
Abstract
Study Design:
Retrospective analysis of consecutive case series.
Objective:
To introduce a novel method of stabilizing the cranium using bivector traction in posterior cervical fusions.
Methods:
A retrospective review of 50 consecutive patients undergoing instrumented posterior cervical arthrodesis was performed. All patients had at least 3 levels of subaxial fusion using the bivector traction apparatus. Patients’ demographic data was recorded for the following: pre- and postoperative cervical lordosis, pre- and postoperative cervical sagittal vertical alignment (cSVA), and intraoperative complications from pin placements.
Results:
A total of 50 patients were studied. There were 31 females and 19 males. The mean age at the time of surgery was 49 years (range 35-79). A mean 5.8 levels were fused. The most common levels fused were C2-T3 in 14 patients followed by C2-T2 in 7 patients. In no case did the surgeon or assistant have to scrub out to adjust the alignment. The mean pre- and postoperative cervical lordosis was −6.0° and −10°, respectively (P = .04). The mean pre-and postoperative cSVA was 30.5 mm and 32 mm, respectively (P = .6). There were no complications related to placement of the Gardner-Well tongs.
Conclusion:
The bivector traction is an easy, safe, and effective method of stabilizing the head and obtaining adequate cervical sagittal alignment.
Keywords
Introduction
Obtaining optimal alignment of the cervical spine in the sagittal plane is of upmost importance as it affects the overall sagittal alignment. The 2 major modes of stabilizing the cranium during posterior cervical surgery are through the use of a Mayfield headholder or Gardner-Wells tongs. The disadvantages of the Mayfield tongs include the need to secure 3 pin sites and necessity for the surgeon to scrub out to adjust the tongs intraoperatively. Scalp laceration and other Mayfield complications are not uncommon. 1 –3 In this article, we present a novel method of stabilizing the head using a Gardner-Wells tongs with a bivector-directed force to ensure optimal head positioning and cervical alignment during posterior cervical fusions. To the best of our knowledge, this is the first description in the literature of this technique being utilized in posterior cervical fusions.
Materials and Methods
A retrospective review of 50 consecutive adult patients undergoing a posterior cervical fusion was performed. Approval was obtained from the Washington University in St Louis Institutional Review Board prior to study. All patients had at least 3 levels of fusion in the subaxial spine. Patients who had a Smith-Peterson osteotomy, had pedicle subtraction osteotomy, or had application of spinous process cables were excluded from the study. Patient demographic data was recorded for the following: pre- and postoperative cervical lordosis, pre- and postoperative cervical sagittal vertical alignment (cSVA), and intraoperative complications from pin placements. Since this study was designed to demonstrate the feasibility of maintaining and/or improving cervical lordosis intraoperatively, patient functional outcomes and follow-up data were not included. Differences between preoperative and postoperative values were analyzed using the Student t test. A P value of <.05 was considered statistically significant.
The Technique
After anesthesia is induced and the patient is intubated, Gardner-Wells tongs are placed on the patient’s head. The pins are aligned with the external auditory canals 1 cm superior to the pinnae. Care is taken that the tongs are in the coronal plane of the patient’s head in order to ensure that the patient’s head is not rotated toward one side once placed in traction.
Once the tongs have been placed, the patient is then carefully rolled from the stretcher onto the Jackson table and placed in the prone position. Pads are placed to support the torso just inferior to the clavicles and to support the pelvis. In cases of significant cervical spine instability the patient can be flipped with a cervical collar in place. Once the patient has been placed on the operating table, 2 traction ropes are attached to the Gardner-Wells tongs (Figure 1). One of the ropes is the “flexion” rope and the other is an “extension” rope. Generally 15 pounds of weight are initially placed on the flexion rope, allowing the patient’s head to remain stable in a position most conducive to skin sterilization and exposure. At this point the patient’s positioning can be completed, arms secured at the sides, and the cervical collar removed. Before surgical drapes are placed, the surgeon notes that the patient’s head is not rotated away from midline.
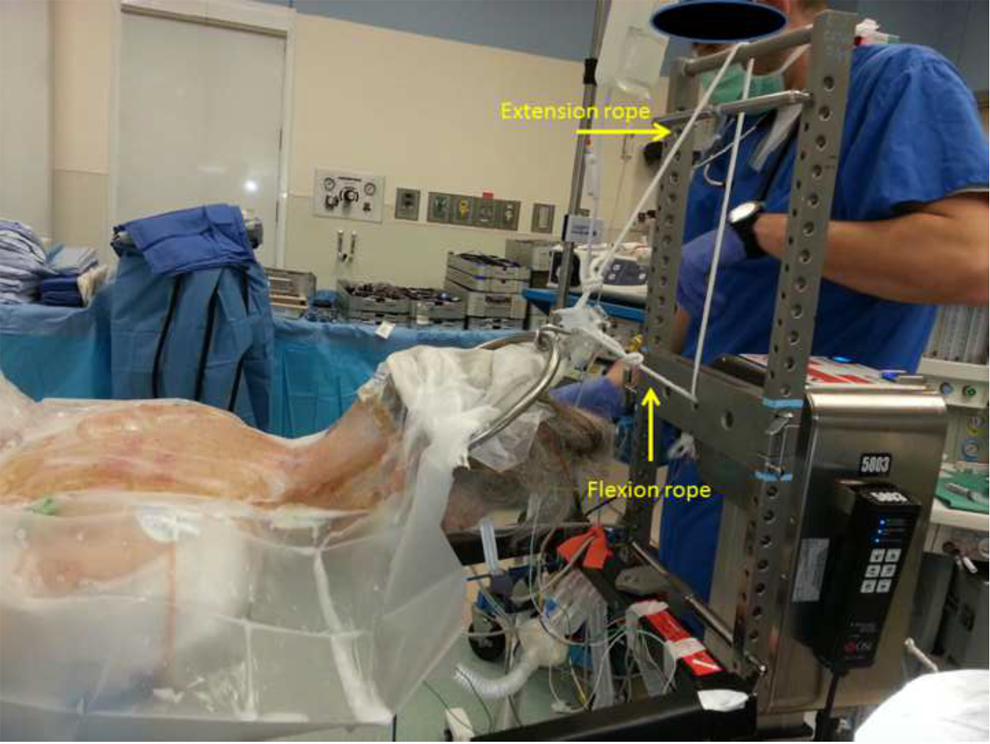
Representative illustration of the Gardner-Wells bivector traction apparatus used during a posterior cervical fusion. The head is supported by 15 pounds of weight attached to flexion and extension ropes.
