
Abstract
Study Design:
Cadaver study.
Objective:
To determine the bone density of lumbar vertebral anatomic subregions. Bone mineral density (BMD) is a major factor in osseous fixation construct strength. The standard region for implant fixation of the spine is the pedicle; however, other regions may be more viable options with higher bone quality.
Methods:
Using computed tomography images, the spine was digitally isolated by applying a filter for adult bone. The spine model was separated into 5 lumbar vertebrae, followed by segmentation of each vertebra into 7 regions and determination of average Hounsfield units (HU). HU was converted to BMD with calibration phantoms of known BMD.
Results:
Overall mean BMD in vertebral regions ranged from 172 to 393 mg/cm3 with the highest and lowest BMD in the lamina and vertebral body, respectively. Vertebral regions formed 3 distinct groups (P < .03). The vertebral body and transverse processes represent one group with significantly lower BMD than other regions. Spinous process, pedicles, and superior articular processes represent a second group with moderate BMD. Finally, inferior articular process (IAP) and lamina represent a third group with significantly higher BMD than other regions.
Conclusions:
Standard lumbar fusion currently uses the vertebral body and pedicles as primary locations for fixation despite their relatively low BMD. Utilization of posterior elements, especially the lamina and IAP, may be advantageous as a supplement to modern constructs or the primary site for fixation, possibly mitigating construct failures due to loosening or pullout.
Introduction
Osteoporosis is an emerging problem worldwide with over 10 million people diagnosed with the disease. 1 One quarter of women older than 65 years and half of those older than of 80 years suffer from the disease in the United States. 2 Surgical indications for these populations are on the rise, with half of women and a fifth of men diagnosed with osteoporosis and older than 50 years requiring spine surgery. 3 One such indication that is becoming more frequent as the population ages is lumbar spinal stenosis, 4,5 which is often treated surgically with decompression and fusion, supplemented with internal fixation, such as pedicle screws and rods. 6 However, the osteoporotic patient is at higher risk of facing construct failure due to reduced bone quality since screw fixation strength relies greatly on bone mineral density (BMD). 7,8 Low BMD has been identified as a major factor in spine construct failure, such as pedicle screw loosening and pullout, especially at the ends of long constructs and in the setting of a deformity correction. 9
Several modifications have been devised to help address the issue of spinal construct failure in the setting of low BMD, including cement augmentation of fenestrated pedicle screws and splaying of the screw tips. 10 Another strategy involves using different types of fixation, such as sublaminar wires and hooks (laminar, pedicle, or transverse process), that rely on the posterior element strength rather than the vertebral body strength. Coe et al 7 showed increased tensile load to failure of laminar hooks over transpedical screws in osteoporotic bone. Improved strength of laminar hooks in these patients may be related to a relative strengthening of the posterior elements in the elderly patient. Niosi and Oxland 11 reported a shift in the transmission of load from the anterior column to the posterior elements of the vertebra. This shift may translate into more sclerosis around the posterior elements in response to the added stress, subsequently increasing the relative strength of those posterior elements. Wang et al 12 demonstrated that the posterior column provides approximately twice the contribution as the anterior column to lumbar vertebral BMD; however, relative contributions of the anterior body and posterior elements to mechanical performance of pedicle screws still remain unknown. A better understanding of these properties may refine and streamline instrumentation strategies to minimize the risk of screw loosening, hardware pullout, and construct failure which leads to reoperations and persistent disability.
The traditional measurement of relative bone density is performed using a dual-energy X-ray absorptiometry (DEXA) scanner. DEXA has been shown to correlate with fracture risk and efficacy of treatment. 13 However, most DEXA scans accessible to patients are 2-dimensional (length and width) and lack depth measurement, confounding the calculation of density (amount/[length × width × depth]). Estimations of depth may be applied for a more accurate measure of density. Complex geometries of the posterior vertebral anatomy further confound the BMD measurement from DEXA. Computed tomography (CT) is an imaging modality that has emerged as a solution to the measurement of complex anatomy and is a process that is commonly performed during routine clinical care. 14 In a comparison of DEXA and CT, Schrieber et al 15 have shown the CT modality to be an effective tool to measure BMD. In their study, average BMD and t-scores measured from DEXA scans across the vertebral body were compared to average Hounsfield units (HU) of similar areas. Significant correlations were observed between HUs, t-scores, and BMD. Pemler et al 16 and Anderst et al 17 have also shown the CT modality to be an effective tool to measure BMD. These researchers have outlined a method for mapping and reporting BMD for different anatomical regions of the vertebra through CT imaging and correlation with HU.
