
Abstract
Emergent phenomena (EP)—sudden unusual mental or somatic experiences—are surprisingly widespread. Although EP often lead to positive impacts on well-being, they are sometimes followed by intense suffering. We examine potential risk factors and protective factors for EP and related suffering using logistic regression on general-population survey data (n = 3,133). The four strongest risk factors are having attempted divine, magical, or occult practices; past psychedelic use; contemplation of mysteries; and total lifetime meditation practice outside retreats. Further risk factors for EP alone include several traditional meditation techniques and spiritually powerful or traumatic childbirth experience. Prayer is a protective factor. Other risk and protective factors for EP and related suffering include past diagnosis of mental illness and several personal characteristics. These results provide implicit guidance for managing the risks of EP and suggesting contraindications for individuals who wish to have a spiritual or meditative practice without EP.
Mindfulness meditation, drawn from ancient contemplative traditions, has developed a reputation for efficacy in clinical settings; however, it may also be associated with the emergence of certain types of sudden unusual mental or somatic experiences. The commencement of its clinical adoption can be traced to a seminal study of chronic-pain patients who had not responded to pharmaceutical treatment, but reported significantly less suffering after completing a 10-week mindfulness-based program (Kabat-Zinn, 1982). Both ancient mindfulness practices and more recently developed derivatives have since gained considerable clinical popularity (Barnes et al., 2008; Clarke et al., 2018; Simonsson et al., 2021) because of their perceived success in promoting general well-being and alleviating symptoms of stress, anxiety, and depression (Alejandre-Lara et al., 2022; Goldberg et al., 2018; Miller et al., 1995). Neuroimaging and brain stimulation have been used to explore the neurobiology of these positive effects of meditation, including the roles of self-awareness, attentional control, and emotion regulation (Abellaneda-Pérez et al., 2024; Sezer et al., 2022), and have informed theoretical accounts of how traditional descriptions of meditative phenomena can be reconciled with neurobiological descriptions of the brain and nervous system (Wright et al., 2023). Many clinicians now view mindfulness practices as a safe and economical way to improve a wide range of symptoms without the risk of drug dependence or unwanted side effects. Mindfulness and meditation practices are also becoming widespread in general populations. A 2017 survey found that 14.2% of U.S. adults reported using meditation, a threefold increase since 2012 (Clarke et al., 2018). Likewise, a 2018 study found that 15% of UK adults have reported learning mindfulness practices, including meditation (Simonsson et al., 2021).
Rather than simply being a temporary clinical intervention or straightforward well-being practice at home, mindfulness practices are potentially part of a broader process of meditative development that may have complex and transformational longitudinal effects (Galante et al., 2023). Among these effects are the emergence of sudden, unusual mental or somatic experiences, often interpreted as spiritual, mystical, energetic, or magical in nature, and characterized in the literature as emergent phenomenology or EP (Sandilands & Ingram, 2024; Wright et al., 2024).
EP are similar to but somewhat broader in scope than altered states of consciousness because they (a) do not assume a baseline against which alteration occurs; (b) often manifest as a fluid or evolving experience rather than being a rigid, stable state; and (c) may include somatic and mental elements and even the cessation of consciousness altogether (Sandilands & Ingram, 2024). The domain of EP thus encompasses the contextualized unfolding of unusual emergent physical and mental phenomena that have the potential for transformational and enduring impacts. This makes EP a particularly salient construct for studying the interplay between acute experiential episodes and their long-term psychological and existential implications.
In ancient contemplative traditions, most EP are treated as a type of phenomena that can be expected to occur at a various stages of meditative development rather than as isolated events with intrinsic, independent significance (Ingram, 2018; Sobhana, 1994). The lists of EP do vary between traditions, and phenomenological reports from individuals are extremely diverse (Sandilands & Ingram, 2024); however, a recent expert panel identified 10 general types of EP that empirically accounted for 95% of subjective reports in a large survey (Wright et al., 2024). These were, in order of occurrence, perceiving the world as a dream or cartoon, unitive experiences, ecstatic experiences, a strong sense of vivid brightness or clarity in perceptions, changes to perceived size, feelings of heat or electricity rising in the body, out-of-body experiences, perception of nonphysical lights, strobing of perceptions, and losing consciousness during a meditative or spiritual experience; for detailed question wording, see Wright et al. (2024).
EP last for varying durations and can be perceived positively or negatively at the time they occur. Traditional meditation manuals characterize EP as integral steps toward enduring liberating transformation with significant benefits for well-being (e.g., Galante et al., 2023; Sobhana, 1994); however, difficulties can arise when these phenomena are not integrated into an individual’s worldview or modes of perception, sometimes leading to significant distress that may even require clinical intervention (Grabovac, 2015). Although positively valenced EP typically result in positive outcomes and negatively valenced EP typically result in negative outcomes, this pattern can occasionally reverse. Such reversals are thought to reflect the complex psychological process of integration, in which meaning making and adaptation may moderate or mediate the eventual effect on well-being (Wright, 2024).
