
Abstract
Study Design:
Prospective clinical study.
Objective:
Many oral surgeons use platelet-rich plasma (PRP) for bone defects, but the efficacy of PRP for spinal arthrodesis remains uncertain. The objective was to compare the efficacy of autologous local bone graft and PRP with local bone graft alone for promotion of bony union in posterolateral lumbar fusion (PLF) surgery, with investigation of the safety of PRP over 10 years.
Methods:
A prospective study was conducted in 29 consecutive patients who underwent one-level PLF at L4/5 for degenerative lumbar disease. Local bone on the left (control) side and local bone with PRP on the right side were grafted. The fusion area and absorption of grafted bone at 58 regions were determined using computed tomography at 2 weeks and 3, 6, and 12 months after surgery.
Results:
Average bone fusion areas on the PRP side were significantly wider at 3 and 6 months after surgery (P < .05). Average absorption values were significantly lower on the PRP side than on the control side at 3 and 6 months after surgery (P < .05). The PRP/control ratio was significantly different at 3 and 6 months compared to that at 2 weeks (P < .005). No adverse events related to PRP occurred with good clinical outcome over 10 years follow-up.
Conclusions:
Local application of PRP combined with autologous local bone graft has a positive impact on early fusion for lumbar arthrodesis with no adverse events over 10 years, and thus is a safe and low cost autologous option in spinal fusion.
Keywords
Introduction
Spinal fusion surgeries have expanded due to the increase in the number of elderly people with spinal deformity and innovation of spinal instrumentation worldwide. Surgical results have improved due to innovations in spinal implants, 1 but bony fusion is necessary to prevent implant failure due to pseudoarthrosis. 2 Recombinant bone morphogenetic protein-2 (rhBMP-2) and rhBMP-7 have good efficacy for this purpose and are widely used to promote bony union. 3 However, recent reports have noted substantial off-label BMP use and a high rate of complications after spinal arthrodesis with BMP. 4 –6 The US Food and Drug Administration does not recommend BMP-2 and -7 use in cervical fusion surgery because of postoperative life-threatening respiratory complications. Therefore, a safe alternative is required for improving the rate and extent of bone fusion after spinal surgery.
Platelet-rich plasma (PRP) is blood plasma with concentrated autologous platelets and many growth factors and cytokines. Platelet-derived growth factor, transforming growth factor, insulin-like growth factor, epidermal growth factor, epithelial cell growth factor, and hepatocyte growth factor are present in platelets, 7 which especially contain platelet-derived growth factor, transforming growth factor, and insulin-like growth factor at high concentrations. 8 Therefore, PRP is likely to stimulate healing of bone and soft tissue.
Marx et al first described PRP for clinical use in dentistry, 9 and many oral surgeons now use PRP for bone defects. However, the efficacy of PRP for spinal arthrodesis remains uncertain. An effect of PRP on posterolateral lumbar fusion (PLF) was recently shown in a rat model, 10 and a clinical paper described the combined use of heterologous bone substitute and PRP in PLF. 11 However, this approach had several limitations, and further studies of the efficacy of combined local bone graft and PRP for treatment of spinal arthrodesis are required.
We first reported application of PRP in bone lengthening surgery in 2004. 12 The objective of this study was to investigate the efficacy of PRP on the rate and extent of bony union in PLF surgery through a comparison of combined local bone and PRP graft on the right side and autologous local bone graft only on the left side in a prospective cohort. In addition, we investigated the safety of PRP application in follow-up for 10 years.
