
Abstract
Family has a major impact on adolescents’ mental health, influencing their emotional and behavioral well-being. This study aims to explore differences in family functioning between community and clinical adolescents and to investigate their perceptions. A mixed-methods approach was used, involving 80 adolescents with mental disorders and 612 non-clinical adolescents (53% girls, Mage = 14.86 years). The Youth Self Report (YSR) and the Family Adaptability and Cohesion Evaluation Scale (FACES IV) were administered. Ten participants from the community group and ten participants from clinical group were interviewed. Significant differences between the groups were found in all dimensions of YSR (p < 0.001), as well as in cohesion (p < 0.001), flexibility (p < 0.001), disengaged (p < 0.001), chaotic (p < 0.05), communication (p < 0.001), and satisfaction (p < 0.001). Family functioning was found to be a strong component in differentiating clinical and non-clinical adolescents (χ2 (8) = 60.38, p < .05); however, the only significant predictor was family satisfaction (β = −.09***). Consistent with quantitative findings, responsiveness and supervision emerged as the most common themes in interviews with non-clinical adolescents, while conflicts and authoritarian control were prevalent among clinical adolescents. These findings highlight the importance of fostering positive family dynamics to support adolescent mental health, suggesting directions for future interventions and research.
Introduction
Epidemiological studies have shown that mental health problems mostly have their first age of onset during adolescence (Essau et al., 2014; Solmi et al., 2022). Globally, one in seven youth experiences a mental disorder (UNICEF, 2021). Therefore, there is increasing attention on the factors that put adolescents at risk of developing mental health problems, with a specific focus on family functioning (Ortiz-Sanchez et al., 2023; Yöntem, 2019). Over the last few decades, the role of family functioning in the development of adolescents’ mental health problems has received increased attention in research, as it can predict both positive and negative outcomes (Buehler, 2020; Sander & McCarty, 2005). On the one hand, adolescents in functional families are less likely to develop mental health problems (Vizard et al., 2020), due to provision of secure attachment, support, and acceptance (Buehler, 2020). On the other hand, studies have illustrated that family functioning is a risk factor, as it has been found to be significantly related to anxiety (Bogels & Brechman-Toussaint, 2006), depression (Daches et al., 2018) and aggression (Perez-Fuentes et al., 2019).
Several family components have been found to be associated with functioning and adolescents’ mental health. Firstly, family communication facilitates the fulfillment of adolescents’ self-esteem (Trong Dam et al., 2023), helps them cope effectively with decision-making (Boele et al., 2024), works against the development of distress (Wong et al., 2023), increases feelings of belonging (Shannon, 2022) and provides satisfaction (Hodge et al., 2017). In comparison, dysfunctional parent-child communication has been associated with adolescents’ depression, anxiety, and behavioral problems (Hawes et al., 2021). Secondly, adolescents who reported being satisfied with their parents have been found to be at a decreased risk of developing anxiety (Essau et al., 2014), delinquency behaviors (Kenny et al., 2013) and antisocial behavior (Theobald & Farrington, 2012). Thirdly, family conflicts and criticism have been identified as indicators for dysfunctional families (Benson & Buehler, 2012). Specifically, Fosco and Lydon-Staley (2020) illustrated that family models characterized by conflicts are associated with low mood, aggressiveness, and lack in cohesion. Finally, another component, parental rejection, including lack of warmth, has been found to be negatively associated with ODD and internalizing disorders (Scully et al., 2020).