The potential for negative effects from mindfulness or other meditative practices was not prominent in the early literature, but recent studies have found that meditative practice is indeed associated with transient distress and other negative impacts at similar rates to other psychological interventions (Britton et al., 2021) and sometimes with unexpected challenging or difficult experiences (Francis et al., 2022). One review found the incidence of adverse events to be 8.3% in meditation studies (Farias et al., 2020), and another found that some mental distress is reported in almost all studies of meditation or mindfulness interventions (Taylor et al., 2022). Adverse effects, such as perceptual changes, fear, and distorted emotions or thoughts, have been observed in numerous meditators, ranging from 25% (Cebolla et al., 2017; Schlosser et al., 2019) to 63% in retreat settings (Shapiro, 1992). Despite evidence of adverse effects of mindfulness practices, four out of five of mindfulness-based stress-reduction randomized controlled trials did not include survey questions about any negative effects (Wong et al., 2018)
Although EP and subsequent difficulties in integrating such experiences are expected to sometimes occur in meditative development (Grabovac, 2015), they are also found in general populations. Recent surveys found up to 45% of general-population participants reported having experienced EP of the type detailed in meditation manuals, and that these were followed by a variety of outcomes, including no effect (30%), positive changes in well-being (40%), and, in some cases, negative changes in well-being (28%). Furthermore, 13% of all participants reported moderately intense or greater suffering following such events (Wright et al., 2024). This finding is surprising because it exceeds the proportion of the population who have practiced meditation, raising substantive questions of why such EP occur in general populations and why they sometimes lead to negative outcomes (i.e., suffering). As interest grows in deeper forms of contemplative engagement—including advanced meditative states and the developmental stages that unfold with sustained practice (Sacchet et al., 2024; Van Lutterveld et al., 2024; Yang, Chowdhury, et al., 2024; Yang, Sparby, et al., 2024)—it is important to understand how to maximize the safety of practitioners given the potential for EP and subsequent varied outcomes on well-being.
Certain influencing factors may increase or decrease the risk of experiencing EP. Meditation-practice histories seem most obviously likely to play a role. Individual practice (rather than in groups), longer durations of meditation sessions, and greater lifetime hours of practice may increase the likelihood of experiencing EP, although the impact of years of practice on adverse effects remains inconclusive (Cebolla et al., 2017; Goldberg et al., 2022; Shapiro, 1992). The type of meditation practice may also vary in likelihood of inducing emergent phenomena. Deconstructive practices, such as vipasanna/insight practices that observe sensations in fine detail, or focused-attention meditation, increase the chances of experiencing EP (Cebolla et al., 2017; Schlosser et al., 2019). Group practices in which meditators feel connected to others may offer buffering effects (Cebolla et al., 2017), although conversely, meditation retreats, despite being in a group setting, can be a risk factor because of silence and social isolation (Lindahl et al., 2017; Schlosser et al., 2019).
Aside from meditation practice, other aspects of personal history may be risk factors. Psychedelic drug use has been linked to subsequent experience of EP, and meditation experiences may also be enhanced through psychedelics (Azmoodeh et al., 2023; Lindahl et al., 2017; Singer et al., 2024). Research suggests that individuals with certain diagnosed mental-health issues, such as posttraumatic stress disorder (PTSD), substance dependence, and psychosis, may be more likely to experience adverse effects (Baer et al., 2019). Relationships within and beyond meditation communities may serve as potential risk factors or remedies, depending on the supportiveness and understanding of the relationships (Lindahl et al., 2017). Women across various traditions and backgrounds have expressed childbirth experiences in spiritual terms that are reminiscent of EP, such as a feeling of getting closer to God, a sense of transcendence, or spiritual transformation (Callister & Khalaf, 2010).
Personal characteristics may also be relevant to EP. There is evidence that males may be more susceptible to negative reactions to EP compared with females (Lomas et al., 2015; Schlosser et al., 2019), which may be due to a higher rate of poor emotion-regulation skills (Lomas et al., 2015). Personality, temperament, and worldview may similarly be potential remedies or risks (Lindahl et al., 2017). For example, religious participants may be less likely to experience unpleasant meditation-related experiences because they may be able to use their religious frame of reference to more easily integrate these effects into their worldview (Castillo, 1990). Healthy behaviors, such as proper sleep, diet, and exercise, may also be protective factors that reduce the risk of negative reactions to EP (Lindahl et al., 2017).
