
Abstract
Social comparison can fundamentally shape health perceptions. Building on existing literature, we first introduce a process model of health-related social comparison that consists of (a) seeking or encountering self-relevant social information, (b) evaluating self-attributes relative to social standards and generating a posterior target construal, (c) valuation of the comparison outcome based on personal motives and coping, and (d) affective, cognitive, and behavior responses. Second, we conducted a systematic review and meta-analysis to summarize existing knowledge about social comparison in populations with mental disorders. We systematically searched Medline, PsycInfo, and Web of Science. The included 72 studies suggest a strong correlation between social comparison and mental health. However, there is lack of research addressing the appraisal of the comparison outcomes and the reciprocal, longitudinal relationship between social comparison and health. Last, based on our model and meta-analytical results, we offer recommendations to inform future investigations of social comparison in mental health.
Theoretical accounts and empirical data suggest that self-evaluations of mental and physical attributes, including mental health, are predicated on relative, ordinal comparisons rather than absolute values (Morina, 2021; Vlaev et al., 2011). Furthermore, ordinal comparisons of any self-attribute (e.g., appearance or intelligence), possession, or social status may affect well-being. Social comparison, a process by which individuals evaluate their attributes in relation to other individuals (Festinger, 1954), is frequently used to judge personal attributes. It has been studied predominantly in social psychology, and evidence points to its ubiquity and impact on behavior (Gerber et al., 2018).
A number of reviews have assessed research on social comparison in relation to mental health. Myers and Crowther (2009) reported that an increased tendency to engage in upward appearance-based comparisons is positively related to body dissatisfaction. Wetherall et al. (2019) found that individuals with depressive symptoms are more likely to judge themselves negatively relative to others. McCarthy and Morina (2020) concluded that social-rank evaluation is positively associated with depression and anxiety. Finally, Hoppen et al. (2020) reported that posttraumatic-stress-disorder (PTSD) symptoms are negatively associated with social-rank evaluation. Although existing reviews clearly indicate that social comparison plays a significant role in mental health, they also highlight a lack of research on the role of social comparison in psychopathology. McCarthy and Morina (2020) and Hoppen et al. (2020) identified only 14 and two cross-sectional correlational and experimental studies, respectively, with patients meeting diagnostic criteria for depression, anxiety disorders, or PTSD. Given the complex nature of the social-comparison process and considering that existing reviews are outdated (Myers & Crowther, 2009), restricted to a narrow range of conditions (Hoppen et al., 2020; McCarthy & Morina, 2020; Myers & Crowther, 2009; Wetherall et al., 2019), or address only one of the many relevant aspects of social comparison (social ranking; Wetherall et al., 2019), a comprehensive and up-to-date systematic review of the role of social comparison in health is warranted. To better identify gaps for further research, such a review should be appraised against a theoretical model specifically developed to guide understanding of social comparison in mental health.
With these considerations in mind, we pursued three aims. First, we sought to outline a theoretical model of social comparison in relation to mental health, drawing on current literature on social and other forms of comparison while integrating important aspects of well-being/ill-being. Second, guided by this model, we conducted a systematic review and meta-analysis to summarize and appraise the existing knowledge about comparison in individuals with mental disorders. Third, based on our model and meta-analytical results, we formulated recommendations for future research on social comparison and health. These three objectives reflect the structure of this work. In doing so, we adopt a continuum-based perspective on well-being. Although our primary focus is on mental-health outcomes, the proposed framework is intended to apply more broadly to health perceptions along a continuum of well-being. From this perspective, mental disorders represent more severe expressions of diminished well-being along a continuous dimension.
The Social-Comparison Process
Festinger (1954) introduced social-comparison theory by postulating a human drive to gain accurate self-evaluations. At present, social comparison is viewed as a fundamental factor influencing overall psychological functioning (Suls et al., 2020; Unkelbach et al., 2023). It is a complex and dynamic process that can vary by several characteristics; the main ones are described in Table 1. To illustrate, consider the following example with John, who suffers from body dysmorphic disorder: Upon entering a social gathering, John notices two of his male colleagues and compares their physical appearance to his own, concluding that they look much more attractive than he does. He experiences a range of emotions, thinks that he might not belong here, and decides to not engage in a conversation with these classmates. Later at home, he dwells on what they might think of him and that he should avoid such social events altogether.
Key Features of Social Comparison
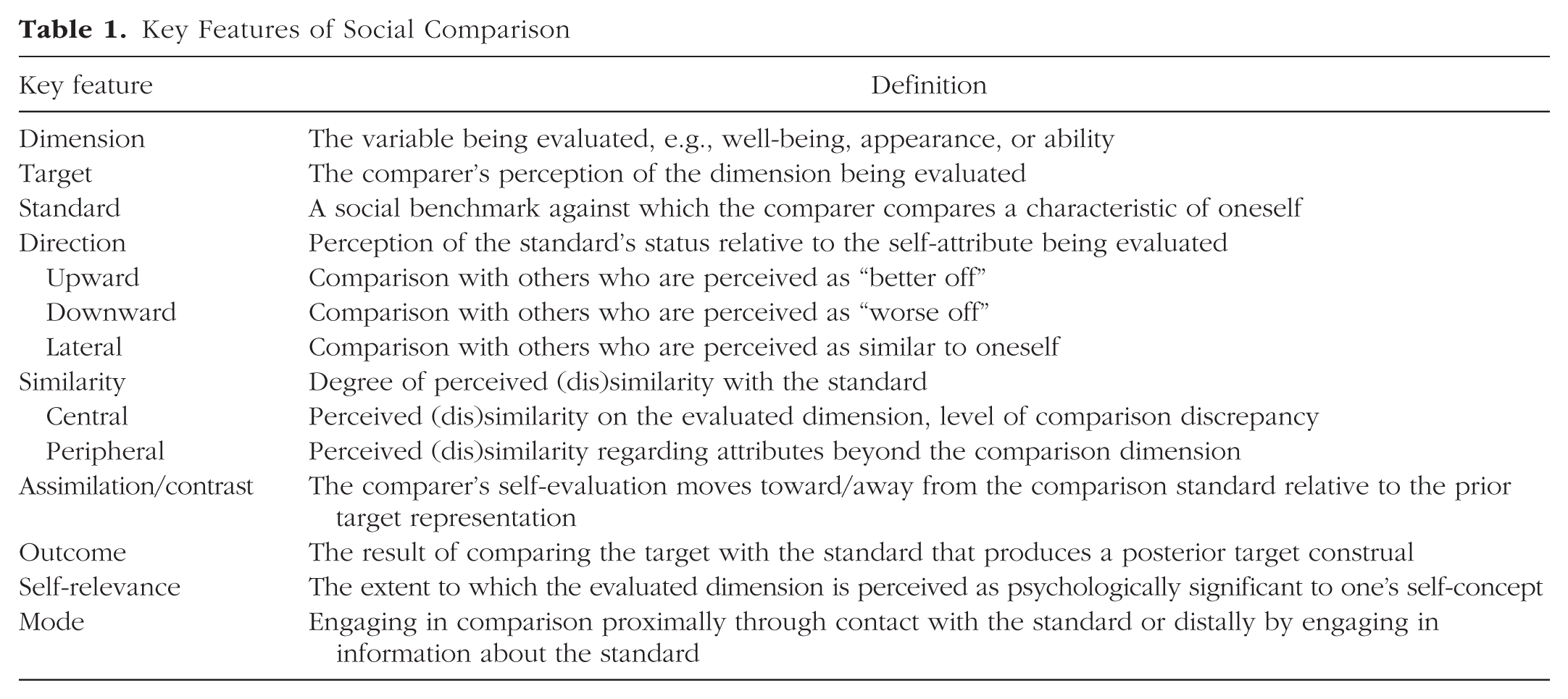
The “dimension” here is physical appearance, the “target” is John’s own appearance, and the “standard” is his two colleagues. Furthermore, the “direction” represents an upward comparison because John perceives them as better looking. Appearance signifies here the notion of “central (dis)similarity” (i.e., target – standard discrepancy on the evaluated dimension). Relatedly, the perceived “peripheral similarity” to the standard is high here because the two standards are John’s male colleagues. The conclusion that the classmates are much more attractive represents the “comparison outcome.” Furthermore, the engendered emotions, cognitions, and avoidance of interaction with the classmates represent the engendered “reactions.” These reactions are driven by the fact that appearance is highly “relevant” to John’s self-concept. Finally, the ruminative behavior later at home and his intention to avoid future social gatherings represent long-term consequences.