To narrow the gap between research and community-based adolescents’ mental health, assessing a clinical sample is a priority. Existing research on adolescents with mental disorders has shown significantly higher rates of emotional and behavioral problems and poorer family functioning compared to children from community settings (Brown & Wright, 2003). Adolescents diagnosed with mood disorders experience miscommunication and behavioral control from their parents, predictors that contribute to the onset of nonsuicidal self-injury in this population (Qiao et al., 2024). Similar findings were reported by Vujovic (2024), who examined juvenile delinquents and found that the predictors of delinquent behavior included parental rejection, overprotection, and lack of monitoring. As argued by Oltean et al. (2020), parents who are affectively involved with their children and solve their problems interfere with the development of autonomy and decision-making skills during depressed and anxious situations, which affects the presence of anxiety and depressive symptoms. The same pattern exists with behavioral problems, where positive parental control and involvement have been found to be associated lower odds of ODD and conduct disorder (Childs et al., 2022; Fairchild et al., 2019).
Differences in family functioning can be found between clinical and community samples of adolescents. Specifically, a study by Santesteban-Echarri et al. (2018) found that adolescents with mental illness were less satisfied with their families compared to non-help-seeking youth, due to impairments in family dynamics and interactions in the families of mentally ill adolescents. A similar study by Pereira et al. (2015), which included qualitative data, showed that depressed adolescents are raised in families lacking affection, experiencing conflict and existing in unstable environment, compared to adolescents without mental disorders who are raised in functional families. Due to the lack of affection and the presence of conflicts, these children learn to hide their emotions and feelings, which contributes to stress, situations that increase the severity of depressive symptomatology (Pereira et al., 2015).
The Present Study
The overall purpose of the present study was to examine the relationship between family functioning and adolescents’ mental health problems. This study predicted that adolescents from clinical setting would have significantly higher scores on emotional and behavioral problems compared to the adolescents from community setting and that family functioning factors would predict adolescents’ mental health problems. In support of this, we predicted that there would be significant group differences in family factors, with adolescents from clinical setting scoring higher on unbalanced factors and lower on cohesion, flexibility, family communication, and family satisfaction compared to the adolescents from community settings. At the same time, these predictors were explored through interviews with adolescents to assess their perceptions on their families’ functioning and to examine their views about its impact on their mental health.
To address these aims, this study uses integrated findings from a mixed-method design. A mixed-method approach was utilized to highlight family functioning factors that predict adolescents’ mental health problems alongside their real experiences and thoughts about their families. The timing of these research methods was carried out sequentially, with the quantitative research taking place prior to the qualitative research. This order provides an integrated approach, as the nature of the study is to use qualitative data to refine and explain in more depth the statistical results from the first phase, which provide a general understanding of the study's aims. Additionally, this research builds upon existing literature in this field by comparing the perspectives of community and clinically referred adolescents.
Method
Participants
Adolescents consisted of six hundred and ninety-two (N = 692) Greek-speaking Cypriot adolescents, aged 12 to 17 years. Specifically, the community sample consisted of a total of 612 adolescents and the clinical sample included 80 adolescents. The mean age of the participants was 14.86 (SD = 1.46). Participants were approximately equally divided between males and females (324 males; 368 females) and reported living in rural (52.6%) and urban (47.4%) areas across all cities in Cyprus. Most of the adolescents came from intact families (n = 593, 85.7%), 35 adolescents were from restructured families (5%), 58 adolescents were from single-mother families (8.4%), and a small number of 6 adolescents were from single-father families (0.9%). A cluster-sampling method was used.
The qualitative sample includes a subgroup of 20 adolescents from the quantitative sample. Specifically, ten (n = 10) adolescents were from community sample and ten (n = 10) were from clinical sample. Half of these participants were males (10 males; 10 females). The mean age of the participants was 14.45. All participants from the community sample came from intact families, whereas 5 adolescents from clinical sample were from single-mother families (50%). All ages and living areas were represented in this phase. The approach to qualitative sampling did not aim to recruit a nationally representative sample, but rather to reflect the demographics of each sample group.