Whether an individual experiences EP or EP-related suffering could thus be contingent on a multitude of individual and sociocultural factors. However, to date, there is little evidence on exactly what factors might be associated with EP and subsequent suffering for general populations. In the present study, we therefore explore this question. We obtained data on three general-population samples from a recently completed study of the prevalence of EP (Wright et al., 2024). The survey data contain a rich set of potential covariates on past-practice histories, diagnosis of mental illness, trauma, psychedelic use, mystical practice, and childbirth experience, as well as demographic information and personal assessments of spirituality, religiosity, and everyday health. We applied logistic regression to explore which of these variables are significant risk or protective factors for the experience of EP and subsequent suffering. We focused on suffering because of its importance to public health but also because it is more precisely defined and measured than the more commonly experienced positive changes to well-being.
Transparency and Openness
Ethical approval was obtained from the Massey University Human Ethics Committee NOR 21/5. The study was not preregistered. The final study data will be available from the corresponding author on reasonable request. We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Method
Participants and procedures
The recruitment of participants and their demographic profile is thoroughly detailed in Wright et al. (2024). Three sources were drawn on: an online community (subscribers to a popular rationalist blog) and two commercial survey panels (UK Qualtrics panelists and U.S. MTurk workers). The selection of three diverse sampling frames and demonstrated sample representativeness compared to underlying populations mitigate the risk of response bias (Wright et al., 2024). The only substantive demographic skew compared with underlying populations was oversampling of the U.S. 35 to 54 age group and undersampling of U.S. Hispanic/Latino ethnicities in the MTurk data. However, MTurk was the smallest of the samples (n = 351) compared with the UK Qualtrics data (n = 1,130) and the rationalist-blog data (n = 1,654). The combined total sample was 3,135.
Detailed procedures are reported in Wright et al. (2024). These include obtaining ethical approval before fieldwork, seeking and obtaining permission to recruit, and restricting participation to adult participants. Participants were briefed with an information sheet, informed that participation was voluntary and anonymous, and provided with support resources before agreeing to participate in the survey.
Measures
The measures used were developed via a modified Delphi method from a panel of experts and then subject to multiple rounds of pretesting (Wright et al., 2024). Exact question wording varied slightly between surveys because minor emendations continued to be made to tailor wording to particular populations, adapt to the survey platform being used, or incorporate ongoing minor feedback on question content. The questionnaire included potential dependent variables on the experience of EP and related suffering and potential independent variables (or risk and protective factors) for these outcomes. The independent variables encompassed a range of questions on practice history and personal characteristics, including potential risk factors, self-assessments, and demographic covariates. Details of these items are as follows.
Experienced EP
The conceptualization of EP as “sudden unusual mental or somatic experiences often interpreted as spiritual, mystical, energetic, or magical in nature” cannot be directly applied in general-population survey questions. It relies on technical terms that are not widely understood (e.g., “somatic”) and risks introducing demand effects—influencing respondents to adjust their answers based on assumptions about the survey’s purpose—by explicitly stating the common interpretations of EP. The expert panel therefore operationalized EP through the question, “Have you ever (while not on mind-altering substances) had sudden unusual mental events that involved strange changes in perception or ecstatic pleasurable feelings?”; multiple selections were possible from response categories encompassing the most commonly reported forms of EP together with an “other” category (“Yes, something else”) and a “none” response (“No, I have never had such experiences”). We extracted a dichotomous measure from these questions on having experienced EP or not.
Experienced suffering
Respondents were also asked a series of questions on their well-being following the experience of EP and, in the case of a negative impact, the types of suffering they had experienced. They were then asked, “How intense was the worst of these experiences?” and invited to choose one response from not at all intense, mildly intense, moderately intense, severely intense, life-threateningly intense, and not applicable/prefer not to answer. From this question, we extracted a dichotomous measure of having experienced suffering (following the experience of EP) or not. We chose a cutoff of moderate or greater intensity suffering because this was deemed to be the point of clinical relevance. Note that having experienced suffering (following EP) is reported as an unconditional event—it is measured for the whole population, not just individuals who experienced EP.
These procedures ensured satisfactory statistical properties for the dependent variables, including equal intervals between categories and adequate data density for analysis.
Practice history
Practice-history variables included two multiple-response questions on types of practice, two questions on attendance at retreats (eliciting integer estimates), and two questions on practice outside of retreats (eliciting a response on an associated scale). As is usual with multiple-response questions, participant answers for the first two questions were converted to dichotomous measures for each response category. The full questions are as follows:
“What are your current types of spiritual or meditative practice?,” from which respondents could select any combination of six types of religious practice, yoga/tai-chi/qi-gong/martial-arts practice, other spiritual or meditative practice, or alternatively, none (“I do not have a current spiritual or meditative practice”). We considered excluding the yoga/tai-chi/qi-gong/martial-arts practice response category as a relatively poor fit for this question stem. Nevertheless, we decided to retain it because respondents could answer independently for each response category, so we could assess the performance of this item separately. In the end, none of the response categories for this question showed significant parameter estimates in our models, making our concern about item suitability moot.
“In your current practice, which specific spiritual or meditative techniques your current practice, which do you use?,” from which respondents could select any combination of 12 techniques, including “other specific techniques.”
