
Abstract
Exsanguinating trauma is a common cause of death. Placing bleeding control kits in public areas has been suggested as a countermeasure. Similarly, automatic external defibrillators (AEDs) are placed in public areas in case of cardiac arrests. Both severe bleeding and cardiac arrests require rapid care and people must be able to quickly find relevant emergency equipment. This study explores where and how people search for such equipment. Twenty participants wearing eye-tracking glasses searched for bleeding control kits and AEDs in a public building. The participants visually searched features such as signs with maps, written information, and other emergency equipment. The participants expressed elevators and staircases, open areas, entrances, and the reception to be places where medical emergency equipment would likely be placed. The results suggest that these features and places may be suitable for medical emergency equipment or directions.
Keywords
Introduction
Trauma kill 4.4 million people yearly world-wide and is one of the most common causes of death for people aged 5 – 29 around the world (World Health Organization, 2021) and the leading cause of death for people aged under 46 in the US (Rhee et al., 2014). In preventable trauma-related deaths, inadequate hemorrhage control has been noted in three out of four cases (Beck et al., 2019), and use of bleeding control (B-Con) equipment such as tourniquets has been recommended in prehospital settings to control severe hemorrhage (Bulger et al., 2014). The Hartford Consensus and the “Stop the Bleed” program has recommended both educating the public in B-Con and placing B-Con kits in public areas (Jacobs et al., 2022).
Having available B-con kits has been reported to increase willingness to provide first aid, and strong support for placing B-con kits in public locations have been reported amongst the American public (Jacobs et al., 2016). Publicly placed B-con kits also provides equipment which may be needed in case of mass casualty events, where recommendations of having publicly available equipment to treat a minimum of about 20 people have been made (Goolsby et al., 2019).
A need for research on optimal placement of B-con kits has been noted (Goralnick et al., 2020), but little research has been conducted. Some recommendations on B-con kit placement exist, unanimously recommending co-locating B-con kits with automated external defibrillators (AEDs) (Jacobs et al., 2015, 2022; Levy et al., 2022). Other recommendations include making kits easy to identify through signage, marking placement of kits in emergency plans, placing B-con material so it can be used within three minutes, and distributing B-con material throughout buildings. However, the efficiency of the recommendations has not been tested empirically. A simulation-based study on different B-Con placements strategies found that distributing multiple kits in several locations and not near emergency exits was preferable in scenarios with moving crowds (Prytz et al., 2020). However, the study used constructive simulations with modelled human behavior, and the authors point out a need of validating assumptions of the model regarding human behavior.
While little research has been conducted regarding placement of B-Con kits, more research has been conducted on AED placement. Like for trauma-related injuries, defibrillation is highly time sensitive, and each minute of delay reduces likelihood of survival (Perkins et al., 2015). Receiving defibrillation within three to five minutes after collapse have been shown to increase survival to hospital discharge, and it has been recommended that publicly accessible defibrillators (PADs) should be placed so they can be reached by a 1 to 1.5-minute brisk walk (Aufderheide et al., 2006).
Multiple studies have proposed and evaluated strategies for increasing PAD coverage by optimized AED placement (e.g., Bonnet et al., 2015; Dahan et al., 2016; Sun et al., 2016). However, this research has not covered how AEDs should be placed within buildings to optimize availability. Research on placement of AEDs inside of buildings has not focused on how to make AEDs easy to find, but rather on how to maximize coverage (e.g., Chan, 2017; Dao et al., 2012; Yang et al., 2021). This despite that people have reported that locating AEDs in simulated scenarios is difficult (Johnson et al., 2022), and that few people report knowing where nearby AEDs are located or knowing how to find AEDs (Bogle et al., 2013; Brooks et al., 2015; Kozłowski et al., 2013; Smith et al., 2017; Zinckernagel et al., 2017).
Some guidelines exist for placement of AEDs within buildings. The American Heart Association (AHA) has recommended placing AEDs near elevators and cafeterias, at reception areas, and in main corridors (AHA, n.d.). However, some studies have suggested that these are not necessarily the places where people intuitively look for AEDs. Bogle et al. (2013) used a survey on university students’ AED knowledge, where most respondents self-reported that they would look for AEDs at fire extinguishers, near entrances, elevators, bathrooms and water fountains. Johnson et al. (2022) used simulated scenarios to investigate the time to find publicly available AEDs, where the participants reported looking for AEDs mounted on walls, near entryways, fire extinguishers, lobby areas, bathrooms, and main hallways.