The specific aims of this study were to quantify the differences in bone density at selected anatomical regions of the vertebrae in effort to characterize the mechanical advantages and disadvantages of each region for placement of surgical hardware.
Methods
Study Specimens and CT Imaging
Three cadaveric spinal columns were imaged and analyzed for the present study (2 male ages 35 and 70 years; 1 female age 90 years). All 5 lumbar vertebrae were analyzed from each for a total number of 15 vertebrae. High-resolution helical CT scans were conducted on all specimens. All scans were performed on the same scanner (GE Lightspeed VCT) with the same imaging parameters (64 slice, 512 × 512 pixel resolution) to reduce interspecimen variability.
CT Image Segmentation
CT scans were postprocessed using commercial medical image processing software (Mimics; Materialise, Leuven, Belgium) in the following manner. The lumbar spine (L1-L5) was digitally isolated from surrounding tissue by applying a preset thresholding filter for adult bone to the CT scans. Using this thresholding as well as manual segmentation, the lumbar spine model was separated into 5 separate vertebrae, followed by segmentation of each vertebra into 7 predefined anatomic regions as displayed in Figure 1. When visible, bone sutures were utilized as anatomic boundaries between vertebral subregions. Average BMD measurements of each vertebral region were recorded. The same team member segmented all the vertebral regions to reduce variability. This team member segmented the L1 and L5 transverse processes, pedicles, inferior articular processes, and superior articular processes twice from 2 of the study specimens to assess the inherent variability in the manual segmentation protocol. The difference between the first and second measurement were expressed in terms of percent of their mean value for comparison across anatomical regions.
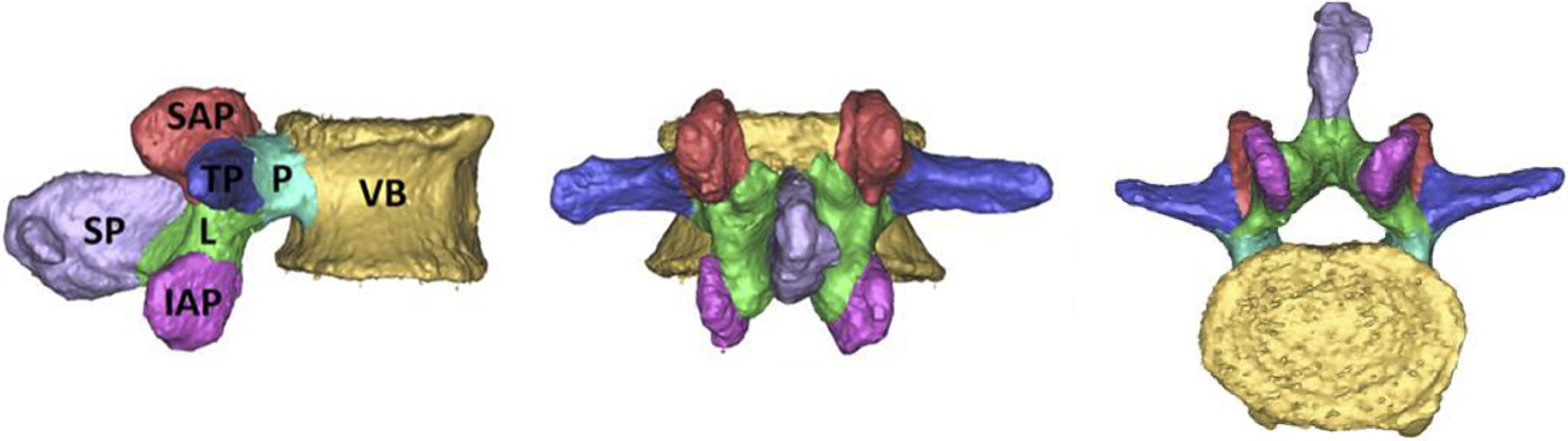
Sagittal, posterior, and cranial views of a representative 3-dimensional model displaying the vertebra segmented in the various regions analyzed in this study. VB, vertebral body; P, pedicles; TP, transverse processes; L, lamina; SAP, superior articular processes; IAP, inferior articular processes; SP, spinous process.
