
Abstract
Few studies have compared the mental health, relationships, and gender dysphoria of male cross-dressers and transfeminine individuals. This research is important because evidence suggests that these two groups overlap and experience increased life challenges. In the present study, we examined differences in measures of mental health, relationships, and gender dysphoria between 519 male cross-dressers and 288 transfeminine individuals recruited online. In this study, we also examined differences between both groups (n = 807) and 293 cisgender men and 301 cisgender women from the general population. Transfeminine individuals reported more mental-health concerns and especially gender dysphoria than male cross-dressers. Furthermore, both groups reported more issues in mental health (e.g., psychological distress, autistic traits), relationships (e.g., less perceived social support), and gender dysphoria relative to cisgender men and women. Results highlight the clinical and scientific importance of clearly distinguishing male cross-dressers and transfeminine individuals when attending to their mental health, relationships, and gender dysphoria.
Keywords
Male cross-dressers were assigned male at birth, self-identify as men, and wear women’s clothing for emotional or sexual reasons and sometimes for entertainment purposes. Transfeminine individuals were assigned male at birth but presently identify as women, trans women, or another feminine identity. Studies have established an overlap between male cross-dressers and transfeminine individuals such that some male cross-dressers transition to living as transfeminine individuals and many transfeminine individuals previously lived as male cross-dressers (Blanchard et al., 1987; Buhrich & McConaghy, 1977; Docter & Fleming, 1992, 2001; Docter & Prince, 1997; Lawrence, 2013; Person & Ovesey, 1974; Wise & Meyer, 1980). The extent of this overlap remains unclear, however, because both male cross-dressers and transfeminine individuals are too often neglected in social-science research. This lack of research is concerning, especially considering that male cross-dressers and transfeminine individuals experience increased rates of psychological distress and other mental-health challenges (Beatrice, 1985; Bockting et al., 2013; Brown et al., 1996; Downing & Przedworski, 2018; Fagan et al., 1988; Långström & Zucker, 2005; Melendez et al., 2006; Newcomb et al., 2020; Nuttbrock et al., 2013; Warren et al., 2016; Wise et al., 1991; Zucker et al., 2012; for a recent review of mental-health disparities affecting transfeminine individuals, see Matouk et al., 2023). Indeed, one study found that 30% of transfeminine individuals had attempted suicide (Toomey et al., 2018).
To date, studies that focus specifically on male cross-dressers (e.g., Fagan et al., 1988) or transfeminine individuals (e.g., Melendez et al., 2006) have often relied on small sample sizes. Other studies have not clearly distinguished between male cross-dressers and transfeminine individuals (e.g., Bockting et al., 2013, Nuttbrock et al., 2013) or between trans individuals assigned male at birth and trans individuals assigned female at birth (e.g., Hanna et al., 2019). Because trans individuals are diverse with respect to their gender identity, sexual orientation, and presentation (Jacobson & Joel, 2019; Kuper et al., 2012), male cross-dressers and transfeminine individuals may face challenges distinct from each other and from trans individuals in general. Studies might benefit from examining the full spectrum of gender and sexual diversity in male cross-dresser, transfeminine, and related communities. Given one estimate that 3% of the general male population are cross-dressers (Långström & Zucker, 2005), it is important that research also attend to the specific challenges and needs of male cross-dressers so that they can be better understood and served.
Previous research suggests that male cross-dressers and transfeminine individuals may sometimes reflect differences in degree rather than kind (Blanchard, 1989; Blanchard et al., 1987; Docter & Fleming, 1992, 2001; Freund et al., 1982; Lawrence, 2009, 2013). However, few empirical studies have examined which factors are similar or different between male cross-dressers and transfeminine individuals. Furthermore, although several studies have reported on the mental health, relationships, and gender dysphoria (i.e., distress related to one’s assigned sex at birth) of transfeminine individuals (Downing & Przedworski, 2018; Newcomb et al., 2020; Nuttbrock et al., 2013; Toomey et al., 2018; Warren et al., 2016), there are few recent and comparable studies of male cross-dressers. In one study, Docter and Prince (1997) showed that male cross-dressers broadly experience difficulties as a result of shame and secrecy related to wearing women’s clothing or behaving in a feminine manner. In another study, male cross-dressers scored lower than transfeminine individuals on measures of gender dysphoria and public presentation as a woman (Docter & Fleming, 2001). Beatrice (1985) and Brown et al. (1996) also compared male cross-dressers and transfeminine individuals and found that the latter reported more psychiatric symptoms and a greater feminine gender role. Finally, a more recent study of clinically referred youths found that youths identified as either male cross-dressers or transfeminine had more difficulties with behavior, emotion, and peer relations than nonreferred youths, according to parental and self-report ratings (Zucker et al., 2012). Transfeminine youths were more likely to have difficulties in some of these areas and to exhibit higher levels of gender dysphoria than male cross-dressing youths.
In the present study, we addressed the above limitations by examining whether a broad range of mental-health factors, relationship quality, and gender dysphoria might differentiate male cross-dressers and transfeminine individuals and both groups from cisgender men and women in the general population. To address previous issues of low sample size and to improve gender and sexual diversity, in the present study, we recruited a large online sample from a wide range of male cross-dresser, transfeminine, and related communities to complete a survey that included measures of mental health, relationships, and gender dysphoria. Importantly and in contrast to many previous studies, we carefully distinguished between male cross-dressers and transfeminine individuals to establish the extent of their overlap and determine circumstances in which they might experience different challenges. We also included samples of both cisgender men and women from the general population for comparison.
Because of the potential overlap between some of our mental-health measures, we examined not only those differences across groups on each individual measure but also any patterns that might suggest some measures reflect broader constructs. We further examined whether some mental-health measures could be conceptualized as indicators of broader constructs by exploring their correlations. This construct-validation framework adds more cohesion and clarity to understanding the larger implications of our findings for helping male cross-dressers and transfeminine individuals. Our mental-health measures are likely to capture important aspects of mental health that are distinct but nevertheless function within interrelated nomological networks rather than in isolation, as suggested by hierarchical models of mental health, such as the Hierarchical Taxonomy of Psychopathology (Kotov et al., 2017, 2021). The results of this study will help male cross-dressers and transfeminine individuals and their health-care providers, partners, and loved ones to better understand how they are similar or different and to make more informed decisions about important issues, such as medical or social transition. By identifying both overlapping and distinct areas of need, clinicians and other health advocates can also design more appropriate interventions to support the diverse needs of these communities.
Transparency and Openness
Preregistration
This study was preregistered on the OSF: https://osf.io/pwsq4. The preregistration included our predictions, study design, sample-size specification, exclusion criteria, and data-analysis plan.
We describe analyses as exploratory if they deviated or extended beyond the preregistration. Furthermore, we deviated from the preregistration in the following two ways. First, we did not randomly split the different samples in half to create exploratory (training) and confirmation (testing) samples, and we did not use the former samples to develop models or predictions that could be applied to the latter samples. Because in the present study we focused on comparisons across groups on mental health, relationships, and gender dysphoria, developing more complex models or predictions from the data was beyond its scope. We intend to pursue this analytic approach in a future study. Second, we did not compare the mean of the effect sizes that resulted from comparisons on the different measures between male cross-dressers and transfeminine individuals with the means of the effect sizes that resulted from those same comparisons between male cross-dressers and transfeminine individuals and cisgender men and women from the general population. We were concerned about the redundancy of these analyses with those comparing groups on a composite variable that represented the mean of all standardized scores (see the section “Testing overall differences between groups on a composite variable” in the Results). Importantly, comparing groups on the composite variable is much more statistically powerful because it uses individual-level data rather than group-level data (i.e., standardized scores across all measures for each participant rather than effect sizes for each comparison or test). The sample sizes are as large as the different samples themselves when comparing groups on the composite variable, whereas the effective sample sizes when comparing effect sizes are equal only to the number of measures, which is 14.
