
Abstract
Objectives:
This study aimed to assess the prevalence of depression, anxiety, perceived discrimination, and weight stigma among bariatric surgery candidates.
Methods:
This cross-sectional study was conducted from April to November 2024 at a tertiary care obesity treatment center using convenience sampling. Participants (N = 210) completed validated tools, including the Beck Anxiety Inventory, Beck Depression Inventory, Weight Self-Stigma Questionnaire, and a discrimination scale. Data were analyzed using descriptive statistics, independent group comparisons, correlation tests, and multivariate adjusted models.
Results:
The median age of participants was 39 years. Based on body mass index (BMI), patients were categorized into Group A (35–40, n = 75) and Group B (>40, n = 135). BMI was significantly associated with marital status (p = 0.049) and education level (p = 0.031). While 43.8% had no or minimal depression, 81.4% reported grade 2 anxiety. Group A showed significantly higher depression scores (p = 0.012), whereas severe anxiety was more frequent in Group B. Moderate discrimination and mild stigma were commonly reported. Adjusted analyses revealed positive correlations between BMI and both discrimination (rs = 0.33, p < 0.001) and stigma (rs = 0.23, p = 0.007).
Conclusion:
Psychological distress and perceived stigma are prevalent in candidates for bariatric surgery. It is recommended to implement psychosocial screening and provide targeted psychological interventions to improve mental health and postoperative outcomes among them.
Introduction
Obesity has become a critical global public health issue, with its prevalence increasing across all age and socioeconomic groups.1,2 Obesity is defined as excessive fat accumulation 3 that is a health risk and closely linked to a wide range of diseases, including diabetes, 4 cardiovascular diseases (CVDs), 5 cancer, 6 and musculoskeletal disorders. 7 These comorbidities not only reduce quality of life and work productivity but also contribute substantially to health care costs. 8 Beyond its well-documented physical implications, obesity is also a major psychosocial burden that adversely affects mental health, self-perception, and quality of life.9,10
Growing evidence indicates the psychological consequences of living with obesity, including depression, anxiety, diminished self-esteem, eating disorders, and body image dissatisfaction. 11 These effects are not merely incidental but appear to be bidirectionally linked with obesity through behavioral, neuroendocrine, and inflammatory mechanisms. Moreover, persons with obesity are exposed to social stigma and discrimination, which further exacerbate their psychological distress.12,13 It has been shown that stigma is both external, in social interactions, and internal, through self-devaluation, and has been shown to predict worse mental and physical health outcomes, independent of body mass index (BMI) itself. 14
Weight stigma and discrimination are harmful experiences reported by individuals living with obesity. Numerous studies have shown that patients with obesity frequently experience negative attitudes, blame, and reduced empathy from health care providers, which can lead to avoidance of medical care.15,16 Meta-analytic evidence also suggests that weight discrimination is significantly associated with psychological distress, low self-esteem, and disordered eating behaviors. 17 Importantly, weight stigma contributes independently to adverse health outcomes through both behavioral and biological pathways. Internalized stigma has been particularly detrimental, correlating with heightened risk for depression, anxiety, social isolation, and avoidance of physical activity. 18 Despite these well-documented consequences, weight stigma remains under-addressed in clinical protocols and preoperative evaluations, including those for bariatric surgery candidates.
In bariatric surgery candidates, who often present with severe obesity and longstanding struggles with weight management, these psychosocial factors may be especially pronounced. The co-occurrence and interplay of depression, anxiety, perceived discrimination, and weight stigma in this specific population are notable, as they may influence surgical candidacy, preoperative decision-making, postoperative outcomes, and long-term adherence to lifestyle modifications. Therefore, the present study aimed to investigate the prevalence and severity of depression, anxiety, perceived discrimination, and weight stigma among candidates for bariatric surgery.
Methods
Study design
This cross-sectional study was conducted between April 2024 and November 2024 and took place at the Taleghani Obesity Treatment Center, Tehran, Iran, a referral center for bariatric surgery. The study employed a convenience sampling approach, which involved the inclusion of all persons with obesity who were candidates for bariatric surgery. These participants were administered questionnaires for data collection purposes. After the questionnaire completion, no further interactions or follow-ups occurred with the participants. This study received approval from the Ethics Committee of the Shahid Beheshti University of Medical Sciences, with approval code IR.SBMU.MSP.REC.1400.120.
Participants
The study involved the selection of persons with obesity who had received an assessment from a medical professional. Individuals with a BMI >35 who were candidates for bariatric surgery were considered for this study. The exclusion criteria included participants who provided incomplete or inaccurate information on demographic or psychological questionnaires, which could potentially compromise the reliability of the data. All participants willingly gave their informed consent and actively completed validated psychological questionnaires.
Variable
The study’s primary outcome measurement focused on the BMI groups, anxiety, depression, stigma, and discrimination scores. Demographic and clinical variables collected for analysis included BMI 35–40 and BMI >40, age, gender, education, marital status, smoking, underlying diseases, and their relationship with the main variables, as the secondary outcome was investigated. Information on metabolic complications as underlying diseases, including hypertension, diabetes mellitus, CVDs, and hypothyroidism, was obtained through self-reported questionnaires and verified using the participants’ medical records, including participants’ medications and paraclinical findings.