Measures
Procedure
Prior to data collection, the necessary ethical approvals were obtained from the Cyprus National Bioethics Committee, the Cyprus Ministry of Health, the Cyprus Ministry of Education, Culture, Sport and Youth and the University of Roehampton Ethics Board. In the first phase, for the community sample, twenty (20) public Junior High Schools and twenty (20) Senior High Schools from all five districts of Cyprus were randomly selected from a list of hundred and twenty (120) schools. All Heads of these schools were contacted and asked if they were interested in participating in this study. Only ten (10) Junior Schools and ten (10) Senior High Schools agreed to participate. The Head of each school circulated the consent forms for both the parents and the adolescents and had the right to decide which classes would participate. Consent forms were taken home to be signed, and only adolescents who returned a signed consent were able to complete the survey. The completion of the questionnaires took place in their classrooms on a specific day and time, in the presence of their teacher and the researcher. On the first page of the questionnaire, there was a question asking adolescents if they had experienced any kind of distress or serious problems the past 12 months. Those who indicated that they had any kind of mental health issue were excluded from the study.
For the clinical sample, adolescents were recruited from the Child and Adolescent Mental Health Services of Cyprus (CAMHS) across all cities in Cyprus. Participants in this group were selected by the psychologists of CAMHS based on their diagnosis and the severity of their symptomatology. Specifically, adolescents with extremely severe symptomatology and diagnoses of disorders that interfere their functioning were excluded. Psychologists provided a list of children, and all of them were informed about the study. Those who were interested in participating were given a consent form, which was taken home to be signed. Once the consent forms were signed, an appointment was arranged in a designated room in the Mental Health Unit to complete the questionnaire. The researcher and a member of staff were present throughout the completion process.
For both the community and clinical samples, adolescents completed the questionnaires anonymously. Additionally, they were informed in writing that their participation was voluntary and that they could withdraw at any time without any interference or penalties. Consent forms included a section where participants were asked to provide contact details in case they were interested in participating in an interview at a later stage. The questionnaires took approximately 45 min to complete. Upon completion, the adolescents were given a debriefing sheet.
In the second phase, a random sample of those who provided their contact details was selected. First, a new consent form was provided and signed by both the adolescents and their parents. The interview then took place in a quiet public location in the adolescents’ hometown and lasted approximately 30 min. It was emphasized that the interview was confidential and would only be used for research purposes. Subject to the participants’ agreement, the interviews were audio recorded, and the recordings were transcribed for analysis. The participants were assigned a unique study number so that only a record number could be linked to their data, ensuring complete confidentiality. At the end, a debrief sheet was provided.
Data Analysis
SPSS 29.0 was used to analyze the quantitative data. Multivariate analyses of variance (MANOVA) were performed to assess group differences in mental health problems and family factors separately. Prior to the analyses, all the assumptions of MANOVA were examined and confirmed, expect for homogeneity of variance-covariance matrices. The results of the Box's M tests were found significant (Box's M test for family factors =113.97, p < 0.01; Box's M test for mental health problems =345.39, p < 0.01), indicating that the matrices were not the same and that this assumption was violated. Therefore, Pillai's Trace Test (V value) was considered. Logistic Regression was conducted to examine the predictors of family functioning on adolescents’ mental health problems. Sample groups were used as binary outcomes, and FACES subscales were included as predictors, using the entry method. The sample size was 692 participants, indicating medium to large effect (Miles & Shevlin, 2001). To assess multicollinearity Spearman's Correlation coefficients were checked among the predictor variables in the model. Intercorrelations among predictors above .80 signal a problem, and those variables should be removed (Cohen, 1988). There were no variables with a correlation higher than .80; thus no variables caused multicollinearity. Therefore, all the FACES subscales were included in the logistic regression model. Residuals were also checked prior to the analysis. The predicted probabilities and residuals were used to examine the goodness of fit of the model. Standardized residuals were used to check that no more than 5% of cases had an absolute value above 2, no more than 1% had an absolute value above 2.5 and no case exceeded 3 (indicating an outlier). Based on this, no cases were excluded. Cook's distance values above 1 were examined and no cases needed to be excluded. The average leverage of the model was calculated (.01) to identify leverage values greater than three times this average value (.03). There were no cases of leverage values above .03; thus no cases needed to be removed. Finally, DFBeta values greater than 1 were checked, and none were found. After checking the residuals, none of the participants were excluded from further analysis. The significant level was set as 0.05. Effect sizes and confidence intervals were calculated.