The current study sought to further explore how people look for emergency equipment. The study extends previous research by including search for both AEDs and B-Con kits, and by including eye-tracking and think-aloud methods to provide more in-depth information on search strategies. Two research questions were considered:
Where do people initially look for medical emergency equipment?
What search strategies do people use in their search for medical emergency equipment?
Methods
Setting
The study was conducted at “Studenthuset” at Linköping University. Studenthuset is a library, information center, and student-centered meetings which is publicly accessible during weekdays, with extended opening hours for students and university staff. The building has six floors containing study places, the campus library, an information desk, a cafeteria, and a restaurant. An AED is placed behind the library desk on the second floor, and a general first aid kit for minor injuries is placed in a room on the entrance floor, but there is no B-con kit. There is an AED-sign immediately adjacent to the AED, but no other signage or information regarding the AED in the rest of the building.
Materials
Eye-tracking
Pupil Labs “Pupil Invisible” eye-tracking glasses (Pupil Labs, n.d.) were used to record the participants field of view and gaze. The eye-tracking glasses were also used to record how the participant moved through the building and the participants’ voices through a built-in microphone.
Think-aloud protocol
While searching for the equipment, the participants were instructed to verbalize what they were doing, their thoughts, and feelings, which was recorded using the eye-tracking glasses.
Pre- and post-study questionnaires
The pre-study questionnaire surveyed characteristics considered relevant to the task, such as whether the participant had worked within healthcare or security and if they had training in first aid or medical caretaking. The participants’ familiarity with Studenthuset and if the participants knew whether and where equipment relevant to first aid or security was placed in the building, including both B-con kits and AEDs, was also covered. The post-study questionnaire considered the participants’ experience of searching for equipment, as well as their overall strategy. It also covered how the search could be facilitated, and whether the participants used previous familiarity with Studenthuset in their search. Participants looking for an AED who found the AED were also asked how challenging they considered finding the AED was.
Procedure
Before the study, participants were informed that they would search for “safety-related items”, although exactly what they would look for was not conveyed to prevent participants from looking for equipment before the study. After receiving initial information and signing a consent form, the participants filled in the pre-study questionnaire. Next, a scenario was presented consisting of a fictional emergency, and the participants were instructed to look for either a B-con kit or an AED. Participants were assigned to one of the conditions using block-randomization. The participants were instructed to search only in publicly available areas of Studenthuset and not to ask anybody for help. They were also informed that speed was not a primary focus for the study, so that they could walk at a leisurely pace. The participants started one floor above the floor where the AED was placed. At a normal walking pace, the AED could be reached in about 40 seconds.
The participants were informed that B-con kits or AEDs might or might not be placed in Studenthuset, so they did not know whether they would find any equipment. The scenario ended either when they found the AED or when they could not come up with more places to search, in which case they would tell the experiment leader. The experiment leader ended the scenario if the participant had been searching for more than 20 minutes. The experiment leader walked with the participant while searching to answer questions about the instructions, make sure that the instructions were followed, and remind the participant to think aloud if needed.
Participants
20 participants, twelve male and eight female, with a mean age of 24.8 years (SD = 2.02) were recruited for the study. Of the participants, 17 were university students with majors such as cognitive science, industrial engineering and management, and computer science. Seven participants had previously worked in security or healthcare, mainly as nursing assistants (n= 3) and security guards (n= 2). Most participants (n= 13) had received some type of training in first aid or medical care, most (n = 8) more than five years ago. Of these participants, seven had training in cardiopulmonary resuscitation and three in first aid. Five had been trained in using an AED, and three in controlling severe bleeding. All but one (n= 19) had visited Studenthuset prior to the study and 16 participants visited it at least once per week on average. Participants were recruited by convenience sampling. Inclusion criteria were that participants had to be 18 years old or older and fluent in Swedish. Only participants naïve to the experimental task were recruited.