“Over your whole lifetime, how many spiritual or meditation retreats have you previously attended lasting one full day or more?”; respondents were first asked to specify number of retreats and then to specify total number of days.
“Over your whole lifetime, how many hours of spiritual or meditative practice have you previously done, outside of retreats?” and “Over your whole lifetime, how many hours of formal physical breath or movement-based practice have you done, outside of retreats.” Here, respondents were offered a choice from a 5-point scale with responses (1) none, (2) up to 100 hr, (3) 101 to 500 hr, (4) 501 to 1,000 hr, and (5) more than 1,000 hr. Although these data are not strictly equal intervals, the response categories have face validity in discriminating between the different levels of nonpractitioner, novice, intermediate, advanced-intermediate, and expert practice. We therefore treat these as metric variables.
Personal characteristics
For other personal characteristics, dichotomous features were extracted from the following questions:
“Have you ever taken psychedelic drugs (such as LSD, magic mushrooms, DMT, peyote, or ayahuasca) and then experienced a lasting and significant change to your emotions, habits, sense of identity, or perception of life?” This included a variety of response categories, including “No, I have never taken psychedelic drugs.”
“Have you ever attempted formal divine, magical, or occult practices, such as healing prayer, banishing, spirit contact, mind reading, clairvoyance, divination, astral travel, spell casting, or telekinesis?” Again, this included a variety of response categories, including “No – I have never practiced or attempted such practices.”
“Has a physician or mental health professional ever diagnosed you as having a mental illness, including anxiety disorder, bipolar disorder, depression, psychosis, schizophrenia or similar, OR have you ever been prescribed medication for mental illness?”
“If you have given birth, please indicate whether . . . ”; response categories included “I have had a spiritually powerful childbirth experience” and “I have had a traumatic childbirth experience.” These two categories were combined because of low sampling proportions.
“Have you served in a military, medical or other dangerous role, or been in a life situation, that subjected you to extreme physical danger, trauma, or combat stress.”
Participants also made self-assessments of religiosity, mental health, functioning, physical health, adjustment, and spirituality on 7-point agree-disagree scales (1 = strongly agree, 7 = strongly disagree). These were included as metric variables. The wording was: “Please indicate your agreement with each of the following statements . . . ”
“I consider myself a religious person”
“I am mentally healthy”
“I am physically healthy”
“I function well in everyday life”
“I consider myself a well-adjusted person”
“I consider myself a spiritual person”
Demographics
Demographic covariates included questions on gender, year of birth, and ethnicity. Derived age was extracted by subtracting self-reported year of birth from year of survey plus one. Gender and ethnicity were asked as multiple-choice questions, and these were again converted into dichotomies for each answer category.
Data analysis
Data preprocessing
Although a cleaned data set was provided from prior research, the variables extracted for the present study had not previously been analyzed, so additional data preprocessing was required. A small number of missing values were replaced to enable all cases to be retained for further analysis. For dichotomous measures, missing values were due to differences in skip logic between survey implementations and were replaced with zero. For the six 7-point scale items, 22 missing values were replaced with the scale midpoint (value of 4). For derived age, 28 missing values were replaced with the average age of participants (value of 42). Seven extreme values (500+) were detected for number of retreats and days on retreat. Although these values were not necessarily implausible, two cases showed inconsistencies between these two variables and so were excluded from further analysis, reducing total sample size to 3,133.
Variables that had a single value accounting for more than 95% of cases were classified as sparse predictors and dropped from the models to minimize the risk of parameter instability. For some multiple-response categories, one category was dropped to ensure the independence of the other variables (e.g., “I do not currently have a spiritual or meditative practice,” male gender, White ethnicity). The results for the retained categories can be interpreted as a comparison with the category dropped from the analysis.
The rationalist-blog survey contained some additional response categories for spiritual and meditative practices, and the Qualtrics survey contained fewer possible responses for ethnicity. To enable data pooling across surveys, these minor mismatches were addressed by combining excess response categories into the “other” response category on the same question. This procedure was also applied to sparse predictors in multiple-response questions, incorporating answers into the “other” response category (or a combined category in the case of childbirth) before each sparse predictor was dropped. Finally, dichotomous variables were added for MTurk and Qualtrics response to account for differences in level between the different populations in the pooled data.
Analysis
Multicollinearity and autocorrelation were assessed through bivariate correlations and from tolerance, variance inflation factors (VIFs), and Durbin-Watson statistics obtained through multiple regression. All bivariate correlations were below the cutoff of r = .8. Some correlations were above r = .7; however, collinearity diagnostics indicated acceptable levels for tolerance and VIF, so all variables were retained for the final analysis. A Durbin-Watson value of 2.047 indicated that autocorrelation was not significant in the data. For descriptive results and collinearity statistics for the final list of included variables, see Table 1.
