
Abstract
Study Design:
Retrospective cohort study.
Objective:
To evaluate for racial disparities in elderly patients having undergone lumbar spinal stenosis surgery.
Methods:
The US Medicare Provider Analysis and Review database (records from 2005 to 2011) was used to identify patients over the age of 65 years, diagnosed with lumbar spinal stenosis, and having undergone lumbar laminectomy or fusion surgery. Blacks were compared to Whites in both unmatched and propensity score-matched populations. The data was analyzed with univariate (χ2 and Wilcoxon rank sum tests for unmatched comparison, and McNemar exact and signed rank sum tests for matched comparison) and multivariate models.
Results:
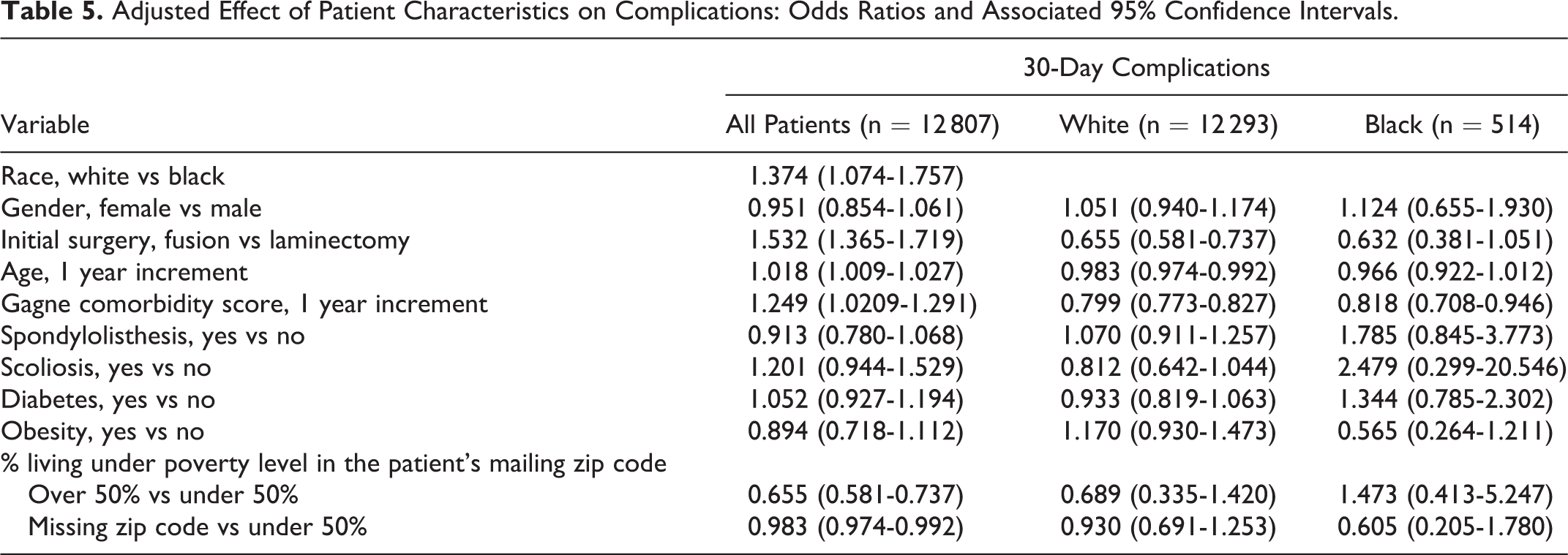
Query of the data resulted in a study sample of 12 807 patients; 514 (4.0%) were identified as Black and 12 293 (96%) as White. Blacks were less likely to be discharged home (42.4% vs 58.9%, P < .0001) and had lower repeat operation rates (6.81% vs 11.5%, P = .0009); both remained significant in the propensity score-matched comparison. Finally, Blacks experienced more postoperative complications, higher median Medicare costs, but lower out-of-pocket expenses (P = .0113). Blacks had higher rates of diabetes (33.7% vs 21.5%, P < .0001) and obesity (9.92% vs 6.85%, P = .0074), when compared to Whites, but these comorbidities did not significantly affect odds of 30-day complications.
Conclusions:
Black patients having undergone lumbar spinal stenosis surgery were more likely to have received fusion at initial operation, had shorter pre- and postoperative follow-up intervals and displayed variances in discharge disposition. Reasons for these differences are not entirely understood; however, educational and socioeconomic factors and possibly ethnic/cultural biases may have contributed. Racial disparities in health care continue to be identified and should be further explored in order to eliminate them.
