
Abstract
Recent evidence suggests that individuals with major depressive disorder (MDD) or borderline personality disorder (BPD) not only experience an excess of negative affect but also hold negatively biased internal representations of their affective experiences. Such biases may play an important role in the maintenance of these disorders. However, previous evidence in this area has mostly been based on nonclinical samples. The current experience sampling study compared the momentary affective experiences of 55 individuals with current MDD, 56 individuals with BPD, and 53 healthy individuals with their prior expectations and subsequent memories of these affective experiences. Results showed that individuals with both MDD and BPD considerably overestimated their future and past negative affect. Furthermore, they did not show the optimistic recall bias for positive affect observed in healthy individuals. Notably, the absence of an optimistic bias regarding the expectation of positive affect was specific to depression. Important theoretical and clinical implications are discussed.
Keywords
Experiencing excessive negative affect and difficulties in its regulation are central features of both major depressive disorder (MDD) and borderline personality disorder (BPD; for reviews, see Ebner-Priemer et al., 2015; Visted et al., 2018). Specifically, individuals with MDD experience sustained negative affect and a lack of positive affect (e.g., Vanderlind et al., 2020), whereas individuals with BPD experience an excess of negative affect with large and sudden shifts (i.e., affective instability; Trull et al., 2008). In the past decades, a great deal of research has been concerned with better understanding the causes of these affective disturbances in MDD and BPD (for reviews, see Ebner-Priemer et al., 2015; Joormann & Quinn, 2014). For a comprehensive understanding, however, it is essential to consider that the mental representation of an affective experience may differ from the original experience itself. For example, one may expect to feel worse than one will, or remember feeling worse than one did. Importantly, evidence suggests that our expectations about how we will feel as well as our memories of past affect have a much stronger impact on our behavior than our current affect (DeWall et al., 2016; Wirtz et al., 2003). If expectations about future affective experiences are negatively biased, people may avoid the situation in question or not engage in activities in which few positive emotions are expected, reducing potentially rewarding activities or social reinforcement. Likewise, negatively biased memories regarding one’s affect might contribute to a negatively biased view of one’s life and foster negatively biased expectations of one’s affect in the future. Thus, negatively biased mental representations of affective experiences may be a key mechanism in the maintenance of depression and BPD.
Past research has mainly examined biases in the mental representation of affective states among students and the general population. Findings indicate that individuals tend to overestimate the emotional impact of both positive and negative future life events, a phenomenon known as impact bias (Wilson & Gilbert, 2005). Impact bias may stem from underestimating one’s ability to regulate one’s emotions in response to adverse events (i.e., immune neglect) or from overlooking the impact of other concurrent events (i.e., focalism; Wilson & Gilbert, 2005). Evidence also suggests that people overestimate the intensity of their affective experiences when recalling them retrospectively (i.e., memory–experience gap; Miron-Shatz et al., 2009). The memory–experience gap has been more reliably found in relation to negative affect (Neubauer et al., 2020) and has been shown to be positively associated with neuroticism (Lay et al., 2017). The few studies in clinical samples suggest that individuals with MDD or BPD show a stronger memory–experience gap for negative affect than do healthy individuals (e.g., Ben-Zeev et al., 2009; Mneimne et al., 2021; Rinner et al., 2019).
A decade ago, research began to examine the role of biased expectations about future affective states for psychopathology (Hoerger et al., 2012; Wenze et al., 2012). The first studies were based on nonclinical samples with a large range in depression symptoms and used the experience sampling method (ESM) to contrast individuals’ expectations to their momentary affect in daily life. Results demonstrated that individuals with elevated depressive symptoms expected and recalled more negative and less positive affect than they reported in their daily lives. The strength of these biases increased with the level of depressive symptoms (Wenze et al., 2012, 2013). Individuals with more depressive symptoms also overestimated their negative affective reaction and underestimated their positive affective reaction to real-life events to a greater extent than individuals with fewer depressive symptoms (Hoerger et al., 2012). In both studies, biases were relatively specific to depressive symptoms and either not associated with anxiety or hypomanic symptoms (Hoerger et al., 2012) or only partiall associated with anxiety symptoms (Wenze et al., 2012).
These findings have stimulated an increasing number of studies examining the role that biased mental representations of affective experience may play in psychopathology. However, most of these studies have been based on nonclinical samples and/or used laboratory settings (for an overview, see Rizeq, 2024). Studies assessing how these processes unfold in daily life and among clinical samples remain scarce.
A previous study by our research group (Zetsche et al., 2019) compared expectations and memories of past and future affect with momentary affective experiences in the daily lives of clinically depressed and healthy individuals. Results demonstrated that depressed individuals expected and recalled considerably more negative affect and less positive affect than they would report in their daily lives. In contrast, healthy individuals’ expectations and memories of their negative affect were aligned with their momentary experiences in daily life. Healthy individuals even expected and recalled more positive affect than they would report in their daily lives. Although these results are informative, the sample size was rather small (N = 67) and warrants a replication. In addition, it remains unclear whether the observed biases are specific to MDD or also present in other mental disorders.
To date, only one study has compared depressed individuals’ affective forecasts and memories with those of a different clinical sample (Mathersul & Ruscio, 2020), that is, individuals with generalized anxiety disorder (GAD), individuals with comorbid MDD and GAD, and healthy individuals. Results demonstrated that all clinical groups overestimated their future and past negative affect to a greater extent and their future positive affect to a lesser extent than did healthy individuals. Interestingly, this pattern of biases was considerably stronger in all depressed individuals compared with individuals with GAD only. This suggests that biases in the mental representation of affective experiences may also be relevant in the context of anxiety disorders but that the extent of such biases may be specific to depression. It is important to consider, however, that depression and anxiety are highly comorbid, and subthreshhold depression symptoms may also be present in GAD.