We originally preregistered this study after collecting data from 4,305 respondents who were recruited for potential inclusion in the sample of male cross-dressers and transfeminine individuals. Following data collection from an additional 962 respondents who were recruited for the same reason, we updated the preregistration with a few changes, most importantly adding a sample of cisgender women from the general population for comparison. At the time of the original preregistration, we expected that funding would be available for only a sample of cisgender men from the general population to compare with male cross-dressers and transfeminine individuals. We later managed to secure additional funding, however, to also collect data from cisgender women. Neither sample of cisgender men or women was recruited before the original or updated preregistration, nor did anyone from the research team download, examine, or analyze any of the data before the original or updated preregistration.
Data, materials, code, and online resources
This study does not have ethical approval to make de-identified data publicly available. The informed consent also states that data are accessible only by the research team. Interested researchers may contact K. J. Hsu to discuss the possibility of sharing data.
Materials used in this study (e.g., measures) can be accessed through the references provided and at the following link, which contains all measures in full: https://osf.io/5gnfc. The study analysis code can be accessed as R script files at the same link. The R script files include the code for independent samples Welch’s t tests that compared male cross-dressers with transfeminine individuals and both groups with cisgender men and women from the general population on all measures of mental health, relationships, and gender dysphoria and the composite variable. The R script files also include the code for multiple regression analyses that compared groups analogously on those same measures and the composite variable while also controlling for demographic characteristics that significantly differed among them. Finally, the R script files include the code for computing measures of effect sizes for each comparison. Other resources are in the Supplemental Material available online.
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Ethical approval
All study procedures were approved by Pennsylvania State University’s Institutional Review Board.
Method
Participants
Male cross-dresser and transfeminine sample
Participants were 807 adults assigned male at birth (age: M = 30.70 years, SD = 11.06, range = 18–76). Out of these participants, 519 (64.31%) were male cross-dressers, and 288 (35.69%) were transfeminine individuals. Participants were categorized as cross-dressers if they identified their gender as male/man and reported a frequency greater than “never” on a 7-point scale (1 = never, 7 = daily) in response to the question, “In the past 12 months, how often have you dressed in women’s clothing for any reason, either in private or in public?” Participants were categorized as transfeminine if they identified their gender as female/woman or transfeminine/trans woman.
This sample included baseline data from a larger longitudinal study of male cross-dressers, transfeminine individuals, and others assigned male at birth who are broadly interested in the idea of presenting as or being women. This larger study will examine not only the developmental trajectory of their mental health, relationships, gender dysphoria, sexuality, identity, and personality over time but also whether changes in one area predict important and clinically relevant outcomes in other areas. Because in the present study we focused on comparing male cross-dressers with transfeminine individuals and both groups with cisgender men and women, we limited the analytic sample from the larger longitudinal study to only the 807 participants who met inclusion criteria for categorization as either a male cross-dresser (n = 519) or a transfeminine individual (n = 288). Out of the participants who were excluded from the larger longitudinal study, the majority (n = 279) were excluded for identifying with a gender other than male/man, female/woman, or transfeminine/trans woman, such as questioning (n = 136), nonbinary/enby (n = 55), or gender-fluid (n = 55). Another 101 participants identifying as male/man were excluded for reporting a frequency of “never” to the question about how often they dressed in women’s clothing in the past 12 months.
Cisgender samples
Participants in the samples from the general population were 293 cisgender men (age: M = 33.88 years, SD = 10.66, range = 18–73) and 301 cisgender women (age: M = 36.34 years, SD = 12.84, range = 19–73). Even though male cross-dressers are also cisgender men, we refer hereafter to the samples from the general population as the “cisgender samples” for lack of a better term to distinguish them from the male cross-dresser and transfeminine samples. For simplicity, it can also be assumed that when we refer to either cisgender men or women, we mean participants recruited from the general population. Participants were included in the sample of cisgender men if they identified their gender as male/man and reported that they were assigned male at birth. Likewise, participants were included in the sample of cisgender women if they identified their gender as female/woman and reported that they were assigned female at birth.
Procedure
Male cross-dressers and transfeminine participants were recruited for an online survey via advertisements placed in Facebook groups, Reddit communities, Discord servers, and other websites or forums that specifically cater to male cross-dressers, transfeminine people, or both. Advertisements specified that eligible participants must be 18 years or older and that we were “recruiting cross-dressers, transfeminine people, and others broadly interested in the idea of presenting as or being women for a study that will examine gender, sexuality, identity, personality, and mental health within these communities.” A total of 5,267 people showed interest in the study by clicking on a link in one of the advertisements that directed them to the informed-consent page and the start of the online survey. Respondents were screened out of the survey if they did not report that they were at least 18 years old (n = 109), did not report that they were assigned male at birth (n = 7), or declined consent to participating in the study (n = 20). Another 3,890 participants were excluded from the final sample because they did not progress beyond 95% of the online survey, which is automatically recorded by Qualtrics under the variable “Progress.” Out of participants excluded for not progressing beyond 95% of the survey, 1,320 (33.93%) did not progress beyond the informed-consent page, and 2,949 (75.81%) did not progress beyond 15% of the survey. There was no compensation for male cross-dressers and transfeminine participants.
Cisgender men and women were recruited for an online survey via advertisements placed on Prolific (https://prolific.co), a crowdsourcing website that connects paid volunteers with researchers who are looking for participants to complete their studies. Prolific has shown the highest data quality compared with similar platforms commonly used by social-science researchers (Douglas et al., 2023; Peer et al., 2022). Advertisements specified that eligible participants must be 18 years or older and that we were “recruiting cisgender men and cisgender women for a study that will compare their gender, sexuality, identity, personality, and mental health with those of cross-dressers and transfeminine people.” A total of 617 people showed interest in the study by clicking on a link in one of the advertisements that directed them to the informed-consent page and the start of the online survey. Respondents were screened out of the survey if they did not report that they were at least 18 years old (n = 1) or identified their gender as nonbinary (n = 3). Cisgender men and women were each compensated USD$10.00.
We excluded 12 participants from the male cross-dresser and transfeminine sample and 16 participants from the cisgender samples because they provided the same rating to all items on at least two of the following three measures that were included in the survey: Short Autism Spectrum Quotient (Allison et al., 2012), Childhood Gender Nonconformity Scale (Bailey et al., 1995), and Socially Desirable Response Set Five-Item Survey (Hays et al., 1989). K. J. Hsu and J. S. Morandini also looked for general patterns in the data and independently coded each participant’s responses on the survey for whether they were not serious or otherwise inappropriate and for whether too many questions were left incomplete. A participant’s responses were coded as not being serious or otherwise inappropriate based on obvious patterns of such responses in their open-ended data (e.g., “Shrek” as their answer to multiple questions with text entry). A participant’s responses were coded as having too many questions not answered based on observing that a large section of questions (e.g., all measures of mental health) were skipped even though the participant proceeded to the end of the survey and were therefore not excluded through the “Progress” metric recorded by Qualtrics. Both K. J. Hsu and J. S. Morandini agreed that 36 participants from the male cross-dresser and transfeminine sample and three participants from the cisgender samples met at least one of these two criteria, and those participants were excluded from all analyses. K. J. Hsu coded an additional six participants from the male cross-dresser and transfeminine sample as having met at least one of the two criteria, but J. S. Morandini did not; K. J. Hsu and J. S. Morandini discussed those cases and reached a consensus that they should be excluded.
The exclusions resulted in a final sample of 1,187 participants who provided baseline data for the larger longitudinal study, which was further limited to the 807 male cross-dressers and transfeminine participants for the present study. The exclusions also resulted in samples of 293 cisgender men and 301 cisgender women who provided data for the present study.