Due to the fact that data from the community sample were collected from different classes, calculating the ICC was considered necessary to check for the impact of clustering variable (i.e., classes). The ICC examines the proportion of the total variance attributed to the variability between clusters; a large ICC indicates a high degree of heterogeneity across clusters (McCoach & Adelson, 2010). For the present study, the ICC for YSR total score was found to be 0.014, for the FACES cohesion total score it was 0.015, and for the FACES flexibility total score it was 0.014. As argued by Killip et al. (2004), a very small value of ICC indicates that the variation within clusters is much greater than the variation between clusters. Considering the fact that the ICC scores of the present study are small, it can be argued that differences among adolescents within the same class are larger that the differences among the classes themslves. Therefore, clustering may not have a significant effect on the measurements being studied, allowing for analyses at the individual level rather than at the cluster level. Nevertheless, it is important to clarify that the present study does not interested in drawing interferences between school classes.
For the analysis of the qualitative data, Thematic Analysis (Braun & Clarke, 2006) was used. The recordings were fully transcribed and coded on a line-by-line basis by the researcher. A detailed reading and preliminary coding of the data were conducted to identify different concepts. Each concept was written on a card with a short quotation from the interview that was relevant to it. The aim of this stage was not to record every instance of a concept but to include examples that added further meaning to the concept. A provisional list of codes (N = 22) was drawn up, and they were redefined or discarded as further analysis took place. Once the coding of concepts was complete, the concepts were refined by checking the cards against the transcripts. Definitions were then