Surprisingly little is known about biases in the expectation of daily affective experiences in BPD. Two previous studies examined affective expectations and their relationship with BPD symptoms in undergraduate students: Hughes and Rizvi (2019) compared students’ expected sadness and general affect in response to a sad film clip that they were scheduled to watch 5 to 7 days later with their momentary affect immediately after watching the clip. Overall, participants predicted more sadness and negative affect than they reported immediately after the clip. Unexpectedly, BPD symptoms were related to a smaller overestimation of sadness and negative affect. In a second study, Hughes et al. (2022) compared students’ expectations regarding their affective response to Valentine’s Day and the two subsequent days with their daily affect on those days. Results showed that BPD symptoms were associated with an overestimation of future negative affect on Valentine’s Day and the day after, and with an underestimation of positive affect on all three days. Notably, the expectation bias for positive affect disappeared when controlling for depressive symptoms. Finally, as mentioned above, individuals diagnosed with BPD have been found to show a stronger memory–experience gap for negative affect than healthy individuals (e.g., Ebner-Priemer et al., 2006; Mneimne et al., 2021).
The current study was designed to replicate our previous findings in a larger sample of clinically depressed individuals and to examine whether these biases are also present in another disorder that is predominantly characterized by affective disturbances (i.e., BPD). On the basis of the findings summarized above, we hypothesized that depressed individuals and individuals with BPD would expect and recall more negative affect than they would report in their daily lives and that these expectation and recall errors would be more pronounced in the two clinical groups than in healthy individuals (Ben-Zeev et al., 2009; Ebner-Priemer et al., 2006; Hughes et al., 2022; Mathersul & Ruscio, 2020; Zetsche et al., 2019). We further hypothesized that depressed individuals would hold a less favorable mental representation of their positive affect levels than would healthy individuals or individuals with BPD, that is, underestimation (see Zetsche et al., 2019) or less overestimation (see Mathersul & Ruscio, 2020) compared with that of healthy controls.
Transparency and Openness
Preregistration
This study is part of a large, preregistered research project on emotion regulation in MDD and BPD (Schulze et al., 2018). The study protocol provides details on the current sample (e.g., inclusion/exclusion criteria and sample size determination), all included measures, and the current research question but not the specific hypotheses.
Data, materials, code, and online resources
Deindividualized data, all statistical code, additional results, and all nonlicensed materials are available on OSF (https://osf.io/bfmtp/?view_only=d614b5cbce4f4958a2dfd74dbe7b1827). All unlicensed questionnaires and experience sampling items can be found in the Method section or the Supplemental Material available online.
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Ethics approval
The study was performed in accordance with the World Medical Association Declaration of Helsinki. The Freie Universität Berlin Ethics Committee approved the study protocol (No. 67/2013; Amendment 136/2017).
Method
Participants
Recruitment
Participants were recruited through online advertisements and flyers at various sites in Berlin. Participants with BPD or MDD were additionally recruited from a psychiatric unit at Charité–Universitätsmedizin Berlin (after being discharged) and from the outpatient clinic at Freie Universität Berlin. After an initial telephone screening, final eligibility was established by face-to-face interviews using the German version of the Structured Clinical Interview for DSM-IV (SCID) Axis I (Wittchen et al., 1997) and Axis II (Fydrich et al., 1997) disorders. All interviewers were trained in applying the SCID and were closely supervised for all interviews.
Inclusion and exclusion criteria
Participants had to identify as female (cf. Zetsche et al., 2024), be between 18 and 65 years old, and be native speakers of German (because of verbal tasks not reported here). Participants were excluded if they were pregnant, reported any severe brain injury or neurological disease, met the criteria for lifetime bipolar or psychotic disorders, or for substance abuse or dependency within the last 12 months. Participants in the healthy control group had to be free of any lifetime mental disorders as assessed by the SCID interviews and any psychotropic medication. Further, they were not allowed to meet more than two BPD criteria from the fourth edition of the Diagnostic and Statistical Manual of Disorders (DSM-IV; American Psychiatric Association, 1994), any of the cardinal DSM-IV MDD criteria, or a Beck Depression Inventory–II (BDI-II) score > 14. 1 Participants in the MDD group had to meet DSM-IV criteria for a current MDD, report a BDI-II score > 14 (Kuehner et al., 2023), and not meet more than two DSM-IV BPD criteria. Participants in the BPD group had to meet DSM-IV criteria for BPD and must not meet DSM-IV criteria for a current MDD. Participants with BPD were allowed to have experienced past depressive episodes to enhance the generalizability of findings in the BPD group. Participants with MDD or BPD were allowed to take psychotropic medication if the dose had been stable for 4 weeks before and during participation. Participants in the three groups were matched for age. In total, we recruited 168 participants (57 participants with MDD, 56 participants with BPD, and 55 healthy participants).
Final sample
Four participants were excluded from the analyses. One participant with MDD had a BDI-II score below the cutoff score (BDI-II = 8). One healthy participant had a BDI-II score above the cutoff score (BDI-II = 15). Another healthy participant completed the expectation questionnaire after the ESM assessment and did not complete the recall questionnaire. Last, one participant with MDD completed only seven ESM prompts (12.5%). The final sample included 55 women with current MDD, 56 women with BPD, and 53 healthy women (N = 164). A total sample size of 159 was determined by an a priori power analysis to ensure adequate power for detecting even small group effects using multilevel analyses of the ESM data (see Schulze et al., 2018).
Measures
Clinical symptom measures
We used the BDI-II (Beck et al., 1996) to assess the severity of depressive symptoms and the short version of the Borderline Symptom List (Bohus et al., 2009) to assess the severity of BPD symptoms. General psychopathological symptom severity was assessed using the Brief Symptom Inventory-18 Global Severity Index (Derogatis, 2001). We assessed basic cognitive capabilities with Leistungsprüfsystem Subtest 4 (Horn, 1983).
Momentary affect in daily life
We assessed participants’ momentary affect in daily life using a study smartphone with a preinstalled experience sampling application (movisensXS; movisens GmbH, Karlsruhe, Germany). The application was programmed to beep eight times a day for seven consecutive days (56 beeps total). The sampling period was divided into eight equal time blocks between 9 a.m. and 9 p.m., and beeps occurred pseudorandomly within each time block with a minimum interval of 45 min between beeps. Prompts could be postponed up to three times for a maximum of 15 min.