Conversion From HU to BMD
Conversion from HU to BMD units was performed in accordance with the guidelines previously described. 16,17 In brief, HUs were converted to BMD through a calibration equation derived from CT scans of tissue surrogate materials (Electron Density Phantom, Model 62; CIRS) using the same scanning protocol as that used for all specimens. Specifically, “phantoms” of 200 and 800 mg/cm3 were utilized to account for the known range of BMD in various anatomic locations of the cervical spine as determined by previously. 17 These “phantom” blocks have been previously reported to produce reliable calibration formulas between HU and BMD. 16
Outcome Measures and Statistical Analysis
The primary outcome measure from densitometry was averaged BMD for each vertebral subregion. One-way analysis of variance was conducted to determine any significant differences in BMD of the vertebral regions, with alpha equal to .05.
Results
The results of our HU to BMD analysis produced a linear calibration equation between the BMD measures of 200 and 800 mg/cm3 and HU measures between 300 and 1000 HU. Our calibration resulted in a relationship of 1 mg/cm3 for every 0.78 HU.
On average, we observed a 1.5% difference in BMD measures between the first and second measures of the same anatomical region. The largest percent discrepancy between the repeated measures was 3.0% and the standard deviation of the percent discrepancies was ±0.7%.
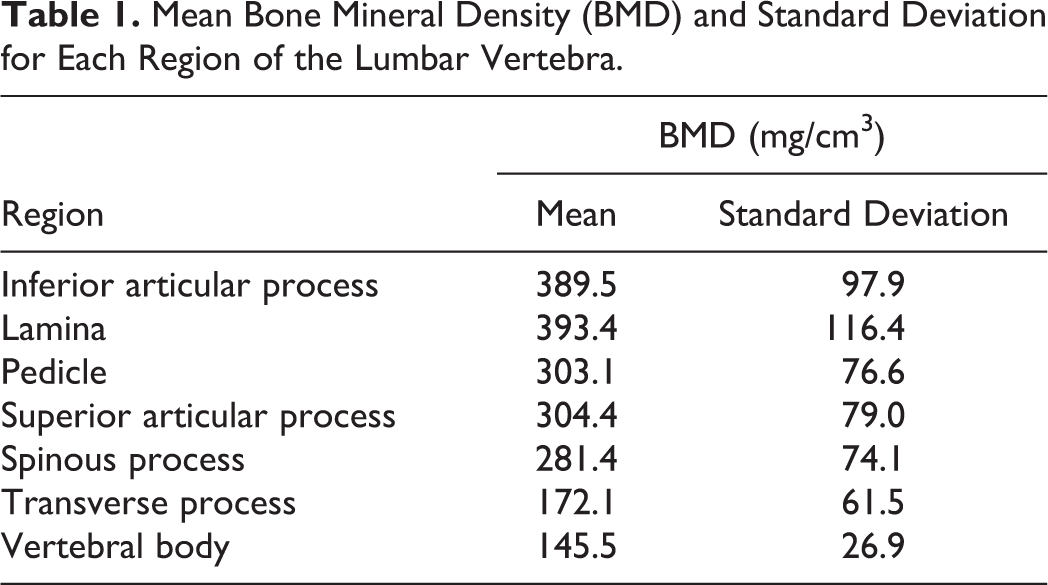
Overall mean BMD in vertebral regions ranged from 172 to 393 mg/cm3 as shown in Figure 2. The highest BMD was observed in the lamina and lowest observed in the vertebral body as displayed in Table 1. Vertebral regions demonstrated BMD in 3 statistically distinct (P < .03) groups as shown in Figure 2. The vertebral body and transverse processes; the spinous process, pedicles, and superior articular processes; and the inferior articular process and lamina.