Data sources/measurement
The study employed several specific questionnaires for data collection and assessment:
Beck anxiety inventory
The BAI consists of 21 items that measure the severity of anxiety. 9 Participants rate their responses on a four-point Likert scale, ranging from 0 (not at all) to 3 (severely), resulting in a total score ranging from 0 to 63. Scoring categories are 0–7 (no anxiety), 8–15 (mild), 16–25 (moderate), and 26–63 (severe). 19 Internal consistency for the BAI has been reported (Cronbach’s α = 0.92), and test–retest reliability for the BAI = 0.75. 20
Beck depression inventory
This 21-item, self-report inventory with a four-point scale from 0 (symptom absent) to 3 (severe symptoms) examines the cognitive, emotional, motivational, and physiological aspects of depression. The minimum score is 0 and the maximum score is 63. Higher scores indicate greater symptom severity. 21 The standard interpretive ranges are as follows: 0–9: No or minimal depression; 10–16: Mild depression; 17–29: Moderate depression; ≥30: Severe depression. 22 Moderate and severe depressions are considered clinically significant. Construct validity has been reported α = 0.92. 23
Stigma
The assessment of weight-related stigma was conducted using the Weight Self-Stigma Questionnaire (WSSQ), developed by Lillis et al. 24 This questionnaire comprises two distinct yet correlated subscales: one focused on self-perceived worthlessness (items 1–6) and the other on the apprehension of external stigmas (items 7–12). The self-worthlessness subscale addresses concerns such as fear of being overweight, confronting weight-related issues, experiencing guilt due to weight problems, feeling powerless in the face of obesity, and struggling with self-control to maintain a healthy weight. The second subscale explores feelings of insecurity arising from societal perceptions of individuals with excess weight, encountering discrimination related to weight issues, and experiencing challenges in establishing positive social relationships. Responses to items in the WSSQ questionnaire are rated on a scale ranging from 1 (strongly disagree) to 5 (strongly agree). The overall score is derived from the sum of scores from the two subscales.
To validate the questionnaire, the initial step involved the creation of an English version of the WSSQ questionnaire. Subsequently, a Farsi version was developed using the forward-backward translation method by two translators. Two Persian translations were then scrutinized and refined by project moderators and colleagues. After a thorough examination and discussion of the differences between the translations, a unified version of the WSSQ questionnaire was established. In the subsequent phase, two individuals fluent in both Persian and English (independent of the initial translators and unaware of the English version, research objectives, and procedures) translated the unified Persian version back into English. The two English translations were merged after review and necessary adjustments by project managers, resulting in a single English version. A comparison with the original English version revealed no significant differences.
For validity and reliability assessment, the final questionnaire underwent testing and retesting among 30 individuals aged 20 and above, at a 1-week interval. The results from the two tests indicated Cronbach’s alpha values of 0.76 and 0.79 for the first and second subscales, respectively, and 0.88 for the overall WSSQ questionnaire. In this instrument, a higher score signifies a heightened perception of stigma.
Discrimination
The assessment of discrimination linked to overweight or obesity involved the utilization of a self-report discrimination questionnaire, formulated by Jackson and Steptoe. 25 The questionnaire comprises five questions addressing various aspects of individuals’ daily lives. Response options range from “never” to “almost every day,” allowing respondents to indicate the frequency of their experiences.
To ensure the questionnaire’s validity, the initial step involved the creation of an English version. Subsequently, for the development of the Farsi version, two translators employed the forward-backward translation method. Two Persian translations were then meticulously examined and refined by project moderators and collaborators. After thorough scrutiny, discussions on differences, and resolution of disparities between the translations, a unified version of the discrimination questionnaire was established. In the subsequent phase, two individuals proficient in both Persian and English (distinct from the initial translators and uninformed about the English version, research objectives, and procedures) translated the unified Persian version back into English. The two English translations, following review and necessary adjustments by project managers, were merged to produce a single English version. A comparison with the original English version revealed no significant differences. For validation and reliability assessments, the final questionnaire underwent testing and retesting among 30 individuals aged 20 and above, at a 1-week interval. The results from the two tests indicated a Cronbach’s alpha of 0.81 for this questionnaire. In this instrument, a higher score signifies a heightened perception of discrimination.
Study size
The determination of the appropriate sample size for the study was accomplished by employing the Cochran formula (1) . The formula, denoted as, With a desired confidence level of 95% (Z = 1.96) and a margin of error of 7% (E = 0.07), and assuming a conservative estimate of 50% prevalence (p = 0.50) of eligible individuals in the population, the calculated sample size (n) is approximately 195 participants.
Statistical methods
All statistical analyses were performed using SPSS v26.0. Qualitative data are presented as frequencies (percentages). Quantitative data are presented as mean ± standard deviation or median (interquartile range) based on the normality of data distribution. Wilcoxon Rank-Sum test, Pearson’s chi-square test, and Fisher’s exact tests were used for the comparison of quantitative and qualitative data between the two groups, respectively. Adjustments for age, education level, and marital status were performed using generalized linear models. Correlation was assessed using Spearman’s correlation (unadjusted) and partial correlation (adjusted). A p < 0.05 was considered significant.
Results
A total of 210 participants with a BMI exceeding 35 kg/m2 were enrolled. The mean age of the patients was 39.28 ± 11.59 years and comprised 147 (70%) female participants. Among them, 143 (68.1%) were married, and 93 (44.3%) participants held high school or lower degrees. Notably, 23 (11.0%) participants engaged in active smoking, while 33 (15.7%) reported alcohol consumption. Underlying diseases were prevalent in 52 (24.8%) cases, with hypertension being the most commonly observed condition in 25 (11.9%) patients, followed by diabetes mellitus in 20 (9.5%) cases. The participants exhibited a mean height of 167.72 ± 10.38 cm and a mean weight of 121.06 ± 21.20 kg, resulting in an average BMI of 42.86 ± 5.87 kg/m2. A detailed summary of patients’ baseline characteristics is presented in Table 1.