Following each prompt, participants were asked to indicate on a scale from 1 (not at all) to 7 (very much) how tense, angry, anxious, depressed, lonely, ashamed, cheerful, and happy they felt just before the beep. Note that we conducted all analyses on the level of a composite negative and a composite positive affect score because individuals with BPD or MDD may have problems differentiating between specific emotions (for a review, see Smidt & Suvak, 2015). The negative affect score was the mean across the items angry, anxious, ashamed, depressed, lonely, and tense at each prompt (ωbetween = .93, ωwithin = .76). The positive affect score was the mean across the items cheerful and happy at each prompt (ωbetween = .97, ωwithin = .88). Participants were asked to answer further questions not part of the current study (e.g., on emotion regulation strategies, self-injury, and sleep quality; see Schulze et al., 2018). Participants received an extra incentive of €10 for responding to more than 90% of the prompts (the standard compensation for participating in the study was €120).
Expectation and recall of affect
One day before experience sampling started, participants completed a questionnaire asking how they expect to feel on average over the next week to assess participants’ mental representations of their future affect (Wenze et al., 2012). The questionnaire consisted of the same eight emotion items and the same response scheme as used in the ESM. We computed expectation scores for negative affect (mean rating for tense, angry, anxious, depressed, lonely, and ashamed; McDonald’s ωtotal = .91) and positive affect (mean rating for cheerful and happy; α = .91).
One day after the end of the experience sampling period, participants completed a questionnaire asking how they had been feeling on average during the past week to assess participants’ mental representations of their past affect (Wenze et al., 2012). The questionnaire consisted of the same eight affect items and the same response scheme as the expectation questionnaire. We computed recall scores for negative affect (mean rating for tense, angry, anxious, depressed, lonely, and ashamed; McDonald’s ωtotal = .92) and positive affect (mean rating for cheerful and happy; α = .94).
Procedure
The study consisted of two laboratory sessions and a 7-day experience sampling period between sessions. In the first session, participants provided written informed consent and completed the questions about their expected affect and their clinical symptoms, among others. Participants were equipped with a study smartphone and were asked to answer the questions prompted by the experience sampling application over the next 7 days. After the experience sampling period, participants returned to the lab to complete the affect recall questionnaire, among others. Participants were debriefed and compensated.
Statistical analysis
To test our hypotheses, we estimated Bayesian regression models using the R package brms (Bürkner, 2017), which is based on Stan (Carpenter et al., 2017). We always chose the default priors of brms, which are selected to be non- or weakly informative (Bürkner, 2017, 2018). For all models, we ran four Markov Monte Carlo chains, each with 1,000 warmup and 15,000 postwarmup samples, for a total of 56,000 postwarmup samples. All models converged with Rˆ < 1.01 (Vehtari et al., 2021) and estimated effective sample sizes of 562 or more (all but four effective sample sizes were greater than 1,000). No divergent transitions occurred. All independent variables were unstandardized. For all multilevel models, we allowed the between-person variance to vary between groups because we assumed that the expected, momentary, and recalled levels of affect might show a greater variance in the two clinical groups than in the control group. Group was always dummy coded with the control group as the reference group. We computed specific contrasts to examine differences between the two clinical groups. We did not impute missing data and computed all Bayesian multilevel models on the basis of the existing data points. This approach corresponds to the Bayesian version of the full information maximum likelihood method in the context of multilevel modeling. The exact R code for all models can be found in the Supplemental Material and on OSF. We considered effects to be clearly different from zero if the 95% credible interval (CrI) for the estimate (i.e., Bayesian confidence interval based on posterior quantiles) did not contain zero.
Group differences in expected and recalled affect
To test whether the groups differed in their expected or recalled affect, we estimated four Bayesian linear regression models with group as the independent variable. The dependent variable was either the expectation or the recall score for positive or negative affect, respectively.
Group differences in momentary affect in daily life
To test whether the groups differed in their momentary affect in daily life, we computed two hierarchical Bayesian multilevel models with group as the independent variable and the scores for negative or positive affect, respectively, as the dependent variable. Both hierarchical multilevel models accounted for the nested structure of our data (prompts nested within individuals), with varying intercepts across individuals.
Group differences in expectation and recall errors
First, we computed error scores between individuals’ predicted and momentary affect and between individuals’ recalled and momentary affect, respectively (Wenze et al., 2012). Error scores were computed by subtracting individuals’ momentary affect score at each prompt from their predicted or recalled affect score, respectively. Thus, positive values indicate an overestimation of future or past affect relative to individuals’ momentary affect at that assessment time, and negative values indicate an underestimation of future or past affect relative to individuals’ momentary affect. Spearman-Brown-corrected split-half reliability estimates for these error scores were as follows: expectation error for negative affect (r = .99), expectation error for positive affect (r = .99), recall error for negative affect (r = .99), and recall error for positive affect (r = .97).
To examine group differences in expectation or recall errors, we estimated four hierarchical Bayesian multilevel models with group as the independent variable and the respective error score (i.e., expectation error for negative or positive affect, respectively, and recall error for negative or positive affect, respectively) as the dependent variable. All hierarchical models accounted for the nested structure of our data (prompts nested within individuals), with varying intercepts across individuals.
Results
Group characteristics
Table 1 shows the sociodemographic and clinical characteristics of our sample. We did not assess ethnic identification or cultural background. Table S1 in the Supplemental Material depicts all comorbid mental disorders by group.