written for the concepts to establish a link between them and to generate the main themes. At the end of this stage, there were four themes for both sample groups. The themes involved the construction of several thematic maps to confirm that they aligned with the overall analysis and research aims. The analysis was conducted at the latent level, aiming to uncover underlying ideas, assumptions, and patterns within the data.
Results
Group Differences on Adolescent Mental Health Problems
MANOVA revealed a significant main effect of adolescents’ setting, V = .18; F(9,682) = 16.50, p < 0.01, η2 = .18. Follow-up univariate tests on each emotional and behavioral problem were conducted. ANOVAs revealed significant group effect on all YSR subscales including total score (Table 1). Adolescents from the clinical setting reported significantly more mental health problems than those from community setting. The effect size was small to medium for all variables.
Group Effect on Adolescents YSR Syndromes.
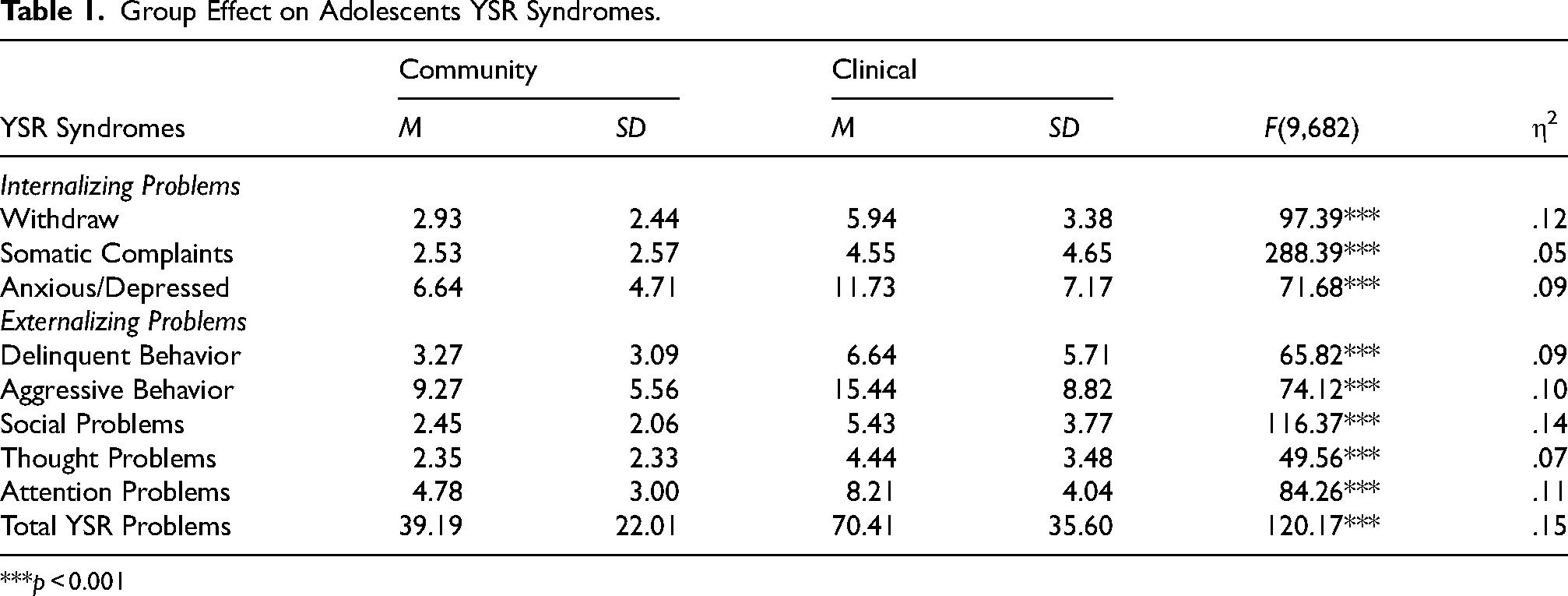
***p < 0.001
Group Differences on Family Functioning Variables
MANOVA revealed a significant main effect of the participants’ settings, V = .09; F(9,682) = 8.54, p < 0.01, η2 = .09. Follow-up univariate tests revealed significant group effect on Cohesion, Flexibility, Disengaged, Chaotic, Communication and Satisfaction (Table 2). Specifically, adolescents from the community setting reported significantly higher scores on the Cohesion, Flexibility Communication and Satisfaction, whereas adolescents from the clinical settings reported significanlty higher scores on Disengaged and Chaotic. No significant differences were found for the Rigid and Enmeshed variables. The effect size was small for all variables.
Group Effect on FACES Variables.
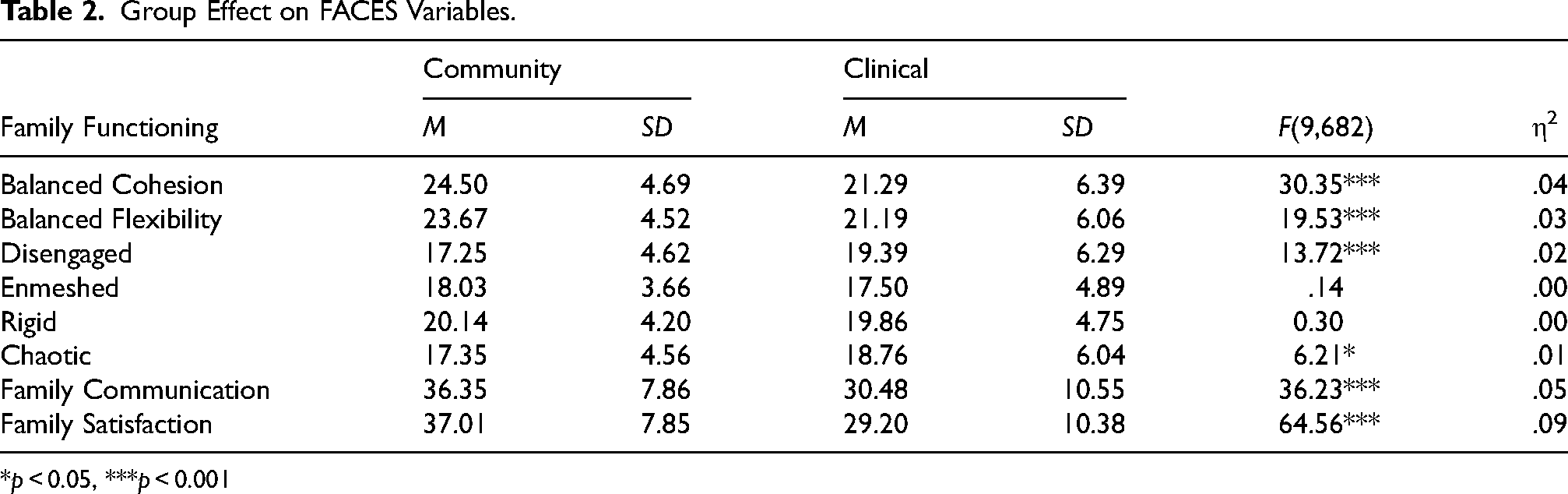
*p < 0.05, ***p < 0.001
Predictors of Adolescents Mental Health Problems