Variables Used in Logistic Regression

1 = none, 2 = < 100 hr, 3 = 100–500 hr, 4 = 501–1,000 hr, 5 = > 1,000 hr.
1 = strongly agree, 7 = strongly disagree.
We applied binary logistic regression to these variables to identify the association between possible risk and protective factors and the dependent variables of having experienced EP and having experienced suffering. Both data preprocessing and logistic regression were undertaken in IBM SPSS (Version 29.0.2.0).
Results
Experienced EP
For having experienced EP, binary logistic regression with independent variables showed significant improvement over the no-variable model, χ2(36) = 901, p < .001. The regression fit the data (Hosmer-Lemeshow p = .09); Cox and Snell R2 = .25 and Nagelkerke R2 = .33, indicating a moderate effect. Table 2 reports results for parameters that were significant at the α = .05 level. For full results, see the supplementary material.
Variables Associated With Having Experienced Emergent Phenomenology

In Table 2, the Exp(B), or the exponent of the regression B values, indicates the percentage change in the odds ratio of having experienced EP given a 1-unit change to the reported variable. For dichotomies, the Exp(B) shows the percentage change in odds ratio for satisfying that condition; for integer or scale values, the Exp(B) shows the percentage change in the odds ratio for each incremental unit measured.
Based on the Exp(B) values, the principal risk factors associated with having experienced EP were attempted divine, magical, or occult practices; psychedelic use; and a variety of individual practice techniques. The scale variables breath- or movement-based practices and spiritual or meditative-based practice outside retreats also increased risks substantively for each scale point. Prayer represented a protective factor against EP.
Nonpractice risk factors mostly showed smaller effects; the largest effect was from traumatic or spiritually powerful childbirth experience, other ethnicity, past diagnosis of mental illness, and disagreement that “I consider myself a well-adjusted person.” Protective factors included disagreement that “I consider myself a spiritual person,” Asian ethnicity, and derived age.
The base rate of occurrence without considering independent variables was lower than the population average. Lower levels of EP were also found among Qualtrics and MTurk participants than among the rationalist-blog participants.
Experienced suffering
For having experienced suffering following EP, binary logistic regression with independent variables also showed significant improvement over the no-variable model, χ2(36) = 591, p < .001. The regression fit the data (Hosmer-Lemeshow p = 0.39); Cox and Snell R2 = .17, and Nagelkerke R2 = .32, indicating a moderate effect. Table 3 reports results for parameters significant at the α = .05 level. For full results, see the supplementary material.
Variables Associated With Having Experienced Suffering Following Emergent Phenomenology

The results indicate that the principal risk factors for having experienced suffering following EP were attempted divine, magical, or occult practices; psychedelic use; contemplation of mysteries; and spiritual or meditative practice outside retreats.
Nonpractice risk factors were mostly smaller effects; the largest effect was from traumatic or spiritually powerful childbirth experience, followed by other ethnicity (not White or Asian), past diagnosis of mental illness, and disagreement that “I am mentally healthy.” Protective factors included disagreement that “I consider myself a spiritual person” and derived age.