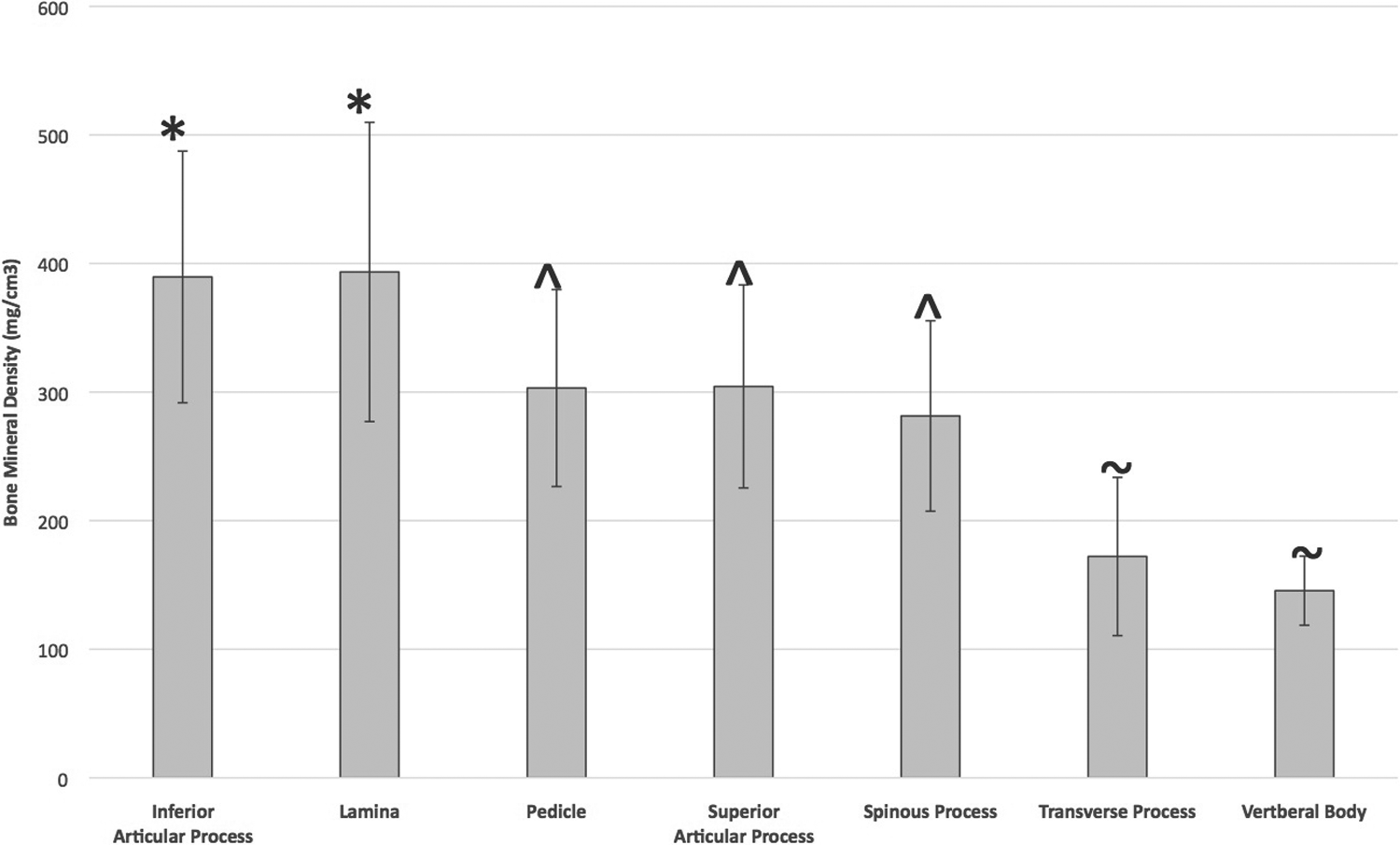
Bone mineral density for each region of the vertebrae. All data is represented as mean ± standard deviation. Means not connected by the same annotation symbol (*, ⁁, or ∼) are statistically significantly different from one another.
Mean Bone Mineral Density (BMD) and Standard Deviation for Each Region of the Lumbar Vertebra.
There was no statistical difference (P = .72) in variability between the L1 or L5 vertebrae used for the analysis and no difference (P = .54) in variability between the anatomical regions measured. Figure 3 is a visual representation of the BMD for each specimen at the lamina and pedicle by lumbar vertebra. The cadaveric specimen from the 35-year-old male consistently had the densest laminar and pedicle bone compared with the 70-year-old male and 90-year-old female specimens.
