
Abstract
Suicide is a public-health concern that has been linked to multiple biological, psychological, and social risk factors. Rural living is purported to be a unique risk for suicide for myriad reasons. Yet there are some concerns with rural suicidology, notably regarding defining and operationalizing “rural.” Furthermore, the last comprehensive review of rural suicide is approximately 10 years old. With this in mind, in the current review, we offer (a) a comprehensive and updated overview of the operationalization and variability of rural in rural suicidology and (b) a summary of differences in direct and indirect suicide factors between rural and nonrural regions and whether potential differences depend on how rural is operationalized. Results indicate a high degree of heterogeneity in defining rural, rendering conclusions about both direct and indirect rural suicide risks unclear. We therefore present a set of recommendations for rural suicidologists to apply to enhance the understanding of suicide and, ultimately, prevent death by suicide in rural regions.
Suicide is multifactorially influenced by both direct (e.g., suicidal ideation; previous attempts) and indirect suicide-related (e.g., hopelessness) factors, which is best understood through intersecting psychological (Gili et al., 2019; Goldston et al., 2009), biological (Ruderfer et al., 2020), and psychosocial (Cero et al., 2015; Van Orden et al., 2010) influences. Indeed, about 50% of people who die by suicide had a previously diagnosed psychological disorder (Stone et al., 2018). Perhaps the most robust and consistent predictor of suicidal ideations or behaviors (SIBs) are past SIBs, particularly past suicide attempts (Franklin et al., 2017; Ribeiro et al., 2015). However, even the most consistent correlates of suicide (e.g., past ideations) are only marginal predictors of later suicide attempts (Franklin et al., 2017), and predicting suicide continues to be challenging (Belsher et al., 2019). Despite the abundance of studies that link specific social, psychological, and biological factors to SIBs in isolation, these factors are best conceptualized as having interacting influence on SIBs (i.e., multifactorial; Crowell et al., 2014). Furthermore, various life circumstances or contexts may facilitate the confluence of suicide risk factors for an individual. A recent critique of contemporary suicide theory noted the lack of consideration for an individual’s contextual background (Hjelmeland & Knizek, 2020). Particularly, it was argued that suicide may be better understood by considering an individual’s historical, economical, political, cultural, and gender-related context. One context that may be particularly salient to suicide risk is residing in a rural region.
Individuals in rural areas may be at higher risk for suicide compared with individuals in nonrural settings because of myriad factors (Fontanella et al., 2015; Hirsch & Cukrowicz, 2014; Sankaranarayanan et al., 2010). These factors include but are not limited to individual (e.g., age, sex, educational attainment), geographic (e.g., lack of access to services), sociocultural (e.g., perceptions that men should be rugged and dominant, stigma toward seeking or receiving treatment for mental-health difficulties), interpersonal (e.g., thwarted belongingness, perceived burdensomeness), psychological (e.g., emotional distress, comorbid diagnoses), and environmental (e.g., economic hardship). To this end, it has been suggested that rural regions may have several unique considerations in the context of suicide prevention (Hirsch & Cukrowicz, 2014; McCarthy et al., 2012; Murphy, 2014). Thus, individuals living in rural areas may face unique challenges, such as indirect suicide factors, that increase the risk of subsequent SIBs. Given the unique considerations relevant for suicide in rural regions, it is imperative for researchers, mental-health professionals, and policymakers to have a comprehensive overview of contemporary rural suicidology. Furthermore, the most recent review in rural suicidology was published in 2014 (Hirsch & Cukrowicz, 2014), meaning there is an abundance of scientific work published within the last decade that has yet to be integrated into a comprehensive review.
