
Abstract
Emotional disturbances are an inherent aspect of most mental disorders and possibly driven by impaired emotion regulation. In the present study, we examined how exactly affected individuals differ from healthy individuals in regulating their emotions and whether individuals suffering from different mental disorders face similar or distinct difficulty in emotion regulation. We overcome earlier methodological constraints by using a 7-day experience sampling assessing the employment and effectiveness of six regulation strategies real time in 55 individuals with current major depressive disorder, 52 individuals with borderline personality disorder (BPD), and 55 healthy individuals. All participants were female. Both clinical groups employed rumination and suppression more often and acceptance less often than healthy individuals. Depressed individuals ruminated even more often than individuals with BPD. Expressive suppression and rumination showed negative effects on subsequent emotions in all groups. Remarkably, both clinical groups were able to benefit from adaptive regulation strategies if they did select them.
Keywords
Emotional disturbances are an inherent aspect of most mental disorders. Affected individuals experience intense feelings of dysphoria, anxiety, euphoria, or a mix of these. In major depressive disorder (MDD), aberrant levels of negative affect are even a cardinal diagnostic symptom. Currently depressed individuals typically experience high levels of inert negative affect with large but slow shifts in affect (Nelson et al., 2020). Another condition with remarkably disturbed affect is borderline personality disorder (BPD). In contrast to depressed individuals, individuals with BPD experience instable affective states with sudden large changes in affect (e.g., Ebner-Priemer et al., 2007).
One possible cause for such emotional disturbances may be difficulties in regulating one’s emotions (e.g., Joormann & Stanton, 2016; Linehan, 1993). Emotion regulation, however, encompasses a variety of different processes (Koole, 2009). One of the most influential models (Gross, 1998; Sheppes et al., 2015) conceptualizes emotion regulation as a set of strategies individuals implement at different stages of the emotion-generation process to manage their emotional experiences. A comprehensive meta-analysis identified three such regulation strategies as being effective in down-regulating negative emotions in healthy individuals (Webb et al., 2012): cognitive reappraisal of the emotion-eliciting situation, acceptance of one’s emotional response, and distraction. In contrast, rumination showed clear negative consequences on individuals’ emotions, whereas suppression of one’s emotional expression showed negative effects on individuals’ physiological responding but not on individuals’ emotional experience. Consequently, deficits in emotion regulation may take many different forms, such as overusing maladaptive regulation strategies, underusing effective strategies, or failing to implement effective strategies successfully.
Numerous studies examining differences in emotion regulation between healthy individuals and individuals with mental disorders have been produced over the past decades. However, with few exceptions, studies either employed retrospective questionnaires to examine what individuals usually did to regulate their emotions or examined the effect of instructed strategy use on experimentally induced emotions in the lab. Both designs bear specific limitations. Individuals with mental disorders exhibit systematic biases in the recollection of emotional states (e.g., Ebner-Priemer et al., 2006; Zetsche et al., 2019). Thus, retrospective global self-reports should be interpreted with caution. Experimental designs have limited ecological validity: Watching video clips may evoke less self-relevant and intense emotions than personal events. Instructed strategy use may also differ from the spontaneous selection of strategies in daily life. Finally, previous research has mostly examined nonclinical samples or compared one clinical sample with healthy individuals. This prevents the ability to learn whether individuals with different mental disorders face similar or distinct difficulties in emotion regulation.
In the present study, we overcome these constraints by assessing various emotion-regulation strategies and their effect on subsequent emotions real time in the daily lives of healthy individuals and two clinical samples (i.e., individuals with current MDD or BPD). We chose these disorders because they both encompass emotional disturbances as a core symptom but differ in the nature of these symptoms. We assessed six different regulation strategies to understand the overall pattern of emotion regulation: rumination, suppression, cognitive reappraisal, acceptance, distraction, and social sharing.
Previous Findings and Hypotheses
Employment of emotion-regulation strategies in MDD and BPD
A comprehensive meta-analysis (Visted et al., 2018) summarized that currently depressed individuals retrospectively report employing maladaptive regulation strategies (rumination, suppression) considerably more often and adaptive strategies (cognitive reappraisal, acceptance) less often than healthy control subjects. There was one experience-sampling study confirming that clinically depressed individuals show more daily rumination than healthy individuals (Kircanski et al., 2015).