A logistic regression was conducted to investigate the impact of family functioning factors on the likelihood of experiencing a mental disorder. The model was statistically significant, χ2(8) = 60.38, p < .05, explaining between 8% (Cox & Snell R Square) and 16% (Nagelkerke R Square) of the variance in the clinical sample and correctly classifying 89% of cases. This result indicates that family functioning predicts the likelihood of developing mental health problems in adolescence. The estimates for the coefficients of predictors included in the model showed that the coefficient for family satisfaction was significant with Confidence Intervals (CI) for exp (B) from 0.88 to 0.95. This indicates that adolescents from the clinical setting reported being less satisfied with their parents than adolescents from the community setting (Table 3), suggesting that negative perceptions of family satisfaction are strongly related to the risk of experiencing mental health problems in adolescents. It should be noted that the Hosmer and Lemeshow test of goodness of fit of the model, χ2(8) = 19.60, p < .05, showed a poor fit, as the model predicted values that are were significantly different from those observed.
Logistic Regression for Predicting The Group (Adolescents from Community and Clinical Settings) of the Participants.
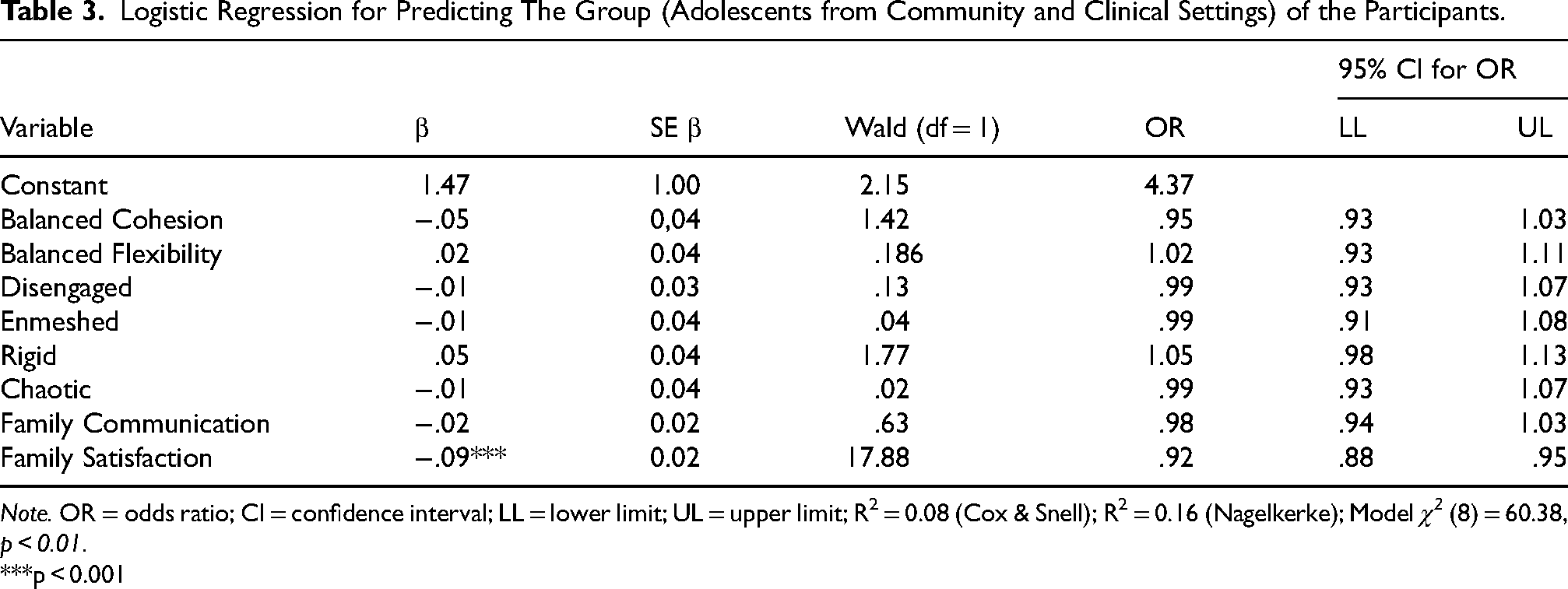
Note. OR = odds ratio; CI = confidence interval; LL = lower limit; UL = upper limit; R2 = 0.08 (Cox & Snell); R2 = 0.16 (Nagelkerke); Model χ2 (8) = 60.38, p < 0.01.
***p < 0.001
Themes from Community Setting
Themes from Clinical Setting
Discussion
The present cross-sectional study aimed to explore differences in mental health problems between adolescents in clinical and in community settings. Additionally, it sought to examine the premise that family functioning impacts adolescents’ psychopathology. Drawing on results from both surveys and interviews, this study found that family functioning significantly affects adolescents’ mental health problems.