Measures
Male cross-dresser and transfeminine participants and the cisgender male and female participants completed the same online survey, which was estimated to take about 1 hr. The survey was completed anonymously on a secure server hosted by Qualtrics using personal electronic devices. Although it was more extensive, the relevant parts of the survey for the present study included demographic questions and measures of mental health, relationships, and gender dysphoria.
Demographics
All participants reported the following demographic characteristics: age in years, the country in which they currently reside, race/ethnicity, education, romantic-relationship status, sexual-orientation identity, gender identity, and sex assigned at birth. For race/ethnicity, participants selected one or more options from White/Caucasian, Black/African American, Hispanic or Latino/a/x, East Asian/Pacific Islander, South Asian, Native American, and other race/ethnicity. If participants selected multiple options, they were categorized as multiracial/ethnic. For education, participants selected the highest level of education that they completed from a list that included less than high school, some high school, high school/GED, some college, bachelor’s degree, master’s degree, and doctoral/professional degree. For romantic-relationship status, participants selected from the following options: single, in a relationship, engaged, married, divorced, and widowed. For sexual-orientation identity, participants were asked what sexual orientation they identify, feel, present, or live most of the time and to choose one of the following labels: heterosexual/straight, bisexual, gay/lesbian, asexual, pansexual, and other. Likewise for gender identity, participants were asked what gender they identify, feel, present, or live most of the time and to choose one of the following categories: male/man, female/woman, transfeminine/trans woman, transmasculine/trans man, nonbinary/enby, gender-fluid, questioning, agender, and other. For sex assigned at birth, participants selected one option from male, female, or other.
Mental health
Satisfaction With Life Scale
The Satisfaction With Life Scale (Diener et al., 1985) is a five-item measure of global life satisfaction. Participants responded to statements on a 7-point scale (1 = strongly disagree, 7 = strongly agree). Total scores are calculated by taking the sum of ratings for all five items (range = 5–35). Higher scores reflect more global life satisfaction. Example items include “In most ways my life is close to my ideal” and “The conditions of my life are excellent.” Using Cronbach’s alpha, we found that the reliability of this measure among the different samples ranged from .88 to .93.
Rosenberg Self-Esteem Scale
The Rosenberg Self-Esteem Scale (Rosenberg, 1965) is a 10-item measure of self-esteem. Participants rated how much they agreed or disagreed with statements about themselves and their self-worth on a 4-point scale (0 = strongly disagree, 3 = strongly agree). Total scores are calculated by taking the sum of ratings for all 10 items; there were five reverse-scored items. Thus, the range is 0 to 30. Higher scores reflect more positive self-esteem. Example items include “I feel that I have a number of good qualities” and “I wish I could have more respect for myself” (reverse-scored). Using Cronbach’s alpha, we found that the reliability of this measure among the different samples ranged from .90 to .93.
Depression, Anxiety, and Stress Scale–21
The Depression, Anxiety, and Stress Scale–21 (Lovibond & Lovibond, 1995) is a 21-item measure of symptoms of depression, anxiety, and stress. Participants rated how much statements about different symptoms applied to them in the past week on a 4-point scale (0 = did not apply to me at all, 3 = applied to me very much or most of the time). Total scores are calculated by taking the sum of ratings for all 21 items and then doubling that number, resulting in a range from 0 to 126. Higher scores indicate more depression, anxiety, and stress. Example items include “I found it hard to wind down” and “I couldn’t seem to experience any positive feeling at all.” Using Cronbach’s alpha, we found that the reliability of this measure among the different samples ranged from .93 to .94.
Short Autism Spectrum Quotient
The Short Autism Spectrum Quotient (Allison et al., 2012) consists of 10 items assessing for autistic traits in the general population. Participants indicated their agreement or disagreement with statements on a 4-point scale that included definitely disagree, slightly disagree, slightly agree, and definitely agree. Responses to each item were dichotomously coded as 1 if they were definitely agree or slightly agree and 0 if they were definitely disagree or slightly disagree. Six items are reverse-scored such that responses were dichotomously coded in the opposite direction. Total scores are calculated by taking the sum of all 10 items after dichotomously coding their responses, resulting in a range of 0 to 10. Higher scores indicate more autistic traits. Example items include statements such as “I often notice small sounds when others do not” and “I find it easy to work out what someone is thinking or feeling just by looking at their face” (reverse-scored). Using Cronbach’s alpha, we found that the reliability of this measure ranged from .49 for cisgender men and .66 for cisgender women to .58 for male cross-dressers and .74 for transfeminine participants. Although the internal consistency of this measure was low for cisgender men, it is consistent with previous findings (e.g., Jia et al., 2019).
Suicidal Behaviors Questionnaire–Revised
The Suicidal Behaviors Questionnaire–Revised (Osman et al., 2001) consists of four items assessing suicidal behaviors and ideation. Participants in the present study completed only the first two items of this measure because we were concerned about the other two items, which would have asked participants whether they had ever told someone else about a suicide attempt and how likely they were to attempt suicide in the future. Participants might not have responded honestly if they worried about being reported to authorities for indicating that they were likely to attempt suicide in the future. For the first item, participants responded to the question “Have you ever thought about or attempted to kill yourself?” on a 6-point scale (1 = never, 6 = I have attempted to kill myself and really hoped to die). For the second item, participants responded to the question “How often have you thought about killing yourself in the past year?” on a 5-point scale (1 = never, 5 = very often [5 or more times]). Total scores are calculated by taking the average of ratings for the two items. Higher scores reflect more suicidal behaviors and ideation. Using Cronbach’s alpha, we found that the reliability of this measure ranged from .57 for transfeminine participants and .68 for male cross-dressers to .64 for cisgender women and .74 for cisgender men.
Alcohol Use Disorders Identification Test–Consumption
The Alcohol Use Disorders Identification Test–Consumption (Bush et al., 1998) consists of three questions about alcohol-use frequency (“How often do you have a drink containing alcohol?”), alcohol quantity (“How many standard drinks containing alcohol do you have on a typical day when you are drinking?”), and excessive alcohol use (“How often do you have 6 or more standard drinks on a single occasion?”). Participants responded to each question on a 5-point scale, which differed by whether the question asked about alcohol-use frequency (0 = never, 4 = 4 or more times a week), alcohol quantity (0 = 1–2, 4 = 10 or more), or excessive alcohol use (0 = never, 4 = daily or almost daily). Participants did not see or respond to the second and third questions if they answered “never” to the first question. For each participant, their total score on this measure is the sum of their responses, and the range is 0 to 12. Higher scores indicate more alcohol use and potentially problematic drinking. Using Cronbach’s alpha and excluding participants who answered “never” to the first question because they did not see the other two questions, we found that the reliability of this measure among the different samples ranged from .64 to .71.
Drug Abuse Screening Test
The Drug Abuse Screening Test (Skinner, 1982) consists of 10 questions about experiences of nonalcoholic drug abuse or dependence in the past 12 months. Participants responded either “yes” or “no” (dichotomously coded as 1 or 0, respectively) to each question, and there was one question reverse-scored and dichotomously coded in the opposite direction. They were also informed that questions do not concern alcohol abuse or dependence and provided a list of possible substances that may apply (e.g., marijuana, psilocybin, ketamine, cocaine, heroin). Total scores are calculated by taking the sum of all 10 items, resulting in a range of 0 to 10. Higher scores indicate more drug abuse or dependence. Example questions include “Have you ever experienced withdrawal symptoms (felt sick) when you stopped taking drugs?” and “Are you always able to stop using drugs when you want to?” (reverse-scored). Using Cronbach’s alpha, we found that the reliability of this measure ranged from .71 for male cross-dressers and .74 for transfeminine participants to .82 for cisgender men and .84 for cisgender women.