Patients and Methods
From September 2003 to September 2004, we conducted a prospective study of PLF surgery for 33 consecutive patients with degenerative lumbar disease. This study was approved by the institutional review board of our hospital, and all patients gave consent for participation in the study. Exclusion criteria were patients with preoperative anemia (hemoglobin <11 g/dL and hematocrit <33%), a history of spinal surgery, severe osteoporosis, systemic disease, malignancy, chronic use of steroids or nonsteroidal anti-inflammatory drugs, renal failure with artificial dialysis, and collagen disease with steroid use, such as rheumatoid arthritis. We excluded 4 patients with vertebral fracture, tumors, pyogenic spondylitis, and an indication of multiple levels of lumbar fusion. Therefore, 29 cases (male: 11, female: 18, mean age: 63.3 ± 8.6 years) were enrolled in the study. All patients had spinal canal stenosis with mild degenerative spondylolisthesis at L4/5. Diabetes mellitus (DM), smoking habit, and alcohol intake were also evaluated as factors that may have an impact on bone union. Preoperative fibrinogen and platelets in serum and PRP were also measured. The Japanese Association Score was used to evaluate the clinical outcome. 13
The endpoints for evaluation were the area and mean density of bone fusion after PLF surgery on computed tomography (CT) at 2 weeks and 3, 6, and 12 months after surgery. For definition of successful fusion, we also evaluated the segmental range of motion under 5° on lateral flexion-extension radiographs with no radiolucent zones surrounding the pedicle screws on CT, 14 as well as continuous fusion mass formation between transverse processes on CT. For 10-year follow-up, all patients underwent plain radiography, CT, and magnetic resonance imaging at an outpatient clinic for evaluation of clinical symptoms and adverse events.
PRP Preparation
A total of 400 mL of whole blood from each patient combined with 56 mL of citrate phosphate dextrose solution (2.51 g/L sodium dihydrogen phosphate, 26.30 g/L sodium citrate, 3.27 g/L citric acid, 23.30 g/L glucose) in a sterile bag was drawn on the day before surgery. This blood sample was centrifuged at 200g for 15 minutes at 1500 rpm (Kubota 9800 Centrifuge, Kubota, Tokyo, Japan) to yield 2 separate layers: red blood cells and autologous plasma with buffy coat. After the autologous red blood cells were eliminated, autologous plasma, along with the buffy coat between the 2 layers, was collected. This was centrifuged again at 560g for 15 minutes to precipitate platelet pellets on the bottom of the bag. After the supernatant was removed, pure PRP (about 15 mL) was obtained. This fraction was stored at 21°C with shaking to prevent platelet aggregation until use during surgery.
Surgery
Open instrumented PLF was performed for all patients. A longitudinal skin incision of the lumbar spine was performed and the lamina and bilateral transverse process at L4 and L5 were exposed. The spinal canal was decompressed with laminectomy, and bilateral pedicle screw (6.5 mm in diameter and length 40 mm) insertion at L4 and L5 and 6.0 mm diameter titanium alloy rod placement were performed. For bone graft, the milled lamina and spinous process bone were divided into 2 equal parts (10 g each) for use as autologous bone grafts. Volumes of 12 mL of PRP and 2 mL of calcium gluconate (Calcicol, Dainippon Pharmaceutical, Osaka, Japan) and 5000 IU human thrombin (Mitsubishi Pharma Corp, Tokyo, Japan) were mixed with one part of the local bone. After decortication, local bone only on the left side (control side) and local bone with PRP on the right side (PRP side) were grafted in PLF. After irrigation and insertion of 2 drainage tubes, the skin was closed. After surgery, patients were allowed to walk on postoperative day 2, after removal of the drain tubes.
Measurement of the Area and Mean Density of Bone Fusion on CT After PLF Surgery
Tiff images with the same window level and width were extracted from coronal CT images of 1 mm slices of lumbar spine stored in the hospital DICOM database. All fused area and absorption pixels of grafted bone between the transverse process at L4 and L5 in PLF surgery using CT slices were automatically calculated in the grafted bone area using ImageJ software (Figure 1). High pixels of pedicle screws were excluded. Bone absorption was used instead of bone density 15 because bone absorption is more accurate without screw halation. Low bone absorption is considered to indicate a process of solid bony fusion. Calculation of an accurate fusion mass volume would be ideal, but volume analysis may be inaccurate at a surgical site with an implant, even with use of a detailed 1-mm slice from CT. Therefore, we evaluated both bone area and bone density in this study. To assess interobserver error, measurements were evaluated independently by 2 spinal surgeons who were blinded to the operative procedures and PRP side. The intraclass correlation coefficients in this analysis were 0.96 for the grafted bone area and 0.95 for bone absorption, and both were highly significant.