Introduction
Lumbar spinal stenosis is the most common preoperative diagnosis for spine surgery in the elderly population. 1,2 The condition is characterized by spinal canal narrowing and nerve root impingement due to herniation of nucleus pulposus, arthritic osteophytes, facet joint arthritis, and/or hypertrophy of the ligamentum flavum. Surgical treatment consists of decompressive laminectomy with or without fusion and has become commonplace in our society.
Several studies have assessed spine surgery for spinal stenosis on a national level, but few have focused on patients over 65 years of age. 1 –4 Moreover, the aforementioned studies reported on complications, readmission rates, postoperative length of stay (LOS), and reoperations, without much regard to the impact of racial disparities on said outcomes.
Two prior studies by our group reported disparities in outcomes based on race and insurance status. 5,6 Both studies utilized data from a Medicaid-based national database, the Thomson Reuter’s MarketScan. The objective of the current study is to evaluate for racial disparities in elderly patients having undergone lumbar spinal stenosis surgery.
Methods
Data Source
The Medicare Provider Analysis and Review (MedPAR) database records (from years 2005 to 2011) were queried. The database contains health care utilization and claims for individuals older than 65 years, individuals younger than 65 years with disabilities, and individuals with end-stage renal disease. MedPAR also contains claims for inpatient hospital and skilled nursing facility stays. The data represents cumulated services and payments for an entire hospital stay.
Patient Selection
Patients older than 65 years of age were identified in the MedPAR. The age criterion was chosen to ensure at least 1-year look-back for all patients. The index hospitalization is defined as the first hospitalization with a concurrent primary diagnosis of lumbar stenosis (International Classification of Diseases, Ninth Edition [ICD-9] codes 724.02, 724.02, 724.09) and primary laminectomy (ICD-9 code 03.09) or lumbar fusion (ICD-9 codes 81.06, 81.07, 81.08). Other inclusion criteria were age as the sole reason for Medicare entitlement, and Black or White race. The race variable represents the race identified on the claims. Patients who died during the index hospitalization, those who had cancers (ICD-9 codes 140-239) within 6 months prior to diagnosis, and those who had undergone back surgery (eg, laminectomy, fusion, or refusion—ICD-9 codes 81.36, 81.37, 81.38, respectively) within 1 year prior to the index hospitalization were excluded.
Explanatory Variables
Explanatory variables comprised patient demographics (age, gender), comorbidities, follow-up time (prediagnosis and follow-up months), the presence of other spine conditions (spondylolisthesis, scoliosis), diabetes and/or obesity, and the percent of people living under poverty level in the patient’s mailing address zip code. Comorbidities were cumulated over hospitalizations occurring within 6 months prior to diagnosis including the index hospitalization. Comorbidity was captured through the Gagne index. The Gagne index is a comorbidity score that was developed to include Charlson and Elixhauser conditions. 7 The Gagne index was found to have better performance than the latter 2 comorbidity scores individually. 7 Comorbidities were factored into the analysis as the 6-month average Gagne score. Prediagnosis follow-up months were calculated as the difference between the date of Medicare coverage initiation and the date of the diagnosis hospitalization. Postdischarge follow-up was calculated as the difference between the discharge date of the index hospitalization and the date of death (for those who died during the years we have data for) or the date of the last follow-up day (December 31, 2011; the last day for which we obtained data). To evaluate whether the patient had diabetes mellitus, we screened the 25 fields of ICD-9 codes for the presence of 250.xx and V77.1. For obesity, we screened for ICD-9 codes 278, 278.0, and V77.8. To assess the percent population living under the poverty level in the patient’s neighborhood, we used census data compiled by the Zip Atlas (http://zipatlas.com/us/zip-code-comparison/population-below-poverty-level.htm).
Outcome Variables
Index Hospitalization Days and Pay
The index hospitalization days represented the total LOS, while index hospitalization pay represented payments by Medicare. In addition, we analyzed total out-of-pocket expense as the sum of co-insurance and deductible. All payments were adjusted to according to the medical component of the consumer price index. The consumer price index can be accessed through the US Bureau of Labor Statistics website (www.bls.gov).
Complications
The complications we screened for included neural, cardiac, pulmonary, pulmonary embolism, deep vein thrombosis, infection, and wound complications. Our team used these complications in prior studies. 8 –10 The ICD-9 codes for these complications are listed in Table 1. A patient was categorized as having complications if any of the aforementioned conditions were found in any diagnosis field at the index hospitalization or at subsequent hospitalizations. Hospitalizations that occurred within 30 days and 90 days after the index hospitalization discharge were reviewed to identify 30-day and 90-day complications, respectively. We assessed the odds of 30-day complications based on diabetes and obesity (among other patient characteristics) in an attempt to identify a correlation between baseline patient characteristics and complications.