Baseline Characteristics of the Participants
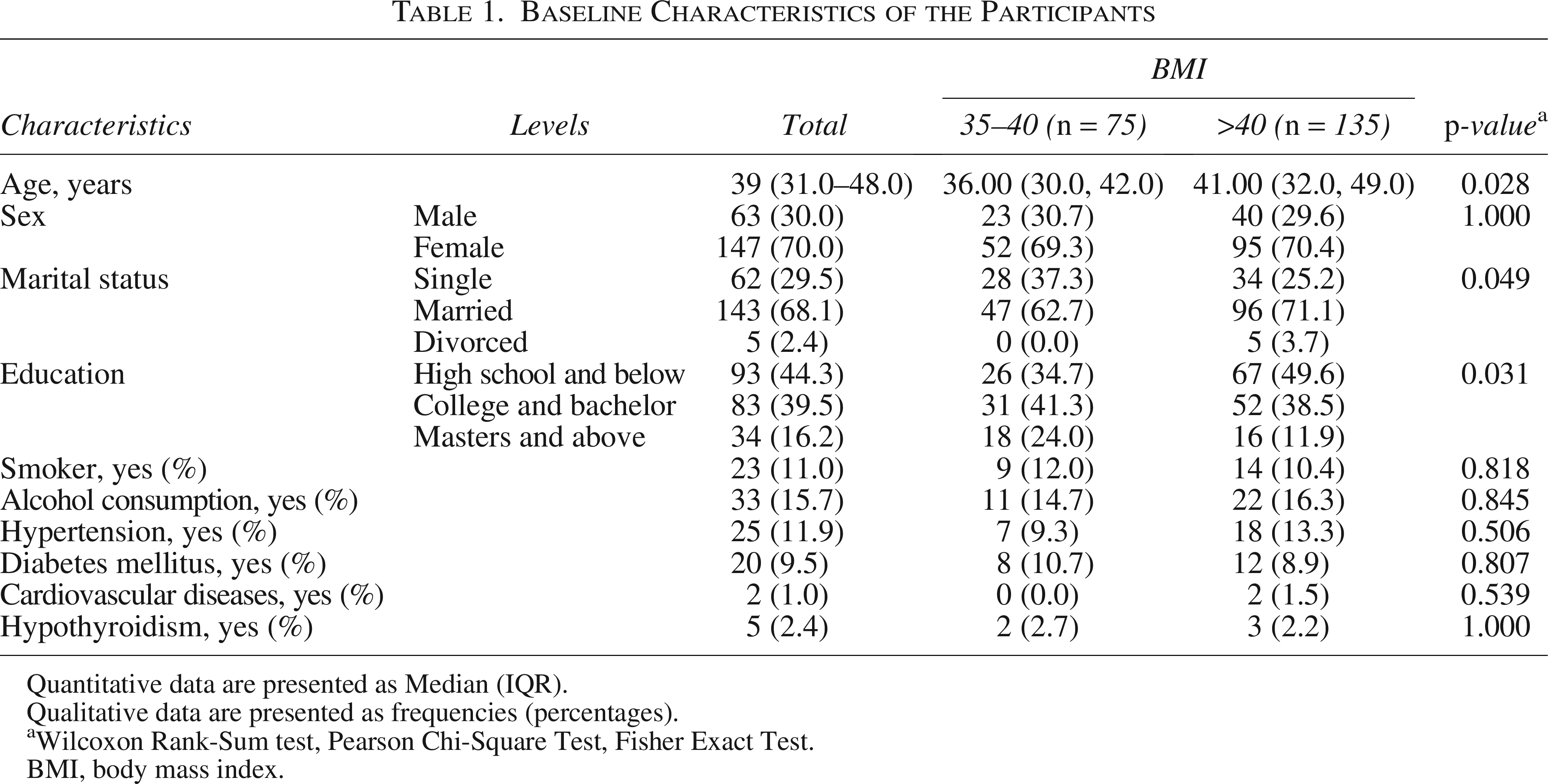
Quantitative data are presented as Median (IQR).
Qualitative data are presented as frequencies (percentages).
Wilcoxon Rank-Sum test, Pearson Chi-Square Test, Fisher Exact Test.
BMI, body mass index.
In terms of findings, the mean depression score was 13.86 ± 10.81, with 92 (43.8%) experiencing no or minimal depression. The mean anxiety score was 34.53 ± 9.82, and 171 (81.4%) participants were categorized with grade 2 anxiety. The mean discrimination score was 7.73 ± 4.39, while the mean stigma score was 30.81 ± 8.17, with 151 (71.9%) reporting mild stigma sensation. A summary of depression, anxiety, and stigma sensation is provided in Table 2.
