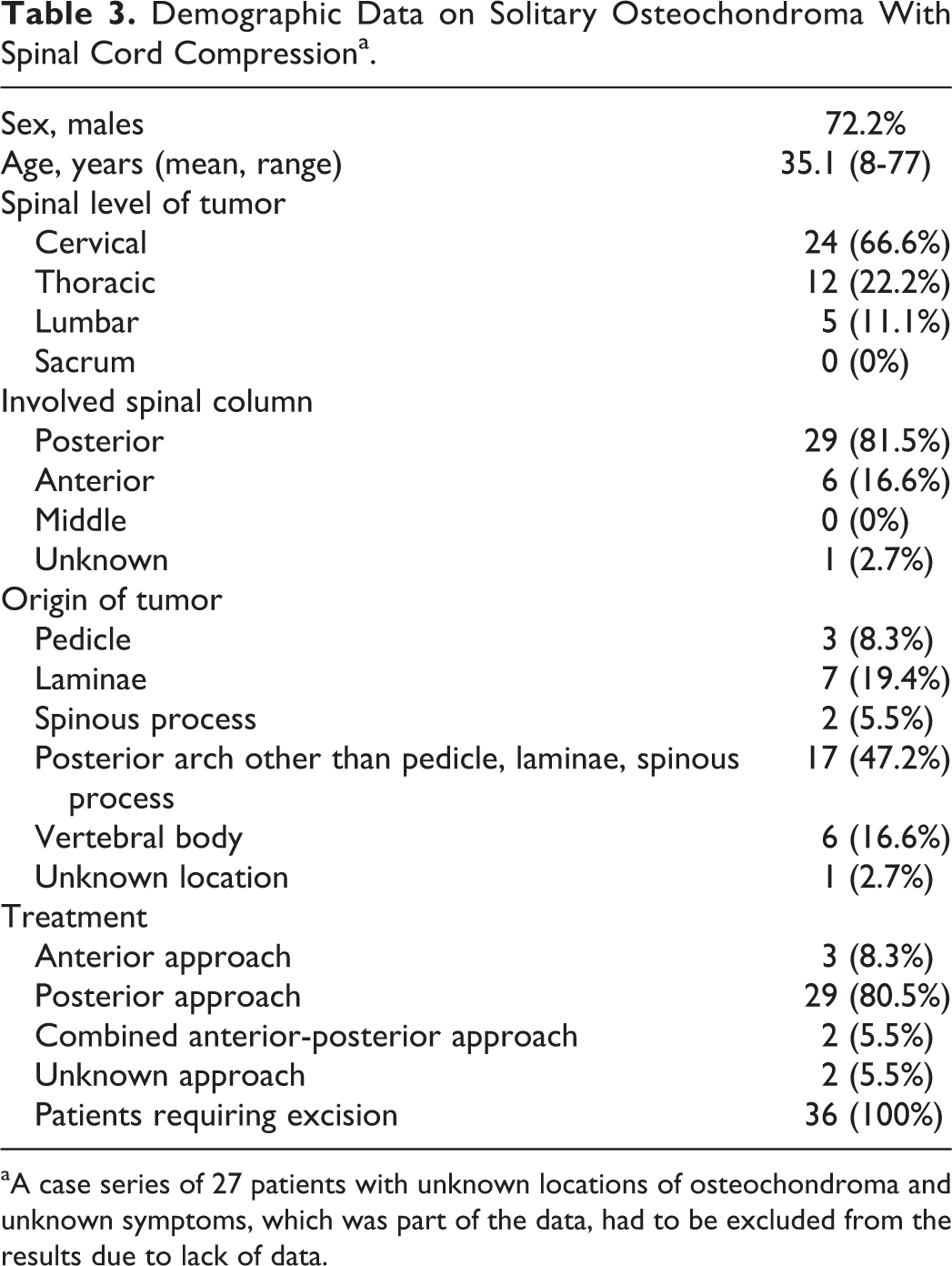
aA case series of 27 patients with unknown locations of osteochondroma and unknown symptoms, which was part of the data, had to be excluded from the results due to lack of data.
All 36 patients underwent surgery, of whom 29 (80.5%) underwent a posterior approach, 3 (8.3%) underwent an anterior approach, 2 (5.5%) underwent a combined anterior-posterior approach, and 2 (5.5%) approaches were unknown. The clinical outcomes showed improvement of symptoms in 34 (94.4%) of the patients, with 28 people showing a complete recovery and 6 with a partial recovery. Two cases showed worsening symptoms after surgery. There were 2 recurrences among all cases recorded, and none among solitary lesions with myelopathic symptoms.
Discussion
The first solitary osteochondroma was reported in 1843 by Reid. 64 Many reports in the literature show that solitary osteochondroma is more common than lesions associated with MHE. The prevalence of osteochondroma in the spine is likely higher than previously thought. There seems to be a rise in the amount of case reports of osteochondroma published in the recent years (2004 to 2016). When Albrecht et al 2 reviewed the relevant English literature from 1843 to 1992, it yielded 96 cases of solitary spinal osteochondroma. When Gille et al 8 updated the review, they identified 54 additional cases of solitary spinal osteochondroma from 1992 to 2003. Our study yielded 132 new cases reported from 2004 to 2016, representing a 2.4-fold increase since 2003.
This increase in the number of cases in a smaller period of time is likely due to a higher rate of case reports being published on the topic rather than an actual increase in the incidence of these tumors. Nevertheless, the higher number of reported cases in the past decade likely underestimates the true prevalence of osteochondroma, because a significant portion of these tumors/lesions remain asymptomatic and, thus, may not be seen by a health care provider and/or require surgical treatment.