Likewise, individuals with BPD retrospectively reported using expressive suppression and rumination more often and cognitive reappraisal and acceptance less often than healthy individuals (for a review, see Daros & Williams, 2019). The few studies that have directly compared the two groups suggest that both habitually use cognitive reappraisal, acceptance, and suppression to similar extent; mixed findings were reported for rumination (Abela et al., 2003; Fernando et al., 2014; Sauer et al., 2016; Svaldi, Griepenstroh, et al., 2012). However, all of these studies included BPD patients suffering from a current comorbid major-depressive episode, which restricts conclusions.
Hence, we expected that both clinical groups employ rumination and suppression more often and cognitive reappraisal and acceptance less often in their daily lives than do healthy individuals. We further expected that individuals in each clinical group select putatively maladaptive strategies more often than adaptive strategies and that healthy individuals show the reversed pattern. We did not formulate hypotheses regarding distraction and social sharing because the respective database is yet sparse.
Effectiveness of emotion-regulation strategies in MDD and BPD
A recent literature review concluded that individuals with current MDD are as successful as healthy individuals in implementing experimental instructions for using reappraisal, distraction, or acceptance to ameliorate their mood (Liu & Thompson, 2017). However, instructed rumination had more detrimental effects on subsequent mood in currently depressed than in healthy nondysphoric individuals (Liu & Thompson, 2017). The latter finding was confirmed by an experience-sampling study that assessed spontaneous rumination (Ruscio et al., 2015).
Individuals with BPD have been found to be as successful in implementing cognitive reappraisal as healthy individuals (e.g., Krause-Utz et al., 2019). Similar to depression, instructed rumination had more detrimental effects on subsequent affect in individuals with BPD than in healthy individuals (Selby et al., 2009). Some findings have indicated that avoidance-based emotion regulation, such as suppression, may have an adaptive short-term function in BPD. For example, emotional suppression reduced negative affect in the daily lives of BPD patients (Chapman et al., 2016). Depressed individuals in the same study experienced less negative affect in response to instructed emotion suppression, suggesting differential effects of regulation strategies in the two groups. However, a third of BPD patients in this study suffered from current comorbid MDD, restricting the conclusions.
Hence, we expected that the negative effect of rumination on subsequent emotions is more pronounced in the two clinical groups than in healthy individuals. Furthermore, we expected that suppression is effective in reducing negative emotions only in individuals with BPD.
Method
Participants
Participants were recruited through online advertisements or specialized treatment facilities. After a telephone screening, eligible participants completed a face-to-face Structured Clinical Interview for DSM-IV (SCID) Axis I (Wittchen et al., 1997) and Axis II disorders (Fydrich et al., 1997). Interviewers were trained in applicating the SCID and were closely supervised for all interviews. Exact inclusion and exclusion criteria are available in the Supplemental Material available online.
The final sample included 52 females with BPD, 55 females with current MDD, and 55 healthy females. Diagnostic groups were matched for age. The sample size slightly exceeds our a priori power analysis suggesting a sample size of 159 (Schulze et al., 2018). For demographic and clinical characteristics by group, see Table S1 in the Supplemental Material.
The study was performed in accordance with the World Medical Association Declaration of Helsinki. The ethics committee at Freie Universität Berlin approved the study protocol (67/2013; Amendment: 136/2017). Participants gave written informed consent and were reimbursed after participating. The study took place in Berlin, Germany, between January 2017 and June 2019.
Materials
Experience sampling of daily emotions and emotion regulation
Participants received a smartphone with a preinstalled experience-sampling application (movisensXS; movisens GmbH, Karlsruhe, Germany). The application was programmed to beep eight times a day for 7 consecutive days (56 beeps total). Beeps occurred pseudorandomly with a minimum delay of 45 min between beeps. Participants were allowed to postpone prompts three times by 15 min.
Following each prompt, participants were asked to indicate on a scale from 0 (not at all) to 6 (very much) how tense, depressed, anxious, angry, lonely, ashamed, cheerful, and happy they felt just before the prompt. Furthermore, participants indicated on a scale from 0 (never) to 6 (very often) how often they had used the following emotion-regulation strategies since the last beep: rumination, suppression, reappraisal, acceptance, distraction, and social sharing. For exact item formulations, which are based on suggestions by Heiy and Cheavens (2014), see the Supplemental Material. Participants received an extra incentive of 10€ for responding to more than 90% of prompts.
Compliance with this protocol was very good. Median response rates were 91.07% (interquartile range [IQR] = 10.48) in the BPD group, 92.86% (IQR = 8.93) in the MDD group, and 89.36% (IQR = 15.76%) in the healthy group.