Patients Depression, Anxiety, Discrimination and Stigma Sensation Findings
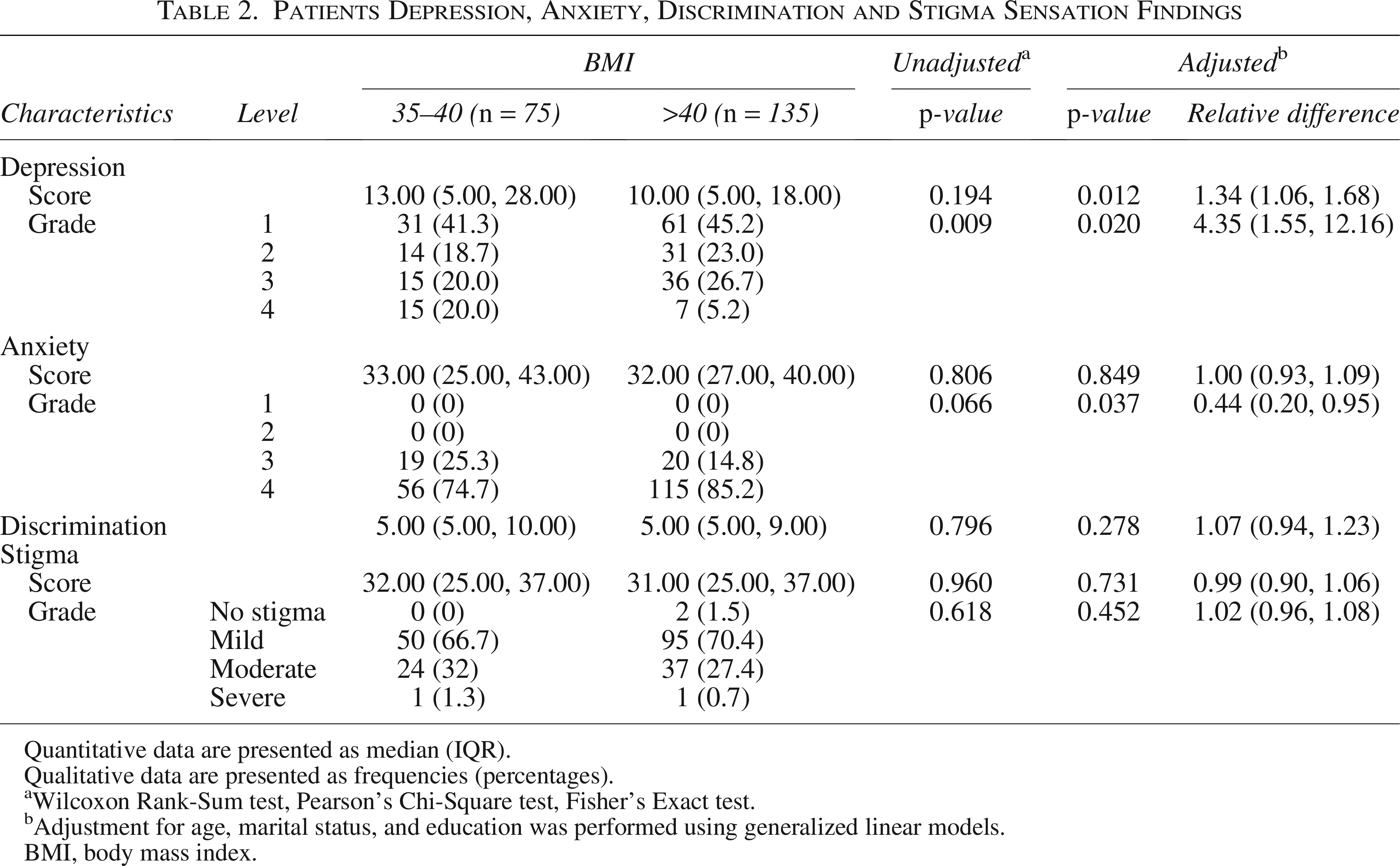
Quantitative data are presented as median (IQR).
Qualitative data are presented as frequencies (percentages).
Wilcoxon Rank-Sum test, Pearson’s Chi-Square test, Fisher’s Exact test.
Adjustment for age, marital status, and education was performed using generalized linear models.
BMI, body mass index.
Subpopulation analysis based on BMI revealed 75 (35.71%) cases in Group A (BMI 35–40) and 135 (64.29%) cases in Group B (BMI 40 and above). The mean age in Group A was 36.92 ± 10.56 years, while in Group B, it was 40.59 ± 11.96. Females constituted 69.3% of Group A and 70.4% of Group B. Smoking was reported by 12.0% in Group A and 10.4% in Group B. Hypertension was the predominant underlying medical condition, with 9.3% and 13.3% in Groups A and B, respectively.
Group B exhibited a significantly higher age (p = 0.028) and a greater proportion of participants with high school or below educational degrees (p = 0.026). In addition, married participants were significantly more in Group B (p = 0.049). Nevertheless, no significant differences were observed in terms of sex, smoking, alcohol consumption, and underlying diseases.
The mean depression score in Group A was 16.23 ± 13.02, compared with 12.54 ± 9.16 in Group B. Although no significant difference was observed between the two groups regarding the depression score (p = 0.194), severe depression was significantly more prevalent in Group A (p = 0.009). Following adjustments for age, education level, and marital status, a significantly higher depression score was observed in group A (p = 0.012).
For anxiety, Group A demonstrated a mean score of 34.81 ± 10.16, while Group B had a mean score of 34.38 ± 9.66. No statistically significant differences were initially observed between the two groups in either anxiety scores (p = 0.806) or anxiety grades (p = 0.066). However, after adjusting for potential confounding variables, a significant difference emerged in anxiety grades (p = 0.037), while the difference in anxiety scores remained nonsignificant (p = 0.849).
The mean discrimination scores were 8.13 ± 5.08 and 7.50 ± 3.96 in Groups A and B, respectively. No significant difference was observed between the two groups (p = 0.796), and this finding persisted even after adjustment (p = 0.278). The mean stigma score was 30.57 ± 8.11 in Group A and 30.94 ± 8.23 in Group B, with no significant differences observed between the two groups with (p = 0.731) and without (p = 0.960) adjustment. In addition, no statistically significant differences in stigma grades were observed between the two groups, either before (p = 0.650) or after adjustment (p = 0.452).
Correlation analysis revealed a significant association between BMI score, discrimination score (p < 0.001), and stigma score (p = 0.007) in patients with BMI exceeding 40 kg/m2. This correlation was consistent following the adjustment for age, marital status, and educational level. No significant correlation was observed between BMI and other factors. Table 3 summarizes adjusted and unadjusted associations. Figures 1 and 2 illustrate an adjusted correlation between BMI and discrimination and stigma scores.