Reflecting on previous work on social comparison (e.g., Wood, 1996) and comparative thinking in general (Morina, 2021), we define comparison as a process consisting of (a) seeking or encountering social information, (b) the basic comparison process of evaluating (dis)similarities between the target and the standard, (c) the valuation of the comparison outcome in terms of one’s own motives and coping, and (d) the engendered affective, cognitive, or behavioral responses (see Fig. 1).

The process model of social comparison and its interaction with health, dispositions, and agency. Adopted from Morina (2021). For an explanation of the key terms of the social-comparison process, see Table 1.
Seeking or encountering social information
The comparison process can be initiated by either external or internal stimuli and can arise either spontaneously or deliberately (Wood, 1996). Social comparison is driven by key self-motives, such as self-assessment, self-improvement, self-enhancement, and self-verification (Sedikides & Strube, 1997). Social comparison is further likely to be driven by the perception of the current health status and personal dispositions and personal agency (Schlechter et al., submitted). Personal dispositions are defined as enduring characteristics that are peculiar to an individual (Allport, 1966). Personal agency, on the other hand, is defined as the ability to exercise control over personally relevant events (Smith et al., 2000) and refers to key personal attributes, socio-structural influences, and contextual affordances (Bandura, 2018).
The basic comparison process
This component involves the actual comparative assessment of the similarities and/or differences between the target and the standard along one or more dimensions. Consequently, it comprises three variables: (a) the comparer’s prior mental representation of the target dimension, (b) the mental representation of the standard, and (c) the integration of the first and second components, which yields the comparison outcome, representing the posterior target construal of the comparer. The distinction between prior and posterior target construal becomes crucial when measuring the extent to which a specific comparison leads to assimilation, contrast, or no shift. This phenomenon is highly relevant to health because judgments of health (i.e., how one is doing) or health-related behavior (e.g., how well one is coping with an illness) are shaped by social comparison (Morina et al., 2022). Assimilation to upward social standards translates into a better perception of one’s own well-being or health-related behavior. Some scholars have applied overly broad definitions of assimilation and contrast by inferring them from elicited reactions rather than changes in self-evaluation. In addition, some researchers have not distinguished between reflection (basking in reflected glory) and assimilation (Collins, 1996; Wheeler & Suls, 2007). In line with Wheeler and Suls (2007), we define, respectively, upward assimilation and downward contrast as an increase in the comparer’s self-evaluation on the evaluated dimension as a result of comparing with an upward standard (upward assimilation) or a downward standard (downward contrast). Likewise, upward contrast and downward assimilation can be defined, respectively, as a decrease in the comparer’s self-evaluation on the evaluated dimension as a result of comparing with an upward standard (upward contrast) or a downward standard (downward assimilation). The argument is that potential assimilation or contrast with respect to self-evaluation can be assessed only when both prior and posterior target presentations are known (see Fig. 2). Note that upward assimilation and downward contrast on the one hand and downward assimilation and upward contrast on the other hand represent appetitive (i.e., satisfying specific needs) and aversive (i.e., frustrating specific needs) shifts, respectively.

Potential social comparison (SC) outcomes relative to the prior target representation.
The valuation of the comparison outcome
When making comparisons, individuals inevitably reflect on the meaning of the comparison outcome, which in turn shapes how they respond to it. In accordance with appraisal models (Ellsworth, 2013), the valuation process involves assessing how the comparison outcome relates to motives, including basic needs, values, and goals (Dweck, 2017), and to controllability and coping capability. In appraisal theories, emotion is understood as a multicomponential phenomenon generated by the cognitive appraisal of a situation’s motivational meaning (Lazarus & Folkman, 1984; Scherer & Moors, 2019). Accordingly, emotional responses emerge from an individual’s evaluative processes that assess the relevance and implications of a given situation for personal needs and goals. These appraisals organize and shape emotional responses across behavioral components (Ellsworth, 2024; Scherer & Moors, 2019). Drawing on this, we note that the general comparative model (gComp) of self-perception (Morina, 2021) suggests that valuing the comparison outcome’s motivational meaning and coping potential yields four outcomes (see Fig. 1). Overall, the motivational significance of the comparison outcome may align with the comparer’s motives, challenge them, prove irrelevant, or pose a threat to them. Comparison outcomes processed as relevant to the comparer’s motives will elicit notable responses. Alignment of the comparison outcome with personal motives will lead to confidence that the desired end state has been or will be achieved in the future. Alternatively, the comparison outcome may challenge personal motives but still result in optimism that the desired end state will be achieved in the future. Finally, the comparison outcome may pose a threat to personal motives and result in pessimism that the desired end state can be achieved.
Affective, cognitive, and behavioral responses
The valuation of relevant comparison outcomes shapes affective reactions. Comparison outcomes that align with motives and instill confidence that the desired end state will be achieved will produce positive emotions. Furthermore, if comparison outcomes challenge motives yet lead to optimism that the comparer has the necessary means to achieve the desired end state, high-intensity positive emotions, such as excitement, will emerge. Alternatively, comparison outcomes that threaten motives and lack optimism about achieving (or avoiding) the desired (or undesired) end state will trigger negative emotions. Depending on the comparison outcome’s motivational meaning and in line with appraisal theories (Ellsworth, 2024; Scherer & Moors, 2019), different affective reactions may follow, including but not limited to fear (if threat or harm is perceived), sadness (if resignation is perceived), and anger (if a major interference with the desired end state is perceived).
Affective responses are accompanied by cognitive orientation, which may affect long-term behavioral responses (Morina, 2021). Goal-directed behavior will be facilitated when the comparer focuses on how to achieve the desired end state. Happiness or enjoyable emotions are likely to be processed as self-affirmation, indicating that no significant behavioral changes are required and hence, current behavior can be maintained. Excitement signals achievability, and individuals’ cognitive orientation drives them to make extra efforts toward achieving it, ultimately leading to behavioral assimilation. Finally, irrelevant comparisons produce low emotional responses, require minimal cognitive resources, and lead to behavioral quiescence.