Firstly, findings from quantitative data indicated that adolescents in the clinical setting reported significantly higher levels of emotional and behavioral problems compared to their peers in the community setting. This aligns with previous research, which found that clinically referred adolescents experience distress related to worry (Üstün & Kennedy, 2009), aggressive family dynamics, and suicide attempts (Korell et al., 2024). Additionally, adolescents often demonstrate less psychosocial competence and satisfaction (Memmott-Elison et al., 2020), characteristics closely linked to their mental health conditions.
Secondly, a key finding of the present study is the significant impact of family functioning on adolescents’ mental health problems. Adolescents in the clinical setting reported their families as more disengaged and chaotic and noting high levels of conflict and criticism. Specifically, adolescents in the clinical sample were more likely to experience decreased family cohesion, flexibility, communication, and satisfaction, alongside increased enmeshment, disengagement, and chaotic environment. This aligns with Meeus (2016), who argues that adolescents play a crucial role in shaping their family environment. Previous research indicates that deficiencies in family functioning lead to reduced support, increased conflicts (Yöntem, 2019), and place adolescents at greater risk for developing mental health problems such as depression (Stavropoulos et al., 2015). Fosco and Lydon-Staley (2020) demonstrated that conflict during adolescence is associated with negative mood, while family disengagement can lower self-esteem and confidence, factors that adversely affect mental health. In contrast, adolescents from the community setting reported their families as flexible and supportive, consistent with findings Byrne et al. (2017), which linked parental monitoring, supervision, and open communication to better mental health outcomes. Additionally, aggressive behaviors were found to decrease in environments characterized by parental knowledge, family communication and expressiveness (Lippold et al., 2014).