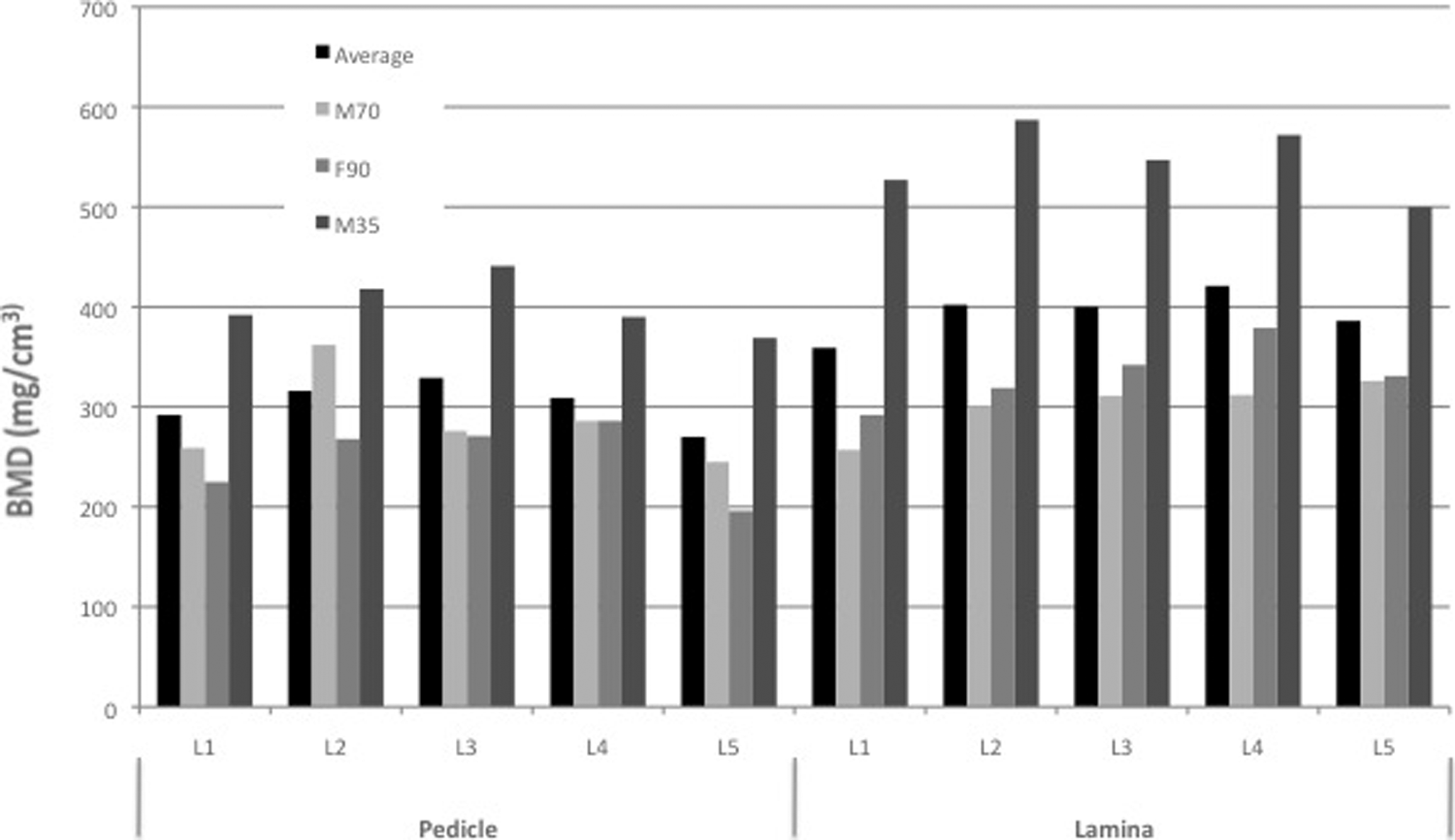
Bone mineral density of pedicles and lamina. Specimens are labeled with M for male or F for female, followed by 2 digit age.
Discussion
This study reported the bone quality of clinically relevant anatomic regions of the lumbar vertebra. The pedicles exhibited significantly lower BMD compared with other regions of the posterior spine; specifically, the lamina and inferior articular processes.