Relevant comparisons that evoke strong negative emotions (e.g., fear) may be appraised as overly threatening to personal motives, prompting a shift in cognitive orientation toward distracting and away from pursuing the desired end state. Yet intense negative affect following a mismatch between a person’s motives and the person’s coping abilities can also lead to reconstrual or rededication (Morina, 2021). Reconstrual comprises a reappraisal of the target construal. For example, in a group-therapy setting, patients with depression may perceive another group members as more engaged and then engage in reconstrual by reasoning that the other person likely faces fewer external stressors. Rededication entails the reappraisal of the motivational significance. For example, the same patients from above might conclude that engagement in treatment is not that important to them.
Another function of cognitive orientation relates to determining whether further target evaluation is needed. If the comparer’s needs are met or if the comparison outcome is processed as too much of a threat to the comparer’s motives, the comparer will move on to new activities. Conversely, if needs are not met, further comparative evaluations may be instigated. In this regard, gComp (Morina, 2021) differentiates between primary, secondary, and tertiary evaluations. When dissatisfaction with the primary comparison outcome is present but affective responses remain bearable, the individual may continue comparing on the same dimension with the same or different standards, a process termed “secondary evaluation.” Tertiary evaluations are used to modify the affective and cognitive consequences of the outcome of primary or secondary evaluations. For instance, after comparing with patients with the same disease, patients may have a very negative evaluation of their own coping, which may conflict with their self-concept and lead to negative affect. To resolve this cognitive dissonance and negative affect, comparers may engage in tertiary evaluations that might involve comparing on a dimension in which they excel, such as playing a musical instrument.
Long-term consequences first relate to whether social comparison influences behavior toward (or away from) the desired (or undesired) end goal (see Fig. 1). Comparing to a standard representing a desired and attainable end state is likely to promote behaviors directed toward that goal, reflecting behavioral assimilation. However, if the standard represents an unattainable end state, comparers are unlikely to modify their behavior and may even exhibit behavioral quiescence. Second, each comparison has the potential to have an impact on future comparative behavior. If the act of comparison leads to strong negative emotional reactions when faced with an unattainable appetitive end state or unavoidable negative end state, the comparer may be inclined to avoid future comparisons altogether. Finally, each comparison has the potential to have an impact on target representation. For example, repeated exposure to fellow patients perceived as coping better with the disease in question will lead to an enduring negative evaluation of one’s own coping.
A Social-Comparison Perspective on Health
The process model of social comparison provides a useful framework for examining the bidirectional links between social comparison and health. Accordingly, we propose distinguishing between (a) social comparison directly related to health, (b) social comparison concerning other dimensions that indirectly affect health, and (c) health and individual characteristics that shape the process of comparative behavior (see Fig. 3).
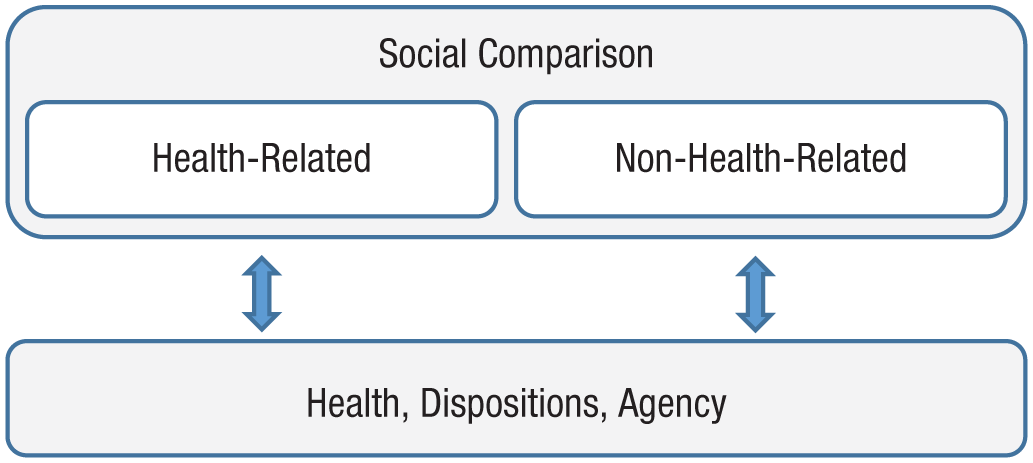
Interdependency between social comparison, health, dispositions, and agency. The figure indicates that health, dispositions, and agency shape individuals’ engagement in social comparisons not only in health-related contexts but also across non-health-related domains.
Health-related social comparison
Two relevant types of social-comparison dimension relate to the evaluation of health and health behaviors. The first type comprises attributes of health, in which comparers evaluate their well-being relative to others. The comparison dimension may consist here of mental well-being in general or some specific aspect of well-being, for example, fatigue for a patient with depression. In line with frame-of-reference theories that posit that all self-judgments are formed in relation to some reference frame (Vlaev et al., 2011), some research suggests that individuals evaluate their well-being partly in relation to the well-being of others (Filus et al., 2020; Melrose et al., 2013; Morina et al., 2022). The second type of dimension relates to health-relevant personal dispositions, agency, risk perception, and illness-coping behavior. For example, patients with depression may compare their coping with the disorder relative to other patients who are coping well. Whether such comparison will positively influence coping behavior will depend on perceived controllability and self-efficacy (Bandura, 2018; Morina, 2021). Such influence is likely when comparers perceive the desired coping behavior as attainable and believe they possess the capacity to execute that behavior. Importantly, perceived controllability and self-efficacy are also informed by social comparison, and research indicates that the role of social comparison in illness-coping behavior is mediated by self-efficacy (Schokker et al., 2010). Social comparison of health-relevant attributes further relates to lifestyle factors that drive health outcomes in general. For example, research has shown that improvements in behavioral risk or protection factors, such as alcohol consumption, smoking, diet, or physical activity, play a major role in health outcomes (Zhang et al., 2021). Lifestyle behaviors are shaped in social contexts, and social influences, including social comparison, play a major role in lifestyle behavior and coping with chronic illness (Klein & Rice, 2020).
Non-health-related social comparison
Social comparison of non-health-related dimensions may also have a significant impact on health. For example, perceptions of having a low social status are based on social comparison, and research indicates that subjective social status is associated with mental health and health-related behavior (Zell et al., 2018). Furthermore, some patients are inclined to engage more frequently in social comparison overall than other patients, as proposed by the social-comparison-orientation model and supported by empirical data (Buunk & Gibbons, 2007). Focusing specifically on non-health-related social comparison can provide valuable insights into how such processes affect health or health behaviors.
Health-related and other individual characteristics affecting social comparison
Finally, the presence of health complaints and the need and means to overcome, manage, or adjust to them influence social-comparison behavior. Specifically, they may influence the choice of comparison standard and dimension such that people with severe mental illness are more likely to engage in comparison with fellow patients (vs. healthy individuals) on health-related dimensions. In addition, comparison with fellow patients (vs. healthy individuals) is likely to have a stronger influence on the comparer. Research also suggests that health complaints are related to a higher frequency of overall social comparison (McCarthy & Morina, 2020). Furthermore, health-related aspects are likely to influence the valuation of the comparison outcome and the reactions generated. Overall, the influence of health perception and health-related behavior may be moderated by illness characteristics, such as type and duration of illness, and by dispositions and agency (Arigo et al., 2014). Finally, and as with any form of human behavior, the relationship between health and social comparison is influenced by contextual factors (Schwarz & Strack, 1999).