The base rate of occurrence without considering the independent variables was much lower than the population average. Compared with the rationalist-blog participants, higher levels of having experienced suffering were found among the Qualtrics participants, and lower levels of having experienced suffering were found among the MTurk participants.
Full results are summarized in the Figure 1. For self-assessed personal characteristics (1 = strongly agree), wording and direction of effects are reversed for ease of interpretation.
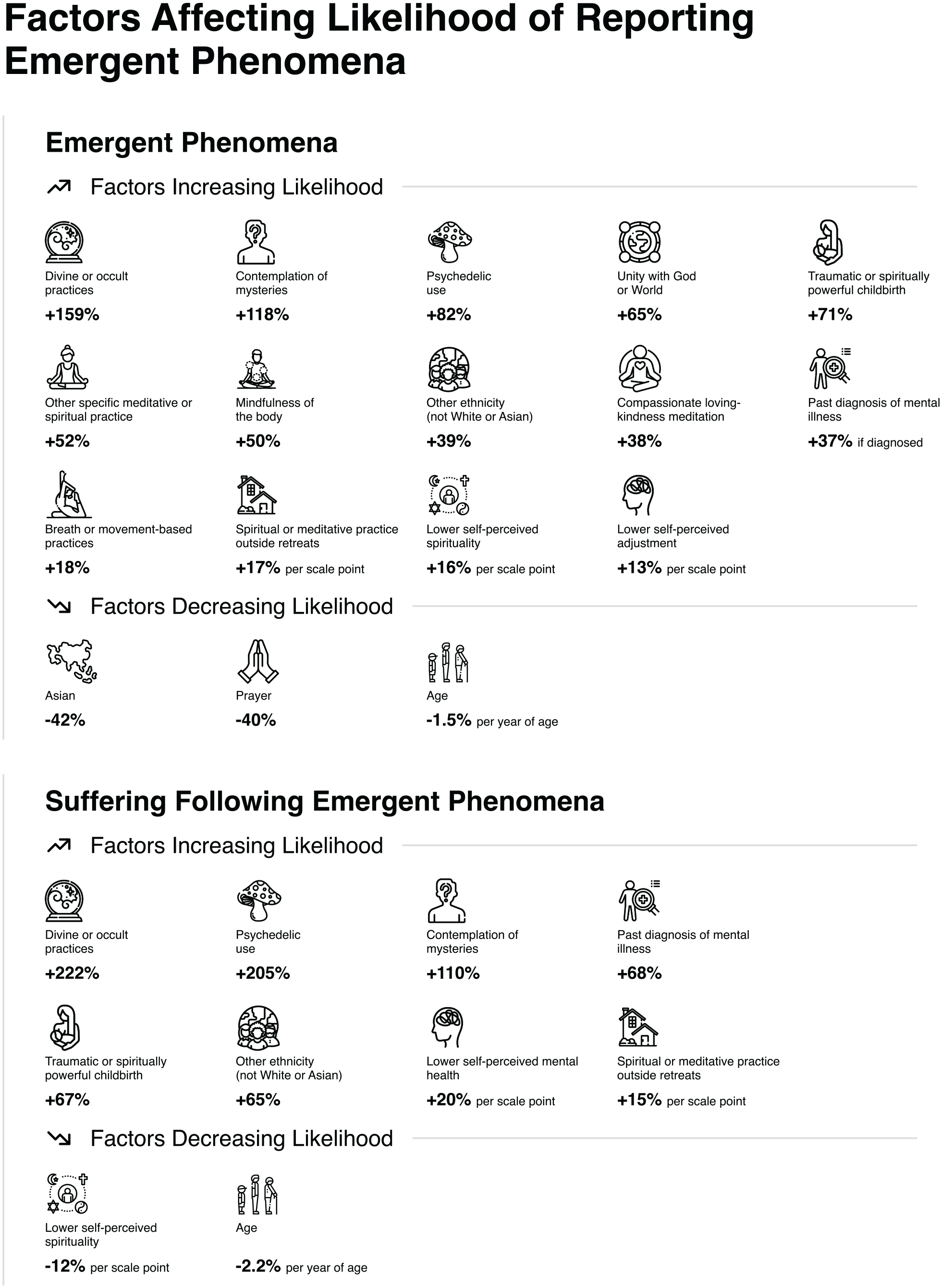
Infographic of significant risk and protective factors. For self-assessed personal characteristics (1 = strongly agree), wording and direction of effects are reversed for ease of interpretation.
Discussion
The results show that a moderate amount of the variation in having experienced EP and having experienced suffering following EP can be explained by practice histories and personal characteristics. The effects of practice-history variables generally have greater influence than the effects of personal characteristics; however, the precise mix of variables and effects varies between the two types of events.
Quite a wide range of meditation-related practices are detectable as risk factors for having experienced EP. The practice of prayer is similarly detectable as a protective factor. Thus, substituting mindfulness-related practices for prayer is likely to lead to an increase in the occurrence of EP. Four specific practice-history factors show particularly large increases in risk: having attempted divine, occult, or magical practices; past psychedelic use; following the practice contemplation of mysteries; and simply having done more spiritual or meditative practice outside retreats. Meditators should proceed with caution when employing combinations of practices that have been identified as risk factors for EP. If the objective of the practitioner is to experience EP, these could be seen as particularly empowering factors, although it may be wise to practice them under supervision of an experienced teacher or spiritual community familiar with the role of EP in meditation practice. Conversely, if the practitioner does not want to experience EP, then risk factors identified above should be avoided in favor of prayer.
Personal characteristics are risk factors to a degree that might reasonably be expected, with past diagnosis of mental illness, self-assessed poorer adjustment, and self-assessed spirituality increasing the risks of having experienced EP. Other ethnicity and traumatic or spiritually powerful childbirth are also risk factors, whereas Asian ethnicity is a protective factor. These personal characteristics may be useful interpretive aids in clinical settings to both help assess the risks of EP based on patient characteristics and consider whether EP is a likely explanation for patients presenting with clinically relevant suffering. Derived age (i.e., older age) is also a protective factor, but this variable should be interpreted with caution because it may be confounded by cohort effects associated with the growth of meditation and mindfulness-related practices in recent decades.
Turning to consider having experienced suffering following EP, we found the risk and protective factors are somewhat different. Here, we find that only four practice-history factors continue to have detectable effects: having attempted divine, magical, or occult practices; past psychedelic use; following the practice of contemplation of mysteries; and larger amounts of spiritual or meditative practice outside retreats. For personal characteristics, the effects found are similar to those for having experienced EP, except that self-assessed mental health replaces self-assessed adjustment as a risk factor and Asian ethnicity is no longer a protective factor.