Data analysis
To examine our hypotheses, we estimated Bayesian hierarchical models accounting for the three-level structure of the experience sampling data: prompts (Level 1) nested in days (Level 2) nested in persons (Level 3). We applied the R package brms (Bürkner, 2017), which is based on Stan (Carpenter et al., 2017) for all analyses, using noninformative priors. For the exact R code and all general model settings, see the Supplemental Material. We computed three types of models.
First, we examined between-groups differences in the frequency of employing a particular emotion-regulation strategy. We computed a separate model for each strategy with the intensity rating for the respective strategy at time t as dependent variable. At Level 1, we entered the mean intensity rating of all other strategies at time t, controlling for differences in overall strategy employment: 1

There were no Level 2 predictors:


At Level 3, we included diagnostic group as main predictor of interest:


with mean-zero random effects µ0ji, ξ0i, and ξ1i. The residuals etji were modeled by an autoregressive process of order 1 (cor(etji, e(t−1)ji) = ρ) with a standard deviation sd(etji) = σ i modeled as σ i = exp(δ0 + δ1 × Group i ); we allowed a serial correlation of successive prompts within days and modeled the within-groups variance to vary across groups.
Second, we examined whether individuals in each group preferred certain strategies over others. For this purpose, we computed one model with the intensity rating of any strategy as dependent variable. At Level 1, we modeled how type of strategy predicts the intensity rating:

There were no Level 2 predictors:


At Level 3, we modeled how diagnostic group interacted with strategy type to predict the intensity rating:


with mean-zero random effects µ0ji, µ1ji, ξ0i, and ξ1i. Again, the residuals etsji were modeled by an autoregressive process of order 1 (cor(etji, e(t-1)ji) = ρ) with a standard deviation sd(etsji) = σ tsji modeled as σ tsji = exp(δ0 + δ1 × Group i + δ2 × Strategy tsji + δ3 × Group i × Strategy tsji ).
Third, we examined group differences in the effect of the regulation strategies on individuals’ emotions. For this purpose, we computed an emotional-valence score by subtracting the mean across all negative-emotion items from the mean across all positive-emotion items. Values can range from −6 to 6. Negative values reflect negative emotional valence, and positive values reflect positive emotional valence. The scale showed excellent internal consistency, between-persons ω = 0.93 (95% credible interval [CI] = [0.91, 0.95]). We preferred this valence score over using negative- and positive-emotion scores because our healthy individuals showed floor effects in negative emotions (Ebner-Priemer et al., 2007). 2
To examine the effect of a specific regulation strategy on the change in emotional valence from time t − 1 to time t, we computed one model with the valence score at time t as a dependent variable. At Level 1, we entered the lagged person-centered valence score (i.e., from time t − 1) and the use of each of the six strategies between time t − 1 and time t (as assessed at time t) as predictors. We entered the time difference between successive experience sampling prompts as additional predictor to control for varying time intervals.
where f is a flexible, two-dimensional, nonlinear function realized via a thin-plate spline (Wood, 2003).
There were no Level 2 predictors:



At Level 3, we predicted how group interacted with each strategy to predict emotional valence:



with mean-zero random effects µ0ji, ξ0i, ξsi, and ξ7i. The residuals etji were modeled by an autoregressive process of order 1(cor(etji, e(t-1)ji) = ρ) with a standard deviation sd(etsji) = σ tsji modeled as σ i = exp(δ0 + δ1 × Group i ).
We consider effects clearly different from zero if the estimate’s 95% CI does not include zero. For directed hypotheses, we estimated the posterior probability (PP) that the respective effect is in the expected direction. PP values range from 0 to 1, and higher values imply more support for the effect going into the expected direction.
Results
Employment of emotion-regulation strategies
Table 1 displays the estimated relative employment of each emotion-regulation strategy by group. Table 2 displays the statistics for all between- and within-groups contrasts described below.