The review and analysis of the reported cases corroborate some of the trends seen in the literature, such as cervical spine being the most common site for a solitary osteochondroma of the spine, complete surgical excision being the most common method of surgical treatment, and the good outcomes and low recurrence rates after excision.
Additionally, the review of literature indicated that 27.2% of the cases with solitary osteochondromas of the spine had myelopathic features. This is in concordance with previous reports of 30% by Albrecht et al. 2 It is proposed that the myelopathic symptoms seen in osteochondroma are due to progressive compression of the spinal structures, but may include a potentiated effect as the tumor grows over several years; likewise, the onset of age-related degenerative changes seen with spinal stenosis may also contribute. 8
Osteochondroma is a form of exostosis that can be seen in any age group. It is generally reported that the age range for symptomatic presentation for solitary osteochondroma is between 10 and 30 years for peripheral lesions, but it appears that spine patients develop symptoms at an average age of 32, distinctly different from the peripheral lesions seen in children. By definition, osteochondroma has a characteristic cartilage cap on histology and a medullary continuity with the host bone, and can be sessile or pedunculated. MHE involves many exostoses in a single patient, unlike in the case of solitary osteochondroma, which is more common. An incidence of 1.3% to 4.1% has been reported as the percentage of solitary osteochondromas that affect the spine; however, 9% of MHE lesions are found in the spine. 2 In the current review, 11.4% of all the cases of osteochondromas of the spine reviewed were associated with MHE.
Malignant transformation is low in solitary osteochondroma (<3%), but can be as high as 10% when associated with inherited genetic mutations as seen with MHE. MHE has an autosomal dominant inheritance pattern and involves mutations in the EXT 1, 2, and 3 genes on chromosome 8, 11, and 19, respectively. Malignant degeneration leads to a low-grade peripheral chondrosarcoma, which is managed with complete surgical resection. Malignant transformation of solitary osteochondroma is most frequently reported in the pelvis and rarely occurs in the spine.
A treatment algorithm for these lesions should begin with a thorough history and physical examination, to evaluate for genetic inheritance of similar lesions and to rule out neurovascular compromise that will necessitate surgery. Moreover, the majority of these lesions remain benign and are painless. In benign cases, observation with radiographic surveillance (computed tomography and magnetic resonance imaging and other advanced imaging may be used as indicated to better characterize the lesion and its local effects). Osteochondromas do have a tendency to increase in size and, depending on its location, may be associated with neurologic sequelae. In cases where unrelenting pain and/or evidence of neurovascular compromise (radiculopathy, myelopathy, or vascular compression) exists, surgical management may be warranted. Surgical treatment may include in situ marginal or wide excision, via a posterior, anterior, or combined approach, with or without instrumentation. In some cases, that is, Case 4, a need for cord or nerve root decompression along with instrumented stabilization with or without fusion may be required. Tumor excision may sometimes require both an anterior approach and a posterior approach. Of paramount importance during surgical excision is complete resection of the characteristic cartilage cap seen with these tumors. Incomplete resection of the cartilage cap may increase the risk of recurrence, and the pediatric population is more susceptible to tumor recurrence given their higher growth potential/age at presentation.
The recurrence rate in the review of the literature was 1.3% for all cases, and 0% for solitary spinal osteochondromas with myelopathic symptoms. Nevertheless, the current review of literature demonstrates a lower recurrence rate than previously reported (4%). 8 However, there may be a number of unreported recurrences, given that not all cases in the literature explicitly reported this parameter. There is also the impact of a better understanding of the biology of the tumor, advanced imaging, and surgical techniques allowing for more expedient treatment in the recent years.
Conclusion
Osteochondroma is a relatively common bone tumor, accounting for 36% of all benign bone tumors, 1 but occurs infrequently in the spine accounting for less than 3% of all osteochondromas. 3,4 The solitary lesions in the spine may cause neurologic symptoms including radiculopathy and myelopathy, 29.5% and 27%, respectively, as reported in this review. The best approach to treatment in almost all symptomatic cases is marginal excision of the tumor. Meticulous surgical excision, with complete resection of the cartilaginous cap of the tumor, is important in preventing recurrence. When tumor excision is performed adequately, the outcomes are excellent with very low recurrence rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RY and IO have no relationships to disclose. JRD is an employee of Norton Healthcare; board member, Scoliosis Research Society; receives consulting fees from Medtronic and DePuy; receives payments for lectures from Medtronic, DePuy, and Norton Healthcare; holds patents and receives royalties from Medtronic; is on the editorial review board of JBJS Highlights, Spine, Spine Deformity, JAAOS, and Global Spine. Nuvasive provided funds directly to database company. No funds are paid directly to individual or individual’s institution 06/2012 to 04/2015. LYC is an employee of Norton Healthcare; member, Editorial Advisory Board, Spine and Spine Journal; institutional review board member, University of Louisville Institutional Review Board; research committee member, Scoliosis Research Society; receives research funds from the Orthopedic Research and Educational Fund, 2013 to present; receives Scoliosis Research Society Research Funding, 2013 to present; received funds for travel for Study Planning Meetings from the Center for Spine Surgery and Research of the University of Southern Denmark; received funds for travel for annual required Continuing Education for Institutional Review Board Members, University of Louisville Institutional Review Board; Nuvasive provided funds directly to database company. No funds are paid directly to individual or individual’s institution 06/2012 to 4/2015.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.