Complications and ICD-9 Codes.
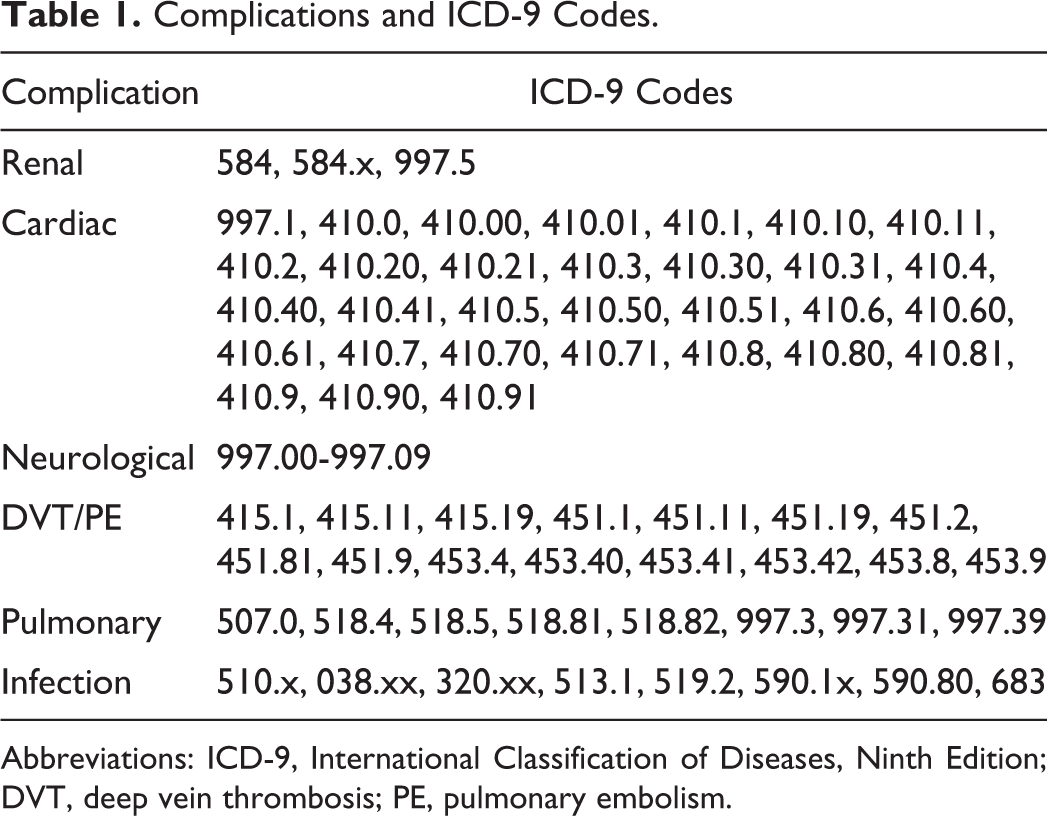
Abbreviations: ICD-9, International Classification of Diseases, Ninth Edition; DVT, deep vein thrombosis; PE, pulmonary embolism.
Repeat Operations
We screened for all postoperative inpatient encounters for claims of laminectomy, fusion, and refusion (ICD-9 codes 81.36, 81.37, 81.38, respectively) during the entire follow-up period for each patient. We also searched all procedure fields.
Survival Time
Survival was measured as the number of months between the date of index surgery discharge and the date of death for those who died in the years for which data was available. The remaining patients were followed until the end date of the study (December 31, 2011) and were censored. Survival-months reflected the difference between the discharge date of the index surgery and the censoring date.
Propensity Score Matching
The propensity score matching method consists of matching individuals in 2 groups with similar or close propensity scores. 11 The aim is to balance the groups on observed confounders. The propensity score was computed using race as the outcome variable and included all characteristics as covariates using a logistic regression model. Black patients were matched to White patients in a one-to-one fashion using 0.2 times the standard deviation of the propensity scores as the caliper. The greedy macro was used to perform the matching. 12 This technique has been used in other studies analyzing racial disparities. 13 –15
Covariate balance before and after matching was assessed using P values and absolute values of the standardized difference. The P value was obtained from 2-sample comparison with nonparametric rank sum test for continuous characteristics and χ2 tests for categorical characteristics. A standardized difference threshold of 0.1 (over 0.1) was used to evaluate for covariate imbalance. 16
Statistical Analysis
Patient characteristics and outcomes were summarized using mean, median, standard deviation, and interquartile range for age, Gagne score, follow-up months, index hospitalization days, and Medicare pay. Frequency counts and percentages for female sex, initial surgery type, discharge location, 30-day readmission, 30-day mortality, 30-day wound infection, repeat operation, and complications were reported.