Estimated Mean Employment of Each Affect-Regulation Strategy, Controlling for the Employment of All Other Strategies, by Group
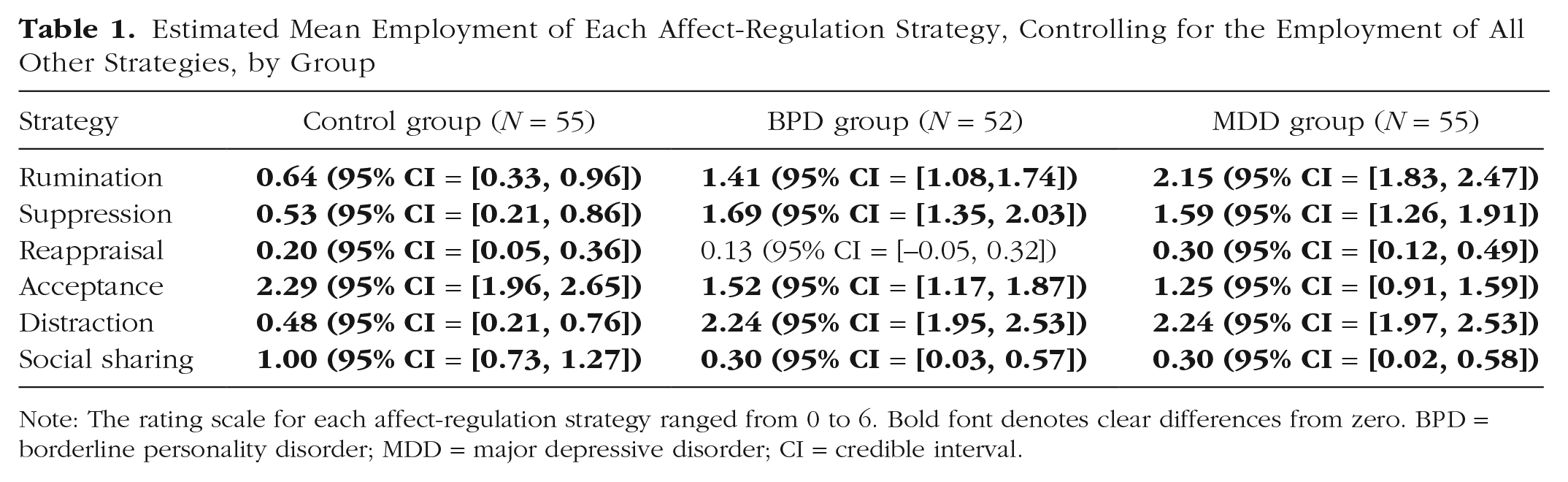
Note: The rating scale for each affect-regulation strategy ranged from 0 to 6. Bold font denotes clear differences from zero. BPD = borderline personality disorder; MDD = major depressive disorder; CI = credible interval.
Between- and Within-Groups Contrasts in Employing Each Affect-Regulation Strategy, Controlling for the Employment of All Other Strategies
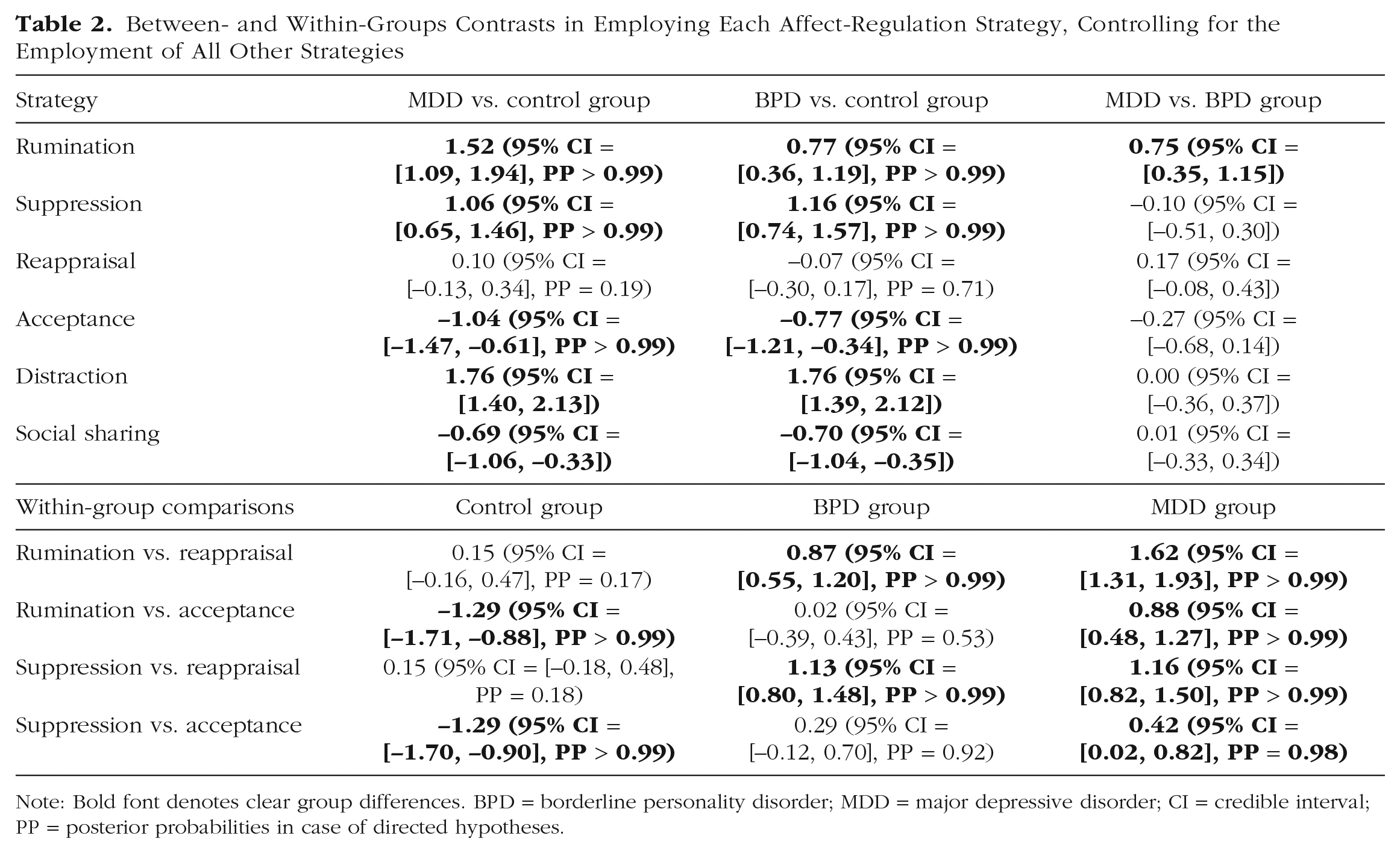
Note: Bold font denotes clear group differences. BPD = borderline personality disorder; MDD = major depressive disorder; CI = credible interval; PP = posterior probabilities in case of directed hypotheses.
Between-groups analyses
Note that results reflect group differences in the relative employment of each strategy accounting for group differences in overall strategy employment (for results on absolute numbers, see https://osf.io/vdrw7; for group differences in overall strategy endorsement, see the Supplemental Material).
Maladaptive strategies
As expected, both clinical groups ruminated clearly more often than healthy individuals. Depressed individuals ruminated even more often than individuals with BPD. As expected, both clinical groups suppressed their emotional expression clearly more often than healthy individuals. However, clinical groups did not differ in using expressive suppression.
Adaptive strategies
Note that there were no group differences in using cognitive reappraisal. As expected, both clinical groups accepted their feelings or an external situation clearly less often than healthy individuals; there were no clear differences between clinical groups. Individuals with BPD or MDD distracted themselves clearly more often than healthy individuals; there were no differences between clinical groups. Finally, individuals with BPD or MDD shared their experiences clearly less often than healthy individuals but, again, did not differ from each other.
Within-groups analyses
As expected, both clinical groups selected rumination and suppression clearly more often than they selected reappraisal. As expected, depressed individuals selected acceptance clearly less often than rumination or suppression. However, individuals with BPD selected acceptance to similar degrees as rumination or suppression. Unexpectedly, healthy individuals did not select reappraisal more often than rumination or suppression. However, they used acceptance clearly more often than rumination or suppression.
Effect of regulation strategies on subsequent emotions
Table 3 presents the estimated mean effect of each regulation strategy on individuals’ subsequent emotional valence. Table 4 displays the statistics for all between-groups contrasts described below. For descriptive values for all emotion items and scales by group, see the Supplemental Material.