Postoperative course of posterolateral fusion between L4-5 on CT coronal images: (A) Two weeks after surgery; (B) Three months after surgery; (C) Six months after surgery. The right side with a bone graft with PRP achieved bony fusion. (D) Twelve months after surgery. Bilateral posterolateral fusion was complete. All panels show an AP view; therefore, the left side of each panel shows the right side of the patient.
Statistical Analysis
Averages are presented as the mean ± standard deviation (SD). An unpaired t test, repeated-measures ANOVA, and Tukey test were used to test differences between groups, with P < .05 considered to be significant. SPSS statistics 22 software was used for all calculations.
Results
All patients had improved symptoms after surgery, with the Japanese Association Score score improving from 15.9 ± 4.6 preoperatively to 26.0 ± 3.3 at 1 year after surgery (a recovery rate of 79.2 ± 18.0%). There was no postoperative sciatica related to PRP use in all patients. In blood tests, the platelet count was 227.2 ± 53.2 (×103) and serum fibrinogen was 293.8 ± 55.3 mg/dL. In PRP, the platelet count was 1759.9 ± 762.0 (×103) and fibrinogen was 259.5 ± 54.3 mg/dL. This indicated that platelets in PRP were concentrated by 7.74-fold, which is almost the same as that in a previous report. 16 There were no anemic patients preoperatively, and no need for intra- or postoperative blood transfusion, although 400 mL of whole blood was collected from each patient before surgery.
An illustrative case of a 63-year-old male is shown in Figure 1. This case shows earlier bony union on the PRP side than on the control side. Fusion area measurements of 58 regions on CT in all patients are shown in Table 1 and Figure 2. The average area on the PRP side was significantly wider at 3 and 6 months after surgery (Table 1, P < .05) and the PRP/control ratio was significantly higher at 3 and 6 months, compared to that at 2 weeks (Figure 2, P < .05). At 12 months after surgery this ratio was still high, but there was no significant difference in fusion area between the sides.
Time Course of the Bone Fusion Area on Coronal Computed Tomography Imagesa.
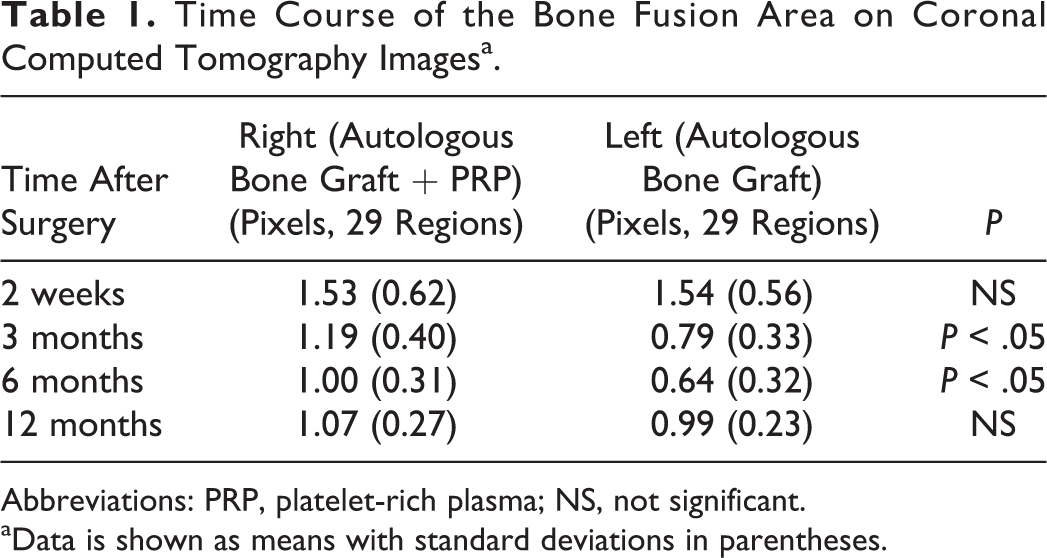
Abbreviations: PRP, platelet-rich plasma; NS, not significant.
aData is shown as means with standard deviations in parentheses.
