
Abstract
The chromosomal band 17q12 is characterized by a high density of genes and is bordered by segmental duplications, the structural arrangement of which increases the susceptibility of the region to deletions and duplications. Duplication of 17q12 is a rare genetic condition associated with variable characteristics from clinically asymptomatic to intellectual disabilities, seizures, and behavioral problems. The variability in phenotype is primarily due to variable expressivity and incomplete penetrance. Diagnosis is mostly established by chromosomal microarray. Treatment involves a multidisciplinary approach. We present a case of a 43-year-old female who initially presented with hyperphagia and was eventually diagnosed with bulimia nervosa, anxiety, mood disorder, and personality disorder. Additional research is required to better understand the impact of 17q12 duplication syndrome on the development of bulimia nervosa since its pathogenesis has not been adequately described in the current literature.
Introduction
17q12 duplication syndrome is characterized by variable overlapping of neuropsychiatric and developmental disorders caused by the heterozygous microduplication of specific 1.4 Mb region on the q arm of chromosome number 17 at position one-two.1–3 The phenotype of microduplication syndrome is less understood and discussed than its counterpart, microdeletion syndrome. The clinical manifestation results from the changes in critical dose-sensitive genes or other singleton genes if duplication hampers its integrity. It varies from asymptomatic to neurodevelopmental disorders, including developmental delay, attention deficit hyperkinetic disorder, epilepsy, autism spectrum disorder, intellectual disabilities, behavioral problems (aggression and compulsion disorders), to multisystem anomalies and abnormalities.4–7 The duplication is commonly diagnosed by chromosomal microarray (CMA) and fails to be identified by karyotyping. 6 The treatment of choice is a multidisciplinary approach.
Although rare, 17q12 duplication syndrome is an underdiagnosed condition that clinician fails to diagnose on the first visit. The patient may be clinically asymptomatic or may present with minor multi-system abnormalities. It may lead to multiple unnecessary Emergency Department (ED) visits, multispecialty clinic visits, and needless follow-up examinations and investigations affect the quality of life of patients. Here we describe a case of 17q12 duplication syndrome with a particular focus on the complex neuropsychiatric manifestation, including depressive episodes, compulsive disorder, bulimia nervosa, anxiety, anger issues, mood dysregulation disorders, etc., to early diagnosis of the syndrome whose diagnosis is often underestimated given the often-mild phenotypic presentation. Furthermore, more research is required to better understand the role of 17q12 duplication syndrome in the pathogenesis of bulimia nervosa, which has not been reported in the literature.
Case report
A 43-year-old Caucasian female patient contacted triage seeking a referral to the Eating Disorder Unit as a result of her long-standing struggle with loss of control over overeating, which had worsened over the past decade. Her current body mass index indicated class three obesity. The patient was facing significant challenges associated with her obesity, including physical health complications such as arthritis and limited mobility, which contributed to depressive symptoms and intermittent suicidal thoughts. She had been on the waiting list for bariatric surgery for 3 years and anticipated another 5-year wait. Arthritis in both knees and hips severely limited the patient’s ability to perform household chores and attend to personal care. The extended wait for surgery had left her feeling overwhelmed, questioning her mental and physical capacity to endure such a lengthy delay. She also reported a complete lack of control over her eating habits. Furthermore, two of her three sons were receiving mental health services to recover from the trauma of witnessing their father’s death from epilepsy.
Despite these challenges, the patient had a supportive partner and three children whom she considered to be protective factors in her life. She described herself as somewhat functional, being able to perform basic household chores and shower once a week. She possessed a good knowledge of diet and nutrition and considered herself intelligent. The patient receives Centrelink payments and was reapplying for Disability Support Pension. Unfortunately, her children’s father passed away from an epileptic fit 10 years ago, necessitating ongoing mental health support for the children.
From a medical perspective, the patient had been diagnosed with hearing loss and a balance disorder caused by an acoustic neuroma, a type of brain tumor as well as arthritis that significantly limited her mobility. The patient had a chromosomal abnormality known as 17q12 duplication syndrome. Array comparative genomic hybridization (array CGH) detected a recurrent 1.4 Mb heterozygous duplication at chromosome 17q12, which is denoted according to ISCN (2020) nomenclature as arr[GRCh37] 17q12(36459259_37832869)x1. The duplication coincides 90% with the region assigned to the 17q12 duplication syndrome The patient had consulted a cardiologist in the past due to frequent fainting but the results of a Holter monitor test came back normal. She also reported Forestier’s disease, which caused back pain due to tendon and ligament issues.
During the assessment, the patient exhibited reasonably cooperative and polite behavior. While expressing some underlying irritability regarding the healthcare system’s waitlist, she maintained good eye contact, established rapport, and occasionally displayed a jovial demeanor and moments of laughter. Her speech was spontaneous and normal in tone, rate, and volume. There were no apparent formal thought disorders, and she articulated herself clearly. However, she also became tearful at one point. The patient actively sought help and specifically requested a referral to the eating disorder unit.