Demographic and Clinical Characteristics for the Three Diagnostic Groups
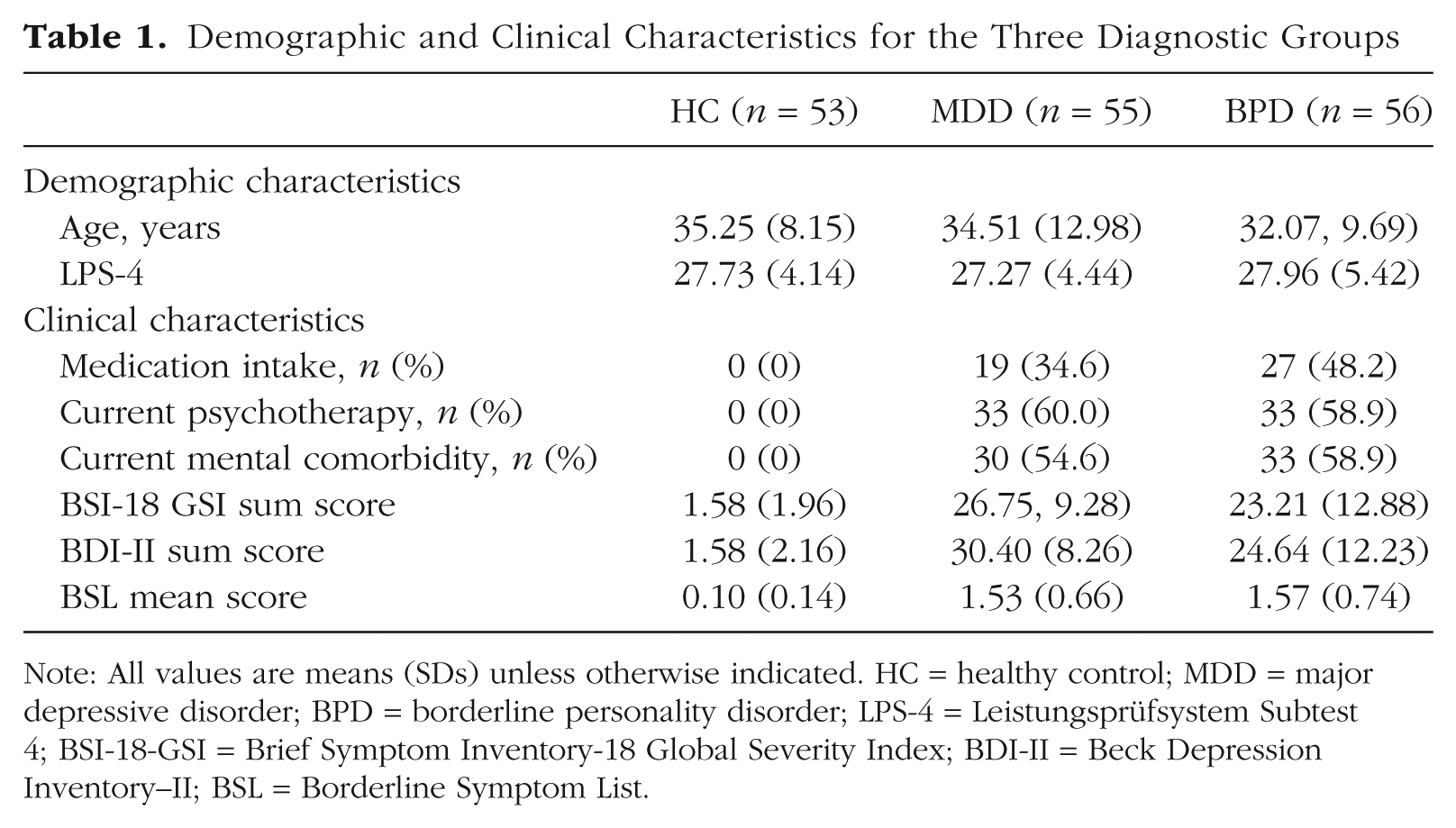
Note: All values are means (SDs) unless otherwise indicated. HC = healthy control; MDD = major depressive disorder; BPD = borderline personality disorder; LPS-4 = Leistungsprüfsystem Subtest 4; BSI-18-GSI = Brief Symptom Inventory-18 Global Severity Index; BDI-II = Beck Depression Inventory–II; BSL = Borderline Symptom List.
Compliance with ESM protocol
Participants’ compliance with the ESM protocol was high. Median response rates (and interquartile ranges; IQRs) to the presented prompts were 91.07% (IQR = 10.75) for the BPD group, 92.86% (IQR = 8.93) for the MDD group, and 89.80% (IQR = 15.79) for the healthy control group. The average completion time for single surveys was 24 s (SD = 18.4). Note that six participants received prompts for only 4 (n = 1), 5 (n = 3), or 6 (n = 2) days because of technical problems. For the same reason, an average of 0.86% of prompts were not presented in the remaining participants.
Interval between questionnaires and ESM period
Most participants (96%) rated their expected affect 1 day before the experience sampling period, and 92% rated their recalled affect 1 to 3 days after the end of the experience sampling period. Only six participants rated their expected affect more than 3 days before the ESM assessment, and 12 participants rated their recalled affect more than 3 days after the end of the ESM assessment. The time intervals between the assessment of expected/recalled affect and the ESM assessment were not associated with expectation or recall errors (all |rτs| < .04; all ps > .48).
Expected future affect
Table 2 shows expected, momentary, and recalled affect scores as well as expectation and recall errors by group. Figure 1 depicts group differences in expected, momentary, and recalled affect levels, and Figure 2 depicts group differences in expectation and recall errors.