The flexion rope runs with a single vector in the cephalad direction, from the Gardner-Wells tongs through the head of the Jackson table frame and then off of a pulley. The extension rope travels from the tongs over an “H-frame” placed on top of the Jackson table, creating an additional extension vector. The amount of maximal extension can be adjusted in 2 ways: by raising the height of the bar over which the extension rope travels and by minimizing the distance between the top of the tongs and the head of the table.
During exposure, decompression, decortication of the facets, and placement of screws into the posterior cervical spine, the patient’s head is maintained on the flexion rope. Flexion allows for easier facet decortication, as well as foraminal decompression. During screw placement, it allows for more oblique trajectories. Once rod measuring and contouring begins, the traction is then switched to the extension rope. In order to change the traction, the surgeon grasps the Gardner-Wells tongs with the sterile drapes and states that he/she has a secure hold. The anesthesiologist then transfers the traction weight from the flexion rope to the extension rope and confirms that the weight is in place before the surgeon removes his/her hand from the tongs. The surgeon can further adjust the patient’s cervical extension by pulling on the tongs. Fluoroscopy is then used to confirm the alignment of the head prior to final securing of the rods and completion of arthrodesis.
Results
A total of 50 patients were studied. There were 31 females and 19 males. The mean age at the time of surgery was 49 years (range 35-79). A mean 5.8 levels were fused. The most common levels fused were C2-T3 in 14 patients followed by C2-T2 in 7 patients. The mean pre- and postoperative cervical lordosis was −6.0° and −10°, respectively (P = .04). The mean pre-and postoperative cSVA was 30.5 mm and 32 mm, respectively (P = .6). Thirty-seven patients had previous anterior cervical fusions and 7 patients had autofusions from diffuse idiopathic skeletal hyperostosis. Fifteen pounds was found to be adequate to stabilize the head in all cases, keeping the neck stable and still during decompression, as well as instrumentation. Switching the weight from one rope to the other typically takes only a few seconds. In no case did the surgeon or assistant have to scrub out to adjust the alignment. There were no complications related to placement of the Gardner-Well tongs.
Discussion
The Mayfield head clamp is the most frequently used head clamp system for stabilization of the head and neck in cervical spine surgery. Despite its widespread use, pin loosening with scalp laceration and other Mayfield failures have been reported. 1 –3 In the authors’ personal experience, the concern for Mayfield loosening is greatest during force application to the spine during insertion of instrumentation or deformity correction. Furthermore, in circumstances where the alignment or position of the neck needs to be adjusted intraoperatively, the surgeon or assistant must scrub out to perform this task risking contamination, further pin loosening and adding operative time.
This study demonstrates the feasibility and easy application of the Gardner-Wells tongs for stabilizing the head and maintaining or improving cervical sagittal alignment. The flexion rope allows for an easy exposure with minimal soft tissue retraction. This is especially useful in patients with short and thick necks and also in patients with multiple neck folds. The extension rope allows for the recreation or enhancement of cervical lordosis. Any adjustment to the position of the neck can be easily accomplished without having to break scrub. In this study, there were no complications from placement of the Gardner-Wells tongs. More important, the overall sagittal alignment of the cervical spine was not compromised with this traction technique. Although this technique is easy to apply, one must always remember to change to the extension rope when introducing the rod so that the patient is not instrumented in a flexed position.
There are limitations to the study may have implications for its interpretation. First, this is a retrospective study and therefore is subject to the weakness of a retrospective analysis. Second, patient-reported outcomes were not collected on our patients, even though the goal of the study was to assess radiographically. Last, the amount of extension needed for each patient in this study was determined based on their preoperative standing cervical lateral X-rays. For patients with normal preoperative cervical lordosis, all attempts were made to ensure it was maintained. In patients with straightening of cervical lordosis or kyphosis, attempts were made to introduce some cervical lordosis based on lateral fluoroscopy prior to insertion of rods. One can manually increase the amount of extension by raising the extension bar on the Jackson table, thereby increasing the extension moment. Ideally, the exact amount of cervical lordosis needed should be determined based on the overall spinal alignment with attention to spinopelvic parameters, thus representing a limitation of this study.
Conclusions
The bivector traction is an easy, safe, and effective method of stabilizing the head and obtaining adequate cervical sagittal alignment. It obviates the need for the surgeon to scrub out to adjust the head. It allows the case to start with the neck in a flexed position, which is optimal for foraminal decompression, and then switch to an extended position for the arthrodesis. We believe that this is a reasonable alternative to using Mayfield headrests.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.