Regarding her mood, she rated it as 4–5 out of 10, with daily and rapid fluctuations. She reported a decrease in angry and tearful outbursts since starting an antidepressant. While expressing a strong desire to lose weight and fearing a loss of mobility, she described feeling helpless and hopeless, displaying eating disorder cognitions such as an inability to stop eating. She acknowledged trying bingeing and purging only once but denied the use of laxatives. The patient’s dietary plan consisted of having coffee for breakfast, with lunch and dinner typically consumed around 15:00 h. The amount of food she consumed varied, and once she started eating, she found it difficult to stop. She rarely exercises and does not engage in purging behaviors. She recognized that her weight restricts her ability to properly shower and perform household duties.
The provisional diagnosis for the patient includes Bulimia Nervosa, major depressive disorder (moderate depressive episode vs chronic adjustment disorder), anxiety, and borderline traits characterized by anger outbursts and lack of impulse control.
The patient received treatment involving Desvelnafaxine 50 mg, participated in eating disorder support groups, and underwent outpatient-based cognitive-behavioral therapy. The patient was also placed on a waitlist for bariatric surgery for a duration of 6 months. In addition, she participated in a complex case management program to address social aspects of her condition. Regular reviews by a nurse were conducted on a weekly basis, while doctor consultations occurred on a monthly basis. Despite improvement in mood, the patient continued to experience challenges related to physical health issues.
Discussion
17q12 deletion syndrome is well documented, but less is known about its counterpart, 17q12 duplication syndrome. Studies have associated the duplication with a wide range of phenotypes, including mild to severe intellectual and developmental delays, speech and motor delays, and varied neuropsychiatric presentations. Reported associations include autism spectrum disorder, schizophrenia, attention/behavioral issues, and physical anomalies. Further research is needed to better characterize the 17q12 duplication phenotypic spectrum.1,8,9 Obesity is a characteristic that has not been described very frequently in cases of this syndrome but, given the low number of cases reported, deserves attention. Describing the patient’s obesity could broaden the phenotypic spectrum associated with this syndrome. A few studies have linked 17q12 duplication to obesity, supporting obesity as a potential characteristic of this condition and may provide further insight into this rare syndrome.10,11
These 17q12 chromosome duplications and deletions are recurrent as these chromosomal imbalances depend on susceptible regions that are flanked by segmental duplications, called low copy repeats which undergo nonallelic homologous recombination. 12 This region is estimated to be 1.4 Mb which includes 17 RefSeq genes. 9
One gene that seems to be implicated is the Lhx1 gene which is proposed to be a dosage-sensitive gene for neuropsychiatric phenotypes in 17q12 genomic instability as it has been implicated in Purkinje cell differentiation and migration of motor axons. 6
17q12 duplication is a rare copy variant and is enriched in patients with intellectual disabilities. A deletion or duplication is pathogenic if it is higher in affected individuals when compared to normal individuals. 6 The phenotypic variability between parents who are unaffected and affected offspring is explained by incomplete penetrance, epigenetic variations, and the different sizes of duplication. 13