Challenges in Rural Suicidology
Despite the need to understand suicide in rural areas, historically, there have been several concerns regarding how rurality has been operationalized. Researchers investigating suicide and rural regions have inconsistently defined and identified “rural.” Studies have used ambiguous population thresholds (Murphy, 2014), population density (Saunderson et al., 1998), or government-identified distinctions (Fontanella et al., 2015; Nestadt et al., 2017) or did not specify the criteria used to distinguish rural and nonrural regions/residents (Zhang & Lin, 2015). In addition, although dichotomous or ordinal indicators of rurality may be commonly used by researchers, likely because of their analytic simplicity, these may be less useful than continuous indicators in determining differences in suicide outcomes (Helbich et al., 2017). That is, transforming continuous data into categorical, discrete, or binary data may result in a loss of information of individual differences and statistical power (Cohen, 1983; MacCallum et al., 2002). Collectively, these inconsistencies preclude cross-study comparisons and a synthesis of the literature, which, in turn, may impede informed efforts to reduce SIBs.
Expanding on this concern is the lack of consideration of the heterogeneity of populations within similar geographies. As a result, factors that influence heterogeneity within a rural region and homogeneity between rural regions prevent accurate summarizations of rural-suicide literature. For example, two communities with identical population densities (a commonly used metric in rural suicidology) may vary in important ways, such as economic prosperity or trending increases or decreases in population. Although these communities are both rural, they may very well have unique suicide-related challenges and needs.
Finally, regions may also vary regarding economic, political, social, and psychological processes, and these will influence SIBs. Variation in the definition of “rural” and the populations studied may thus obfuscate the ability to amalgamate findings into a coherent knowledge base. Understanding variability of samples used in rural-suicide literature may help understand gaps in the contextual understanding of suicide. That is, trying to understand suicide in rural regions may be less effective when combining studies that have investigated rural regions with disparate contexts.
Considering the importance of context in understanding suicidal thoughts and behavior (Hjelmeland & Knizek, 2020) and the challenges with rural suicidology outlined above, mental-health providers and researchers may benefit from an up-to-date comprehensive review of the variability in the operational definition of rural. Furthermore, differences in direct-suicide constructs may vary by rural definitions and, thus, warrant investigation. Indeed, researchers, clinicians, and policymakers can best make decisions when informed by comprehensive summaries of the literature.