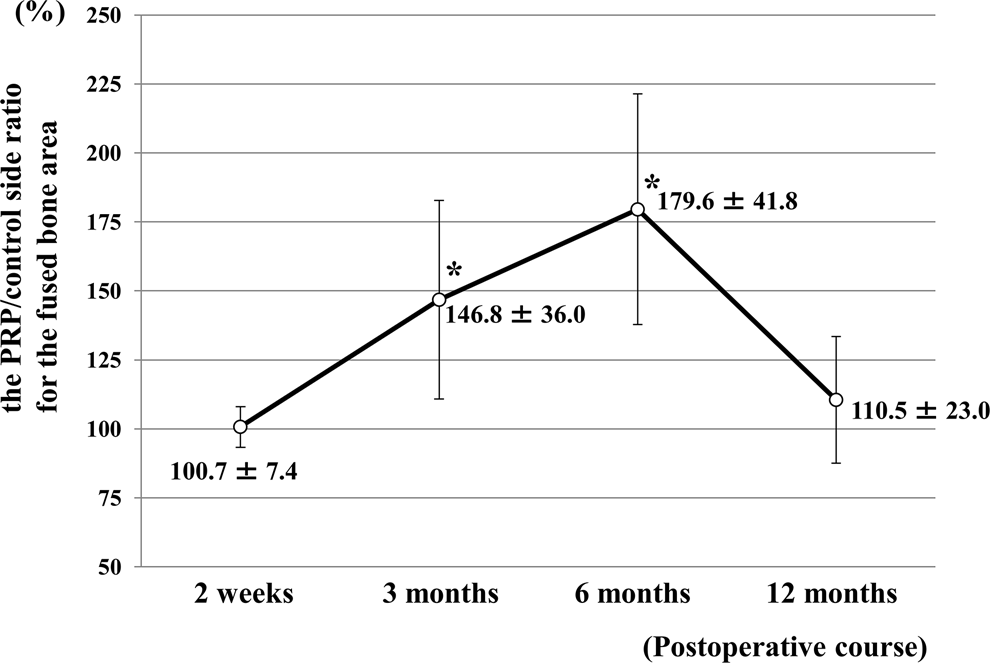
Time course of the PRP/control side ratio for the fused bone area. Fused bone areas on the PRP and control sides were almost the same at 2 weeks after surgery. At 3 and 6 months after surgery, this area was significantly wider on the PRP side than on the control side with autologous bone graft only (*P < .05). At 12 months after surgery, the area on the PRP side was still wider, but with no significant difference between the sides.
Results for bone absorption of 58 regions are shown in Table 2 and Figure 3. The average absorption on the 2 sides was the same in the grafted bone area. Absorption was significantly lower on the PRP side at 3 and 6 months after surgery (Table 2, P < .05) and the PRP/control ratio was significantly lower at 3 months (P < .01) and 6 months (P < .005), compared to that at 2 weeks (Figure 3). There was no significant difference in absorption between the 2 sides at 12 months after surgery.
Time Course of Bone Absorption on Coronal Computed Tomography Imagesa.
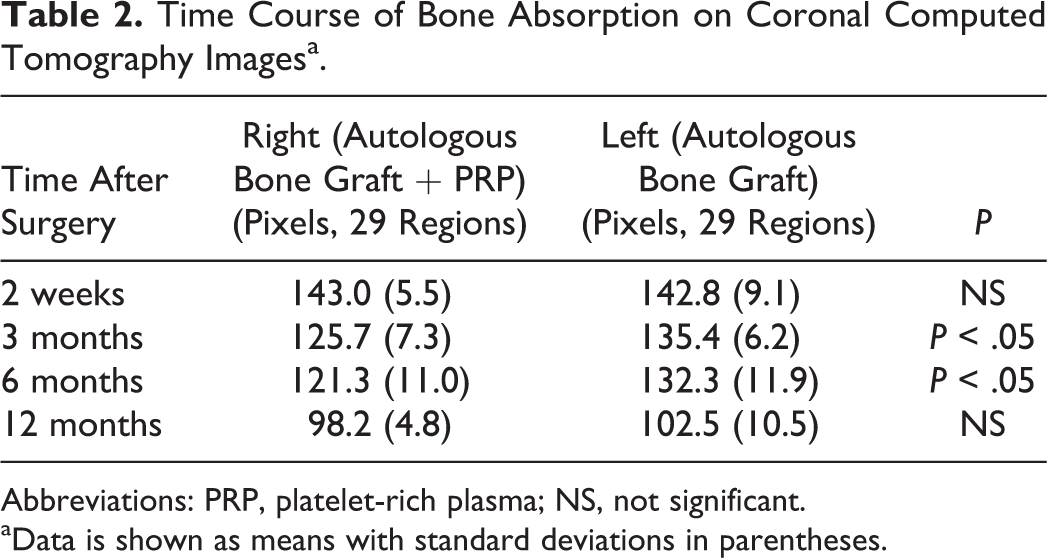
Abbreviations: PRP, platelet-rich plasma; NS, not significant.