Health-Related Quality of Life Scale
The Health-Related Quality of Life Scale was developed by the Centers for Disease Control and Prevention (2000). It includes four questions about general health and the number of days during the past 30 days that a participant was physically unhealthy, mentally unhealthy, or limited in doing their usual activities. For the present study, we examined data only for the first question, which asked, “Would you say that in general your health is excellent, very good, good, fair, or poor?” Participants responded on a 5-point scale (1 = poor, 5 = excellent). We did not calculate reliability because of our focus on this single question.
Relationships
Couples Satisfaction Index–4
The Couples Satisfaction Index–4 (Funk & Rogge, 2007) is a four-item measure of participants’ perceived satisfaction with their romantic relationship. Participants rated three items on a 6-point scale (0 = not at all, 5 = completely) and one item about their degree of happiness with the relationship on a 7-point scale (0 = extremely unhappy, 6 = perfect). Total scores are calculated by taking the sum of ratings for all four items such that the range is 0 to 21. Higher scores reflect more satisfaction with the relationship. Example items include “I have a warm and comfortable relationship with my partner” and “In general, how satisfied are you with your relationship?” Only participants who indicated that they were currently in a relationship, engaged, or married completed this measure. Using Cronbach’s alpha, we found that the reliability of this measure among the different samples ranged from .93 to .95.
Multidimensional Scale of Perceived Social Support
The Multidimensional Scale of Perceived Social Support (Zimet et al., 1988) is a 12-item measure of participants’ perceptions of social support from family, friends, and significant others. Participants indicated their agreement or disagreement with statements on a 7-point scale (1 = very strongly disagree, 7 = very strongly agree). Total scores are calculated by taking the average rating across all items. Higher scores reflect more perceived social support from others. Example items include “There is a special person who is around when I am in need,” “I get the emotional help and support I need from my family,” and “My friends really try to help me.” Using Cronbach’s alpha, we found that the reliability of this measure among the different samples ranged from .91 to .95.
Gender dysphoria
Utrecht Gender Dysphoria Scale – Gender Spectrum
The Utrecht Gender Dysphoria Scale – Gender Spectrum (McGuire et al., 2020) is an 18-item measure of gender dysphoria, revised from a previous version to be inclusive of all gender identities and expressions. It can be used longitudinally and at any stage of medical or social transition. Participants rated how much they agreed or disagreed with statements about dissatisfaction with their assigned sex at birth and comfort with their current or affirmed gender identity on a 5-point scale (1 = disagree completely, 5 = agree completely). Total scores are calculated by taking the average rating across all items. Higher scores reflect more feelings of gender dysphoria. Example items include “Every time someone treats me like my assigned sex, I feel hurt” and “I feel unhappy because I have the physical characteristics of my assigned sex.” Using Cronbach’s alpha, we found that the reliability of this measure ranged from .75 for cisgender women and .80 for cisgender men to .90 for male cross-dressers and .93 for transfeminine participants.
Single-item measures
All participants responded either “yes” or “no” (dichotomously coded as 1 or 0, respectively) to questions about whether they had ever experienced gender dysphoria, had gender-affirming medical interventions, or taken steps toward social transition. Because each of these three questions comprised its own single-item measure, we did not calculate reliability.
Data analyses
First, we created two between-groups contrasts that were orthogonal and thus statistically independent: Contrast 1 compared male cross-dressers with transfeminine participants, and Contrast 2 compared both male cross-dressers and transfeminine participants with cisgender men. Because we wanted to compare male cross-dressers and transfeminine participants not only with each other and cisgender men but also cisgender women, we created a third between-groups contrast. Contrast 3 was orthogonal to Contrast 1 but not Contrast 2, comparing both cross-dressers and transfeminine participants with cisgender women.
Next, we examined differences in the measures of mental health, relationships, and gender dysphoria using a series of planned comparisons for each of the three between-groups contrasts. We used only independent samples Welch’s t tests, which rely on the unpooled rather than the pooled error variance because they improve performance when sample sizes and variances are unequal between groups and they also produce the same result when sample sizes and variances are equal (Delacre et al., 2017). For the following measures, tests were one-tailed in the direction of male cross-dressers (Contrast 1), cisgender men (Contrast 2), or cisgender women (Contrast 3) because it was expected that they would score higher: the Satisfaction With Life Scale (Diener et al., 1985), the Rosenberg Self-Esteem Scale (Rosenberg, 1965), the first question from the Health-Related Quality of Life Scale (Centers for Disease Control and Prevention, 2000), the Couples Satisfaction Index–4 (Funk & Rogge, 2007), and the Multidimensional Scale of Perceived Social Support (Zimet et al., 1988). For all other measures, tests were one-tailed in the direction of transfeminine participants (Contrast 1) or both male cross-dressers and transfeminine participants (Contrasts 2 and 3) because it was expected that they would score higher. These predictions were preregistered and based on the limited research examining differences between male cross-dressers and transfeminine individuals (Beatrice, 1985; Brown et al., 1996; Docter & Fleming, 2001; Zucker et al., 2012) or their mental-health disparities (e.g., Bockting et al., 2013; Melendez et al., 2006).
In addition to presenting the results of independent samples Welch’s t tests comparing male cross-dressers with transfeminine participants (Contrast 1) and both groups with cisgender men and women (Contrasts 2 and 3), we report Cohen’s d and its 95% confidence interval (CI) as measures of effect size for every comparison. To correct for Type 1 error from multiple comparisons, we applied the Bonferroni correction, which was easy to implement, straightforward to interpret, and already familiar to us. Because we preregistered a total of 100 tests in anticipation of examining differences in more measures than those reported in this study, we considered only p < .0005 (p < .05 / 100 tests) as statistically significant. We report the results comparing groups on measures of sexuality and attitudes as separate studies, keeping the focus on mental health, relationships, and gender dysphoria in the present study.
Finally, we excluded participants from any test if they were missing more than 25% of the data relevant to that analysis. Based on this exclusion criterion, participants were excluded for missing any data if a test compared groups on a measure with fewer than four items. We replaced participants’ missing values on a measure with the mean of the values that they did report if they were missing 25% or less of the data. For measures computed with a sum score, we rounded to the nearest whole number. Data were analyzed using R (Version 4.2.3; R Core Team, 2023) and the packages lsr (Version 0.5.2; Navarro, 2021), rstatix (Version 0.7.2; Kassambara, 2023), and ggplot2 (Version 3.4.3; Wickham et al., 2023).
Results
Demographic differences
Table 1 presents demographic characteristics for male cross-dressers and transfeminine participants, both together as a combined sample and separately, and those for cisgender men and women. For the details of statistical tests examining demographic differences between groups, see the Supplemental Material. We report details such as effect sizes in Cohen’s d or odds ratio and their 95% CIs.
Demographic Characteristics of Male Cross-Dressers, Transfeminine Individuals, Cisgender Men, and Cisgender Women

To summarize the demographic differences, male cross-dressers were significantly older, more likely to have identified as heterosexual/straight, and less likely to have identified as bisexual than transfeminine participants (all ps < .005). Male cross-dressers and transfeminine participants did not significantly differ in how likely they reported being White/Caucasian or being in a relationship, engaged, or married (both ps > .3933). As a combined sample, male cross-dressers and transfeminine participants were significantly younger, more likely to have identified as White/Caucasian, and less likely to have identified as heterosexual/straight than either cisgender men or women (all ps < .0001). In addition, compared only with cisgender women but not men, male cross-dressers and transfeminine participants were significantly less likely to have reported being in a relationship, engaged, or married (p < .0001). Finally, there were no significant differences between any groups in how likely they were to have reported living in the United States and completing either some college or a bachelor’s-degree level of education (all ps > .0517).