Comparative analyses of both unmatched and matched groups were performed.
For unmatched comparisons, χ2 test was utilized for categorical outcomes (discharge location, 30-day readmission, 30-day mortality, 30-day wound infection, repeat operation, and complications) and Wilcoxon rank sum test for continuous outcomes (index hospitalization days and Medicare pay) in univariate modeling. Log-linear methodology was used to analyze continuous variables and logistic regression for categorical variables in multivariate modeling.
For matched comparisons, McNemar test was used for categorical outcomes and the Wilcoxon signed-rank test for continuous outcomes. For multivariate modeling, continuous outcomes were analyzed with linear mixed models in which the matched pair was included as a random effect. Categorical outcomes were analyzed with conditional logistic regression.
All tests were 2-sided, using a significance level of .05. Multiple tests were accounted for by adjusting the P values to control for the false discovery rate (FDR) in each table using Benjamini and Hockberg’s approach. 17,18 SAS 9.4 (SAS Institute, Inc, Cary, NC) was used for all data preprocessing and data analyses.
Results
Patient Characteristics
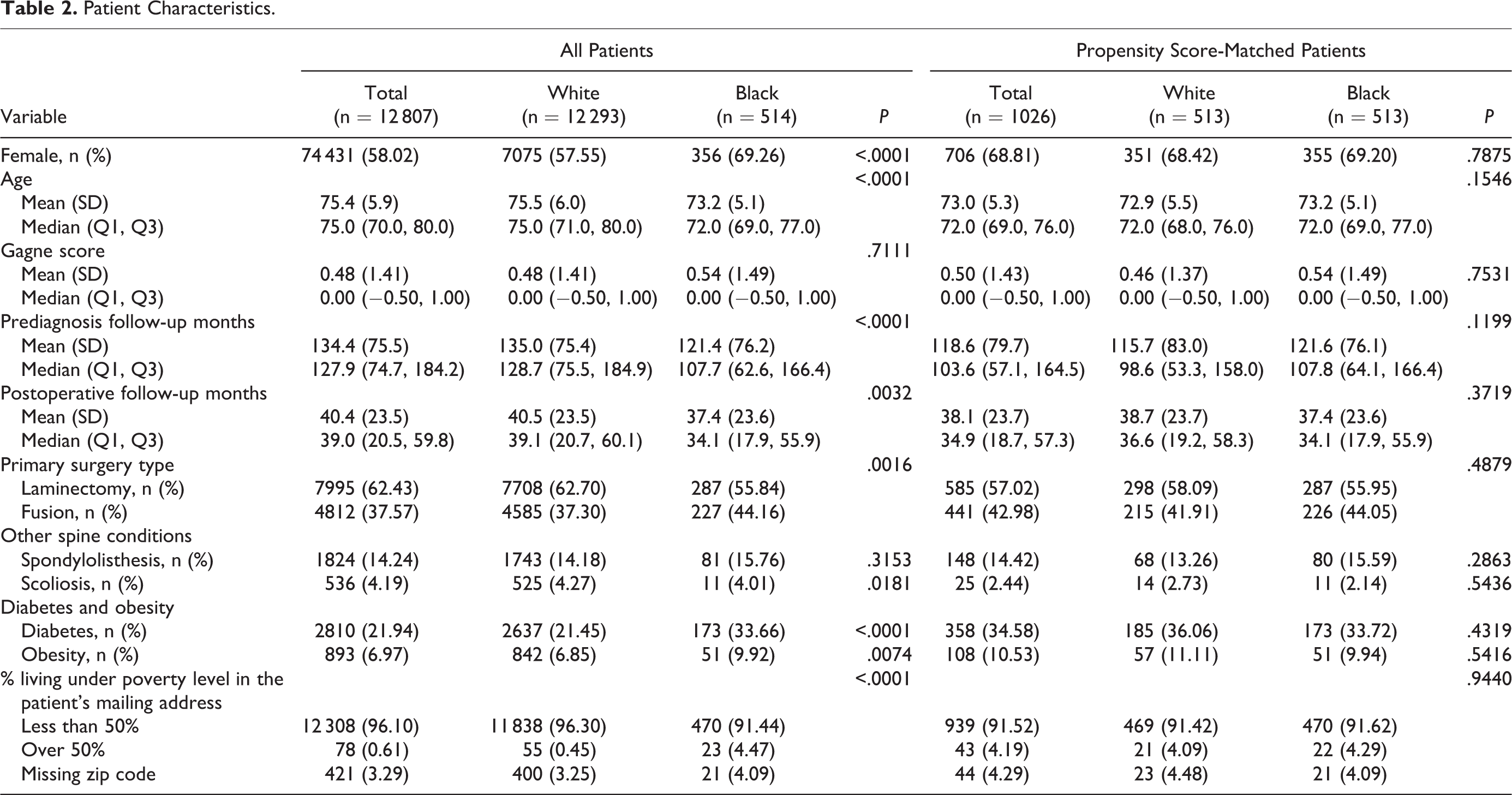