Estimates and 95% CrIs for All Relevant Variables by Group
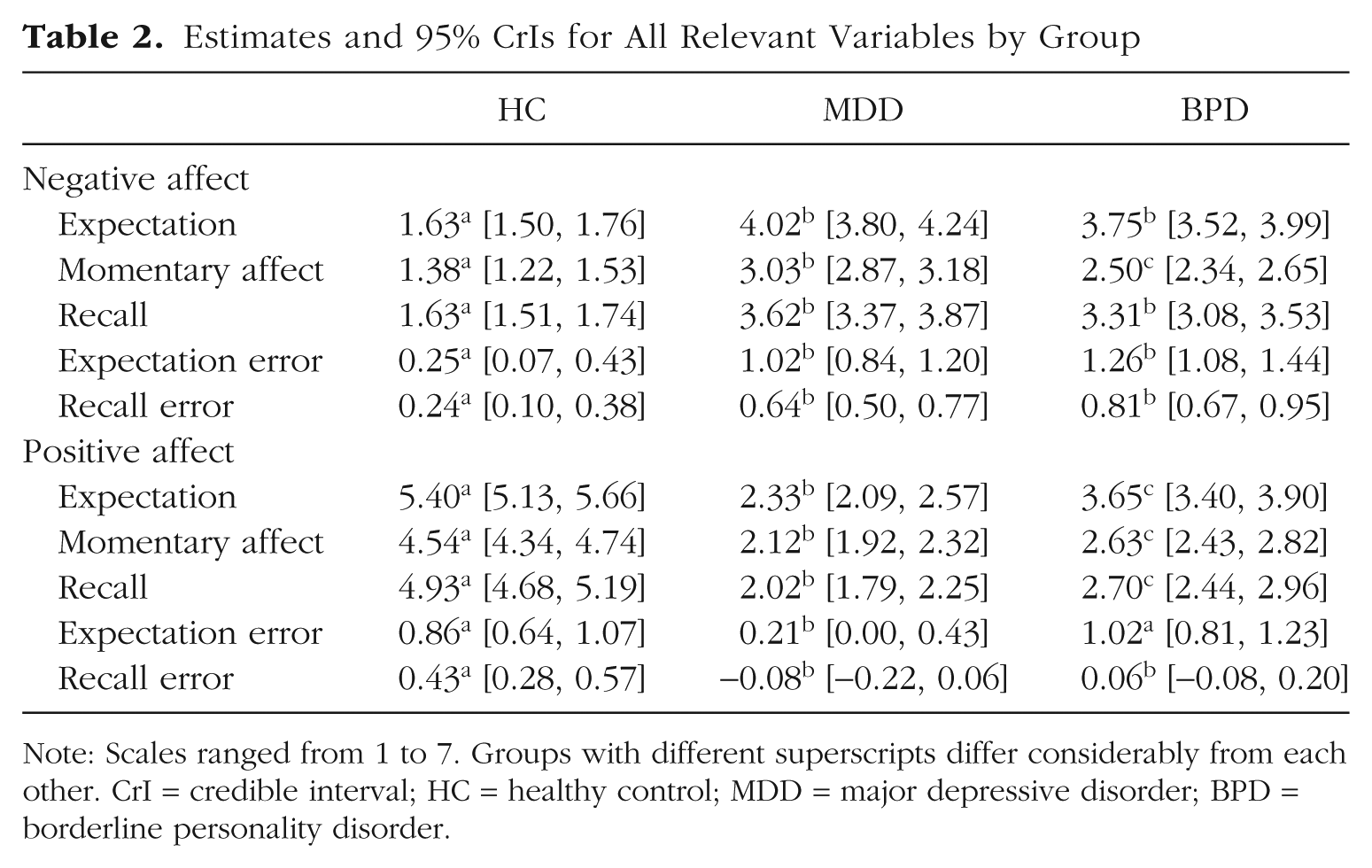
Note: Scales ranged from 1 to 7. Groups with different superscripts differ considerably from each other. CrI = credible interval; HC = healthy control; MDD = major depressive disorder; BPD = borderline personality disorder.
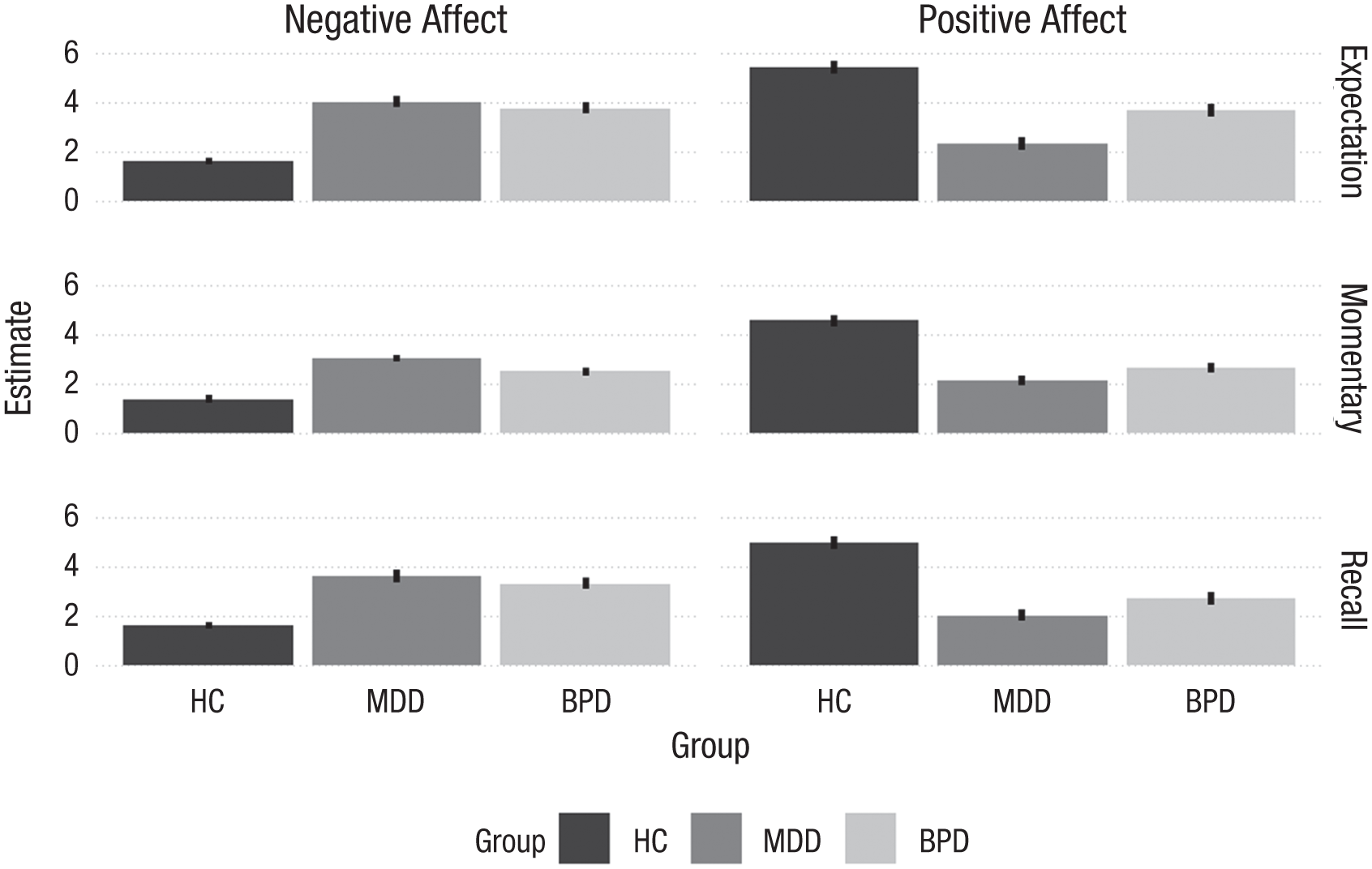
Expected, momentary, and recalled negative and positive affect by group. The bars represent the model estimates for the group means and the lines their 95% credible intervals. HC = healthy control; MDD = major depressive disorder; BPD = borderline personality disorder.