aData is shown as means with standard deviations in parentheses.
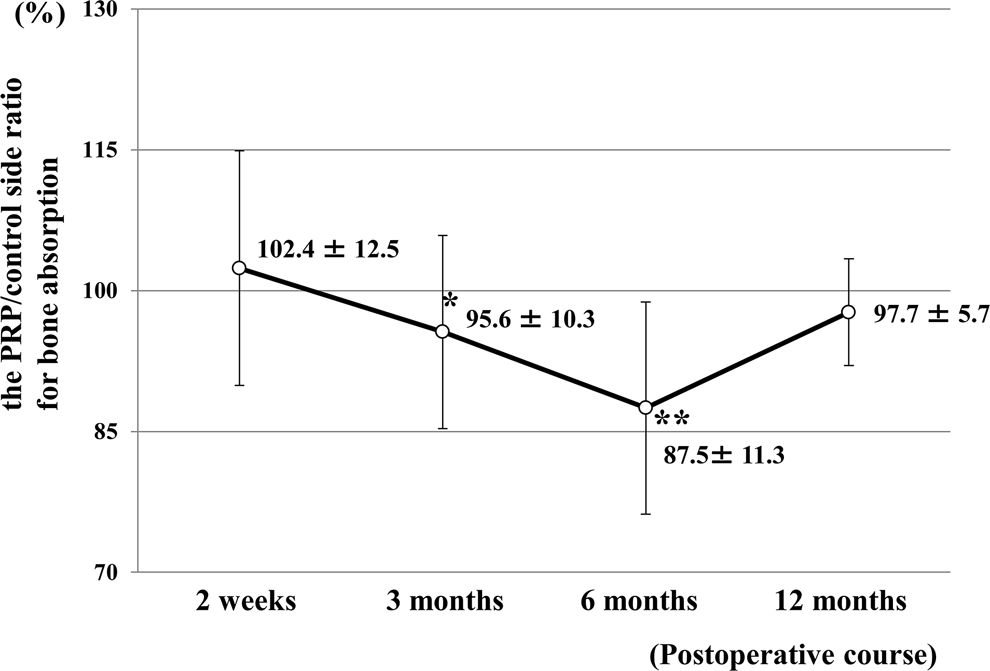
Time course of the PRP/control side ratio for bone absorption. The rates of bone absorption on the PRP and control sides were almost the same at 2 weeks after surgery. At 3 and 6 months after surgery, there was significantly less bone absorption on the PRP side than on the control side with autologous bone graft only (*P < .01, **P < .005). At 12 months after surgery, bilateral bone absorption did not differ significantly.
Five patients (17%) had DM, 9 (31%) were smokers, and 6 (21%) consumed alcohol. There were no significant differences in the fusion area and bone absorption on CT in patients with and without DM, smokers and nonsmokers, and patients who did and did not drink alcohol.
At final follow-up at over 10 years after surgery, bony union after PLF at L4/5 was fully achieved on plain radiographs and CT in all cases (fusion rate: 100%). There was no reoperation case with any lumbar symptoms. There were no adverse symptoms and events related to PRP, including seroma, and no massive bone formation or deep infection on magnetic resonance imaging.