Analysis
Three analyses were performed to answer the research questions. The pre-study questionnaire and total search time were analyzed descriptively. For the first question, how much time participants spent looking at different features was tracked based on the eye-tracking data. This analysis was performed using the Pupil Labs software by manually reviewing and tagging what the participants looked at and for how long. A thematic analysis was conducted on the think-aloud data and post-study questionnaire to answer the second question.
Results
None of the participants knew if there was an AED or B-con kit placed in Studenthuset prior to the study. Nine out of ten participants in the AED group managed to find the AED. For the participants who did find the AED, it took on average 3 minutes and 39 seconds (SD = 122.7 s, min = 41 seconds, max = 6 minutes 23 seconds) to find the AED. Two out of the nine participants found the AED in under 1.5 minutes and three in under three minutes. The participants in the B-con group searched on average for 13 minutes and 2 seconds (SD= 375.3 s, min = 4 minutes 54 seconds, max 22 minutes 47 seconds).
Visual search
The first three minutes from the eye-tracking data were analyzed to investigate where the participants intuitively searched. The results, expressed in proportion of visual search time by feature, are presented in Table 1.
Proportion of visual search time of different features.
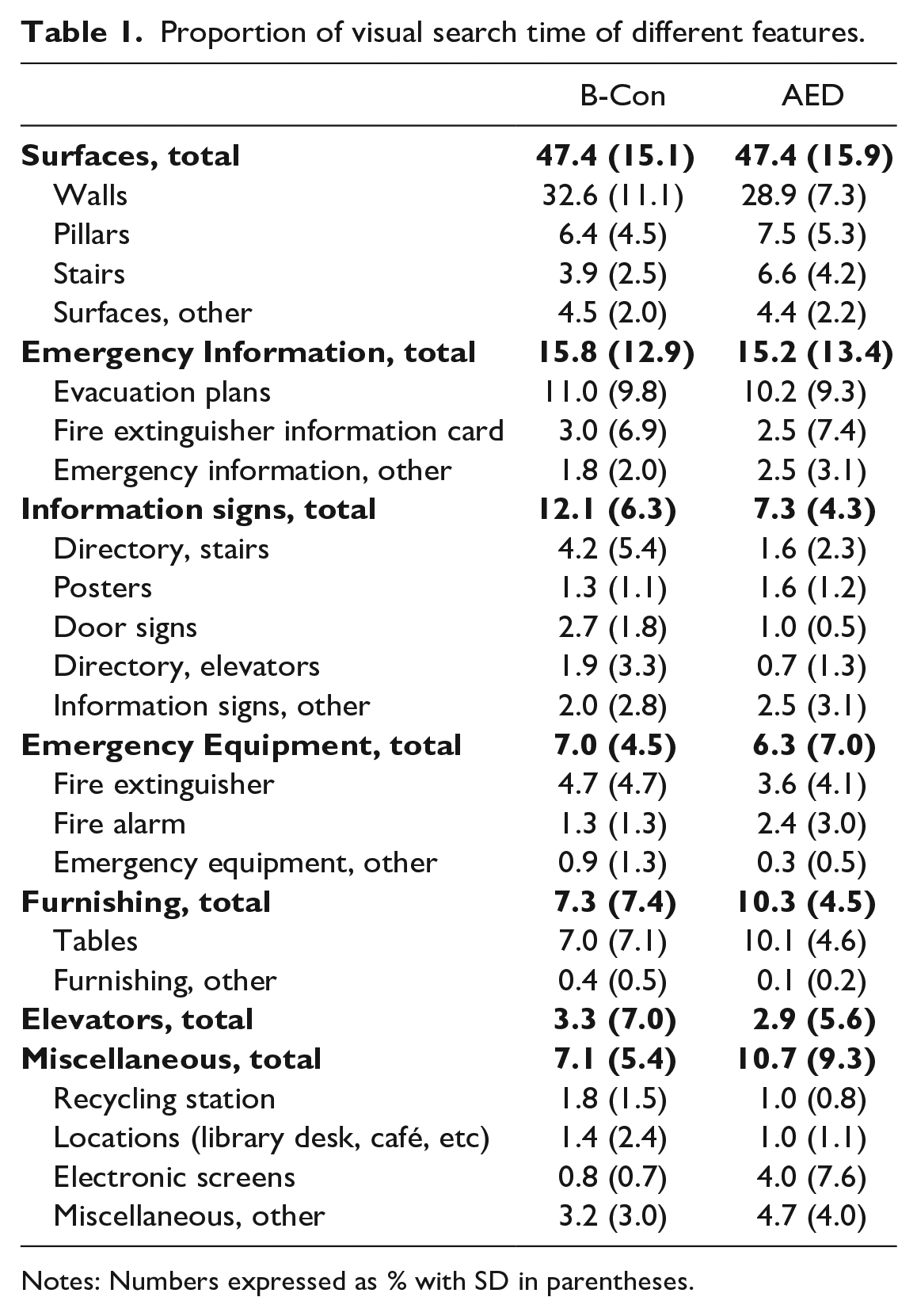
Notes: Numbers expressed as % with SD in parentheses.