Estimated Effect of Each Affect-Regulation Strategy on Affective Valence, a Controlling for the Effect of All Other Strategies, Across the Entire Sample and by Group
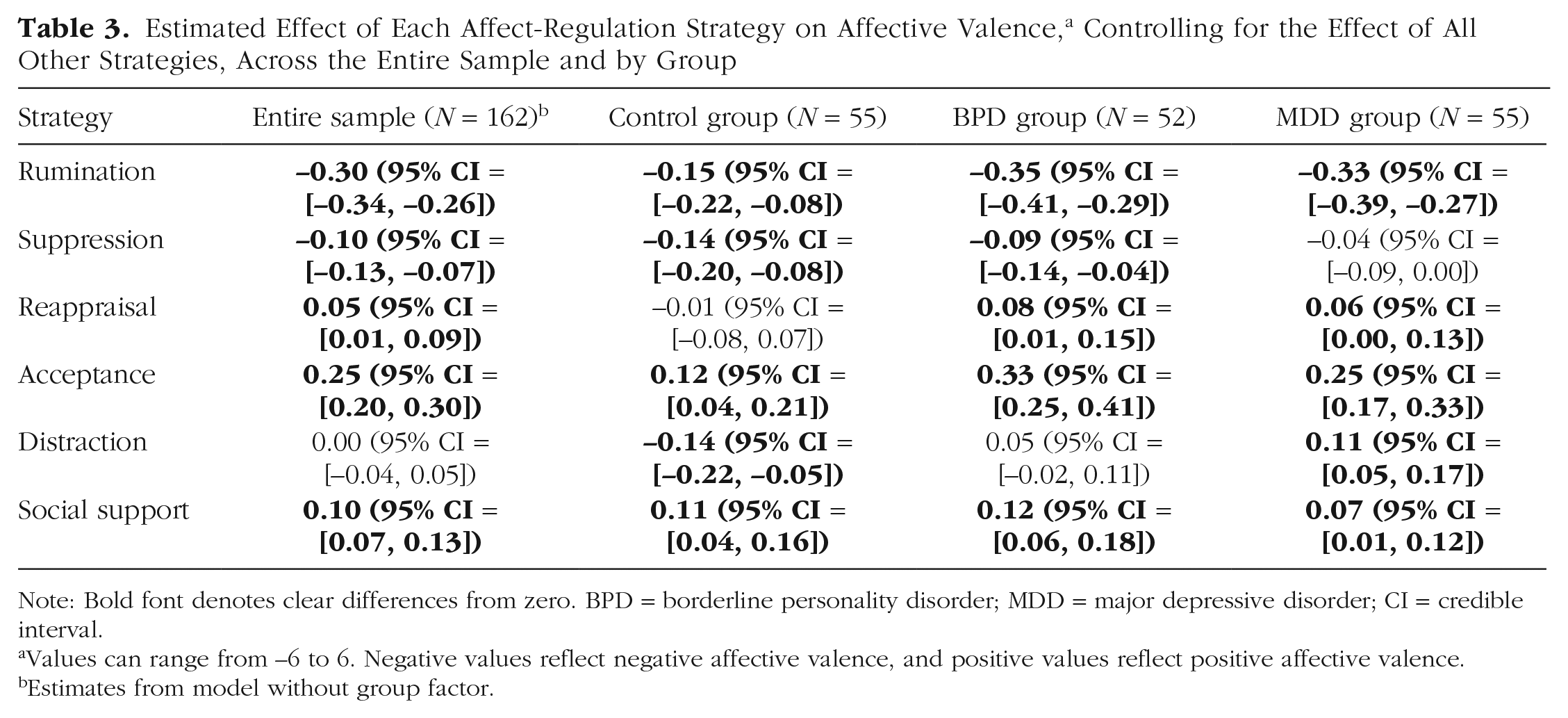
Note: Bold font denotes clear differences from zero. BPD = borderline personality disorder; MDD = major depressive disorder; CI = credible interval.
Values can range from −6 to 6. Negative values reflect negative affective valence, and positive values reflect positive affective valence.
Estimates from model without group factor.
Between-Groups Contrasts for the Estimated Effect of Each Regulation Strategy on Affective Valence, a Controlling for the Effect of All Other Strategies
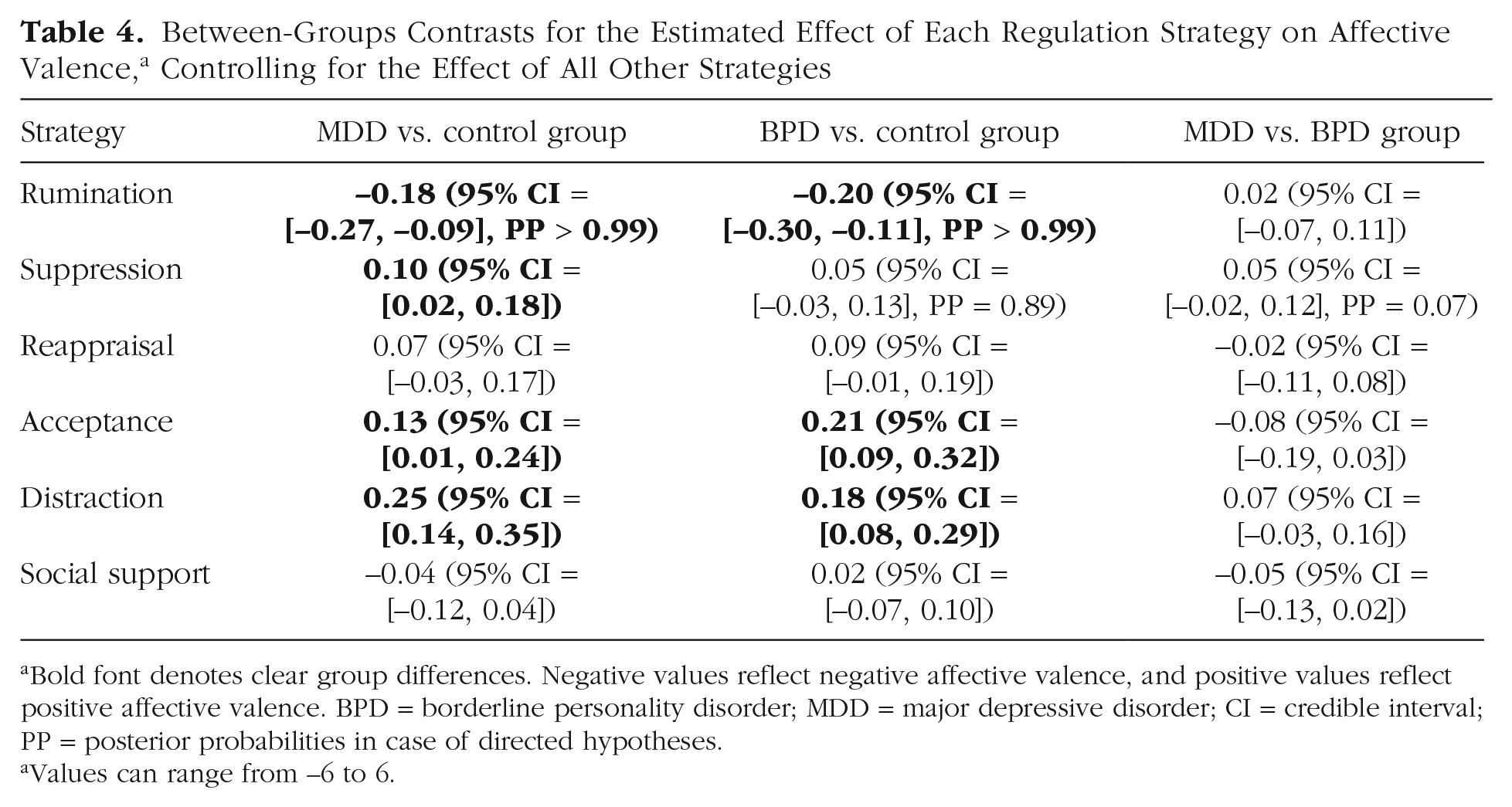
Bold font denotes clear group differences. Negative values reflect negative affective valence, and positive values reflect positive affective valence. BPD = borderline personality disorder; MDD = major depressive disorder; CI = credible interval; PP = posterior probabilities in case of directed hypotheses.
Values can range from −6 to 6.
Effect of maladaptive strategies
As expected, the effect of rumination on subsequent emotions was clearly more negative in individuals with BPD or MDD compared with healthy individuals but did not differ between clinical groups. The effect of suppression on subsequent emotions was less negative in depressed individuals than in healthy individuals. Unexpectedly, individuals with BPD also showed a negative effect of suppression on subsequent emotions, but there were no differences to the other two groups.
Effect of adaptive strategies
The relatively small positive effect of reappraisal on subsequent emotions did not differ between groups. The positive effect of acceptance on emotions was clearly more pronounced in individuals with BPD or MDD than in healthy individuals but did not differ between clinical groups. Distraction resulted in a clear negative effect on subsequent emotions in healthy individuals but led to an amelioration of emotional valence in depressed individuals. Individuals with BPD experienced no clear effect of distraction on their emotions. Accordingly, there were clear differences in the effect of distraction between the clinical groups and the control group but no clear difference between the two clinical groups. Individuals who shared their experiences with others experienced an amelioration of their emotional valence; there were no group differences in this effect.
Discussion
The present results demonstrate that both currently depressed individuals and individuals with BPD show an unfavorable pattern of overusing maladaptive emotion-regulation strategies in their daily lives. Three findings regarding the selection of regulation strategies are worth highlighting.
First, depressed individuals ruminated clearly more often than individuals with BPD. The present study thus clarifies the mixed findings on rumination from past studies (Abela et al., 2003; Sauer et al., 2016) by including only individuals with BPD without comorbid current MDD. The uniquely high levels of rumination in depressed individuals correspond with an extensive body of research identifying rumination as a key mechanism in the development of major depression (Nolen-Hoeksema 2000).