Contrast 1: Male cross-dressers versus transfeminine participants
Table 2 presents the means, standard deviations, effect sizes, and results of independent samples Welch’s t tests for Contrast 1, which compared male cross-dressers with transfeminine participants on the measures of mental health, relationships, and gender dysphoria. Figure 1a shows the effect sizes as a forest plot, ordered from those largest for transfeminine participants to those largest for male cross-dressers.
Means, Standard Deviations, Effect Sizes, and Results of Independent Samples Welch’s t Tests Comparing Male Cross-Dressers With Transfeminine Individuals on Measures of Mental Health, Relationships, and Gender Dysphoria
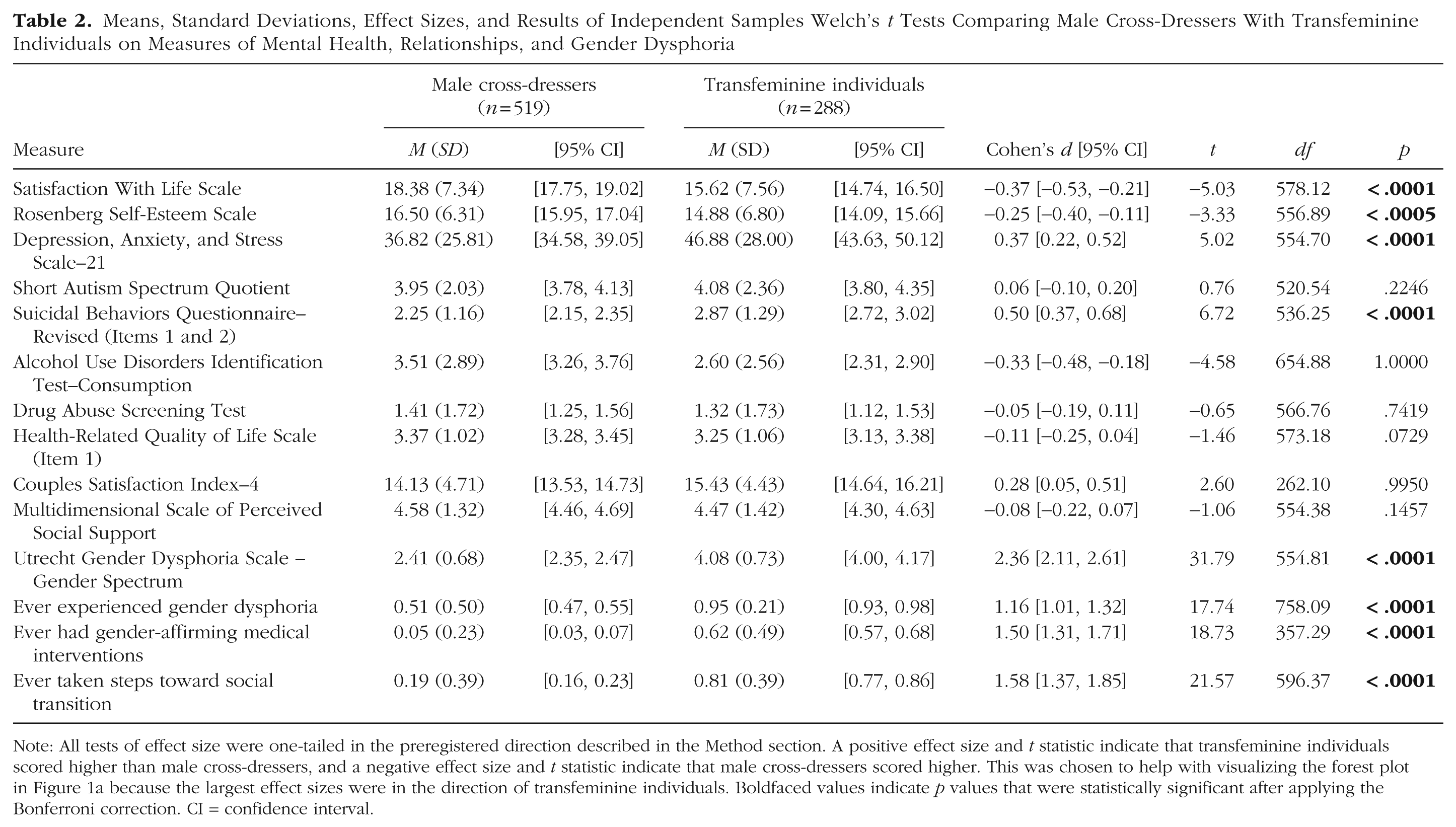
Note: All tests of effect size were one-tailed in the preregistered direction described in the Method section. A positive effect size and t statistic indicate that transfeminine individuals scored higher than male cross-dressers, and a negative effect size and t statistic indicate that male cross-dressers scored higher. This was chosen to help with visualizing the forest plot in Figure 1a because the largest effect sizes were in the direction of transfeminine individuals. Boldfaced values indicate p values that were statistically significant after applying the Bonferroni correction. CI = confidence interval.

Forest plots of effect sizes comparing male cross-dressers with transfeminine individuals and both groups with cisgender men and women on measures of mental health, relationships, and gender dysphoria. (a) Forest plot of effect sizes comparing male cross-dressers (n = 519) with transfeminine individuals (n = 288). (b) Forest plot of effect sizes comparing male cross-dressers and transfeminine individuals (n = 807) with cisgender men (n = 293). (c) Forest plot of effect sizes comparing male cross-dressers and transfeminine individuals with cisgender women (n = 301). Points represent effect sizes as Cohen’s d. Left and right lines represent 95% confidence intervals. Positive values indicate that transfeminine individuals scored higher than (a) male cross-dressers or male cross-dressers and transfeminine individuals scored higher than either (b) cisgender men or (c) cisgender women. Negative values indicate the reverse patterns.
As predicted, male cross-dressers scored significantly higher than transfeminine participants on global life satisfaction and self-esteem, and transfeminine participants scored significantly higher on depression, anxiety, and stress; suicidal behaviors and ideation; feelings of gender dysphoria; and the single-item measures of having ever experienced gender dysphoria, had gender-affirming medical interventions, or taken steps toward social transition. Effect sizes ranged from d = −0.37, 95% CI = [−0.53, −0.21], in the direction of male cross-dressers for global life satisfaction to d = 2.36, 95% CI = [2.11, 2.61], in the direction of transfeminine participants for feelings of gender dysphoria. Contrary to expectations, male cross-dressers scored higher than transfeminine participants on alcohol use, and transfeminine participants scored higher on relationship satisfaction. There were also no significant differences between the two groups on autistic traits, drug abuse or dependence, general health, and perceived social support.
A post hoc sensitivity analysis revealed that the minimum detectable effect size was d = 0.18 in either direction for comparing our sample of male cross-dressers (n = 519) with transfeminine participants (n = 288) at an alpha level of .05 and 80% power. Except for autistic traits, drug abuse or dependence, general health, and perceived social support, all observed differences between the two groups were larger than the minimum detectable effect size and followed our predictions.
Contrast 2: male cross-dressers and transfeminine participants versus cisgender men
Table 3 presents the means, standard deviations, effect sizes, and results of independent samples Welch’s t tests for Contrast 2, which compared both male cross-dressers and transfeminine participants with cisgender men on the measures of mental health, relationships, and gender dysphoria. Figure 1b shows the effect sizes as a forest plot, ordered from those largest for male cross-dressers and transfeminine participants to those largest for cisgender men.