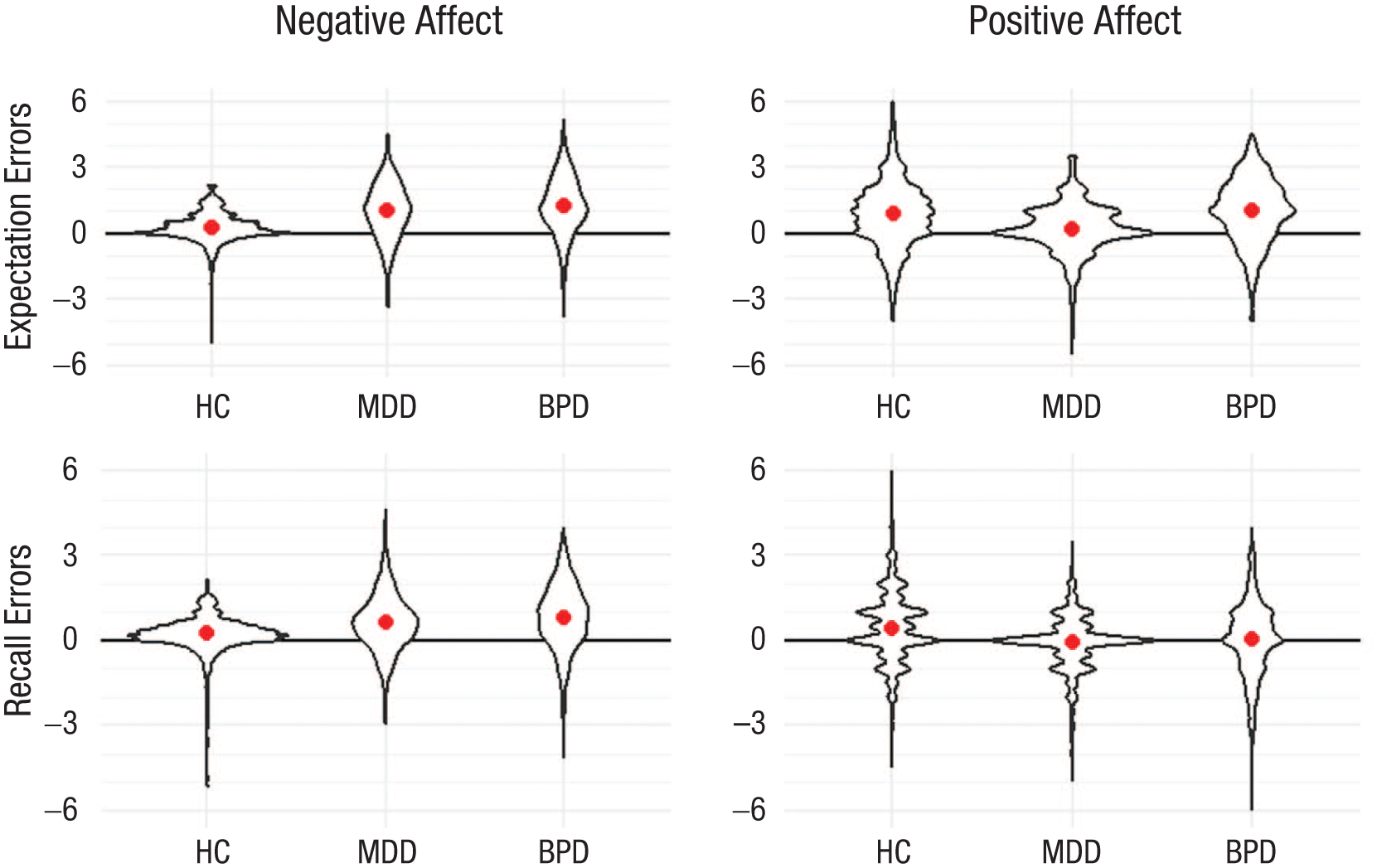
Expectation and recall errors for negative and positive affect by group. Violin plots represent actual data. The dots and lines in the violin plots represent the model estimates for the group means and their 95% credible intervals. Error scores were computed by subtracting individuals’ actual affect score at each prompt from their predicted or recalled affect score, respectively. Error scores > 0 indicate an overestimation of future or past affect relative to individuals’ momentary affect. Error scores < 0 indicate an underestimation of future or past affect relative to individuals’ momentary affect. HC = healthy control; MDD = major depressive disorder; BPD = borderline personality disorder.
Individuals with MDD or BPD expected to experience considerably higher levels of negative affect than healthy individuals, bMDD − bcontrol = 2.39, 95% CrI = [2.14, 2.64]; bBPD − bcontrol = 2.12, 95% CrI = [1.86, 2.39], but did not differ from each other, bMDD − bBPD = 0.27, 95% CrI = [−0.05, 0.58].
Individuals with MDD or BPD expected to experience considerably lower levels of positive affect than healthy individuals, bMDD − bcontrol = −3.07, 95% CrI = [−3.43, −2.71]; bBPD − bcontrol = −1.74, 95% CrI = [−2.11, −1.38]. Depressed individuals expected to experience considerably less positive affect than individuals with BPD, bMDD − bBPD = −1.32, 95% CrI = [−1.67, −0.97].
Momentary affect in daily life
Individuals with MDD or BPD reported considerably more momentary negative affect than healthy individuals, bMDD − bcontrol = 1.65, 95% CrI = [1.43, 1.87]; bBPD − bcontrol = 1.12, 95% CrI = [0.90, 1.33]. Moreover, individuals with MDD reported considerably more momentary negative affect than individuals with BPD, bMDD − bBPD = 0.53, 95% CrI = [0.31, 0.75].