Second, there were no group differences in using reappraisal. This is in contrast to previous studies showing that individuals with MDD or BPD retrospectively report less habitual use of reappraisal than healthy individuals (Daros & Williams, 2019; Visted et al., 2018). In our study, reappraisal was one of the regulation strategies employed the least often in all groups. Thus, the missing between-groups difference might be driven by the fact that healthy individuals rarely used reappraisal. This may be a mere sample effect. Otherwise, healthy individuals may report higher rates of reappraisal only when retrospectively asked about their habitual use but may not actually employ reappraisal that often in their daily lives (see also Heiy & Cheavens, 2014). Further experience-sampling studies are needed to clarify this question.
Third, both clinical groups used distraction extensively and considerably more often than healthy individuals. Likewise, another experience-sampling study in a nonclinical sample found depressive symptoms to be associated with increased use of distraction (Panaite et al., 2019). Past experimental or questionnaire studies found that depressed individuals select distraction less or as often as healthy individuals (Liu & Thompson, 2017). Our results indicate that individuals with MDD or BPD distract themselves more often than they remember retrospectively. Our study demonstrated that distraction is effective in improving depressed individuals’ emotional states but has no effect in individuals with BDP.
Effectiveness of regulation strategies
Currently depressed individuals and individuals with BPD were able to benefit from adaptive regulation strategies if they did select them. These positive effects on emotions were either comparable with (reappraisal, social sharing) or even greater (acceptance) than in healthy individuals. Remarkably, most strategies showing a positive effect on emotions were those employed relatively less often by individuals with MDD or BPD. Thus, despite their intact ability to effectively implement adaptive regulation strategies, both clinical groups did not primarily select them.
We did not replicate findings indicating a positive effect of suppression in BPD. However, the only study demonstrating a positive effect of instructed suppression on affect in clinical BPD instructed patients to suppress their emotional experience (Chapman et al., 2016). We assessed suppression of emotional expressions. Past findings on the effect of expressive suppression in BPD have been mixed. Svaldi, Dorn, Matthies, and Philipsen (2012) found no effect of expressive suppression on negative emotions in BPD. Evans and colleagues (2013) found that suppressing the experience and expression of emotions showed a positive effect on affect independent of BPD symptom severity. Future research will benefit from differentiating more clearly between the suppression of emotional experiences and emotional expressions.
Finally, this study demonstrated that the detrimental effect of rumination on emotions was more pronounced in both clinical groups than in healthy individuals. This is in line with our expectations and in accordance with findings suggesting that rumination exerts only negative consequences in individuals already in a negative mood (Nolen-Hoeksema et al., 2008), as can be assumed for individuals with MDD or BPD.
Limitations
The present study included only female participants, limiting the generalizability of our results. The exclusion of men was a recruitment decision: only a few men with BPD present in treatment facilities and/or often suffer from comorbid substance dependency, which was an exclusion criterion in this study. Given similar prevalence rates for BPD in men and women (Grant et al., 2008), it will be important to include men in future studies to examine potential gender differences in emotion regulation. Furthermore, we used single items to assess each regulation strategy. Single-item measures are generally thought to be inferior to multiitem measures in terms of reliability and validity. However, single-item measures reduce the burden on participants and prevent biases because of fatigue, especially in designs with dense sampling schemes. Indeed, a recent study demonstrated good predictive validity of single-item experience-sampling measures in a clinical sample (Song et al., 2022). Last, the duration of experience sampling was restricted to 7 days.
Summary and outlook
This is the first study directly comparing the employment and effectiveness of six emotion-regulation strategies in the daily lives of healthy individuals and two carefully diagnosed clinical samples (i.e., individuals with MDD or BPD). Results demonstrated that both clinical groups showed a marked pattern of maladaptive strategy selection, with depressed individuals ruminating even more often than individuals with BPD. Remarkably, both clinical groups successfully implemented adaptive strategies if selected. It remains an exciting question why individuals with MDD or BPD show a clear preference for emotion-regulation strategies that actually increase their negative emotions. Possibly, they are not able to implement helpful strategies in moments of intense negative emotions. Alternatively, they may hold erroneous beliefs about positive effects of these strategies. It will be intriguing for future research to examine this question.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026231160709 – Supplemental material for Daily Emotion Regulation in Major Depression and Borderline Personality Disorder
Supplemental material, sj-docx-1-cpx-10.1177_21677026231160709 for Daily Emotion Regulation in Major Depression and Borderline Personality Disorder by Ulrike Zetsche, Paul-Christian Bürkner, Julian Bohländer, Babette Renneberg, Stefan Roepke and Lars Schulze in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Aidan G. C. Wright
Editor: Jennifer L. Tackett
Author Contributions
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.