The Current Review
Given the above, the variability in conceptualizing rural in rural suicidology merits investigation. In addition, given that the most recent rural-suicidology review was almost a decade ago (Hirsch & Cukrowicz, 2014), an updated review of suicide-rural risk factors is warranted to assess the exponential increase in publications in rural suicidology over the last decade (see Fig. 1; approximately 1,300 new records since 2014). The current systematic review was conducted to serve these two objectives.
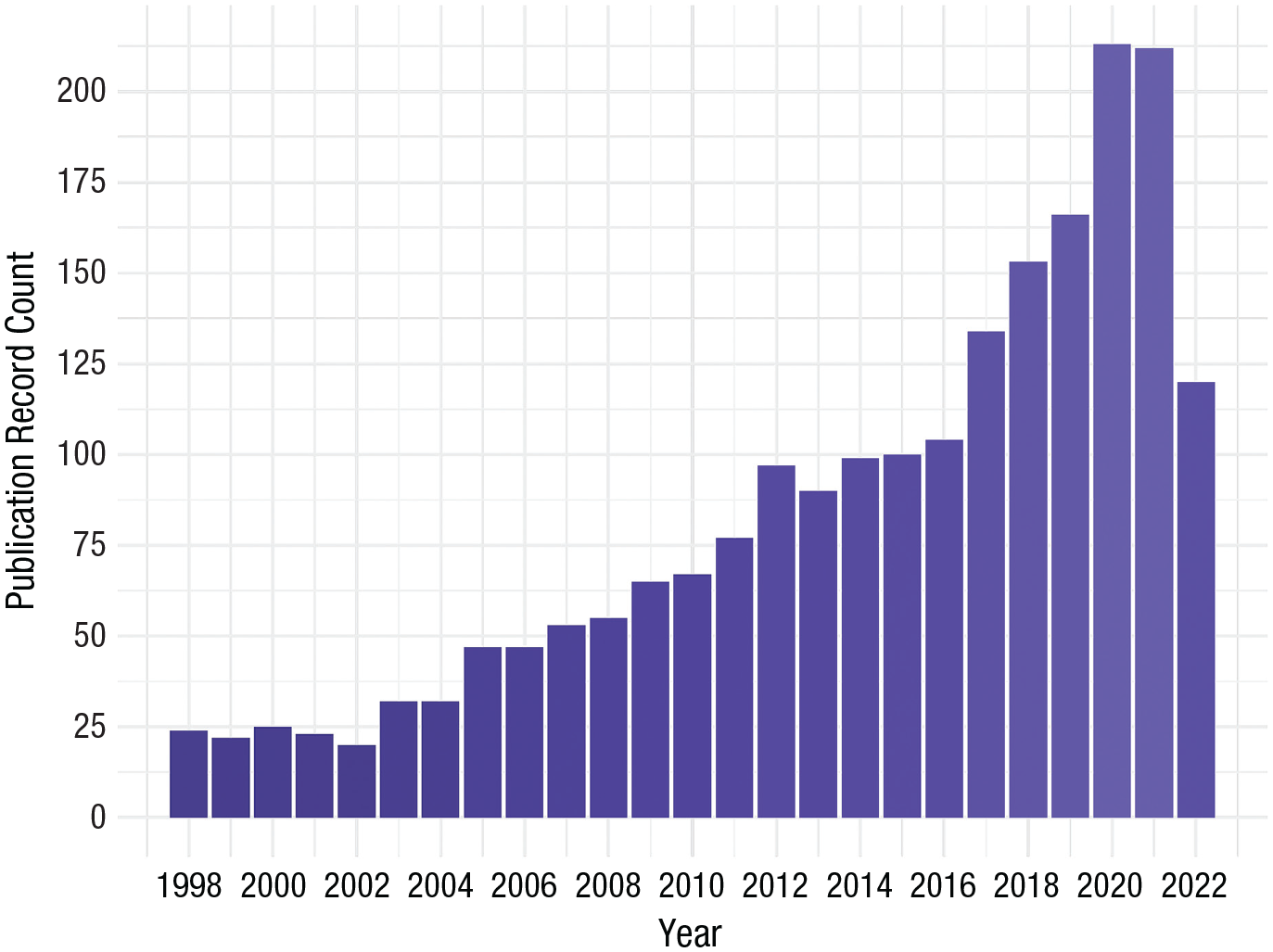
Publication records for topics “rural” and “suicide” since 1998 (from Web of Science).
The first goal of the review was to understand the variability in the definition of “rural” in suicidology. Rurality has seemingly been conceptualized in various ways with no clear or consistently used definition, which may inadvertently group heterogeneous populations when making conclusions about suicide in rural areas (Cantor & Coory, 1993; Lin & Zhang, 2015; Nestadt et al., 2017). Illuminating potential discrepancies in the definition of rurality can therefore help to enhance the understanding of rural suicide and guide future work in this area. This can, in turn, enhance suicide intervention and prevention in rural contexts.
The second goal of the review was to summarize differences in direct- and indirect-suicide-related constructs in the context of rural regions and whether these differences were associated with the operationalization of rural. Past rural studies have highlighted numerous differences between rural and nonrural regions regarding direct-suicide outcomes (e.g., prevalence of suicides, levels of suicidal ideation) and indirect-suicide-related mechanisms (e.g., depression association to suicidal ideation). Ultimately, an update review that considers the operationalization of rural can inform and direct researchers, clinicians, and policymakers in their efforts to support those experiencing SIBs.
Taken together, the objectives were to address the following questions:
Research Question 1: How has rurality been operationally defined in the rural-suicide literature?
Research Question 2: What are the differences in rural and nonrural regions regarding direct-suicide constructs (i.e., suicidal thoughts and behaviors)?
Research Question 3: What are the differences in rural and nonrural regions regarding indirect-suicide-related constructs (i.e., the mechanism that authors purport to be risks/causal risks for suicide in rural regions)?