Altogether, a social-comparison perspective on health suggests that valuable insights will be gained by conceptualizing social comparison as a process comprising multiple components that interact with one another and with health behaviors. To provide a systematic overview of the current literature on the link between social comparison and mental health, we conducted a systematic review and meta-analysis of relevant studies on this link.
The Present Systematic Review and Meta-Analysis
We considered studies that examined social comparison in populations with mental disorders. The search, coding, analysis, and presentation of the findings were informed by the theoretical considerations presented above. In terms of the design of potentially relevant studies, the systematic search was greatly informed by Wood’s (1996) taxonomy of methods applied in comparison assessment that distinguishes among selection, reaction, and narration methods, which has been applied in related meta-analyses on social comparison (Arigo et al., 2014; Gerber et al., 2018). Accordingly, selection studies were required to have used (quasi)experimental designs to investigate conditions under which certain social standards (e.g., upward vs. downward) are selected for comparison. Reaction studies needed to have used (quasi)experimental designs to examine potential reactions that might follow social comparison. Finally, narration studies were defined as assessments of naturally occurring social comparison through forced-choice or open-ended items of a self-report or an interview. Although narration studies may focus on any aspect of the social-comparison process, including comparison selection and engendered reactions, they do so by narrative assessment, whereas selection and reaction studies apply (quasi)experimental designs to manipulate certain variables. We coded and investigated selection, reaction, and narration studies separately.
Importantly, we also aimed at reviewing the literature for research employing alternative methodologies to examine any aspect of the social-comparison process and its relation to mental health. In particular, we were interested in the frequency or tendency of spontaneous and instructed social comparison (upward, lateral, or downward), the level of discrepancy between the target and the standard, the degree of assimilation or contrast to upward or downward comparison standards, the valuation of the comparison outcome, and affective, cognitive, and behavioral reactions to social comparison (see Fig. 1).
Method
Our work was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). Articles were identified through systematic literature searches in PsycINFO, Medline, and Web of Science. We searched the databases from inception to January 2025 using various search terms for social comparison to identify all social-comparison-related research: “social compar*” OR “upward comparison*” OR “downward comparison*” OR “lateral comparison*”. Related published systematic reviews and meta-analyses were also systematically screened for relevant citations.
Eligibility criteria, selection procedure, and data collection
Inclusion criteria consisted of (a) reporting of primary data measuring social comparison as defined by Wood (1996), (b) reporting data from at least 10 participants overall or at least 10 per group when multiple groups were compared, and (c) at least 80% of the clinical sample was diagnosed with mental disorders based on the International Classification of Diseases (World Health Organization, 2019) or the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013) and assessed with either a validated structured clinical interview or a validated self-report with a cutoff for clinical diagnosis.
Search results were initially screened for abstracts and titles by two independent reviewers using Rayyan (Ouzzani et al., 2016). Selected publications were then reviewed for coding and qualitative synthesis by three independent reviewers (N. Morina, F. K. Lemmel, and T. H. Hoppen). Discrepancies between reviewers’ ratings were analyzed after each assessment step and subsequently discussed by at least two coauthors until consensus was achieved. When eligible studies reported insufficient information on relevant outcomes, the corresponding authors were contacted at least twice by email, and attempts were spaced at least 1 month apart. Using a data-extraction sheet developed for this meta-analysis, we coded study and sample characteristics and the data on the relationship between social comparison and health.
Statistical analysis
We conducted the random-effects analyses in RStudio (R Core Team, 2023) using the metafor package (Viechtbauer, 2010). To conduct a meta-analysis on a specific outcome, a minimum of four publications was required (Hoppen et al., 2024; Morina et al., 2016). Weighted average effect sizes for correlational results were calculated using Fisher’s z transformations and then back-transformed to r for interpretation. For the meta-analyses on comparison selection and frequencies/tendencies, we used the metaprop function in RStudio. To test the homogeneity of effect sizes, we calculated the Q and I2 statistics. We further performed outlier checks in which outliers were defined as observations being at least 3.3 SD above/below the pooled effect (Tabachnick et al., 2013). For moderator analyses, we followed Borenstein et al. (2011) for a ratio of at least 10 studies (or independent data points) for each moderator. The presence of publication bias was examined with Egger’s test, which assesses significant asymmetry in the funnel plot and is recommended when at least 10 studies (or independent data points) are included in the analysis (Sterne et al., 2011). We categorized the outcomes as either aversive (e.g., negative affect or symptom severity) or appetitive (e.g., positive affect or life satisfaction). When analyzing aversive and appetitive outcomes jointly, we reversed the direction of the effect sizes for appetitive outcomes to ensure that all effects point in the same direction for meaningful interpretation. We also conducted subanalyses for appetitive outcomes only and aversive outcomes only.
Quality assessment
We assessed the quality of the included studies using a scale reported in McCarthy and Morina (2020). The quality of selection, reaction, and narration studies was assessed separately because the study designs varied widely. Overall, the assessment focused on the extent to which social comparison was measured using a validated instrument or approach, whether the direction of social comparison was clear, and whether the outcome variable was assessed using a validated measure.
Transparency and openness
The review was preregistered with PROSPERO (ID: CRD42021252676). The data files used for all performed meta-analyses, the R analysis codes, and an overview of meta-analytic results per analysis category have been deposited and can be viewed at here: https://osf.io/kcvyz/?view_only=698c3939dfd349719374be6c5d890033. Note that the second inclusion criterion in the article (≥ 10 participants per group) was inadvertently omitted from the preregistration. We report all analyses conducted as part of this work either in this article or in the Supplemental Material available online.
Meta-Analytic Findings
The PRISMA diagram in Figure 4 illustrates the process of study synthesis. A total of 72 studies were eligible. Of these, 63 studies were included in the meta-analysis, and the remaining studies were summarized in narrative synthesis (see Tables S1–S4 in the Supplemental Material). For quality assessment per study, see Tables S1 through S4 in the Supplemental Material.