A substantive conclusion is that although the spread of standard mindfulness, meditation, and related practices increase the risks of having experienced EP, they do not increase the risks of having experienced suffering following EP. Rather, a specific set of practices emerges as principal risk factors for both having experienced EP and more importantly having experienced subsequent suffering. Three of these practices involve deliberate attempts to distort ordinary perceptions of or relationships to reality, that is, having attempted divine, occult, or magical practices; past psychedelic use; and following the practice of contemplation of mysteries. The fourth, spiritual or meditative practice outside retreats, provides a measure of the total dose of practice in a nonsupervised setting. The implications of these findings are straightforward: practitioners should be wary of engaging in deliberate distortions of reality or high doses of spiritual or meditative practice because these factors are associated with having experienced suffering following EP.
Conversely, traditional mindfulness and meditative experiences, including breath- or movement-based practices, are not detectably associated with having experienced suffering, other than through increasing the total dose of spiritual or meditative practice. These techniques may therefore be considered relatively safe if undertaken in isolation from the riskier practices, and when practiced by individuals whose personal characteristics do not include other risk factors.
The 205% increase in risk of EP-related suffering associated with psychedelic use is a particularly notable result given increasing attention being paid to the use of psychedelics as treatments for various psychological disorders, such as PTSD and depression. Our findings imply that there may be long-term risks of suffering associated with psychedelic use, and this ought to be considered in developing treatment regimens and obtaining informed consent from participants. However, the present research does not distinguish between different types of psychedelics, so work is clearly needed not only to confirm or reject our preliminary result but also to determine whether it applies to all psychoactive substances or only a subset.
The experience of EP-related suffering may nonetheless be welcomed by some practitioners as indicative of progression on the path of insight, the development sequence of the Buddhist meditation practices from which mindfulness-based interventions are drawn (Grabovac, 2015). Meditation teachers may regard EP-related suffering as a prerequisite for the positive transformational changes sought from meditative endpoints (Galante et al., 2023), so blanket judgments about the suitability of individual practices are not easily made. Rather, the judgement ought to be contingent on the objective of the practice and the resilience of the practitioner. One implication is that research on the effects of psychedelics could usefully include not just their role in clinical treatments or the longer-term risk of EP-related suffering but also their potential to promote positive-changes models of meditative development (Galante et al., 2023).
However, positive changes in meditative development are less well defined than EP-related suffering and so are more difficult to measure. Advanced meditators may believe they can precisely define such positive changes to well-being; however, the language they use (e.g., “path,” “cessation,” “fetters,” “relinquishment”) is typically specific to their particular frame of reference. It would be useful to translate traditional accounts of positive transformation arising from meditation and meditative endpoints into objective phenomenological language, to enable empirical research on the occurrence of positive changes to well-being following the experience of EP (Sacchet et al., 2024; Sparby & Sacchet, 2022, 2024; Wright et al., 2023).
The results also indicate that EP and subsequent suffering will occur at different rates in different circumstances. For individuals operating in Asian contexts, with older meditators, who engage in prayer but avoid reality-distorting practices, the risk of having experienced or observed EP and related suffering is much lower. Conversely, for individuals operating in a non-Asian context, with younger meditators, eschewing prayer in favor of reality-distorting practices, there is much greater risk of having experienced or observed EP and related suffering. Should debates on these matters arise from personal experience and anecdotal observation, it is possible that very different conclusions might reasonably be reached simply because of the different contexts experienced by different individuals. This may be an explanation for some disputes between experts (e.g., Anālayo, 2020). Such possibilities emphasize the importance of rigorous empirical investigation of these phenomena rather than reliance on arguments from anecdotal experience (Sacchet et al., 2024).
The variety of nonsignificant effects is also rather surprising. None of the variables measuring current types of religious meditative or spiritual practice have a detectable effect on the outcome variables. Rather, it is the specific practice techniques that show the effects (e.g., prayer rather than Christian practice and mindfulness of the body rather than Buddhism). This finding invites further research on the interplay between religiosity and EP. Because EP are well known in many religious traditions, it would be useful to inventory the actual practice techniques used to see if this reveals commonalities overlooked by attributing outcomes to membership of a particular denomination.
Variables measuring attendance at retreats did not have a detectable effect, whereas variables measuring practice outside retreats did have detectable and indeed quite strong effects. This indicates retreats may be safer environments for individuals who do not want to experience EP or EP-related suffering but also surprisingly ineffective for individuals who wish to pursue the path of insight outlined in the meditation manuals, given that the experience of EP and exposure to the risks of EP-related suffering is normally seen a prerequisite for liberating insights (Sobhana, 1994). For researchers and practitioners who believe retreat participation promotes meditative development, this null result may be surprising. Individuals who do wish to pursue the path of insight may therefore be advised to employ a variety of individual practice techniques at high dose outside a retreat setting, while being mindful of the psychological risks that this may involve.