Research Question 4: Do any differences in Research Question 2 or Research Question 3 depend on how rural has been operationally defined?
Transparency and Openness
Preregistration
This study was not preregistered.
Data, materials, code, and online resources
The final study data will be available from the corresponding author on reasonable request. For a full reference list of studies included in this review (Appendix A), study protocol (Appendix B), and summary table (Appendix C), see the Supplemental Material available online.
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Ethical approval
In the current review article, we synthesized existing literature, which did not involve the collection of new data. No formal ethical approval was required from the authors’ institutions for this research study.
Method
Review strategy
We sought to adhere to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations (Page et al., 2021) for the current review. A protocol was developed to guide the study, reduce bias (e.g., rater bias), and ensure that the research team followed a reliable approach to determining study inclusion and coding. Thus, the protocol outlined the scope and objectives of the review, search strategy to identify candidate studies, screening process, eligibility criteria, and quality-assessment guidelines. For the protocol, see the Supplemental Material.
Search strategy
T. R. Pritchard worked with a library consultant familiar with systematic reviews and the other authors to finalize a search strategy to best answer the research questions. Overall, the goal was to be inclusive (i.e., reduce false exclusions) at the initial stages of the review (Siddaway et al., 2019). The final search strategy used PsycINFO, PubMed, and Embase databases. For PsycINFO and PubMed, the Medical Search Heading (MeSH) were specified as: MeSH: “Suicide” OR MeSH: “Suicidal Ideation” AND MeSH: “Rural Population.” Index terms were also used for PsycINFO and specified as follows: ({Suicide} OR {Suicidal Ideation}) AND ({Rural Environments} OR {Regional Differences}). Last, Emtree search terms were used for Embase and specified as follows: suicidal behavior’/exp AND (‘rural health care’/exp OR ‘rural population’/exp).
Additional search strategies were implemented to ensure an unbiased representation of the rural-suicide literature. First, given that the published literature is an incomplete representation of scientific efforts and knowledge (Rosenthal, 1979), efforts were made to identify unpublished research that fit inclusion criteria. Specifically, ProQuest Dissertations & Theses A&I was used to search for the subjects and indexing terms: “su(rural) AND su(suicide).” Second, included studies’ reference sections were reviewed for studies that fit the inclusion criteria but were missed in the initial search.
Screening
T. R. Pritchard and two trained coders screened all abstracts for eligibility for inclusion in a full-text review (see criteria below). Meetings were then held to discuss abstracts that did not clearly fit within the eligibility criteria and to reach consensus for inclusion/exclusion. All studies that met inclusion at the abstract-screening stage went on to a full-text review for an additional screening stage. Here, a team member reviewed the full study and decided on its inclusion in data extraction. Finally, the remaining studies had their data extracted for analyses (e.g., operational definitions of rural; variables used in analyses). See the protocol (Supplemental Material) for a complete list of data that were extracted from each study.
Protogerou and Hagger’s (2020) proposed study-quality criteria were used to evaluate the overall quality of the included studies. This checklist of 20 items assesses the quality of articles across the study introduction, participants and recruitment, data analysis and findings, and ethics. Studies can be scored 0 (absent) or 1 (present) on each criterion, resulting in a range of 0 to 20. Several cutoffs for an “acceptable” quality study have been proposed (Protogerou & Hagger, 2020). However, we included studies with any score, given one of our research questions is directly tied to properly operationalizing variables. The mean quality score of the included studies was 6.89 (range = 0–15).
Inclusion and exclusion criteria
Several inclusion and exclusion criteria were used to determine studies’ appropriateness for inclusion in this review.
Study design
Both qualitative and quantitative scientific approaches can inform the research objectives of a review. Thus, there were no study design limitations (e.g., circumscribing to randomized control trials). In addition, studies were included if they were in peer-reviewed journals or published as theses/dissertations and written in English.