Means, Standard Deviations, Effect Sizes, and Results of Independent Samples Welch’s t Tests Comparing Male Cross-Dressers and Transfeminine Individuals With Cisgender Men on Measures of Mental Health, Relationships, and Gender Dysphoria

Note: All tests of effect size were one-tailed in the preregistered direction described in the Method section. A positive effect size and t statistic indicate that male cross-dressers and transfeminine individuals scored higher than cisgender men, and a negative effect size and t statistic indicate that cisgender men scored higher. This was chosen to help with visualizing the forest plot in Figure 1b because the largest effect sizes were in the direction of male cross-dressers and transfeminine individuals. Boldfaced values indicate p values that were statistically significant after applying the Bonferroni correction. CI = confidence interval.
As predicted, male cross-dressers and transfeminine participants scored significantly higher than cisgender men on depression, anxiety, and stress; autistic traits; suicidal behaviors and ideation; drug abuse or dependence; feelings of gender dysphoria; and the single-item measures of having ever experienced gender dysphoria, had gender-affirming medical interventions, or taken steps toward social transition. Also as predicted, cisgender men scored significantly higher on global life satisfaction, self-esteem, relationship satisfaction, and perceived social support. Effect sizes ranged from d = −0.47, 95% CI = [−0.61, −0.33], in the direction of cisgender men for self-esteem to d = 1.84, 95% CI = [1.65, 2.01], in the direction of male cross-dressers and transfeminine participants for having ever experienced gender dysphoria. Contrary to expectations, there were no significant differences comparing male cross-dressers and transfeminine participants with cisgender men on alcohol use and general health.
A post hoc sensitivity analysis revealed that the minimum detectable effect size was d = 0.17 in either direction for comparing our samples of male cross-dressers and transfeminine participants (n = 807) with cisgender men (n = 293) at an alpha level of .05 and 80% power. Except for alcohol use and general health, all observed differences between the two groups were larger than the minimum detectable effect size and followed our predictions.
Contrast 3: male cross-dressers and transfeminine participants versus cisgender women
Table 4 presents the means, standard deviations, effect sizes, and results of independent samples Welch’s t tests for Contrast 3, which compared both male cross-dressers and transfeminine participants with cisgender women on the measures of mental health, relationships, and gender dysphoria. Figure 1c shows the effect sizes as a forest plot, ordered from those largest for male cross-dressers and transfeminine participants to those largest for cisgender women.
Means, Standard Deviations, Effect Sizes, and Results of Independent Samples Welch’s t Tests Comparing Male Cross-Dressers and Transfeminine Individuals With Cisgender Women on Measures of Mental Health, Relationships, and Gender Dysphoria

Note: All tests of effect size were one-tailed in the preregistered direction described in the Method section. A positive effect size and t statistic indicate that male cross-dressers and transfeminine individuals scored higher than cisgender women, and a negative effect size and t statistic indicate that cisgender women scored higher. This was chosen to help with visualizing the forest plot in Figure 1c because the largest effect sizes were in the direction of male cross-dressers and transfeminine individuals. Boldfaced values indicate p values that were statistically significant after applying the Bonferroni correction. CI = confidence interval.
As predicted, male cross-dressers and transfeminine participants scored significantly higher than cisgender women on depression, anxiety, and stress; autistic traits; suicidal behaviors and ideation; alcohol use; drug abuse or dependence; feelings of gender dysphoria; and the single-item measures of having ever experienced gender dysphoria, ever had gender-affirming medical interventions, or ever taken steps toward social transition. Also as predicted, cisgender women scored significantly higher on global life satisfaction, self-esteem, and perceived social support. Effect sizes ranged from d = −0.56, 95% CI = [−0.70, −0.42], in the direction of cisgender women for perceived social support to d = 1.67, 95% CI = [1.47, 1.85], in the direction of male cross-dressers and transfeminine participants for having ever experienced gender dysphoria. Contrary to expectations, there were no significant differences comparing male cross-dressers and transfeminine participants with cisgender women on general health and relationship satisfaction.
A post hoc sensitivity analysis revealed that the minimum detectable effect size was d = 0.17 in either direction for comparing our samples of male cross-dressers and transfeminine participants (n = 807) with cisgender women (n = 301) at an alpha level of .05 and 80% power. Except for general health, all observed differences between the two groups were larger than the minimum detectable effect size and followed our predictions.
Testing the robustness of contrast findings with multiple regression
We followed up the preregistered analyses with a set of exploratory analyses that compared male cross-dressers with transfeminine participants (Contrast 1) and both groups with cisgender men and women (Contrasts 2 and 3) on the measures of mental health, relationships, and gender dysphoria while also controlling for demographic characteristics that significantly differed across the groups. For example, male cross-dressers were significantly older than transfeminine participants, and both groups were significantly younger than either the cisgender men or women. Male cross-dressers and transfeminine participants were also significantly more likely to have identified their race/ethnicity as White/Caucasian and significantly less likely to have identified their sexual orientation as heterosexual/straight compared with either of the cisgender samples.
Because multiple regression analyses were exploratory and tested the robustness of our findings from the preregistered analyses after controlling for demographic differences, the details of these analyses can be found in the Supplemental Material available online, which includes information about the predictors, dummy coding, and contrast codes that were used. Results of the multiple regression analyses are presented in Tables S1 through S3 in the Supplemental Material. In general, previously observed differences between male cross-dressers and transfeminine participants (Contrast 1) held even when accounting for age, race/ethnicity, and sexual orientation. One notable exception to this pattern was that transfeminine participants were even less likely to have reported drug abuse or dependence relative to male cross-dressers, with a decreased 0.13 SD in effect size. Likewise, previously observed differences between both male cross-dressers and transfeminine participants and either cisgender men (Contrast 2) or cisgender women (Contrast 3) held even when accounting for age, race/ethnicity, sexual orientation, and differences between male cross-dressers and transfeminine participants (Contrast 1).
Testing overall differences between groups on a composite variable
To test whether there was an overall difference in mental health, relationships, and gender dysphoria between male cross-dressers and transfeminine participants and between both groups and cisgender men and women, we first standardized scores on all measures in this study among all participants regardless of sample. Thus, scores on each measure were converted from their original metric to z scores using the entire sample. For this standardizing procedure, all measures were scored in the same direction such that higher scores corresponded with more issues in mental health, relationships, and gender dysphoria. We then created a composite variable representing the mean of all standardized scores (z scores) for which a participant had data not missing or excluded.
With the same three between-groups contrasts, we used independent samples Welch’s t tests to examine differences on this composite variable comparing male cross-dressers with transfeminine participants (Contrast 1) and both groups with cisgender men and women (Contrasts 2 and 3). All three tests used the unpooled error variance, and the test of Contrast 1 was two-tailed because we did not have a prediction about whether male cross-dressers or transfeminine participants would score higher on the composite variable. The tests of Contrasts 2 and 3 were one-tailed in the direction of the male cross-dressers and transfeminine participants because we predicted that they would score higher than either of the cisgender samples. Although these tests were exploratory, a version of these analyses was included in our preregistration that involved standardizing scores on all measures from this study and those from studies that we will report in the future because they have a different focus.
Figure 2 shows the mean and 95% CI for each group on the composite variable as a violin plot. Transfeminine participants (M = 0.40, SD = 0.34) scored significantly higher than male cross-dressers (M = −0.01, SD = 0.28) on the composite variable, t(513.93) = 17.66, p < .0001, d = 1.33, 95% CI = [1.17, 1.49]. Furthermore, as predicted, both male cross-dressers and transfeminine participants (M = 0.14, SD = 0.36) scored significantly higher than either the cisgender men (M = −0.20, SD = 0.25) or cisgender women (M = −0.18, SD = 0.24) on the composite variable, t(754.52) = 17.28, p < .0001, d = 1.07, 95% CI = [0.94, 1.20], and t(821.85) = 17.08, p < .0001, d = 1.04, 95% CI = [0.91, 1.16], respectively.