However, it is important to note that this evidence is correlational, suggesting a potential bi-directional. Parenting a child with mental disorder may present challenges that negatively impact family functioning. While family functioning has been shown to influence adolescents’ emotional and behavioral problems, it is also possible that these problems shape adolescents’ perceptions of their parents and family dynamics. For instance, adolescents whose parents effectively monitor their behavior have fewer opportunities to engage in emotional and behavioral problems (Yang et al., 2024). Those raised in dysfunctional families characterized by lower cohesion and flexibility are at higher risk for mental health problems (Mastrotheodoros et al., 2020). Conversely, research predicts poorer adjustment and increased emotional dysregulation, which can subsequently affect parental monitoring, involvement and support (Lansford et al., 2018; Sander & McCarty, 2005). Collectively, these findings suggest a reciprocal influence between family functioning and adolescents’ mental health.
Lastly, the results showed that only family satisfaction was a significant predictor of adolescents’ mental health problems. This finding stands in contrast to existing literature, which suggests that a range of family factors, including communication, cohesion, support, and control, are typically important predictors of psychopathological symptoms in adolescents (Ronan et al., 2008). Notably, low communication, low cohesion, low support, and high parental control have been closely linked to family satisfaction (Shittu et al., 2014). These elements may highlight the connection between family functioning and adolescents’ mental health, as they can have either direct or indirect effect on adolescents’ sense of fulfillment within their families (Marshall & Henderson, 2014).
Limitations
Several limitations should be considered when interpreting the findings. First, while logistic regression is a robust analytical method, caution is warranted regarding the interpretation of results. Second, the cross-sectional design of the study limits the ability to assess causality; further longitudinal studies are needed to better understand the trajectories of mental health problems in adolescents and to clarify the nature of the association observed. Third, there was a lack of control and acknowledge regarding the clinical diagnoses of adolescents, as these were not confirmed within the sample group. clinical adolescents’ diagnosis as it was not confirmed by this sample group. This limitation complicates the ability to draw conclusions about the influence of symptomatology on the examined associations. Fourth, the two sample groups were unequal, with a greater representation from the community sample. Finally, the study focused solely on family factors, making it challenging to develop a comprehensive understanding on the risk and protective factors related to adolescents’ mental health. Future research should consider collecting data from multiple aspects of the social environment, such as school and peer influences, to gain a more holistic understanding of adolescents’ mental health problems.
Conclusion
In conclusion, adolescents from clinical settings exhibited higher rates of mental health problems compared to those from community setting. While differences in family functioning were noted, only family satisfaction emerged as a significant predictor of mental health problems. Interestingly, qualitative findings highlighted that support, responsiveness, and parental involvement in adolescents’ problem-solving and decision-making processes significantly influenced their mental health. Conversely, unsupportive parenting, conflict, and authoritarian control were identified as critical factors affecting clinically referred adolescents. Thus, even though family functioning and communication did not statistically predict mental health problems, the interviews indicated that they do have an impact. This underscores the value of employing a mixed-method approach in this study. Future research should further investigate the role of socio-demographic variables in the relationship between family functioning and adolescents’ mental health to gain a deeper understanding of how family dynamics affect adolescent well-being.
Footnotes
Acknowledgments
I would like to thank Ministry of Education, Sport and Youth, Ministry of Health and Child and Adolescent Mental Health Services and all children participated.
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional, national research committees and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the Cyprus National Bioethics Committee, No. ΕΕΒΚ ΕΠ 2011/05), the Cyprus Ministry of Education Culture Sport and Youth (No. 7.19.46.7/16), the Cyprus Ministry of Health (No: M.H.S.5.34.3) and the University of Roehampton London (No. PSY10/055).
Consent to Participate
Written informed consent was obtained from all children included in the study and from their parents. Participants signed informed consent regarding publishing their data.
Consent for Publication
In the consent form, gained from all children and their parents, there was a clear statement indicating that they consent to publish the results of the study on the condition that their identity cannot be revealed.
Funding
The author received no financial support for the research, authorship, and publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.