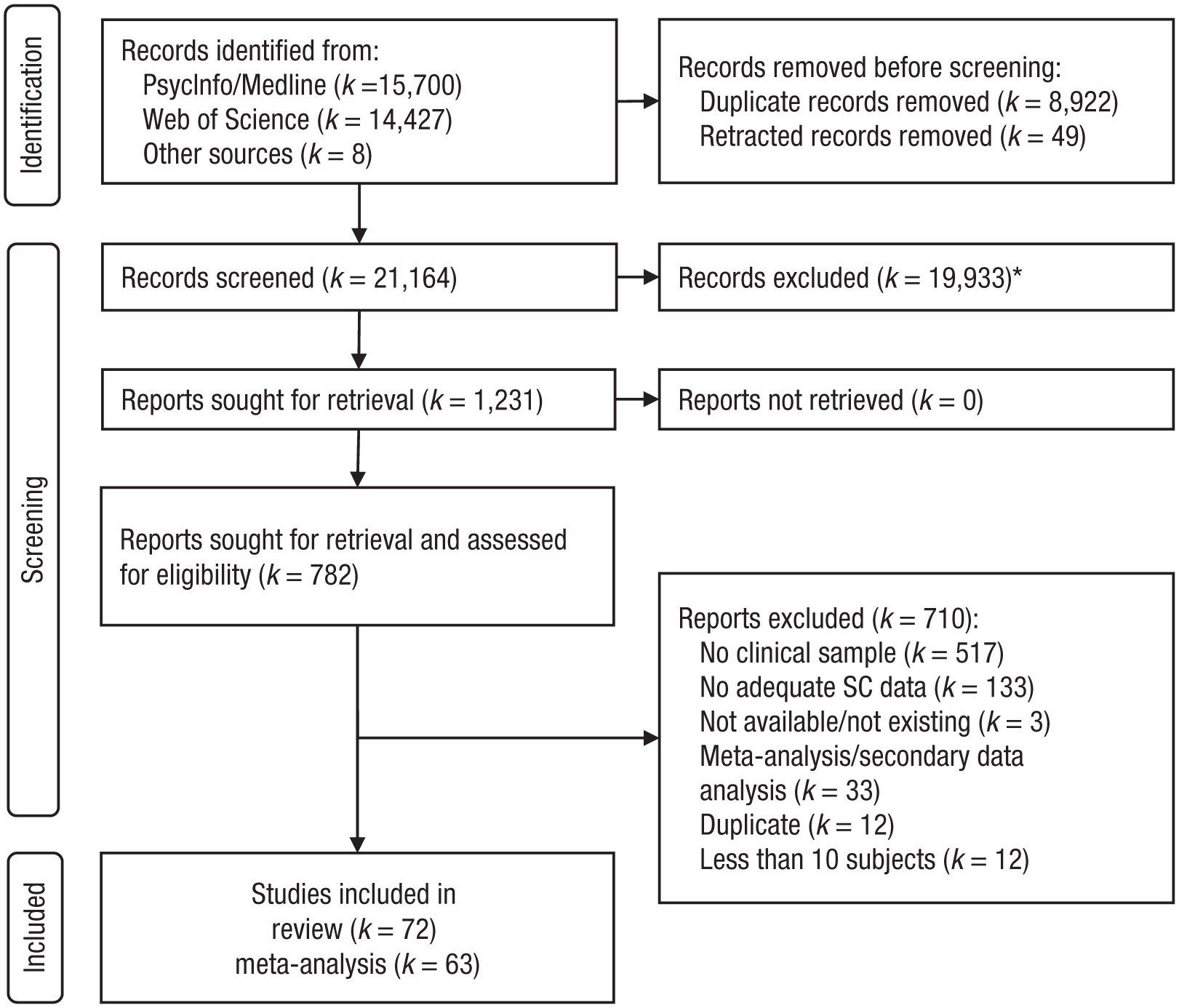
Flow chart depicting the study synthesis process. *Excluded at title/abstract screening: nonprimary social-comparison data (Wood, 1996), sample size < 10 overall or per group, < 80% clinical samples.
Experimental studies: selection studies
None of the included studies had investigated the conditions under which upward, lateral, or downward social standards are selected for comparison in individuals with mental disorders. In fact, all of the included experimental studies were identified as reaction studies.
Experimental studies: reaction studies
Ten studies examined the effect of experimentally induced social comparison in samples with a mental disorder relative to nonclinical samples, nine of which could be included in the meta-analysis. The overall quality of these studies was rated at 78%; all of the studies met at least 50% of the quality criteria. Clinical samples reported a significantly stronger effect of social comparison on envy (k = 2; Appel et al., 2015; Bauminger, 2004), attractiveness (k = 3; Blechert et al., 2009; Horndasch et al., 2015), negative affect (k = 3; Legenbauer, Rühl, & Vocks, 2008; Paz et al., 2024; Vocks et al., 2010), emotional arousal (Lin et al., 2023), and performance expectations (Liu et al., 2024) relative to nonclinical samples (overall Hedges’s g = 0.95, 95% confidence interval [CI] = [0.57, 1.33]; see Fig. S1 in the Supplemental Material). Note that Horndasch et al.’s (2015) study reported data on an adolescent and adult sample, which we treated as two separate samples. Large effect sizes resulting from subgroup analyses with studies assessing aversive outcomes only (three studies on negative affect, two on envy, and one on performance expectations) and studies assessing appetitive outcomes only (three studies on attractiveness, two on positive affect, and one on happiness) indicated that clinical samples showed stronger negative reactions or less strong positive responses to social comparison. In addition, a subgroup analysis with studies on eating disorders only (representing the largest clinical subgroup with k = 5) and including both aversive and appetitive outcomes also produced an effect size similar in size and direction (see Table S5 in the Supplemental Material). Finally, Sfärlea et al. (2023) reported that when female adolescents with anorexia nervosa are presented with photos of upward social comparisons, they focused longer on bodies than faces relative to individuals without anorexia nervosa.
Narration studies
A total of 65 studies reported on self-report data on social comparison in samples with mental disorders. Of these, 57 studies could be included in the meta-analytic review and were categorized into the four groups described below. The average quality rating of the narration studies was 70.2%; six studies had a quality rating below 50%.
Social-comparison tendency
A total of 17 studies examined social-comparison tendency in clinical versus nonclinical samples (Anson et al., 2015; Bardone-Cone et al., 2022; Blechert et al., 2009; Buunk & Brenninkmeijer, 2001; Fernández-Theoduloz et al., 2019; Fioravanti et al., 2024; Grynberg et al., 2020; Hamel et al., 2012; Horndasch et al., 2015; Jackson & Chen, 2007; Lavell et al., 2025; Legenbauer, Kleinstäuber, et al., 2008; Mölbert et al., 2017; Paz et al., 2024; Robinson et al., 2019; Schönhals et al., 2024; Turner et al., 2024). Again, the Horndasch et al. (2015) project provided separate data for adolescent and adult samples. The analyses revealed a significantly stronger social-comparison tendency in clinical groups relative to nonclinical groups (Hedges’s g = 0.98, 95% CI = [0.76, 1.21]; for related subanalyses, see Fig. S2 and Table S6 in the Supplemental Material).
Correlation between social-comparison tendency and health outcomes
A total of six studies assessed the correlation between social-comparison tendency and psychopathology (Anson et al., 2015; Grynberg et al., 2020; Hamel et al., 2012; Mölbert et al., 2017; Morrison et al., 2003; Schönhals et al., 2024). The analyses revealed a nonsignificant correlation between these two variables (r = .29, 95% CI = [.05, −.49]; see Fig. S3 and Table S7 in the Supplemental Material).
Social-rank evaluation
A total of 23 studies assessed how clinical and nonclinical samples evaluated their social rank relative to other individuals (Allison et al., 2013; Anson et al., 2015; Călin & Bică, 2024; Cardi et al., 2014; C. B. Carvalho et al., 2018; S. Carvalho et al., 2013; Collett et al., 2016; Cunha et al., 2008; De Paoli et al., 2017; Fatih et al., 2022; Ferreira et al., 2013; Giacolini et al., 2013; Gillard et al., 2021; Goodman et al., 2021; Kalaycı et al., 2019; Michail & Birchwood, 2013; Moscovitch et al., 2009; Pinto da Costa et al., 2024; Şahin et al., 2011, 2012; Troop & Hiskey, 2013; Weisman et al., 2011; Yokusoglu, 2024). All but three studies used the Social Comparison Scale (Allan & Gilbert, 1995) or a modified form thereof to assess how participants rate themselves in relation to others on 11 bipolar constructs (e.g., unlikeable to more likeable, incompetent to competent); lower sum scores indicate less favorable self-evaluation. Clinical samples reported a significantly lower self-evaluation relative to other people than nonclinical samples (Hedges’s g = −1.18, 95% CI = [−1.28, −0.88]; see Fig. S4 in the Supplemental Material). Large effects relative to nonclinical samples were also found when samples with anxiety disorders, depression, eating disorders, and psychotic disorders were each examined in isolation (see Table S8 in the Supplemental Material).