Violin plot of means and 95% confidence intervals for male cross-dressers, transfeminine individuals, cisgender men, and cisgender women on the composite variable. Center horizontal lines represent means. Upper and lower lines represent 95% confidence intervals. Points represent individual participants. Units are means of standardized scores on all measures (i.e., scores on the composite variable).
Finally, we tested the robustness of our findings comparing groups on the composite variable by using multiple regression analyses (see Tables S1–S3 in the Supplemental Material). The same predictors, dummy coding, and contrast codes from previous multiple regression analyses were used. After controlling for age, race/ethnicity, and sexual orientation, transfeminine participants still scored significantly higher than male cross-dressers on the composite variable, p < .0001, d = 1.27, 95% CI = [1.11, 1.43]. After controlling for these same demographics and differences between male cross-dressers and transfeminine participants, both groups also still scored significantly higher than either cisgender men, p < .0001, d = 1.24, 95% CI = [1.08, 1.40], or cisgender women, p < .0001, d = 1.19, 95% CI = [1.05, 1.34].
Testing the construct validity of mental-health measures
We employed a construct-validation framework to address the potential overlap between some of our mental-health measures, examining whether they could be distilled into a smaller number of latent constructs. Because this approach followed our preregistered analyses that compared groups on each individual measure of mental health, tests of construct validity were exploratory. More comprehensive analyses testing construct validity, such as factor analysis (Cronbach & Meehl, 1955), are beyond the scope of the present study. For our purposes, we determined whether some of our mental-health measures were indicators of a broader mental-health construct by looking for patterns in their effect sizes that were shared across differences on the individual measures, examining their correlational structure, and considering how much they are conceptually similar.
As shown in Tables 2 to 4, several mental-health measures shared effect sizes that were similar in magnitude and direction across our comparisons of male cross-dressers with transfeminine participants (Contrast 1) and both groups with cisgender men and women (Contrasts 2 and 3). First, differences on the Satisfaction With Life Scale (Diener et al., 1985) and the Rosenberg Self-Esteem Scale (Rosenberg, 1965) were comparably strong and negative across the three between-groups contrasts, and the two measures were strongly correlated in the full sample, p < .0001, r = .66, 95% CI = [.62, .68]. Because both measures seem to capture how well participants think of themselves, we conceptualized them as reflecting a broader construct of subjective well-being. The Depression, Anxiety, and Stress Scale–21 (Lovibond & Lovibond, 1995) and the first two items of the Suicidal Behaviors Questionnaire–Revised (Osman et al., 2001) were comparably strong and positive in their differences across the three between-groups contrasts, and they were strongly correlated in the full sample, p < .0001, r = .53, 95% CI = [.49, .57]. Considering that both measures assess internalizing symptoms of mental health, we conceptualized them as reflecting a broader construct of psychological distress. Although the Alcohol Use Disorders Identification Test–Consumption (Bush et al., 1998) and the Drug Abuse Screening Test (Skinner, 1982) did not show consistent patterns in their effect sizes across the three between-groups contrasts, they were moderately correlated, p < .0001, r = .31, 95% CI = [.26, .36], and share conceptual similarity in measuring externalizing symptoms of mental health, specifically those involving either alcohol or other drugs. As a result, we conceptualized these two measures as reflecting a broader construct of substance abuse.
Finally, the Short Autism Spectrum Quotient (Allison et al., 2012) and the first question from the Health-Related Quality of Life Scale (Centers for Disease Control and Prevention, 2000) did not clearly fit as indicators of a fourth construct or one of the other three constructs. They shared no obvious patterns with other mental-health measures in their effect sizes across the three between-groups contrasts, and they were not strongly correlated with or conceptually similar to any other measure. These two measures instead formed their own unique mental-health constructs of autistic traits and general health, respectively. Even though our approach to construct validation is partly based on empirical findings (e.g., patterns in effect sizes, correlations between measures), it is still highly subjective. We emphasize that its main purpose is to improve the cohesion and clarity of our findings. For correlations among all eight of our mental-health measures in the full sample, see Table S4 in the Supplemental Material.
Discussion
In the present study, we examined the extent to which male cross-dressers differed from transfeminine individuals and both groups differed from cisgender men and women in their mental health, relationships, and gender dysphoria. Previous studies focused on male cross-dressers and transfeminine individuals have relied on small sample sizes (e.g., Fagan et al., 1988) or failed to clearly distinguish between these two groups (e.g., Bockting et al., 2013). Recognizing these limitations, in the present study, we used data from large samples of male cross-dressers and transfeminine individuals recruited through many online communities diverse in gender and sexuality. Furthermore, we determined specific criteria in advance for categorizing participants as either male cross-dressers or transfeminine individuals.
Despite a few points of overlap in autistic traits, drug use or dependence, general health, and perceived social support, male cross-dressers and transfeminine individuals largely differed in their mental health, relationships, and especially gender dysphoria. As we predicted based on the little prior research comparing these two groups (Beatrice, 1985; Brown et al., 1996; Docter & Fleming, 2001; Zucker et al., 2012), transfeminine individuals were more likely to experience mental-health challenges and gender dysphoria than male cross-dressers, and this general finding held even when accounting for age, race/ethnicity, and sexual orientation. Effect sizes before and after controlling for demographic differences were very large for measures of gender dysphoria and small or moderate for other measures that differed between the two groups. Based on a post hoc sensitivity analysis, these effect sizes also passed the statistical threshold for what our study could reliably detect (i.e., the minimum detectable effect size). Previous research and theory have argued for these same differences, making it clear that they are important for understanding those needs specific to male cross-dressers versus transfeminine individuals in clinical settings. There were three exceptions to this pattern of results: On average, transfeminine individuals reported more relationship satisfaction, and male cross-dressers reported more alcohol use and potentially problematic drinking and more drug abuse after controlling for demographic differences. Using a construct-validation framework, broader constructs of subjective well-being, psychological distress, and substance abuse emerged as potential latent factors differentiating these two groups.
Male cross-dressers have been shown to experience shame and secrecy related to wearing women’s clothing or behaving femininely (Docter & Prince, 1997), which might explain their lower ratings of relationship satisfaction on average. In addition, previous research has indicated that transfeminine individuals tend to report more mental-health concerns (Beatrice, 1985; Brown et al., 1996; Zucker et al., 2012), but studies have not looked specifically at alcohol or substance use. It is possible that mental-health differences between male cross-dressers and transfeminine individuals follow a similar pattern as mental-health differences between cisgender men and women, especially when focused on our broader constructs of substance abuse and psychological distress. Much of this previous work has suggested that cisgender men tend to experience externalizing problems, such as substance abuse, and cisgender women tend to experience internalizing problems, such as psychological distress, from depression and anxiety (Eaton et al., 2012; Hartung & Lefler, 2019; Kramer et al., 2008). This pattern is consistent with our findings comparing male cross-dressers and transfeminine individuals, who identified as men and women or trans women in this study, respectively.
In contrast to this pattern, autistic traits did not differ on average between male cross-dressers and transfeminine individuals even though they tend to be higher in cisgender men than cisgender women (Baron-Cohen et al., 2001; Ruzich et al., 2015). Several studies, however, have found that transfeminine individuals do not tend to have higher or lower levels of autistic traits relative to cisgender men (Jones et al., 2012; Kung, 2020; Nobili et al., 2018; Pasterski et al., 2014; Stagg & Vincent, 2019). Because autistic traits typically emerge early in life and are thought to be the result of atypical neurodevelopment that occurs prenatally, this lack of difference between male cross-dressers and transfeminine individuals might reflect that both were assigned male at birth. Unlike subjective well-being and psychological distress, autistic traits may also be less influenced by gender-minority stress, which refers to the external and internal stressors specific to navigating the world as a trans or gender-diverse individual (Hendricks & Testa, 2012; Testa et al., 2015). Future research is necessary to further explore similarities and differences between male cross-dressers and transfeminine individuals, which can help the field understand why there are disparities in some areas of mental health, relationships, and gender dysphoria but not others. For example, it is unclear whether and to what extent more psychological distress in transfeminine individuals relative to male cross-dressers is due to differential experiences of gender role or gender-minority stress. Finally, results comparing male cross-dressers and transfeminine individuals suggest that future research would benefit from clearly distinguishing the two groups.