Because some participants in the AED group found the AED in less than three minutes, the proportion of search time is used instead of total time in seconds. To summarize the findings, participants in both groups spent most of the time looking at different surfaces (e.g., walls, pillars), emergency information (e.g., evacuation plans), information signs (e.g., floor plans, posters), emergency equipment (e.g., fire extinguishers, fire alarms), and furnishing (e.g., tables, lockers). The participants also looked at the elevators and various miscellaneous features (e.g., the recycling station and locations such as the library desk). Independent samples t-tests did not reveal any significant differences between the two groups (all p > .070).
Search strategies
Three main themes were identified from the think-aloud data: Placement, Signage, and Co-location. The first theme, Placement, concerns where the participants believed that equipment would likely be placed. Two different views were expressed by participants regarding how the equipment was believed to be distributed in the building; that there would be equipment on each floor or that equipment would be located only on the ground floor. In many cases participants expressed both views, starting by searching the floor where the test started and, after not finding equipment there, proceeding to the ground floor. The every-floor view was more common in the B-con group and the ground-floor view more common in the AED-group. When it comes to specific places where the participants looked, participants generally believed that equipment would be placed in locations where people passed by, such as near entrances either to the building or to a specific floor. Most commonly participants thought that equipment would be near elevators and staircases or in open spaces with good visibility, and specifically for the ground floor near the entrance or the main information desk. Both groups generally considered the same places as likely.
The second theme, Signage, regards maps and information signs. Nearly all participants explicitly and thoroughly searched the maps, looking for symbols indicating placement of equipment, as well as information signs for relevant written information. The evacuation plans in particular were considered likely places for information on where equipment was placed. In a few instances, participants expressed disbelief that there would be equipment on that floor or in the building at all after not finding information on the evacuation plan. Many participants also explicitly mentioned looking for signs similar to the signs indicating fire extinguishers while walking around. Many participants also expressed that they expected there to be signs near the equipment, and a lack of signage was sometimes stated as a reason for leaving an area.
For the third theme, Co-location, many participants expressed that AEDs or B-con kits may be placed at or nearby other emergency equipment, such as fire extinguisher or the AED in the case of B-con kits. Participants also went to other equipment to find information about the equipment they were looking for, and for example examined the evacuation cards placed at fire extinguishers for information.
Post-study evaluation
Based on the post-study questionnaire, the most common experience was that the task was difficult, especially among the B-con group. The participants of the AED-group who found the AED on average rated the task as easy to moderately difficult (M = 3.2, SD = 1.99, on a 7-point Likert scale). Regarding strategy, the themes from the think-aloud data were echoed, as the participants expressed that they looked at maps and written information, looking for signs, and searching in open areas. To make the task easier, the participants mainly mentioned the need for maps with the equipment marked on it or written information on placement, as well as a need for having signs on walls or other surfaces. Most participants, 17 out of 20, said that they used their familiarity with Studenthuset in their search, mainly by knowing where different places were located.
Discussion
None of the participants recruited for the study knew whether there was an AED placed in Studenthuset, echoing the sentiment from other studies of low public knowledge of AED availability (Bogle et al., 2013; Brooks et al., 2015; Kozłowski et al., 2013; Smith et al., 2017; Zinckernagel et al., 2017). This is despite the fact that most participants visited Studenthuset on a weekly basis. The participants also did not know whether B-con kits were available in Studenthuset. Overall, this suggests a low public knowledge regarding the availability of medical emergency equipment.