Discussion
Growth factors and BMPs can achieve a faster union rate compared to autograft in femoral bone union in rats, rabbits, and rodents. 17 Clinical use of BMPs also shows acceleration of bone formation, and this has resulted in extensive use of BMPs in spinal fusion surgery in the United States. 3,18 However, unexpected aggressive bone formation, inflammatory problems such as soft tissue swelling, pain/radiculopathy, vertebral bone osteolysis, and a risk of cancer are also often reported with use of BMPs. 19 –23 In a study of adverse events reported to the Food and Drug Administration after use of rhBMP-2 in spinal surgery, Woo found that 370 of 834 cases (44.4%) required revision surgery or other invasive interventions such as tracheostomy. 23 The high cost of BMPs is another concern. 24 In contrast, PRP can be made and used for less than US$30 in this study. Thus, use of PRP in spinal arthrodesis is of interest due to its safety and lower cost. In this study, PRP application with autologous local bone was cheaper than use of a bone substitute. Preoperative blood drawing and storage of PRP after preparation are time-consuming for patients and medical staff, but the cost benefit and safety may overcome these concerns. If the preoperative preparation is a burden, PRP can also be made in the operating room after general anesthesia, but we prefer to use a preoperative approach to ensure that the PRP is produced appropriately.
In a previous study of combined use of bone and PRP for lumbar arthrodesis, Hee et al conducted a prospective investigation of the effects of autologous growth factors in instrumented transforaminal lumbar interbody spinal fusion (TLIF). 25 The outcomes of 23 patients treated with TLIF who received PRP made from 450 mL of whole blood were compared with those of earlier patients who underwent TLIF without PRP. Faster bone fusion occurred with the combined PRP graft, but plain radiographs did not show an overall increase in fusion; however, this may be because it is difficult to evaluate spinal fusion on plain radiographs only. 14 There may also have been bias in the comparison of prospective and historical cohort data, and therefore further investigation of the efficacy of PRP is needed.
In a randomized controlled study of one-level posterior lumbar interbody fusion (PLIF) with instrumentation in 2011 in 19 cases treated with an autologous bone graft with a carbon and PEEK (poly-ether-ether-ketone) cage and 19 cases treated with PRP, Sys et al concluded that PRP gave no substantial improvement in clinical and radiographic outcomes. 26 However, only a small amount of PRP from 54 mL of blood was used because of the narrow space of the intervertebral cage in PLIF surgery. In addition, an iliac crest autologous bone graft was used in both groups, which may be the optimal bone graft. 11,27 As indicated by Sys et al, the rate of pseudoarthrosis in instrumented one-level PLIF with iliac bone use for relatively healthy patients is generally extremely low, and therefore this study design may have had difficulty in establishing a difference in efficacy of autologous bone graft with and without PRP for lumbar arthrodesis. Use of an iliac crest bone graft has recently decreased in spinal fusion surgery due mainly to donor site pain in approximately 25% of cases, 28,29 with 6 of 38 cases (16%) in the Sys et al study complaining of donor site pain for several months. Therefore, iliac bone graft alone seems not to contribute to solid fusion after long spinal fusion surgery for aging patients. There were no adverse events or deterioration in clinical and radiographic outcomes in the 19 patients treated with PRP in the study by Sys et al.
Interbody spinal fusion with an intervertebral cage is more common than PLF in clinical settings, 30,31 but radiographic evaluation of intervertebral fusion can be difficult. 14 In this respect, PLF may be advantageous for evaluation of changes in bony fusion in spinal arthrodesis. Regarding the efficacy of PRP for arthrodesis in PLF surgery, Kamoda et al recently found that PRP promoted bone formation after PLF in a rat model, suggesting that PRP can be used for shortening the time required for bone union. 10 However, further studies in humans are needed because bone formation in rats occurs more quickly than in humans. The current prospective study showed that PRP does accelerate bony union after PLF surgery.