Similarly, individuals with MDD or BPD reported considerably less momentary positive affect than healthy individuals, bMDD − bcontrol = −2.42, 95% CrI = [−2.71, −2.14]; bBPD − bcontrol = −1.91, 95% CrI = [−2.19, −1.63]. Individuals with MDD reported considerably lower levels of momentary positive affect than individuals with BPD, bMDD − bBPD = −0.51, 95% CrI = [−0.79, −0.23].
Recalled past affect
Individuals with MDD or BPD recalled considerably higher levels of negative affect than healthy individuals, bMDD − bcontrol = 1.99, 95% CrI = [1.72, 2.27]; bBPD − bcontrol = 1.68, 95% CrI = [1.43, 1.93], but did not differ from each other, bMDD − bBPD = 0.31, 95% CrI = [−0.02, 0.65].
Individuals with MDD or BPD recalled considerably lower levels of positive affect than healthy individuals, bMDD − bcontrol = −2.91, 95% CrI = [−3.26, −2.57]; bBPD − bcontrol = −2.23, 95% CrI = [−2.60, −1.87]. Further, depressed individuals recalled considerably less positive affect than individuals with BPD, bMDD − bBPD = −0.68, 95% CrI = [−1.03, −0.33].
Expectation errors
All three groups overestimated their future negative affect compared with their momentary negative affect reported in daily life (i.e., their expectation errors for negative affect were clearly different from zero; see Table 2). Both clinical groups overestimated their future negative affect considerably more than healthy controls, bMDD − bcontrol = 0.77, 95% CrI = [0.51, 1.02]; bBPD − bcontrol = 1.01, 95% CrI = [0.75, 1.27], but did not differ from each other, bMDD − bBPD = −0.24, 95% CrI = [−0.50, 0.01].
Surprisingly, all three groups also overestimated their future positive affect compared with their momentary positive affect reported in daily life (i.e., their expectation errors for positive affect were clearly different from zero; see Table 2). Depressed individuals overestimated their future positive affect considerably less than individuals with BPD or healthy individuals, bMDD – bBPD = −0.81, 95% CrI = [−1.12, −0.51]; bMDD − bcontrol = −0.65, 95% CrI = [−0.95, −0.33], who did not differ from each other, bBPD − bcontrol = 0.17, 95% CrI = [−0.14, 0.47].
Recall errors
All three groups retrospectively overestimated their past negative affect compared with their momentary negative affect reported in daily life (i.e., their recall errors for negative affect were clearly different from zero; see Table 2). Both clinical groups overestimated their past negative affect considerably more than healthy controls, bMDD − bcontrol = 0.40, 95% CrI = [0.21, 0.59]; bBPD − bcontrol = 0.57, 95% CrI = [0.38, 0.77], but did not differ from each other, bMDD − bBPD = −0.18, 95% CrI = [−0.37, 0.01].
Interestingly, only healthy individuals retrospectively overestimated their past positive affect compared with their momentary positive affect reported in daily life (see Table 2). Accordingly, healthy individuals overestimated their past positive affect considerably more than individuals with MDD or BPD, bMDD − bcontrol = −0.51, 95% CrI = [−0.71, −0.31]; bBPD − bcontrol = −0.37, 95% CrI = [−0.57, −0.17], who did not differ from each other, bMDD − bBPD = −0.14, 95% CrI = [−0.34, 0.06].
Robustness of main analyses
To examine whether our results were robust, we reran all analyses with only those participants who completed at least 6 days of the ESM assessment and filled in their expectations and recall ratings within 3 days of the start and end of the ESM assessment, respectively. Results remained the same (for details, see Tables S2a and S2b).
In addition, we examined whether group differences in expectation or recall errors were an artifact created by group differences in individuals’ average momentary affect in daily life. To this end, we included average momentary affect levels as a covariate in the models examining group differences in expectation and recall errors. The results remained the same (see Table S3).
Discussion
Negatively biased expectations and memories of one’s affective experiences may be a key mechanism by which affective disturbances in MDD and BPD are maintained. This study compared biases in the mental representations of daily affective experiences in individuals with MDD or BPD with those in healthy individuals.
Both clinical groups expected, recalled, and experienced more negative and less positive affect than healthy individuals. However, when looking at the alignment of individuals’ expectations and memories, results revealed more unfavorable distortions in both clinical groups compared with healthy individuals: Whereas all groups overestimated their momentary negative affect in daily life to some degree, biases in these expectations and memories were three to five times the size in the two clinical groups than those in healthy individuals. In addition, both clinical groups lacked the optimistic memory bias for positive affective experiences that was observed in healthy individuals. Notably, the absence of an optimistic bias regarding the expectation of positive affect was specific to depression: Depressed individuals exhibited a considerably smaller overestimation of their future positive affect than healthy individuals and individuals with BPD, who did not differ from each other.
These results allow several conclusions. First, there is accumulating evidence that overestimating one’s future positive affect might be an adaptive psychological process. Across all previous studies in this field, healthy individuals consistently expected to experience more positive affect than they would later report in daily life (e.g., Mathersul & Ruscio, 2020; Zetsche et al., 2019). This is also consistent with the literature on impact bias, which shows that people typically overestimate their positive affect in response to positive life events (e.g., Wilson & Gilbert, 2005). Overestimating future positive affect may serve motivational purposes (Morewedge & Buechel, 2013) and protect a positive self-image. In the current study, healthy individuals also slightly overestimated their levels of negative affect, both in prediction and retrospect. Slight biases in the representation of negative affective states are also in line with comprehensive findings from basic psychology research: People typically recall more negative affect than they originally reported (e.g., Miron-Shatz et al., 2009) and expect somewhat stronger emotional reactions to negative future events than they will later report (e.g., Wilson & Gilbert, 2005). Slight normative biases in the representation of negative affect may serve an adaptive function in coping with potentially threatening situations. However, if these biases become so pronounced that they overshadow those regarding positive affect, they may impair mental well-being.