Assessing Body Mass Index Correlation with Depression, Anxiety, Discrimination and Stigma Scores
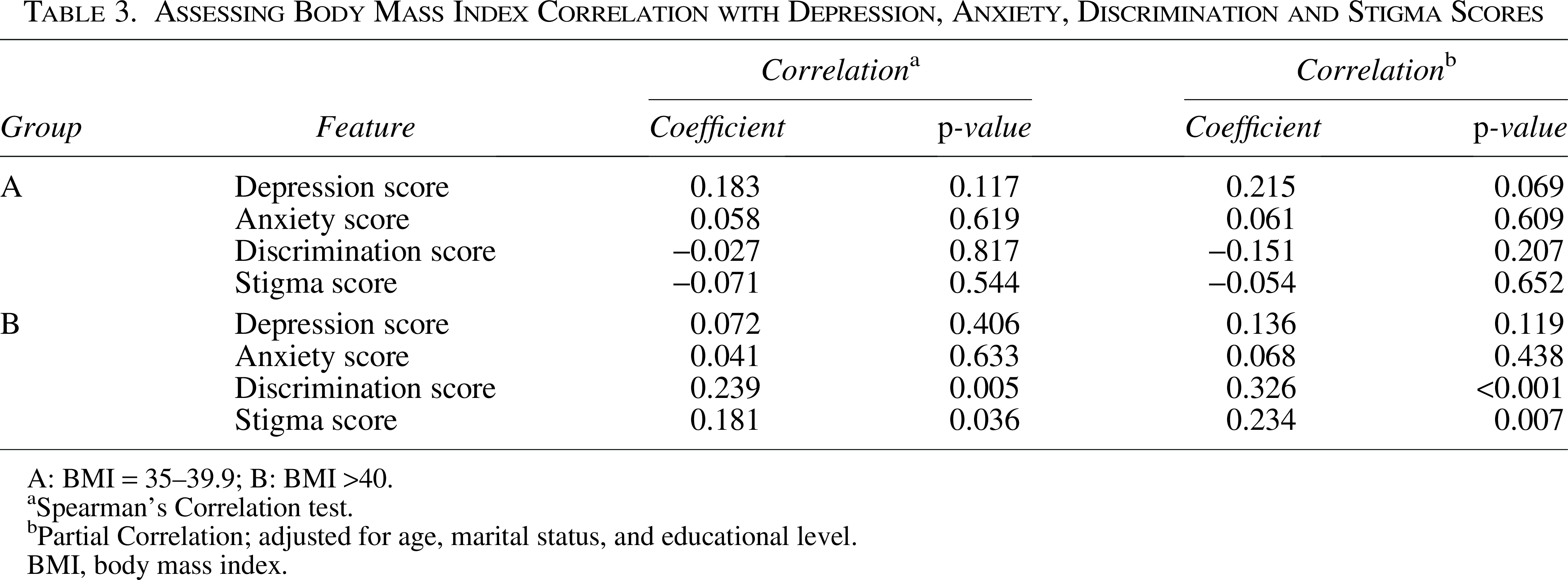
A: BMI = 35–39.9; B: BMI >40.
Spearman’s Correlation test.
Partial Correlation; adjusted for age, marital status, and educational level.
BMI, body mass index.
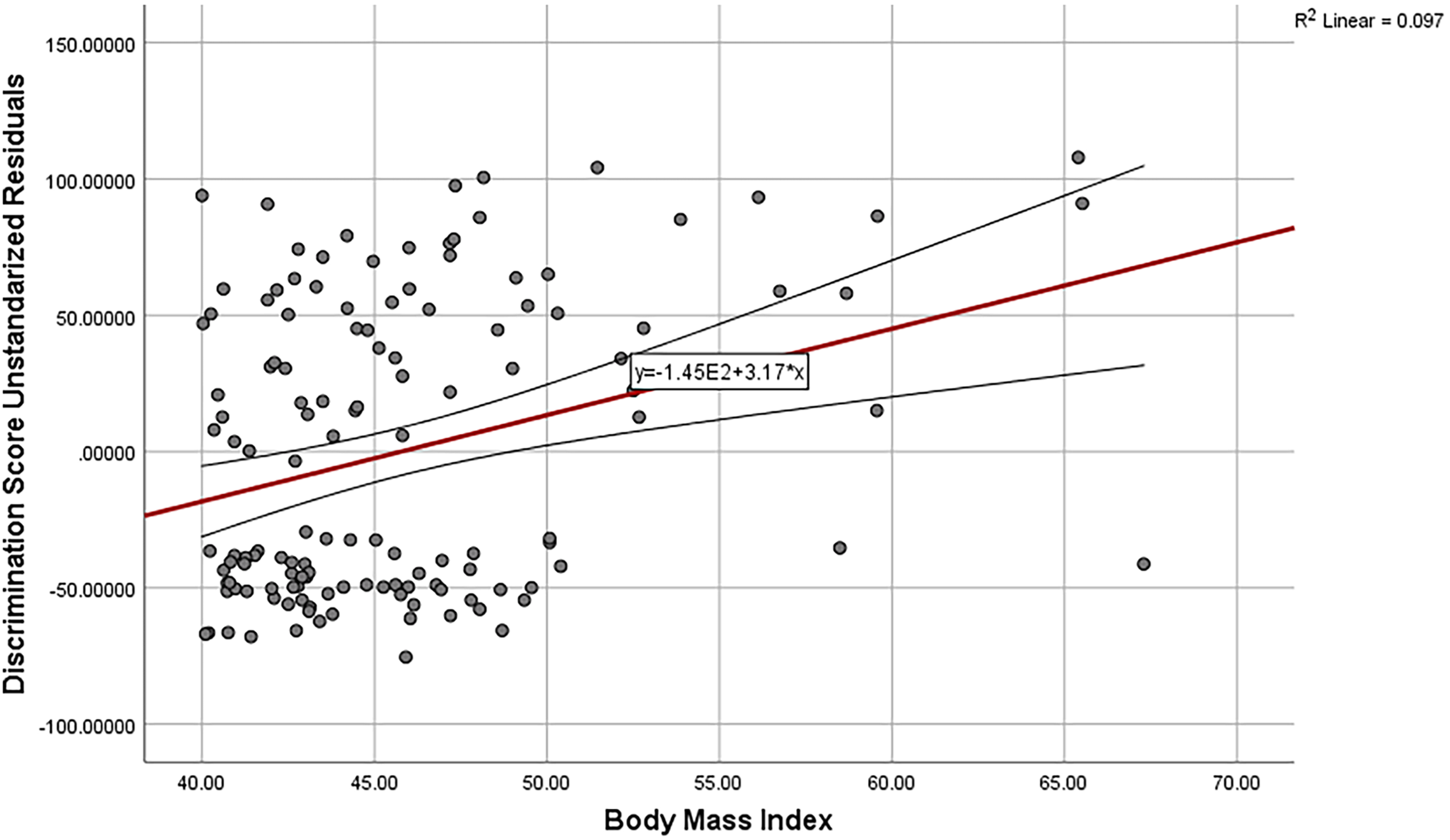
Scatterplot of discrimination score and body mass index adjusted for age, marital status, and educational level in BMI >40 groups. BMI, body mass index.