The reported fusion rate for uninstrumented PLF with iliac crest bone graft is 45%, which suggests that instrumented PLF has an advantage of increased fusion. 32 However, the fusion rate of 83% to 88% in instrumented PLF with autograft including iliac bone or local bone is still insufficient for clinical use. 32 –34 In the current study, we obtained a 100% fusion rate after instrumented PLF surgery with local bone and PRP graft. Tarantino et al 11 have also shown the efficacy of PRP for early bony fusion in PLF surgery, based on measurement of the bone density in the fusion area using CT in 20 cases treated with instrumented PLF surgery with a cancellous bone substitute soaked with PRP and saline on the right and left sides, respectively. The combined use of bone substitute and PRP gave excellent results for early bone fusion for 6 months after surgery. However, the SP-Block Soft BS7E (25 × 50 × 30 mm) cancellous bone substitute (Tecnoss, Torino, Italy) used in the study is not widely used worldwide, and thus Tarantino et al suggested that a future study is required to analyze the effects of PRP combined with autologous local bone graft.
A further difference with the current study is the inclusion of patients with one-level to 4 multilevel PLFs in Tarantino et al, 11 with 25% of the patients having lumbar body fractures. These conditions are likely to influence the fusion course after PLF surgery. Also, only axial CT views were used, which makes it difficult to observe bony fusion between the transverse processes. The advantages of the current study include the limitation to single-level PLF at L4/5 for degenerative lumbar disease, local bone usage without bone substitute, analysis of CT scans in detailed 1-mm slices in the coronal view, investigation of smoking and alcohol intake, and a long follow-up period of over 10 years. These factors permitted demonstration of the efficacy of PRP for lumbar arthrodesis surgery in a prospective cohort study. The effect on bone fusion with and without PRP did not differ significantly at 1 year after surgery, but the acceleration of bony union with combination use of PRP and autologous local bone achieved faster bone fusion, which is useful for prevention of implant failure after instrumented surgery.
In 10 years of follow-up, none of our patients had infection or pain related to the L4/5 PLF surgery. The antibacterial effect of PRP and increased tissue repair and remodeling occur through promotion of leukocyte chemotaxis. 35 An effect on inflammatory pain relief may also occur because PRP augments the inflammation cascade. 36 PRP also reduces pre- and postoperative pain in knee and shoulder joints. 37 –39 We note that PRP was applied only at the PLF site and after surgical decompression of the spinal canal and nerve root in this study, and therefore it may be inappropriate to conclude that the postoperative reduction of pain and antibacterial effect are due to PRP. However, the absence of adverse events in symptoms and radiographic evaluation for a long time after PLF surgery is encouraging for clinical use of PRP in spinal arthrodesis surgery.
Limitations
This study is limited by the small number of cases, and this might have influenced the finding that smoking did not have a significant effect on bony fusion in this study. Calculation of the sample size beforehand with a power of 0.95 and effect size of 0.4 indicated a requirement for a total sample size of about 30 cases with 60 regions. This was proposed with the approval of our institutional review board, based on analysis of bone formation at 2 sites in each patient. Second, the necessary minimum amount of PRP has yet to be defined. In this study, a total of 400 mL of whole blood from each patient was used, but this may be too much, especially in elderly patients. Fortunately, no patients were anemic or needed blood transfusion after surgery, but a further investigation is needed to determine the minimum PRP amount required for each fusion level. Third, the study design using each patient as their own “control” has advantages. However, the occurrence of fusion on one side of a motion segment may have an effect on the contralateral side. One side fuses and makes the whole motion segment more rigid, which may have an impact on fusion on the contralateral side. Furthermore, some PRP might have flowed from the PRP side to the control side after the decompression procedure. These factors may explain the absence of a difference in bony fusion at 12 months, despite early fusion on the PRP side. The advantages of the current study were the single level of lumbar fusion, inclusion of cases with surgery for degenerative disease excluding trauma and collagen disease, and use of prospective long-term follow-up data collected at one institute.
Conclusion
This is the first study to show that local application of PRP combined with autologous local bone had a positive impact on early fusion in lumbar arthrodesis, with no adverse events over 10 years. These results suggest that this approach is a safe and low-cost autologous option for spinal fusion.
Footnotes
Acknowledgments
The authors thank Ms Marie Miyazaki and Ms Erika Takano in Nagoya University, for their assistance throughout this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.