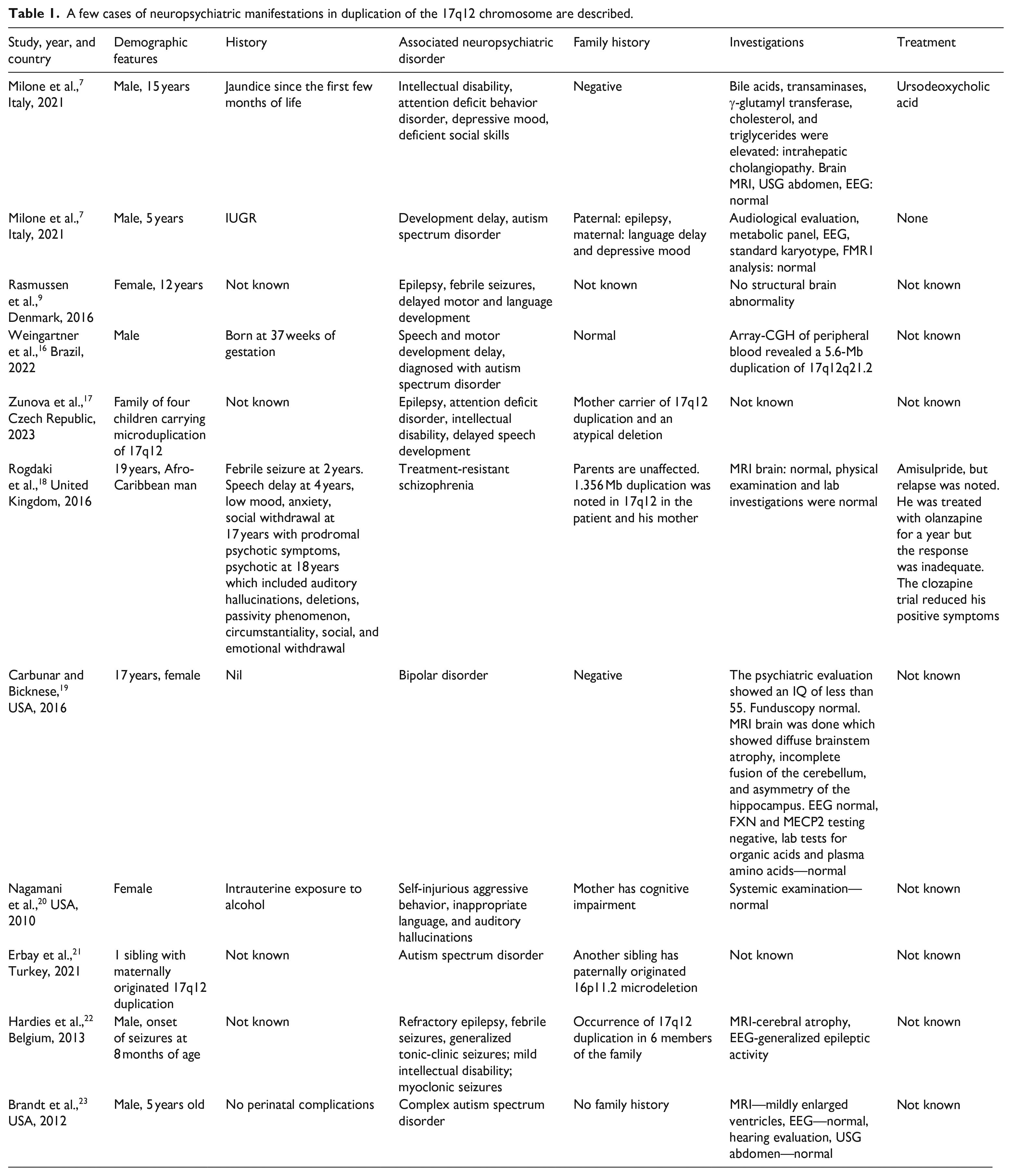
Psychiatric disorders like schizophrenia have also been to be linked to 17q12 duplication. In particular, the possibility that treatment resistance of schizophrenia could be linked to copy number variant should not be ruled out, which can suggest that this type of schizophrenia could be enriched for common risk alleles. 14 To diagnose these conditions, Array-CGH is used. G banded karyotype was used previously, but it was found that CMA yields a higher diagnostic yield (15%–20%) for genetic analysis due to its high sensitivity for submicroscopic duplications and deletions. 15 Treatment for these patients typically involves a multidisciplinary approach tailored to the individual’s specific clinical presentation. A coordinated care plan drawing from multiple specialties, such as psychiatry, psychology, occupational therapy, and social work, is commonly utilized based on the patient’s predominant symptoms (Table 1).
A few cases of neuropsychiatric manifestations in duplication of the 17q12 chromosome are described.
Limitation
A limitation of this study is the lack of whole-exome or whole-genome sequencing to fully characterize the patient’s genetic profile. While the CMA identified a 17q12 duplication, it is possible that other rare variants or a polygenic contribution could also be influencing the patient’s phenotype. The duplication may be an incidental finding, rather than the sole causative factor. Without exome/genome data, there could be additional variants missed that are relevant to the clinical presentation. Furthermore, recent evidence suggests many complex psychiatric conditions have a polygenic basis, yet a polygenic risk score was not calculated here. Additional genetic investigation, such as exome sequencing, would help address these limitations and more comprehensively evaluate the potential etiological role of both rare and common genetic variants in this case.
Conclusion
Multiple genetic factors have been identified to contribute to the development of neuropsychiatric conditions. At present, published reports include less than 100 individuals with the 17q12 duplication syndrome. Included in these reports are certain phenotypes, the most common of which is intellectual disability/developmental delay, sometimes associated with structural brain defects and seizures. The variability in clinical manifestations can be attributed to variable expressivity and reduced penetrance. To date, none of these reports have distinctly described bulimia nervosa. Given that our patient presented with neuropsychiatric manifestations of bulimia nervosa, depressive episodes, anxiety, and anger issues, the range of phenotypic manifestations of 17q12 duplication can be expanded. Further investigation is required to gain a better understanding of how the 17q12 duplication syndrome influences these neuropsychiatric presentations, as there is limited literature regarding this association.
Footnotes
Acknowledgements
The authors express their gratitude to the patient for her consent to publish this report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for her anonymized information to be published in this article. The patient regained fair insight and judgment over the course of her treatment regime to provide written informed consent by herself.