A large majority of these results are corroborated by Anderst et al 17 who reported a similar analysis on the cervical spine. Anderst et al 17 found that the cervical vertebral body contained statistically lower BMD compared with a majority of the posterior elements; however, the pedicles were found to exhibit the highest bone quality followed by the lamina and lateral masses. In comparison, the lamina and inferior facets were the densest regions in our study of lumbar vertebrae. This suggests that while the distribution of BMD between the anterior vertebral body and posterior elements may remain consistent between cervical and lumbar regions, the distribution within the posterior elements may be different.
These conclusions have led our team to develop the following research questions: Are there areas of the posterior elements that represent optimal opportunities for implant fixation? Are these disparities between the pedicles and other posterior elements consistent with age and/or disease populations? Common lumbar fusion currently uses the vertebral body and pedicles as primary locations for osseous fixation. We have demonstrated that these anatomic regions have a relatively low density. Thus, utilization of the posterior elements of the lumbar spine, especially the lamina and inferior articular processes, may be advantageous either as a supplement to traditional trans-pedicle fixation or possibly to serve as the primary site for fixation.
We observed a statistically significant difference between the region evaluated for bone quality (vertebral body) and the region utilized for posterior fixation (pedicle). This result suggests that the standard procedure of determining spine BMD by DEXA scans may have limited efficacy in surgical planning due to the inability to assess the variation of BMD within the vertebrae. Wang et al 12 demonstrated that the vertebral body, while contributing two-thirds of the vertebral volume in the lumbar spine, on average, only contributed one-third of the BMD, with the posterior elements contributing the remainder. Additionally, they found weak correlation between BMD in the posterior elements and the vertebral body (r = 0.34, P < .0001), further suggesting that DEXA alone is an insufficient predictor of lumbar bone quality throughout subregions of the vertebrae, such as the pedicle. Our results further quantify the variation of BMD within the posterior elements, with BMD highest in the lamina and lowest in transverse processes, indicating a possible need to evaluate specific anatomic regions when bone quality is in question. CT may be more valuable than standard DEXA when assessing BMD of specific anatomic regions prior to lumbar spinal fusion, particularly in patients with existing poor bone quality. Further research is needed in this area to validate the use of the vertebral body as a predictor for pedicle bone quality.
Limitations of this study included sample size and specimen age. Even with the current sample size, however, trends with statistical significance were observed. These overall trends were consistent within each evaluated specimen. Additionally, the age of the specimens used had a wide range (35-90 years) and were not specifically osteoporotic, which is the patient demographic we are interested in. Also, although cadaveric specimens were utilized for testing, all were fresh frozen, which aimed to avoid any artifacts from tissue preservation. In order to address some of these limitations as well as apply the results of this study to further research, several directions of future work can potentially be pursued. A larger set of patient data, rather than cadaver specimens, can be utilized to validate the findings of this initial study in the clinical setting. The larger sample size will allow grouping of populations by factors such as osteoporosis, gender, and age. Additionally, the findings of this study may be useful for design of future fixation constructs tailored to patients with poor bone quality. Finally, software innovation to develop image processing algorithms that translate CT scans into BMD by vertebral subregion may be beneficial for preoperative planning to assess viability of traditional spinal fusion with pedicle fixation.
In conclusion, we report that bone mineral density of the lumbar spine was shown to differ significantly within the anatomical subregions of the lumbar vertebrae. The posterior elements, specifically the lamina and articular processes, exhibited superior bone quality compared with the pedicles. The results may be utilized for surgical planning and development of extrapedicular fixation strategies and technologies. However, further clinical data regarding the density of lumbar vertebral segments are needed to better understand treatment options and fixation strategies, particularly in patients with osteoporosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Connor Telles is a consultant for Spine Art USA and Misonix Inc. Jeremi Leasure is in association with DePuySynthes, Medtronic, Stryker, Exactech, Spineart, SI-Bone, ConforMIS, Kinamed, Cotera, RJI Orthopaedics, and Neptune Orthopaedics. Dimitriy Kondrashov is in association with AO Foundation, Spineart, SI-Bone, and LifeSpine.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided by The Taylor Collaboration and the SF Orthopaedic Residency Program.