Participants’ characteristics
Studies involving participants living in a rural setting were included in the review. An objective of this review was to assess the variability in the operational definition of rural; thus, any study claiming that the sample consisted of individuals from rural regions was selected, including those that lacked an operational definition of rural. In sum, studies were included if they contained a sample of rural participants or rural and nonrural participants together.
Types of outcomes to be included
Included studies were required to investigate suicide-related constructs. Specifically, included studies must have (a) measured direct-suicide constructs in rural regions, (b) tested for differences in direct-suicide constructs between rural regions and nonrural counterparts, (c) tested for associations between indirect- and direct-suicide-related constructs in rural regions (e.g., used rural or the indirect-suicide-related construct as a mediator), or (d) tested differences in the associations between indirect- and direct-suicide-related constructs between rural regions and nonrural counterparts (i.e., moderation). For example, a study may have tested if a lack of social support (i.e., an indirect construct) mediated the relation between rurality and suicide death rates (i.e., Criteria c; rural living → social support → suicide). Risk factors have historically taken many roles in psychological research, such as being correlated with, being mediated by another factor, or being causally linked to an outcome (Kraemer et al., 2001). Differentiating the mechanisms that link risk to suicidality is needed to further the understanding of and prevention efforts toward suicide. With this in mind, in the present review, we focused only on mechanisms (e.g., hypermasculinity) that were either purported by the authors of reviewed studies to link rurality to suicide or those that linked rurality to suicide by way of theory.
Direct-suicide outcomes are those that fit within the taxonomy proposed by Posner et al. (2014) and incorporate suicide behaviors (e.g., attempts, deaths) and ideations (e.g., wishing to die). Indirect-suicide-related outcomes are those that authors purport to mediate or moderate suicide-rural associations (e.g., lack of service availability; hypermasculinity).
Results
The initial search yielded 1,089 unique results (1,874 with duplicates) that proceeded to abstract review. Figure 2 presents a flowchart outlining the search results and included studies at each level of review. After abstract and full-text review, the final sample size for the study was 142. These final studies were published in 80 different journals, and most were published in the last decade (2012–2020). See Figure 3 for the distribution of publications across years. Most studies had cross-sectional and observational designs (n = 107; 75.35%). An additional 27 studies had a longitudinal and observational design (19.01%), seven had a qualitative design (4.93%), and one was a systematic review (0.70%). No studies implemented experimental designs or meta-analyses.