Limitations and future research
Further investigation is needed into the reasons for the relative efficacy of retreat and nonretreat practice. One approach could be to gather phenomenological accounts of meditative experiences in each context, either from direct interviewing of meditators or through content analysis from published sources, and to analyze these to determine similarities and differences in EP experienced in each setting, and the extent to which these consistently manifest the phenomenology expected from meditation manuals (Sparby & Sacchet, 2022, 2024). An alternative approach would be to use meditation theory to propose and test explanations for differences between retreat and nonretreat settings. For example, it could be that engaging in more diverse practices better achieves the objective of freeing up the default chain of perceptual processing that meditation seeks to reshape, or alternatively that excessive focus on a particular stage of meditative development is counterproductive because it establishes new ingrained default modes of perception (Galante et al., 2023; Sobhana, 1994; Wright et al., 2023).
Turning to methodological issues, future research could consider the possibility of interactions in the data, including moderating effects (e.g., particular practices being complementary) or mediating effects (e.g., the effects of religion being mediated by practice technique). The present exploratory data sets have not been designed for analysis of interactions, nor is the theory on these matters particularly well developed. Further research could aim to develop a psychometric instrument grounded in theory and capable of investigating interactions in a systematic manner, including through longitudinal measurement. This is no small task because many issues will need to be considered, including appropriate theory to inform instrument development, the type of psychometric scales to be developed, and the most important interactions to study. The results of the present study may help to set priorities for this future work.
A related methodological problem is to disentangle the casual pathways relating the valence of EP to changes to well-being. As noted earlier, this relationship is moderated or mediated by unobserved factors related to how the individual integrates the experience of EP into their worldview and modes of perception. Future research could develop models for this process of integration, hypothesize the underlying factors and relationships, and then undertake formal tests of these effects. A complication is that changes to well-being usually take time to fully manifest, so research in this area may require the use of moderated-mediation hazard models rather than cross-sectional analysis, requiring data from large cohort studies.
The present research does not differentiate between individual EP. Conceptually, individual EP are idiosyncratic examples of a general type of experience. Thus, for current purposes, it is more appropriate to model EP in aggregate, as a potential precursor to clinically relevant suffering, rather than to investigate individual EP. Given that individual EP occur at sampling fractions ranging from 2% to 17% of the population (Wright et al., 2024), many are too sparse for use as separate dependent variables and aggregation therefore maximizes the information available for statistical analysis. Nonetheless, it may be interesting to explore risk factors for the more frequently occurring individual EP in future research.
Ongoing development of variable sets and question phrasing would be useful. There are likely omitted variables that could increase the explanatory abilities of the models. Identifying these would require additional research to better understand what other risk and protective factors that may be at play. Similarly, because many current variables were derived indirectly from questions on related topics, it would be useful to revise these items to capture the intended constructs directly. This would streamline measurement and facilitate more extensive fieldwork through deployment of a more efficient instrument.
Finally, because the present work is cross-sectional in nature, relying on respondent recall, it is difficult to attribute causation or rule out the possibility that third factors are responsible for the observed relationships. Ideally, cohort studies should be used to track the occurrence of EP and related positive and negative transformations over participants’ lifetimes. Alternatively, for cases in which randomized trials of interventions such as the use of MDMA or psilocybin are taking place, the study designs could be amended to allow longitudinal follow-up of the factors and outcomes observed in this study.
Notwithstanding the possibilities for further research, clear findings have emerged from the present work. Given the lack of prior research on risk factors for EP-related phenomena, it was unknown what this initial, exploratory study would discover. We found a clear set of risk and protective factors, some of which are quite surprising, and these risk and protective factors differ substantially between the two dependent variables: having experienced EP and having experienced EP-related suffering.
Notions of risk and protection nonetheless depend on personal contemplative goals, the meaning derived from EP, and expectation of the value of any resulting suffering. EP may come to be interpreted as ultimately growth-producing or somehow positive, with associated suffering seen to be integral to this change. To take an analogy, crying during psychotherapy may ultimately provide some sort of release or enhanced capacity for integrating past experiences, enabling personal growth. We leave these issues of the deeper meanings of EP and varied goals of practitioners as additional matters for future research.
Supplemental Material
sj-xlsx-1-cpx-10.1177_21677026251330250 – Supplemental material for Risk Factors for Emergence of Sudden Unusual Mental or Somatic Experiences and Subsequent Suffering
Supplemental material, sj-xlsx-1-cpx-10.1177_21677026251330250 for Risk Factors for Emergence of Sudden Unusual Mental or Somatic Experiences and Subsequent Suffering by Malcolm J. Wright, Vanessa L. Cha, Melissa R. Streifert, Daniel M. Ingram and Matthew D. Sacchet in Clinical Psychological Science
Footnotes
Acknowledgements
Artificial-intelligence tools were not used in this study.
Transparency
Action Editor: Vina Goghari
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.