A total of 12 807 patients were identified and analyzed (Table 2). Of these, 514 patients were Black (4.0%) and 12 293 were White (96%). Mean age was 75 years. Females made up 58.0% of the cohort. Black patients were more likely to be women and to be younger when compared to White patients. Black patients had fewer median prediagnosis follow-up months (107.7 vs 128.7, P < .0001) and postsurgery follow-up months (34.1 vs 39.1, P = .0032). Blacks were more likely to have received fusion as the initial surgical procedure (44.16% vs 37.30%, P = .0016). Blacks had higher rates of diabetes (33.66% vs 21.45%, P < .0001) and obesity (9.92% vs 6.85%, P = .0074), as compared to Whites, but these comorbidities did not significantly affect odds of 30-day complications. Blacks also lived in poorer neighborhoods (P < .001). The propensity score matching method successfully provided comparative groups for all these variables.
Patient Characteristics.
Outcomes
Table 3 details outcomes for Black and White patients in our study sample. Blacks had significantly longer LOS during the index hospitalization (P < .0001), and this effect persisted after multivariate adjustment (Table 4) as well as after propensity score matching (Table 5). Blacks incurred higher median Medicare payout costs ($7360 vs $6594); however, this difference was not statistically significant after adjusting the P value for FDR or after propensity score matching. Blacks were less likely to have been discharged home (42.4% vs 58.9%, P < .0001) and more likely to have been sent to skilled nursing facilities (21.4% vs 14.3%, P < .0001) or inpatient rehabilitation services (20.2% vs 10.7%, P < .0001). This outcome measure remained statistically significant in the propensity score-matched analysis. Blacks had a lower overall repeat operation rate (6.81% vs 11.5%, P = .0009) and lower laminectomy repeat operation rate (3.31% vs 6.16%, P = .0079) versus Whites. These remained statistically significant with multivariate and propensity score matching adjustments. Finally, Blacks experienced more complications (in-hospital, 30 and 90 days after discharge) although this was not statistically significant in the matched cohort. Postoperative survival did not differ between the 2 races (see Figure 1).
Outcomes in All Patients in the Propensity-Score Matched Groups: Univariate Analysis.
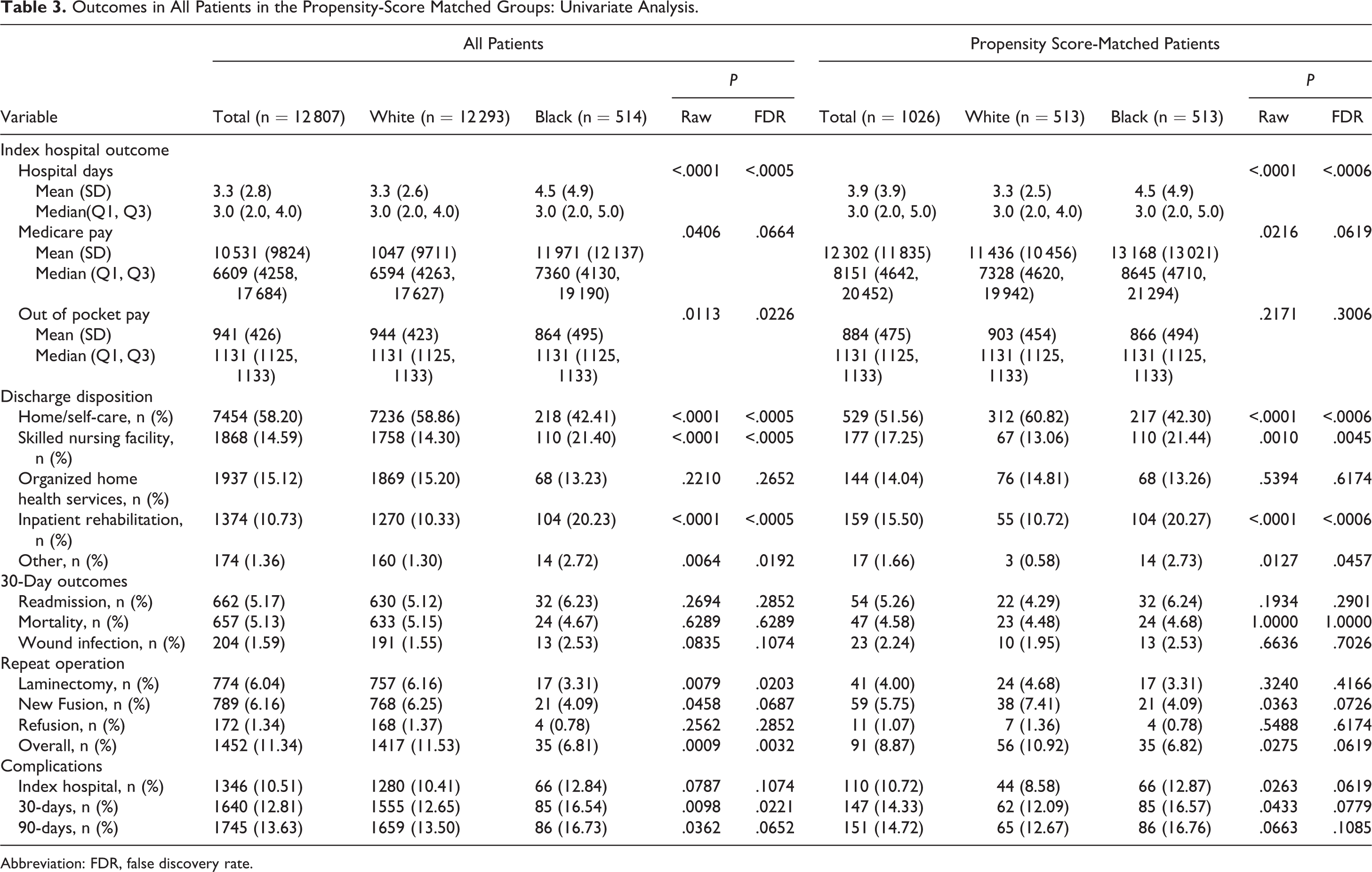
Abbreviation: FDR, false discovery rate.
Outcomes in All Patients and in the Propensity Score-Matched Groups: Multivariate Analysis.
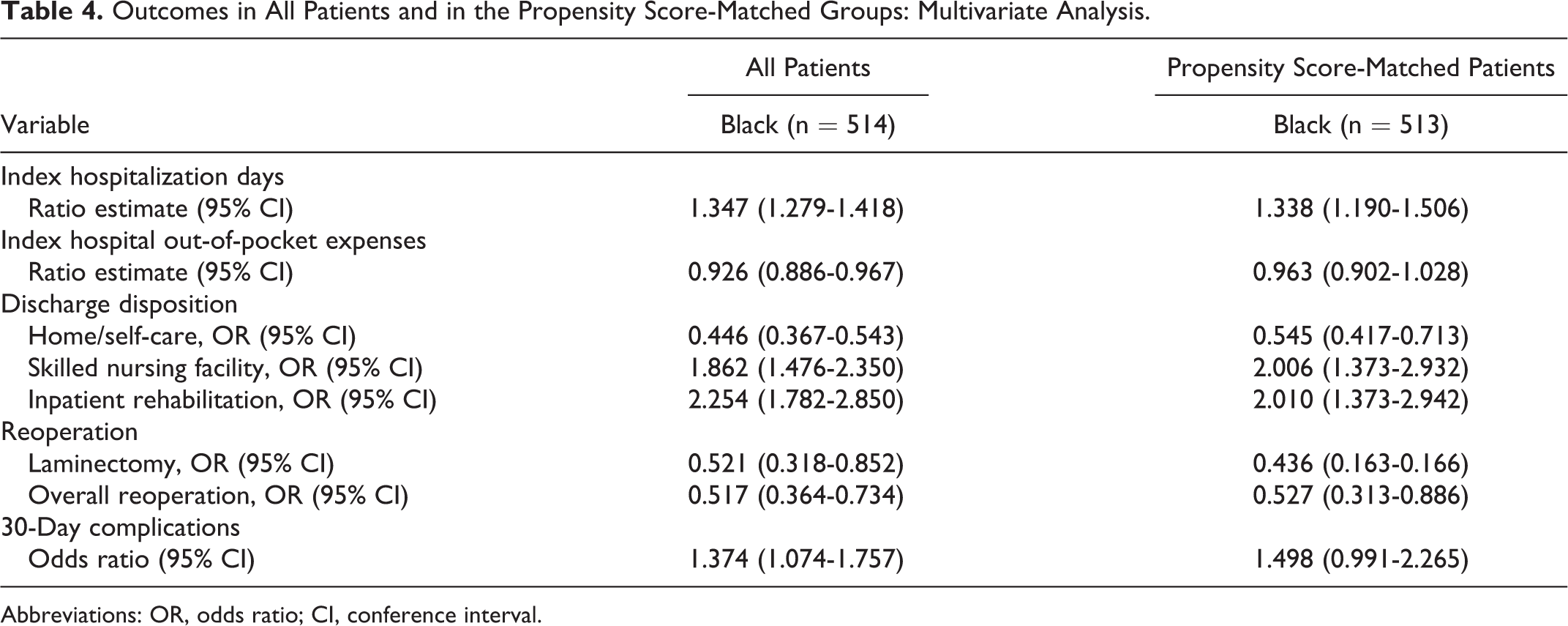
Abbreviations: OR, odds ratio; CI, conference interval.