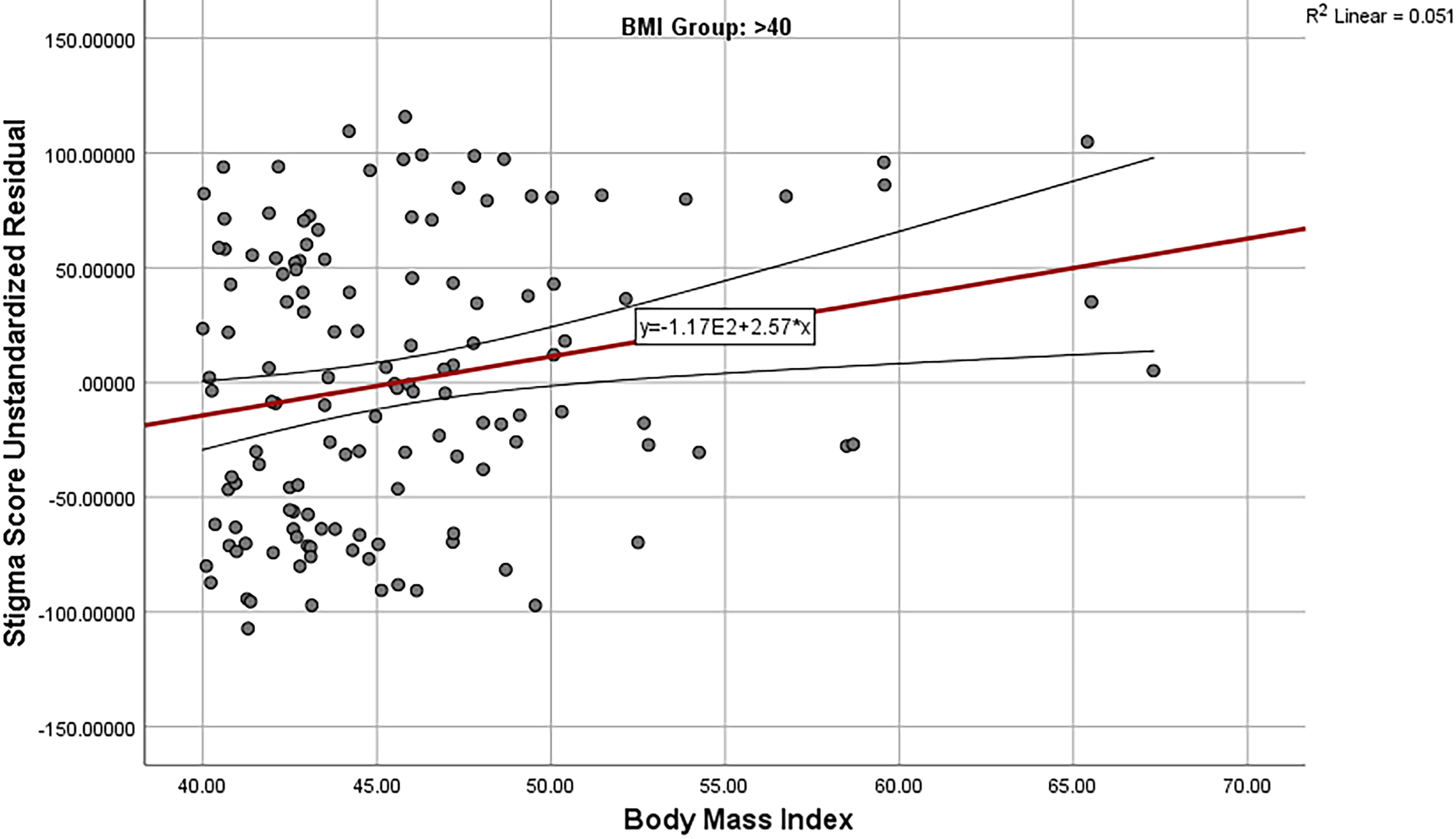
Scatterplot of stigma score and body mass index adjusted for age, marital status, and educational level in BMI >40 groups. BMI, body mass index.