With only a few exceptions, male cross-dressers and transfeminine individuals were different from samples of cisgender men and women in mental health, relationships, and gender dysphoria. Consistent with our predictions based on previous findings (e.g., Bockting et al., 2013; Melendez et al., 2006), male cross-dressers and transfeminine individuals in the present study reported more negative mental health across all of our broader constructs, more negative relationships, and more gender dysphoria than either cisgender men or women. Even when accounting for age, race/ethnicity, sexual orientation, and differences between male cross-dressers and transfeminine individuals, the overall pattern of findings comparing those two groups with the cisgender samples remained the same. Effect sizes before and after controlling for demographic differences were very large for measures of gender dysphoria and small or moderate for most other measures. Nearly all effect sizes comparing male cross-dressers and transfeminine individuals with cisgender men or women were larger than the minimum detectable effect sizes. This overall pattern converges with both previous work and many of the differences we found between male cross-dressers and transfeminine individuals, suggesting that many mental-health concerns are shared but still more strongly experienced by one group.
Limitations and future directions
Findings should be cautiously interpreted because of several important limitations. First, most participants across the different samples reported that they were White/Caucasian and living in the United States or Western Europe. Although our samples might have better captured the diversity of gender and sexual orientation in male cross-dresser and transfeminine communities relative to previous studies, they do not allow for much generalizability of findings beyond a White and Western framework. Future research on male cross-dressers and transfeminine individuals would benefit from samples with more racial/ethnic diversity and that recruit outside of Western or industrialized nations. Although it is impossible to obtain a truly representative sample of either male cross-dressers or transfeminine individuals, some promising approaches to improve racial/ethnic diversity are more targeted recruitment strategies and partnerships with local organizations and health-care clinics. By collaborating with community-based organizations and health-care clinics for trans individuals, two recent studies recruited samples of transfeminine individuals in the United States with more racial/ethnic diversity than samples from previous studies (Valente et al., 2020; Wirtz et al., 2019).
Second, we prioritized maximizing sample sizes of male cross-dressers and transfeminine individuals by recruiting online from a wide range of Facebook groups, Reddit communities, Discord servers, and other websites or forums where they can be found and where we also had access and approval to post advertisements. Because of the expected challenges of reaching these populations with more traditional recruitment methods, we targeted online interest groups catering to male cross-dressers and transfeminine individuals, which may have introduced sampling biases. Differences between these two groups and cisgender samples might therefore reflect differences between the kinds of people who frequent online communities like those on Reddit and the kinds of people who complete studies on Prolific. For example, people who frequent online communities might be more digitally literate or willing to discuss sensitive topics, such as mental health, relationships, and gender dysphoria. Future research would benefit from using the same recruitment strategy for all comparison groups.
Third, the criteria used to categorize participants as male cross-dressers or transfeminine relied only on self-reported gender identity and frequency of how often they dressed in women’s clothing in the past 12 months. Although this categorization produced meaningful differences between the two groups, it does not account for gradations in presentation or experience among either male cross-dressers or transfeminine individuals (Jacobson & Joel, 2019; Kuper et al., 2012). For example, male cross-dressers who wear women’s clothing more frequently or transfeminine individuals who have taken more steps toward medical or social transition may not show the same patterns in mental health, relationships, and gender dysphoria as male cross-dressers or transfeminine individuals do as a whole. More sophisticated comparisons of male cross-dressers and transfeminine individuals that incorporate their full range of presentation and experience would provide further insight into the specific challenges and needs of subgroups in these communities. Using multiple self-report measures to categorize participants as male cross-dressers or transfeminine or finding alternatives to self-report might also ensure the precision and validity of group comparisons.
Finally, we examined only a subset of constructs related to mental health, relationships, and gender dysphoria because of concerns about the overall length of the online survey. It would be useful for future studies to not only attempt to replicate our findings by assessing the same constructs with different measures but also extend them by examining constructs that we did not include, such as body image, borderline personality, and adverse childhood experiences. Future studies could also investigate the relationships between gender-minority stress or other negative experiences and mental health, relationships, and gender dysphoria, which would build out the nomological networks in which these constructs are functioning. Although we included some preliminary tests of construct validity, which found evidence for several broader constructs of mental health reflected in the measures that we used (e.g., subjective well-being), more comprehensive testing is necessary.
Conclusions
In the present study, we identified both overlapping and distinct areas of need in mental health, relationships, and gender dysphoria for male cross-dressers and transfeminine individuals. Although transfeminine individuals are more vulnerable than male cross-dressers to mental-health challenges and especially gender dysphoria, both groups appear to carry increased risk for a broad range of issues, including psychological distress, autistic traits, substance abuse, relationship dissatisfaction, and less perceived social support, relative to the general population. Both groups especially tended to report stronger feelings of gender dysphoria and were more likely to have ever experienced gender dysphoria, had gender-affirming medical interventions, or taken steps toward social transition compared with cisgender men and women.
Although recent studies have established elevated rates of mental-health and related concerns in transfeminine individuals specifically (Downing & Przedworski, 2018; Newcomb et al., 2020; Nuttbrock et al., 2013; Toomey et al., 2018; Warren et al., 2016) or in samples of transfeminine individuals that also included some male cross-dressers (Bockting et al., 2013; Melendez et al., 2006), this is the first study in more than a decade to show that male cross-dressers experience similar challenges, if not less strongly. Such findings may help inform those involved in the mental-health care of male cross-dressers, a population whose struggles have largely been ignored despite one study showing they may be more prevalent than transfeminine individuals (Långström & Zucker, 2005).
Furthermore, effect sizes were comparable between male cross-dressers and transfeminine participants and between both groups and either cisgender men or women (see Tables 2–4 and Fig. 1). Results comparing groups on the composite variable also indicate that overall differences in mental health, relationships, and gender dysphoria between male cross-dressers and transfeminine participants were about equal to those between the two groups and cisgender men or women (see Fig. 2). Future studies might investigate the possibility that male cross-dressers and transfeminine individuals reflect two different groups that share the same underlying dimension, with transfeminine individuals representing further movement or progression along this dimension (e.g., Blanchard et al., 1987; Docter & Fleming, 2001; Lawrence, 2009). This idea is consistent with evidence that some male cross-dressers transition to living as transfeminine individuals.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026261442427 – Supplemental material for Mental Health, Relationships, and Gender Dysphoria in Male Cross-Dressers and Transfeminine Individuals From an Online Community Sample
Supplemental material, sj-docx-1-cpx-10.1177_21677026261442427 for Mental Health, Relationships, and Gender Dysphoria in Male Cross-Dressers and Transfeminine Individuals From an Online Community Sample by Kevin J. Hsu, James S. Morandini and S. Rudd in Clinical Psychological Science
Footnotes
Acknowledgements
We thank Phil Illy, Sean Doster, Anna Fields, Kayla Waring, Naomi Salama, and other members of male cross-dresser, transfeminine, and related communities who provided helpful feedback on survey design and recruitment. We also thank those community members who took the time and effort to participate in this research.
Transparency
Action Editor: Jennifer L. Tackett
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.