Adjusted Effect of Patient Characteristics on Complications: Odds Ratios and Associated 95% Confidence Intervals.
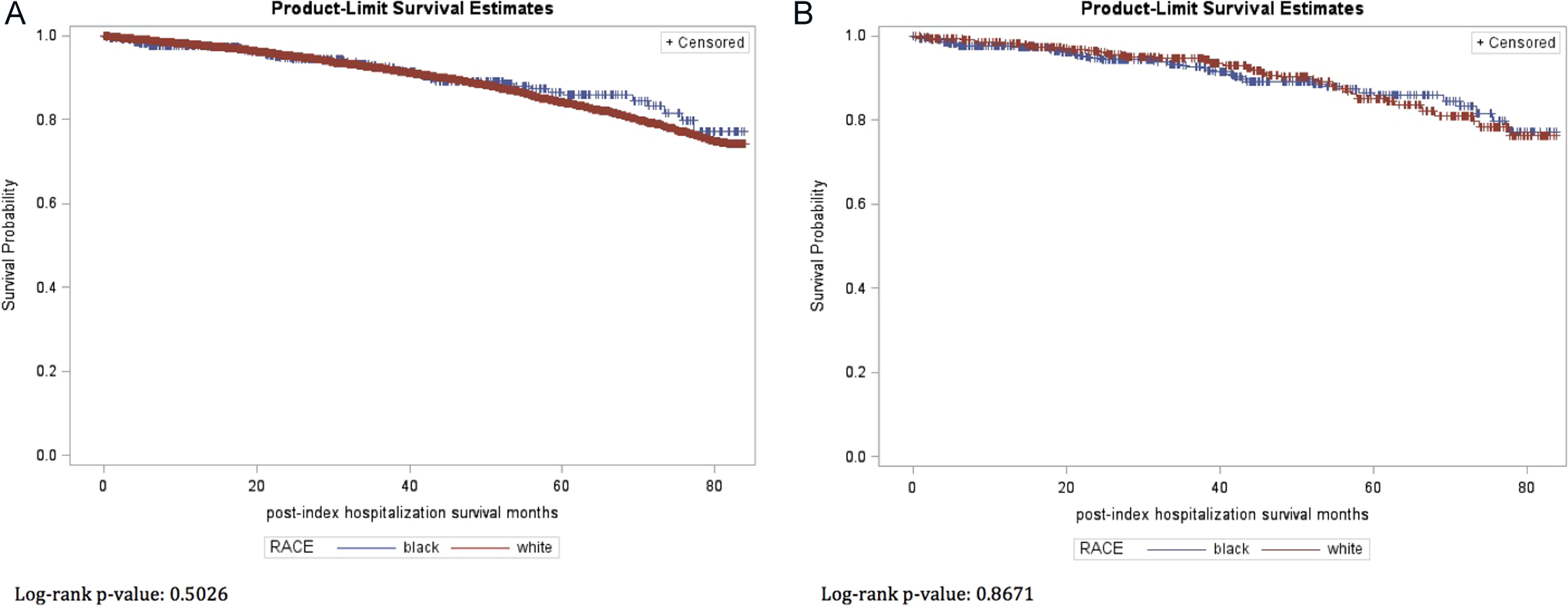
Survival curves for the overall Medicare-eligible elderly population (A) and the propensity score-matched patients (B) stratified by race.
Discussion
The study herein described sheds light on racial disparities among Black and White patients receiving lumbar spinal stenosis surgery in the United States. Significant differences in the initial type of surgery performed, discharge disposition, and rates of complications and readmissions were identified.