Discussion
The primary objective of the present investigation was to examine the prevalence of depression, anxiety, feelings of discrimination, and stigma, and their correlation with BMI in individuals undergoing consideration for bariatric surgery. BMI was analyzed in both numerical and categorical formats (35–40 and >40 kg/m2). Significant associations were identified between BMI groups and demographic variables such as age, marital status, and education. Subsequently, adjusted analyses were conducted to explore the interplay between depression, anxiety, feelings of discrimination, stigma, and BMI. Notably, no or minimal depression emerged as the most prevalent. Furthermore, grade 2 (mild) anxiety exhibited the highest occurrence. Participants reported moderate levels of discrimination and mild levels of stigma. No significant associations were detected between psychosocial indices and the categorical representation of BMI, adjusting demographic variables. However, a positively significant correlation was observed between BMI and psychological indices, encompassing discrimination and stigma scores, after adjusting for age, marital status, and education level.
Limitations of the study include several factors that may impact the generalizability and interpretation of the findings. Firstly, the cross-sectional design and the use of convenience sampling limit the establishment of causal relationships and may introduce selection bias. The study’s exclusive focus on individuals eligible for bariatric surgery restricts the applicability of the results to a broader population with varying degrees of obesity or individuals not seeking surgical intervention. In addition, the lack of follow-up interactions with participants after questionnaire completion hinders the exploration of potential changes over time. Furthermore, the reliance on self-report measures, such as psychological questionnaires, may introduce response bias and may not fully capture the complexity of participants’ experiences. Moreover, the study does not explore certain relevant variables, such as socioeconomic status or cultural factors, which could contribute to a more comprehensive understanding of the relationship between obesity, psychological factors, and discrimination. Lastly, the absence of information on the study size in the methods section leaves a gap in understanding the power and precision of the statistical analyses performed. On a positive note, the study boasts several strengths. Notably, it employed validated questionnaires, enhancing the reliability and validity of the gathered data. Furthermore, the design and validation of discrimination questionnaires reflect a robust methodological approach, contributing to the credibility of the study’s findings.
Depression was prevalent among the candidates, with over half of the participants (56.2%) experiencing clinically relevant symptoms, ranging from mild to severe. In contrast, 43.8% reported no or minimal depressive symptoms. Contrary to some previous literature,26–29 the prevalence and severity of depression were significantly higher in the BMI 35–40 group compared with those with a BMI over 40. This difference became more pronounced after adjusting for age, education, and marital status, suggesting that individuals with moderately elevated BMI may face more psychological burden, possibly due to unaddressed comorbidities or social pressures. These findings contradict prior studies such as Herhaus et al. 26 and Jung et al., 27 which found higher depression rates in patients with BMI >40. The divergence may be explained by population differences, comorbidity profiles, and psychological adaptation among individuals with higher BMI.
Concerning the connection between depression and education among persons with obesity, by the outcomes of the current study, some research studies have affirmed that the impact of BMI on depression tends to be more pronounced in individuals with lower educational levels.30–33 It appears that higher education exerts a protective influence against depression. 33 Unlike income, education remains stable after reaching adulthood and contributes to positive mental health. 34 Individuals with higher education levels tend to employ more mental resources when facing challenges and possess superior problem-solving skills. 35 Moreover, their heightened adaptability in coping with pressures and stresses serves as a protective factor against depression. 36 In our study, lower education levels were associated with a higher incidence of depression, underscoring the importance of considering educational factors in understanding the relationship between BMI and depression. In conclusion, our findings emphasize the complex interplay between educational background, obesity, and depression, highlighting the need for personalized interventions and support for individuals with lower educational attainment in mitigating the risk of depression associated with obesity.
Although anxiety was predominantly mild (grade 2) in 81.4% of participants, further analysis revealed a more nuanced picture. While unadjusted comparisons showed no statistically significant differences in anxiety scores or grades between BMI groups, adjusted models identified significantly higher anxiety grades in the BMI 35–40 group. This unexpected finding may indicate a greater psychological sensitivity or reduced coping resources in individuals at lower obesity levels, who may face stronger internalized stigma or social pressure to lose weight. Notably, individuals who were married reported notably higher levels of anxiety. The study also identified a significant correlation between elevated anxiety levels and increased alcohol consumption. Consistent with our study’s findings, Hakan et al. similarly reported a significantly higher prevalence of mild anxiety among persons with obesity compared with those with a normal BMI, with no notable gender-based differences. 37 Other studies have indicated elevated levels of anxiety, ranging from moderate to severe, in both persons with obesity and overweight.38–40 Nigatu et al. emphasized that when anxiety progresses to an anxiety disorder, its prevalence tends to be higher among persons with obesity, contrasting with those without anxiety disorders who typically experience better mental well-being and lower anxiety levels. 41
Alcohol consumption emerges as an unfavorable lifestyle factor among persons with obesity, influencing the severity of their anxiety. 42 Interestingly, when persons with obesity resort to alcohol as a coping mechanism to alleviate anxiety, it introduces a nuanced perspective. 43 Under these circumstances, alterations in the structure and function of the central amygdala, a key player in physiological and behavioral responses to stressful stimuli, come into play. This transformative process ultimately results in the inhibition of downstream effector regions associated with the regulation of anxiety and behaviors related to alcohol consumption. 44 The intricate interplay between obesity and mental health issues further heightens the likelihood of anxiety within this demographic. 45 Factors such as low self-esteem, 46 mental pressure stemming from self-perception, 11 and physiological causes involving chemical and hormonal changes with diverse effects on the brain and nervous system collectively contribute to increased anxiety levels. 47 In addition, experiences of discrimination, a significant aspect of the lives of persons with obesity, serve as another influential factor leading to anxiety. 48 Recognizing these complicated relationships is critical for developing focused interventions to alleviate anxiety in persons with obesity while taking into consideration the many factors that contribute to their mental health problems.