Correlation between social-rank evaluation and health outcomes
A total of 29 studies investigated associations between social-rank evaluation and levels of psychopathology (Allan & Gilbert, 1995; Allison et al., 2013; Călin & Bică, 2024; C. B. Carvalho et al., 2018; S. Carvalho et al., 2013; Collett et al., 2016; De Paoli et al., 2017; Duarte et al., 2016; Fatih et al., 2022; Giacolini et al., 2013; Gilbert, 2000; Gilbert & Allan, 1998; Gilbert et al., 1995, 2002, 2005, 2006, 2009, 2010; Grady et al., 2025; Judge et al., 2012; Kalaycı et al., 2019; McEwan et al., 2012; Rammou et al., 2022; Troop et al., 2003; Troop & Hiskey, 2013; Vázquez Morejón et al., 2022; Weisman et al., 2011; Yokusoglu, 2024; Zaffar & Arshad, 2020). All but one of the included studies used the original Social Comparison Scale (Allan & Gilbert, 1995) or a modified version thereof. The pooled correlation across studies with various clinical samples was large and negative (r = −.49, 95% CI = [−.54, −.44]; see Fig. S5 in the Supplemental Material). This pattern was also found when subanalyzing only depressed samples and only individuals with anxiety disorders (see Table S9 in the Supplemental Material).
Eight narration studies were not included in meta-analytic review because their design and outcomes were too different. For a narrative synthesis of these eight studies, including their main findings, see Table S4 in the Supplemental Material. These studies suggest that individuals with anxiety and depressive disorders report more overall and upward comparisons and lower self-ranking than nonclinical populations (Antony et al., 2005; MacMahon & Jahoda, 2008; Morina et al., 2022). Two studies reported that individuals with schizophrenia make less upward than downward or lateral social comparisons (Franz et al., 2000) and report more negative reactions on upward and downward comparisons than healthy control subjects (Arigo & Torous, 2022). Two other studies reported frequent social comparison of participants with eating disorders (Tan et al., 2016) or individuals with various mental disorders (Nesi et al., 2019). Finally, Saffran et al. (2016) reported a high correlation between social comparison and eating-disorder symptoms. For further information, see Table S4 in the Supplemental Material.
Discussion
Our process-based framework of social comparison and health segments the social-comparison process into four components: (a) acquiring social information, (b) evaluating (dis)similarities between the target and the standard, (c) the valuation of the comparison outcome, and (d) the engendered responses. It further posits reciprocal influences between social comparison and health behavior. We use this model to structure and interpret current findings and make recommendations for future research.
Our meta-analysis drew on an established categorization of studies into selection, reaction, and narration designs, reflecting the predominant approaches used in this field. At the same time, our systematic search also sought to capture studies employing alternative methodologies. A total of 72 studies on social comparison on mental health could be included. The data clearly suggest a strong relationship between social comparison and psychopathology. Overall, our findings are in line with and extend results of previous meta-analyses. They confirm that upward appearance comparisons are negatively related to body dissatisfaction (Myers & Crowther, 2009), that individuals with depressive symptoms evaluate themselves negatively relative to others (Wetherall et al., 2019), and that frequency of upward social comparison is significantly associated with depression, anxiety, and PTSD (Hoppen et al., 2020; McCarthy & Morina, 2020). Our work further extends prior reviews by providing an up-to-date synthesis of the accumulated evidence base.
Applying our model of social comparison to the available findings reveals several major limitations in the existing literature. First, research has predominantly examined isolated aspects of social comparison, limiting conclusions about how social comparison functions as a process that influences health and health behavior and vice versa. Second, important components of social comparison remain largely unexplored. For example, no data are available from individuals with mental disorders on social-comparison selection or on the impact of social comparison on prospective behavior. Finally, most studies relied on self-report measures of social comparison, raising concerns about the validity of the conclusions.
In the following and drawing on the social-comparison-process segmentation outlined in the introduction (see Fig. 1), we first summarize and situate the meta-analytic findings and then identify directions for future research in this domain.
Seeking or encountering social comparison
Remarkably, we found no study that investigated how patients select social-comparison standards in their daily life or therapeutic settings. A recent study with individuals with subclinical depression (Schlechter et al., 2024b) reported that when those individuals were instructed to select and read one vignette from four depicting varying symptom severity and coping potential, they predominantly chose a vignette portraying mild depression with effective coping rather than severe depression with poor coping.
Limited research yielded that patients with mental disorders frequently engage in daily life comparisons as assessed in 2-week diaries (Antony et al., 2005; Goodman et al., 2021) or spontaneously report social comparison when asked to substantiate their well-being judgment (Morina et al., 2022). Relatedly, 17 studies assessed social-comparison tendency; most of them used the Iowa-Netherlands Comparison Orientation Measure (Gibbons & Buunk, 1999), which assesses comparison tendency with items such as “I often like to talk with others about mutual opinions and experience.” The results yielded a significantly stronger social-comparison tendency in clinical groups than in nonclinical groups. However, the assessment of comparison orientation only indirectly informs about actual comparison behavior. In particular, they do not assess actual social-comparison behavior or differentiate between upward, lateral, and downward comparisons. This limitation is relevant because the frequency of comparison to upward versus downward comparisons may change over time as a result of illness duration (Helgeson & Taylor, 1993), treatment characteristics (Bogart & Helgeson, 2000), or other person or context variables (Arigo et al., 2014). Failing to distinguish between upward and downward comparisons may miss changes in their relative proportions. In addition, findings with individuals with subclinical psychopathology suggest that upward social comparisons are more strongly associated with psychological well-being and psychopathology than downward comparisons (Churbaji & Morina, 2024; McCarthy et al., 2023; Morina, 2020; Morina et al., 2024; Schlechter et al., 2023).
The basic comparison process
Recall that the basic core variable in social comparison concerns the evaluation of (dis)similarities between the target and the standard. Surprisingly, hardly anything is known about this core variable in individuals with mental disorders. We included a total of 23 narration studies that examined how individuals with mental disorders evaluated themselves relative to other individuals. All but three of them used the Social Comparison Scale (Allan & Gilbert, 1995), which instructs participants to rate themselves “in relation to others” on 11 bipolar constructs (e.g., unlikeable to more likeable). Although social ranking is an important construct that is significantly correlated with psychopathology, defining judgments of relative standing as social comparison can be problematic because such judgments do not necessarily involve consideration of real or imagined social comparisons (Wood, 1996). In this regard, Alicke et al. (2013) argued that self-judgments at this level are heuristic (e.g., doing worse than the average heuristic) rather than deliberate. Otherwise, researchers would have to treat virtually any self-descriptive evaluation (e.g., how intelligent one considers oneself) as an instance of social comparison. In addition, given that the Social Comparison Scale summarizes the self-evaluation across 11 dimensions, dimension-specific effects might be overlooked. When it comes to self-report assessments of social comparison, employing measures that directly assess the extent to which individuals examine (dis)similarities between themselves and others along specific dimensions (e.g., appearance, Morina et al., 2024) may substantially advance understanding. However, experimental designs and ecological momentary assessments are better suited to achieving this aim. Currently, there is a lack of knowledge about how individuals with mental disorders construct mental representations of social comparison. Likewise, it is not known how a comparer’s prior mental representation of the target dimension is modified in the course of social comparisons.