Racial inequalities have been described previously in various surgical interventions such as coronary artery bypass grafting, lung cancer resection, and arthroplasty. 7 –10 In a recent study, Singh and colleagues reported racial disparities in patients receiving total knee and hip joint arthroplasty, which included differences in 30-day hospital readmission and discharge disposition. 7 The authors of that study also highlighted the existence of racial and ethnic healthcare disparities in other countries.
Currently, while there may be an overall trend with respect to disparities in spine care, such an association has not yet been clearly defined. 11,12 There have been previous reports suggestive of a greater risk of morbidity and mortality among Blacks following spine surgery; however, these studies were not particularly conclusive. 11 A recent study analyzed the impact of race in the Spine Patient Outcomes Research Trial (SPORT). The SPORT was a prospective study by 13 centers in the United States performed between 2000 and 2005. 11 Analysis of the SPORT revealed that there were racial differences in quality of life outcomes (eg, SF-36 bodily pain, physical function, and Oswestry Disability Index), specifically, that Black patients had poorer measures than White patients receiving spine therapy regardless of the type of treatment offered. Interestingly, Blacks were less likely to be offered surgical intervention. However, the authors pointed out that though such differences do not necessarily translate to a current disparity in spine care in the United States. Furthermore, this was a post hoc analysis of the SPORT trial, which itself was not designed to assess racial inequalities and had fewer patients than the current study.
Schofield and colleagues suggested potential bias and discriminatory care among racial and ethnic groups receiving surgery in a recent meta-analysis. 12 The authors cited a number of studies that reported worse health care utilization and outcomes in Black patients: less likelihood to receive surgery, higher postoperative complications, longer LOS, poorer functional recovery, and mortality.
In prior studies, our group analyzed national trends in lumbar spinal stenosis surgery through the Thomson Reuters MarketScan. In one study, we reported that Blacks were more likely to have postoperative complications, longer LOS, higher hospital costs, and were prescribed fewer medications after surgery. 6 In a different article, we found that insured patients had significantly lower reoperation rates, were less likely to undergo fusion for reoperation, and had greater health care utilization (hospital days, outpatient services, medications, etc). 5
In the current study, we utilized Medicare data to assess and analyze the presence of racial disparities in elderly patients having undergone lumbar spinal stenosis surgery. The benefits of this analysis include its use of national data, large patient numbers, and uniform insurance coverage. In the study population, Blacks were younger, more likely to be women, and had shorter postsurgical follow-ups. Fusion surgery was more likely to be performed on initial intervention in Blacks. Blacks had worse outcomes in multiple measures, including repeat operations and discharge dispositions. Reasons for these racial disparities are likely multifactorial and may include discrimination, differences in education and socioeconomic status, ethnic and cultural biases, preferences regarding medical treatment and health care utilization, and comorbidities. Black patients had higher Gagne comorbidity scores. Although this metric failed to achieve statistical significance, it is reasonable to conclude that disease processes, such as diabetes and obesity (both of which were shown to be increased in Black patients), contribute to poorer surgical outcomes. Recent studies reported that Blacks have more undiagnosed rates of diabetes and obesity than Whites, specifically, that variances in glycemic markers (eg, A1c, glycated albumin, fructosamine, and 1,5-anhydroglucitol) do exist. 19 However, the clinical significance of these differences, in terms of risk of complications, has yet to be fully elucidated. Higher rates of diabetes and obesity in Black patients may be related to complications such as wound infections, but these factors did not affect 30-day complication rates in our study, regardless of race. These findings may have been affected by a failure to stratify 30-day complications into specific events. The current health care workflow is complex and it is likely that breakdowns are occurring at multiple levels. Future studies should seek to identify these areas of concern and address them prudently.
Limitations
This study was limited to information in the MedPAR database. The racial mix of 4% Black and 96% White is not representative of the racial mix of Blacks and Whites in the United States. It is also not possible to determine body mass index, glycemic marker levels, specific living situations, or long-term functional outcomes such as SF-36 and Oswestry Disability Index. Finally, there is a potential for coding errors when dealing with large national databases. All things considered, the large sample size (12 807 patients: 514 Black and 12 293 White patients) did allow for adequate data analysis of the issue at hand.
Conclusion
The authors identified racial disparities in elderly patients having undergone lumbar spinal stenosis surgery: Black patients had longer hospital stays, lower reoperation rates, and were more likely to be discharged to skilled nursing facilities and inpatient rehabilitation services (versus White patients). Potential studies could expand on our data to include all races and further stratify ethnicities and religious affiliations to determine if cultural and/or religious beliefs contribute to these disparities, respectively.
Footnotes
Authors’ Note
Beatrice Ugiliweneza had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.