Second, individuals with MDD or BPD greatly overestimated their future and past negative affective states, consistent with our hypothesis. The negative bias in their expectations and memories was three to five times the size of that in healthy individuals, which is consistent with previous studies in the context of depression (Mathersul & Ruscio, 2020; Zetsche et al., 2019). Notably, the current study is the first to demonstrate large negative biases in the expectation of future negative affect in individuals diagnosed with BPD. This is in accordance with evidence from a nonclinical student study that found that higher levels of BPD symptoms were associated with a greater tendency to overestimate one’s negative affect in response to Valentine’s Day (Hughes et al., 2022). Another study of undergraduates found that BPD symptoms were associated with a decreased tendency to overestimate negative affect after watching a sad film (Hughes & Rizvi, 2019). This converse relationship may have been due to the laboratory nature of the study and may not generalize to real-life settings. In sum, the pattern of our results demonstrates that individuals with MDD or BPD experience excessive negative affect and that their mental image of how bad they feel is greatly exaggerated. Our results also suggest that biases in the mental representation of one’s negative affect are substantially increased across different mental disorders. This is in line with previous findings by Mathersul and Ruscio (2020), who showed that individuals with GAD also overestimated their negative affect, albeit to a lesser extent than those with MDD. It is possible that individuals with a mental disorder may rely more heavily on general beliefs about themselves than on specific memories when answering questions about past or expected future affect states (for a review on the overgeneral memory effect, see Weiss-Cowie et al., 2023).
Notably, our study detected disorder-specific biases in the mental representation of future affective states. Specifically, blunted expectations of future positive affect were specific to depression in our study. Depressed individuals only minimally overestimated their future positive affect, and this bias was only one third the size of that of healthy individuals or individuals with BPD. This is consistent with the findings by Mathersul and Ruscio (2020) and similar to findings by Zetsche et al. (2019), who found that depressed participants even underestimated their future positive affect experienced in their daily lives. Interestingly, Mathersul and Ruscio (2020) also found that only depressive symptoms but not GAD symptoms predicted blunted expectations about individuals’ positive affect. In our study, depressed individuals (and individuals with BPD) also lacked the optimistic memory bias found in healthy individuals. Taken together, these findings align with evidence showing that aberrations in the experience and handling of positive affect are a hallmark feature of depression (e.g., Vanderlind et al., 2020). Expecting little positive emotions in the future may foster feelings of hopelessness, which are at the core of depressive disorders. Depressed individuals may also not be motivated to engage in pleasurable activities if few positive emotions are anticipated. Thus, depressed individuals’ blunted expectations of future positive affect may be a crucial mechanism by which depressive episodes are maintained.
The current study has some important limitations. First, the results are based on female participants only, which limits their generalization. Excluding men was a recruitment choice: Only one of three BPD patients in treatment centers are male, and these individuals often have a comorbid substance dependence, which was an exclusion criterion in this study (Sanchious et al., 2024). Second, individuals with BPD and comorbid current MDD were excluded, which limits the generalizability of our results to broader BPD populations. The aim of the current study was to replicate our previous findings in a larger sample of individuals with MDD and to compare their biases with those observed in a clinical control group. In addition, we aimed to extend previous correlational findings in nonclinical samples by examining the extent of biases in mental representation of affective states in individuals diagnosed with a mental disorder. We selected individuals with MDD or BPD because they both experience affective disturbances of similar magnitude, albeit of different quality (e.g., Trull et al., 2008). As a consequence, however, we considered it important to distinguish clearly between the two groups with regard to a current MDD diagnosis. Third, our study was cross-sectional, like all previous studies in this area. It will thus be intriguing for future research to examine whether biased mental representations of affective experiences predict the maintenance of mental disorders using longitudinal designs. Fourth, we assessed positive affect with only two items and therefore were not able to differentiate between low and high arousal positive affect. Last, we assessed expectations and memories of affective experiences across a 1-week period. It will be intriguing to examine whether the biases in mental representations of affective states increase in the clinical groups when longer time periods are used. Lay et al. (2017) found that the association between neuroticism and the memory–experience gap increased when participants reflected over longer time intervals, wich is in line with this assumption.
Taken together, the current study demonstrates that individuals with current MDD or BPD show greatly biased mental representations of their momentary affective experiences in daily life. Whereas the biased expectations and memories of negative affect are shared features of both disorders, the absence of an optimistic expectation bias regarding positive affective experiences is specific to depression (at least compared with BPD). These findings have important theoretical and clinical implications. First, the large extent of biases found in this study suggests that MDD and BPD are accompanied not only by disturbed affective experiences but also distortions in the mental representation of affective experience. Importantly, the latter impairments seem to be of the same magnitude as the impairments in momentary affective experience. It may thus be worth to include biases in the mental representation of one’s affect more explicitly into models of affective disturbances and affect regulation in these disorders. Second, our findings suggest that the absence of an optimistic expectation bias regarding positive affect is a characteristic of depression. These findings add to accumulating evidence showing that aberrations in the experience and handling of positive affect are a hallmark feature of depression (e.g., Vanderlind et al., 2020).
The current results also have important clinical implications: They suggest that it will be important for therapists to support patients in developing a more realistic and differentiated view of their momentary affective experiences. In depressed patients, a special focus should be placed on anticipating positive affective experiences. This may be done by thoroughly evaluating results of mood diaries and by communicating hope and focus on positive aspects and feelings as in “strength-based methods” (Flückiger et al., 2023) and “positive psychology” approaches (e.g., Santos et al., 2013).
Supplemental Material
sj-docx-1-cpx-10.1177_21677026261426975 – Supplemental material for Beyond Feeling Down: Expectations About and Memories of Daily Affective Experiences in Major Depressive Disorder and Borderline Personality Disorder
Supplemental material, sj-docx-1-cpx-10.1177_21677026261426975 for Beyond Feeling Down: Expectations About and Memories of Daily Affective Experiences in Major Depressive Disorder and Borderline Personality Disorder by Ulrike Zetsche, Julian Bohländer, Paul-Christian Bürkner, Stefan Roepke, Babette Renneberg and Lars Schulze in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Jennifer L. Tackett
Editor: Jennifer L. Tackett
Author Contributions
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.