Valuation of the comparison outcome relative to personal motives and coping
Valuation of the comparison outcome will influence how the comparer reacts to the comparison outcome (Morina, 2021). Alignment of a significant comparison outcome with personal motives and perceived coping abilities will lead to different reactions than nonalignment. For example, a patient with depression compares herself with another fellow patient who is doing better and valuates the comparison outcome (worse well-being) as challenging and the desired end state as attainable. However, another patient in the same situation might valuate the comparison outcome as threatening and the desired end state as nonattainable. These two comparers might react differently as a result, with the first patient being more likely to focus on how to improve their well-being than the second patient. However, none of the included studies in our systematic search had investigated how the comparison outcome was valuated.
Responses following social comparison
Nine experimental studies reported a significantly stronger negative effect of experimentally induced social comparison on affect, envy, or perceptions of attractiveness relative to nonclinical groups. Furthermore, social comparison seems to increase attention for disorder-related features, for example, appearance in individuals with anorexia nervosa (Sfärlea et al., 2023). Importantly, however, there is lack of experimental research examining the long-term effects of social comparison on affect, cognition, or behavior. There is also lack of narration studies assessing responses to social comparison, apart from a diary study (Antony et al., 2005) and an ecological-momentary-assessment study (Goodman et al., 2021), both of which reported greater changes in affect following upward social comparison in individuals with social anxiety relative to nonclinical groups.
Altogether, research has focused almost exclusively on short-term comparison reactions. This represents a major limitation because such short-term reactions have limited relevance for predicting long-term behavior in both health and nonhealth domains.
Future directions on social comparison and health behavior
The included studies indicate that individuals with (vs. without) mental disorders compare more often and report a lower social ranking and that frequent social comparison is significantly related to health. Furthermore, individuals with mental disorders have stronger reactions to experimentally induced social comparison than nonclinical samples. Overall, the available literature on social comparison and well-being supports the assumption that social comparison is a key factor in the development of, maintenance, and coping with ill-being (Klein & Rice, 2020; Morina et al., 2022). However, to advance a clinically meaningful understanding of social comparison in mental health, future research must move beyond documenting associations and toward identifying processes through which social comparison shapes well-being, symptoms, and behavior over time. Below, we outline several interrelated directions that are particularly relevant for clinical-psychological science because they offer leverage at distinct stages of the comparison process and can inform the identification of modifiable targets for intervention.
Seeking or encountering social information
A foundational task for future research is to elucidate how individuals with mental disorders construct and select social-comparison standards, under what conditions, and for what functional purposes. Although comparison standards span a wide spectrum, ranging from close others to distant, abstract, or even fictional targets and stereotypes (Wood, 1996), empirical research has largely relied on implicitly assumed standards (e.g., the “average patient”), often obscuring how comparison targets are actually generated, recalled, and prioritized in daily life. Future studies should therefore investigate how cognitive availability, representativeness, diagnostic uncertainty, and contextual constraints shape the construction of comparison standards in clinical populations. Closely related is the need to clarify comparison-selection mechanisms. Building on coping-oriented and motivational accounts (Wood, 1989), we believe research should examine how self-motives, health perceptions, dispositional factors (e.g., perceived agency, intolerance of uncertainty), comparison attitudes (Schlechter et al., 2024a), and situational demands influence the selection of comparison targets. Importantly, lateral comparisons remain largely neglected in clinical research. Individuals with mental disorders are likely to evaluate their well-being, coping abilities, and treatment considerations through comparisons with similar others. In addition, little is known about the prevalence, functions, and attitudinal underpinnings of comparison avoidance, that is, when and why individuals refrain from engaging in social comparison. Comparison nonselection can reflect a broader pattern of avoidance that maintains symptoms over time. Moreover, such avoidance may preclude access to potentially informative comparison information, thereby limiting opportunities to recalibrate self-evaluations and to identify more adaptive ways of coping with complaints.
The basic comparison process
Beyond engaging in social comparison, future research must address how individuals with mental disorders construct mental representations of comparison targets (e.g., personal well-being) and how these representations change as a consequence of comparison. This is clinically relevant because social comparison shapes perceptions of well-being, symptom meaning, and illness identity (Diener & Fujita, 1997; Morina et al., 2022). Accordingly, research should examine factors that direct attention toward perceived similarities versus differences between self-attributes and comparison standards and processes that determine the perceived discrepancy to the standards. To advance theory, it will be essential to disentangle assimilation and contrast effects by assessing both prior and posterior construals of comparison targets and dimensions (see Fig. 2). Without separating these stages, it remains unclear whether observed effects reflect preexisting representations or comparison-induced changes in meaning. Process-sensitive designs that capture representational change over time are therefore crucial for understanding how social comparison dynamically reshapes self-evaluation and symptom appraisal.
Valuation of the comparison outcome
Given the importance of comparison-outcome appraisal in shaping behavioral consequences and the lack of empirical work on it, future research should prioritize the systematic investigation of how comparison outcomes are appraised and regulated. Our social-comparison model incorporates the literature on appraisal (e.g., Ellsworth, 2024) and motives (e.g., Dweck, 2017) to provide a systematic framework for analyzing the mechanisms underlying comparative valuation. Appraisal theories conceptualize emotions as dynamic processes composed of interrelated components, including cognitive appraisals, action tendencies, physiological activation, expressive behavior, and subjective experience. The resulting configuration of appraisal values activates a corresponding action tendency, which in turn elicits physiological changes that prepare the organism for context-appropriate action (Scherer & Moors, 2019). In line with this view, our social-comparison framework posits that the valuation of the comparison outcome determines both the immediate affective consequences of social comparison and its longer-term effects on motivation, behavior, and well-being. Future research should examine how individuals with mental-health complaints appraise comparison outcomes in terms of goal relevance, valence, perceived controllability, and coping capability. A key challenge is to identify mechanisms that determine whether comparison outcomes are experienced as appetitive, neutral, or aversive and whether they are appraised as challenges or threats. These appraisal pathways are likely to differentially predict adaptive engagement versus avoidance, withdrawal, or quiescence. Evidence from nonclinical samples suggests that upward comparisons can, under certain conditions, function as sources of inspiration and motivation (Buunk et al., 2020). Determining when and how comparisons with fellow patients serve as a source of inspiration and motivation represents a crucial translational question. In this context, perceived discrepancy magnitude and attainability are likely to be decisive in shaping whether upward comparisons will foster motivation.