An examination of discrimination levels among candidates for bariatric surgery revealed a prevalence of 50%, with no significant difference observed between BMI ranges of 35–40 and above 40. In addition, there was no significant relationship found between discrimination and factors such as gender, age, education, and marriage. However, a positive correlation was identified between marriage and weight concerning experiences of discrimination. Dutton et al. reported a discrimination prevalence of 53.9%, 49 while Sikorski et al. found that up to 38% of individuals with BMI class III experienced discrimination. 50 Discrimination emerges as a significant factor jeopardizing mental health, leading to the disorganization of the hypothalamus-pituitary-adrenal stress axis in response to ongoing adaptation to psychosocial challenges, ultimately resulting in adverse health consequences. 51 Moreover, discrimination can pose a major obstacle to the successful treatment of obesity, contributing to the overall disease burden in society. It also fosters social injustice and has the potential to widen the gap between socioeconomic classes. Notably, persons with obesity encounter workplace discrimination, translating into reduced job application opportunities, a higher likelihood of termination, and lower wages. 50 The notable prevalence of discrimination, both in this study and previous research, underscores its significance, not only for promoting individual well-being but also for fostering a more equitable and inclusive society that acknowledges the complex challenges faced by persons with obesity.
In the examination of stigma in the present study, a staggering 99.1% of individuals reported experiencing stigma, with 71.9% describing it as mild and 26.7% as moderate. There were no significant correlations found between stigma and various variables, including BMI, age, gender, education, marriage, history of smoking and alcohol habits, and underlying diseases. However, a weakly positive correlation was identified between stigma and weight, suggesting that individuals facing more stigma tended to have higher weights. Further examination of stigma scales revealed that individuals with higher self-devaluation tended to have lower education, while those with greater height, weight, and age expressed more fear of being stigmatized. Consistent with past studies, persons with obesity commonly encounter stigma and are subjected to negative words and behaviors, as well as societal disregard and nonacceptance.52–56
The consequences of obesity stigma are profound, contributing to depression, anxiety, low self-esteem, body image concerns, overeating, avoidance of physical activity, self-harm, and even suicidal tendencies. 54 In alignment with our study, Pearl et al. reported that stigma, especially in the internalized stigma subscale, is prevalent among bariatric surgery candidates, leading to a range of mental issues and destructive behaviors, including depression, anxiety, exacerbated overweight, diminished motivation for weight loss, and diet abandonment. Notably, this stigma does not show a significant relationship with BMI. 57 Persons with obesity or overweight often face stereotypes portraying them as lazy, lacking willpower and self-discipline, unmotivated to improve their health, and personally blamed for their weight. 55 The reinforcement of these false stereotypes across various social settings, coupled with a lack of systematic efforts to challenge and counter these views, establishes a basis for social disapproval, stigma, and unjust treatment of persons with obesity. 57 In addition to the numerous social consequences, economic disparities, and psychological impacts of weight stigma, those who experience weight bias or discrimination may be more susceptible to engaging in risky health behaviors and experiencing outcomes that can exacerbate poor health and obesity. 58
This study explored the prevalence and interrelationships of depression, anxiety, perceived discrimination, and weight stigma among bariatric surgery candidates. While significant positive correlations emerged between BMI and both discrimination and stigma scores, no associations were found with categorical BMI groupings. Interestingly, depression severity exhibited a negative correlation with BMI, potentially due to the influence of comorbidities. Educational attainment moderated the link between BMI and depression, with lower education levels associated with a higher incidence. Anxiety primarily manifested as mild, with marriage linked to higher levels. Discrimination and stigma were highly prevalent, with stigma affecting nearly all participants. These findings underscore the complex interplay between obesity and mental health, highlighting the need for multifaceted interventions that address not only weight management but also psychological well-being, social stigma, and educational disparities. Future research should explore causal relationships and investigate the impact of interventions aimed at improving mental health and reducing stigma for persons with obesity. From a clinical perspective, the study’s findings underscore the importance of incorporating comprehensive psychosocial evaluations, including assessments of stigma and discrimination, into the routine preoperative assessment of bariatric surgery candidates. While existing protocols often screen for depression and anxiety, our data suggest that perceived weight-based stigma and discrimination are highly prevalent. These psychosocial stressors can negatively affect motivation, treatment adherence, and postoperative outcomes. In addition, identifying subgroups at higher risk, like individuals with lower education levels, may allow for more personalized interventions, such as targeted counseling, stigma reduction strategies, and enhanced psychological support.
Future studies are recommended to employ longitudinal designs to examine how these psychosocial variables evolve over time before and after surgery and how they influence long-term weight loss and psychological outcomes. Furthermore, qualitative investigations could provide deeper insights into the lived experiences of stigma and discrimination among bariatric candidates. Finally, evaluating the effectiveness of preoperative psychological interventions targeting stigma, depression, and anxiety may enhance mental health outcomes and overall surgical success.
Authors’ Contributions
S.S.B. and L.A.: Writing the draft of the article. S.S.B. and M.V.: Supervisors. L.A., M.B., and B.A.: Data gathering and data registry. R.R.: Writing the main article. M.V. and R.R.: data analysis. M.B.: Editing the main article. All authors reviewed and approved the final version of the article.
Footnotes
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
No funding was received for this article.
Ethics Approval and Consent to Participate
All participants were enrolled after describing the study and its purpose in an understandable way. Subsequently, written informed consent was obtained for participation in the study and its purpose and for providing written informed consent. This study was conducted as part of a research project following evaluation and approval from the Ethics Committee of the Shahid Beheshti University of Medical Sciences, with approval code IR.SBMU.MSP.REC.1400.120.
Availability of Data and Materials
The datasets used during the current study are available from the corresponding author upon reasonable request.
Consent for Publication
Written informed consent was obtained from participants for study publication.