On average, participants looking for the AED took about 3.5 minutes to find it. This is longer than the recommended 1.5 minutes of brisk walk. However, the participants were instructed that they did not have to hurry, and the times may have been considerably reduced if instructed to do so. Even still, the AED could be reached in 40 seconds at a normal walking pace and the participants took on average more than five times as long to find it. These results indicate that consideration should be taken in how to make the equipment easily findable, either through placement, signage, or other means.
AHA guidelines for AED placement are near elevators, cafeterias, reception areas and in main corridors (AHA, n.d.). Previous research has suggested co-location with fire-emergency equipment, on walls near entrances, as well as receptions, lobbies, bathrooms and main hallways (Bogle et al., 2013; Johnson et al., 2022). The result of the current study replicates the findings of Bogle et al. (2013) and Johnson et al. (2022) in that the participants allocated most attention to wall areas, emergency information signage, other information signage and emergency equipment. The current study specifically shows through the eye-tracking data that structural surfaces such as walls and pillars stand for nearly half of the visual search allocation at 47%, with emergency information accounting for about 15%, information signs 7-12% and emergency equipment about 7%. The participants also explicitly noticed and searched other emergency equipment such as fire equipment and looked for both equipment and information nearby. The participants expressed that they expected to find equipment near heavily trafficked areas, floor entrances (elevators, staircases), and building entrances and exits.
The results also suggest that people actively look for signage when searching for equipment and use it to guide their search. Therefore, providing visible signage might be important to decrease search times. Many participants noted and spent considerable time looking at maps and reading written information, for example on evacuation plans. Including information on where and on which floor equipment is placed on such signage is likely advantageous. Some participants expressed doubt as to whether equipment existed on the particular floor or in the building at all after failing to find information on such signage. Thus, even though it is unclear whether people would take time to look at maps and written information to the same extent in a real emergency scenario, providing information on for example evacuation plans would be easy to do and might prevent premature termination of search. Many participants believed that equipment would be placed on every floor in the building, particularly for the B-Con group. If equipment is placed only on a single floor, providing information on every floor directing people to the correct floor is likely beneficial.
The groups seem to have searched in similar manners. There were quite small differences between the groups for features such as surfaces, emergency-related information, and emergency fire equipment. The B-Con group spent somewhat longer on general information signs, although not significantly so. Future studies with greater statistical power could be carried out to potentially find smaller effects.
Although the similarity in search behavior might suggest that co-location of AEDs and B-Con kits is beneficial from a findability standpoint, it is also important to keep their different use cases in mind. An AED is commonly used with a single patient suffering from a cardiac arrest. B-Con kits are typically added to public spaces to be used during mass-casualty events. Differences between these contexts, such as number and distribution of victims, crowd behavior, and possible risks of moving through the environment when searching for equipment are also important factors to consider.
One limitation is that this study was carried out in a single building, and the layout of the building is likely to have influenced search behavior. Most participants were students familiar with the building, which might also have influenced the results. Replication studies in other settings and with participants from other backgrounds, and who are not familiar with the building, should be conducted. Further, there was no time pressure or induced stress in this study. While this was intentional to allow participants to think aloud and express their thoughts freely, it does not reflect a real-life hemorrhage or cardiac arrest scenario. Studying search behavior under more time-pressured conditions might reveal other search behaviors. Further studies could examine the effects of increased visibility for example by use of signage, which has also been suggested in previous research (Brooks et al., 2015, 2022; Johnson et al., 2022; Merchant et al., 2014; Sidebottom et al., 2018; Yang et al., 2021), by supplying more detailed maps, or by varying placement of equipment.
Conclusions
Naïve participants use similar search strategies for both AEDs and B-Con kits. Most visual attention during search is directed at wall surfaces, emergency information signage, other information signs, emergency equipment, and furnishing. Including information about the presence of such emergency equipment on information signage may prevent premature termination of search. These findings are in line with previous research and provide additional context for in-building AED and B-Con equipment beyond existing AHA guidelines.