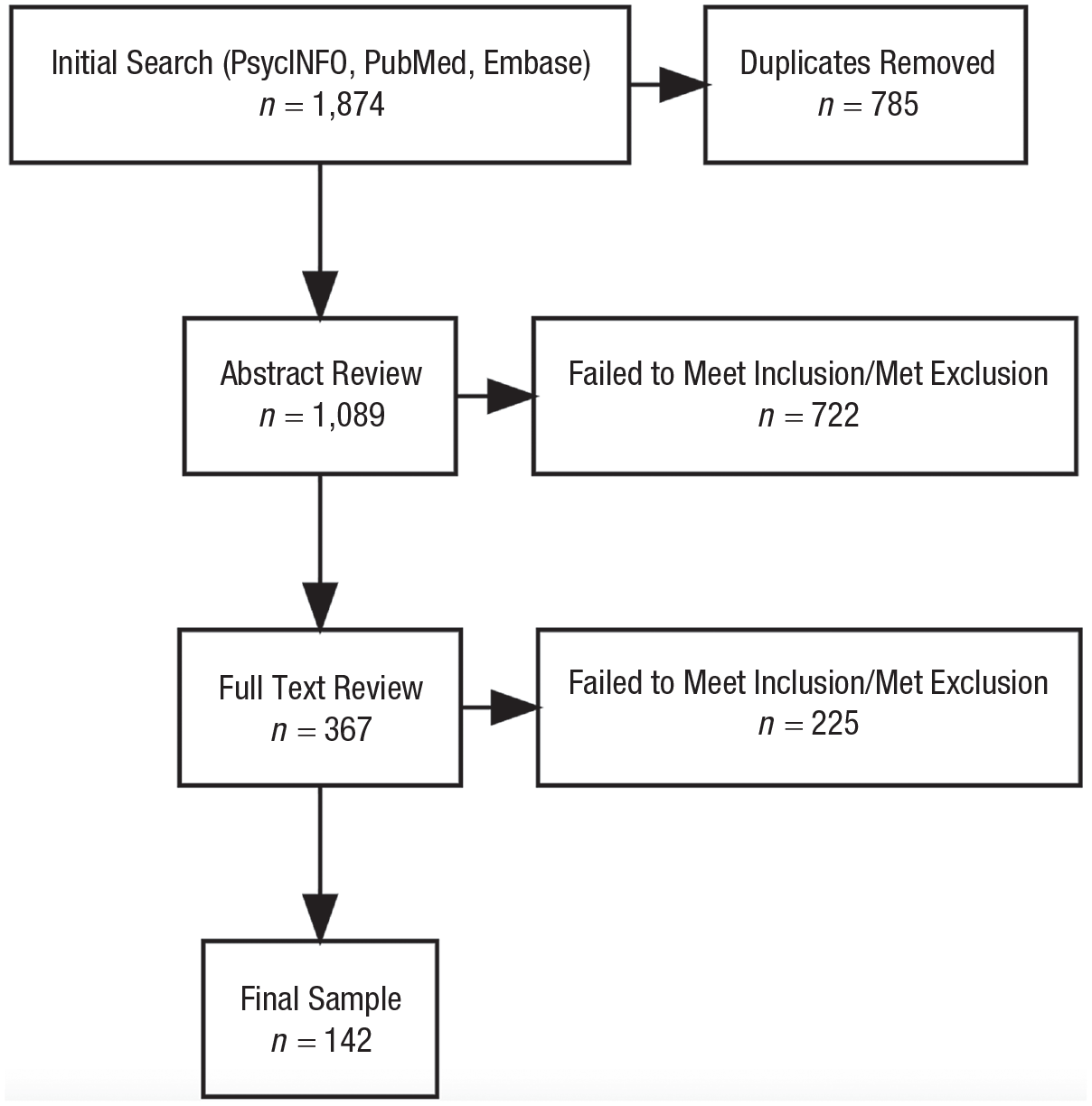
Flowchart outlining included and excluded articles.
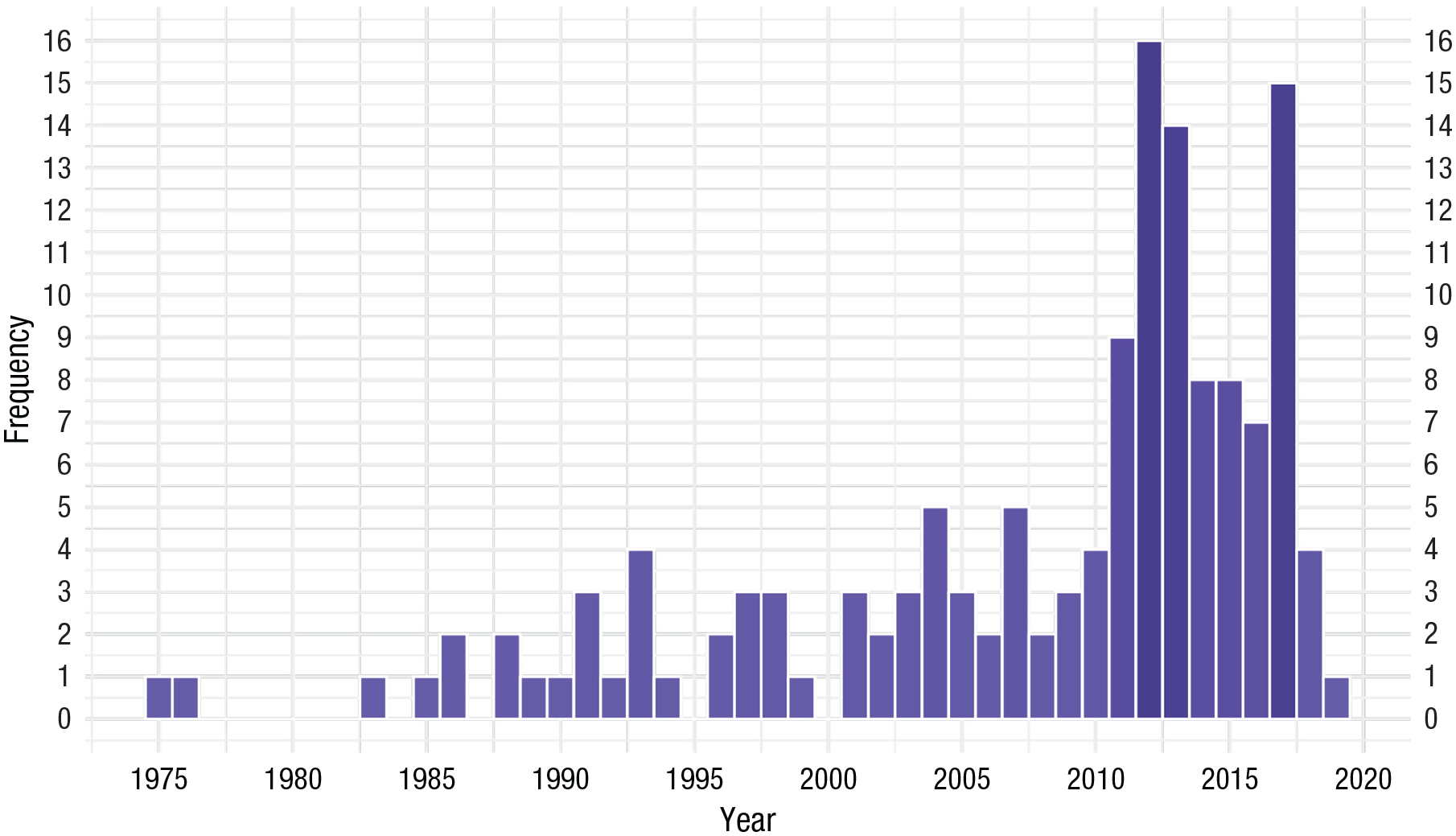
Publication of rural-suicide studies over time.
How has rural been defined in the literature?
No studies provided an explicit definition or conceptualization of rural in the introduction sections. However, the authors of one study presented rurality as a latent construct represented by indicators of employment and household patterns (Congdon, 2011).
On the bases of the articles examined, we classified studies that operationally defined rural in the method or later sections (e.g., results) across five categories (described below): population cutoff, population density, classification categories, other methods, and unclear methods. Of the 142 studies reviewed, 79 (55.63%) provided indices or measurements of rurality.
First, 14 (9.86%) studies used a population cutoff, which varied by as high as a 1:25 ratio (i.e., the largest cutoff was 25 times larger than the smallest). Specifically, studies considered places or people as rural using a cutoff of fewer than 2,000 (n = 2), 2,500 (n = 1), 3,000 (n = 1), 5,000 (n = 1), 6,000 (n = 1), 10,000 (n = 3), 15,000 (n = 1), and 20,000 (n = 2). In addition, some studies used specific ranges: 1,000 to 25,000 (n = 1) and 3,000 to 7,000 (n = 1). A simulation of these various population sizes with similar population density is shown in Figure 4.