Comparison responses
Future research should identify the mechanisms through which social comparisons shape well-being, motivation, and behavior over time. Although social comparisons are known to function as potent emotional cues by signaling relative standing, goal progress, and social evaluation (Diel et al., 2021), the processes linking comparison outcomes to emotional and behavioral trajectories remain insufficiently understood. A first priority is to examine how the appraisal of comparison outcomes gives rise to distinct emotional responses. Appraisal theory and empirical evidence suggest that emotions are initiated when a stimulus is evaluated along multiple appraisal dimensions, such as its relevance to personal goals, its congruence or incongruence with those goals, and its perceived controllability. Research should systematically investigate how goal congruence, perceived controllability, and the meaning and attainability of comparison standards shape emotional reactions, such as pride, shame, anxiety, anger, or envy (Diel et al., 2025; Meier & Johnson, 2022). In particular, future studies should distinguish between benign and malicious forms of envy and clarify the conditions under which upward comparisons promote motivation versus exacerbate distress (Diel et al., 2025). Second, integrating appraisal-based emotion models (Scherer & Moors, 2019) into the study of social comparison may help to explain why similar comparison outcomes elicit different emotions across individuals and contexts. This includes examining attributional processes that differentiate emotions such as anger or fear from guilt or shame following unfavorable comparisons (Tracy & Robins, 2006). Third, a key challenge for future research is to clarify how short-term affective responses to social comparison translate into longer-term behavioral and motivational outcomes. We propose that this translation is mediated by individuals’ cognitive orientation toward the comparison outcome, including regulatory processes, such as self-affirmation, commitment, distraction, reconstrual, and rededication (see Fig. 1). Empirical work is needed to test whether these orientations systematically mediate the effects of affective valuation on persistence, disengagement, assimilation, or quiescence and to determine how reconstrual and rededication reshape the meaning of comparison outcomes over time.
Moderators, generalizability, and transdiagnostic relevance
The examination of moderators in our review was substantially constrained by heterogeneity in study designs and operationalizations. Studies differed widely in whether they addressed selection, reaction, or narration processes, and even within these categories, the number of studies per design and per outcome was often too small to permit reliable moderator analyses, highlighting a critical gap in the literature. To advance understanding of the mechanisms that drive social-comparison behavior in clinical populations, researchers need to systematically target distinct components of the social-comparison process and employ more consistent operationalizations.
Future studies should explicitly examine how individual characteristics (e.g., age, gender, socioeconomic status, personality traits), illness-related factors (e.g., diagnosis, symptom severity, illness duration), and contextual influences (e.g., cultural norms, treatment settings, or life events) moderate the effects of social comparison (Schlechter, Hoppen, & Morina, 2026). Such work algins with clinical-personalization research and is necessary for identifying for whom and under what conditions social-comparison processes are most likely to be harmful or beneficial (Huibers et al., 2020). In addition, cross-cultural and developmental perspectives are needed because comparison standards, meanings, and consequences are likely to vary across cultural contexts and across the life span. Importantly, research should routinely include nonclinical and subclinical samples not merely as control groups but as integral components of a continuum-based, transdiagnostic approach to mental health. Such designs are essential for distinguishing general psychological processes from those that are amplified, dysregulated, or rigidified in mental disorders.
Methodological priorities
Addressing these questions will require methodologically diverse and process-sensitive designs. Longitudinal and ecological-momentary-assessment approaches are especially well suited to capturing the dynamic and context-dependent nature of social comparison in daily life and its implications for well-being (Arigo et al., 2020). These methods allow researchers to assess social-comparison processes as they unfold in naturalistic settings, thereby reducing retrospective bias and enabling the examination of within-persons fluctuations in comparison standards, valuation, and associated emotional and behavioral responses that cumulatively shape momentary and longer-term well-being (Goodman et al., 2021; Schlechter, Meyer, et al., 2026). For example, event-contingent assessments allow researchers to sample comparison selection, target characteristics, perceived discrepancy, appraisal, and immediate affect proximal to the comparison event itself, thereby minimizing reconstruction biases and enabling fine-grained tests of short-term causal sequences. Complementarily, modeling within-persons daily fluctuations in comparison frequency, direction (upward, lateral, or downward), and valuation makes it possible to distinguish stable individual differences from momentary deviations and to examine whether day-to-day increases in maladaptive comparison predict same-day or next-day changes in mood, symptom severity, motivation, or health behavior. Such designs can test temporal ordering (e.g., whether heightened negative affect precedes increased comparison or vice versa), identify lagged effects, and detect accumulation processes through which repeated small comparison-related perturbations compound into longer-term symptom trajectories. Experimental studies remain critical for isolating causal mechanisms and should be complemented by multimethod approaches integrating self-report and behavioral and physiological indicators. Together, this approach promises to advance a clinically meaningful, mechanistic understanding of social comparison as a transdiagnostic process that shapes behavior across the continuum of mental health and psychopathology.
Systematic-review limitations
A first limitation of this systematic review concerns construct validity. Several findings included in the meta-analysis were based on self-report measures of social comparison that are unlikely to validly assess core features of the social-comparison process. In particular, the most frequently used self-report measure, the Social Comparison Scale (Allan & Gilbert, 1995), is often interpreted as an index of social comparison, yet it primarily assesses perceived social rank rather than process of comparing oneself to specific targets along concrete dimensions. Future research relying on self-reports should therefore apply measures that explicitly involve thinking about real or imagined social comparisons (e.g., Antony et al., 2005; Morina et al., 2024) and clearly specify which features of social comparison they intend to access. A second limitation relates to study design and temporal scope. The majority of studies included in the review were cross-sectional and focused on short-term reactions to social comparison, substantially limiting the ability to draw causal inferences or to examine longitudinal processes. As a result, it remains unclear to what extent the observed associations reflect stable effects of social comparison, transient affective reactions, or bidirectional relationships between social comparison and health-related outcomes. Moreover, there is comparatively little research examining how individuals value comparison outcomes and how mediating and moderating mechanisms shape the longer-term emotional, cognitive, and behavioral consequences of social comparison. Finally, the generalizability of the findings is constrained by several factors. Most studies were conducted in relatively homogeneous samples, with limited representation of diverse cultural contexts, developmental stages, and specific clinical subgroups. In addition, there was substantial heterogeneity in the operationalization of core social-comparison dimensions across studies, further complicating the integration and interpretation of results. The experimental studies included in the review also employed highly diverse designs, precluding several potentially informative analyses.
Conclusion
In sum, current literature reveals that several unitary aspects of social comparison play a significant role in mental health. Yet the mechanisms of health-related social comparison are still poorly understood. The framework presented here suggests that the field needs to study health-related social comparison as a dynamic process consisting of social-comparison activation, basic comparison process, valuation, and engendered responses. Accordingly, future experimental and observational research needs to apply multifactorial designs to simultaneously examine several social-comparison components as they unfold in daily life and interact with each other and with relevant individual and contextual variables over time. Furthermore, researchers need to investigate the role of non-health-related comparisons on health. A better understanding of how social comparison shapes health perceptions and behavior will help identify effective strategies toward more adaptive comparisons and better well-being.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026261442164 – Supplemental material for Unraveling Social Comparison in Mental Health: A Process-Based Model and a Systematic Review and Meta-Analysis of Current Evidence
Supplemental material, sj-docx-1-cpx-10.1177_21677026261442164 for Unraveling Social Comparison in Mental Health: A Process-Based Model and a Systematic Review and Meta-Analysis of Current Evidence by Nexhmedin Morina, Frederike K. Lemmel, Pascal Schlechter and Thole H. Hoppen in Clinical Psychological Science
Footnotes
Acknowledgements
Transparency
Action Editor: Pim Cuijpers
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.