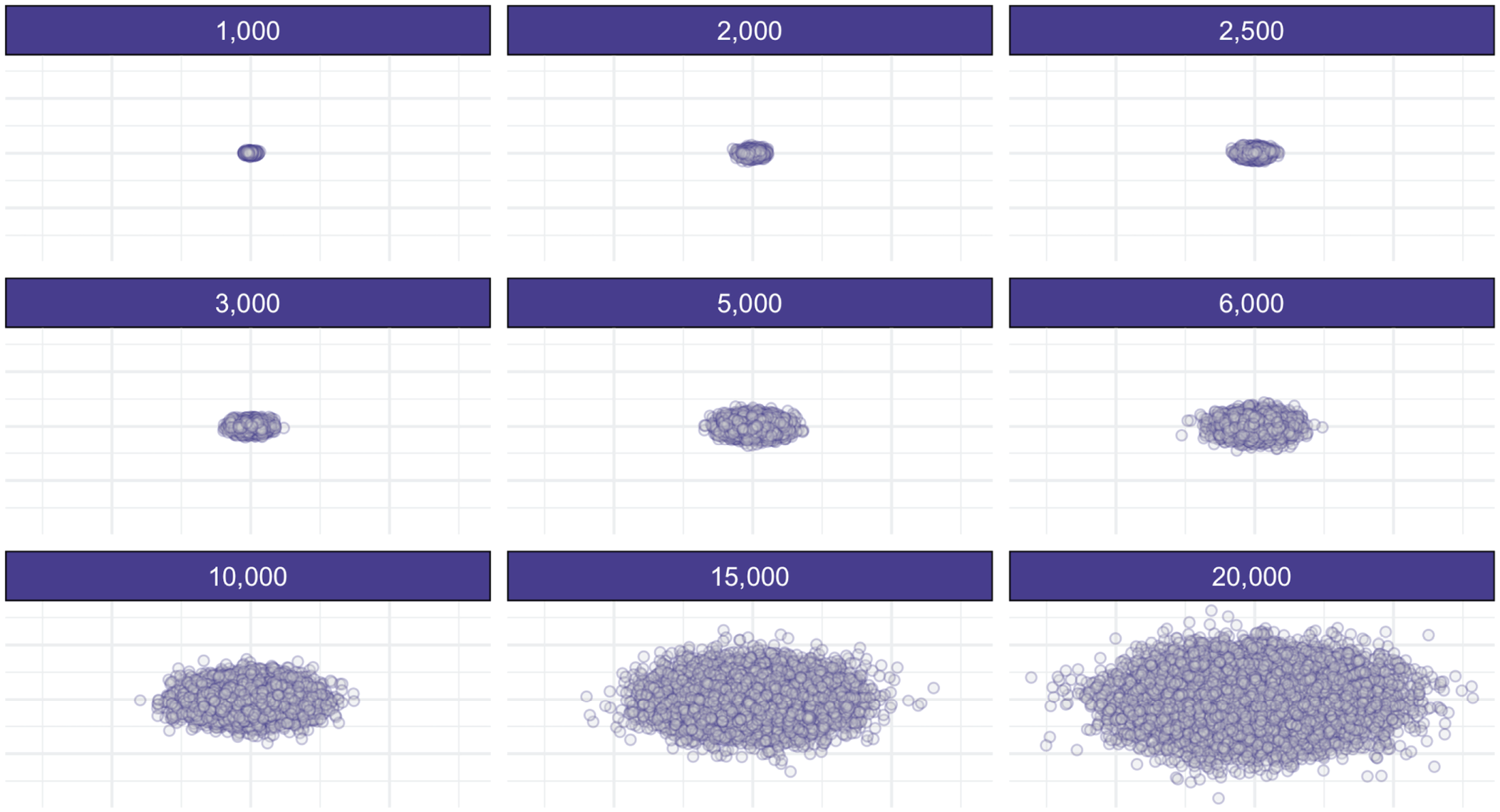
Comparing simulated sample sizes.
Second, 15 (10.56%) studies used population density to classify people or regions as rural. Specifically, studies considered places or people as rural using a density of fewer than 28/mi2 (n = 1), 1,000/mi2 (n = 2), 12/km2 (n = 1), 3,000/km2 (n = 1), and quantiles of density (n = 3). Another seven studies did not clearly present the density that was used for classification. A simulation of these various population densities randomly distributed within a standard unit (e.g., mi2) is shown in Figure 5.
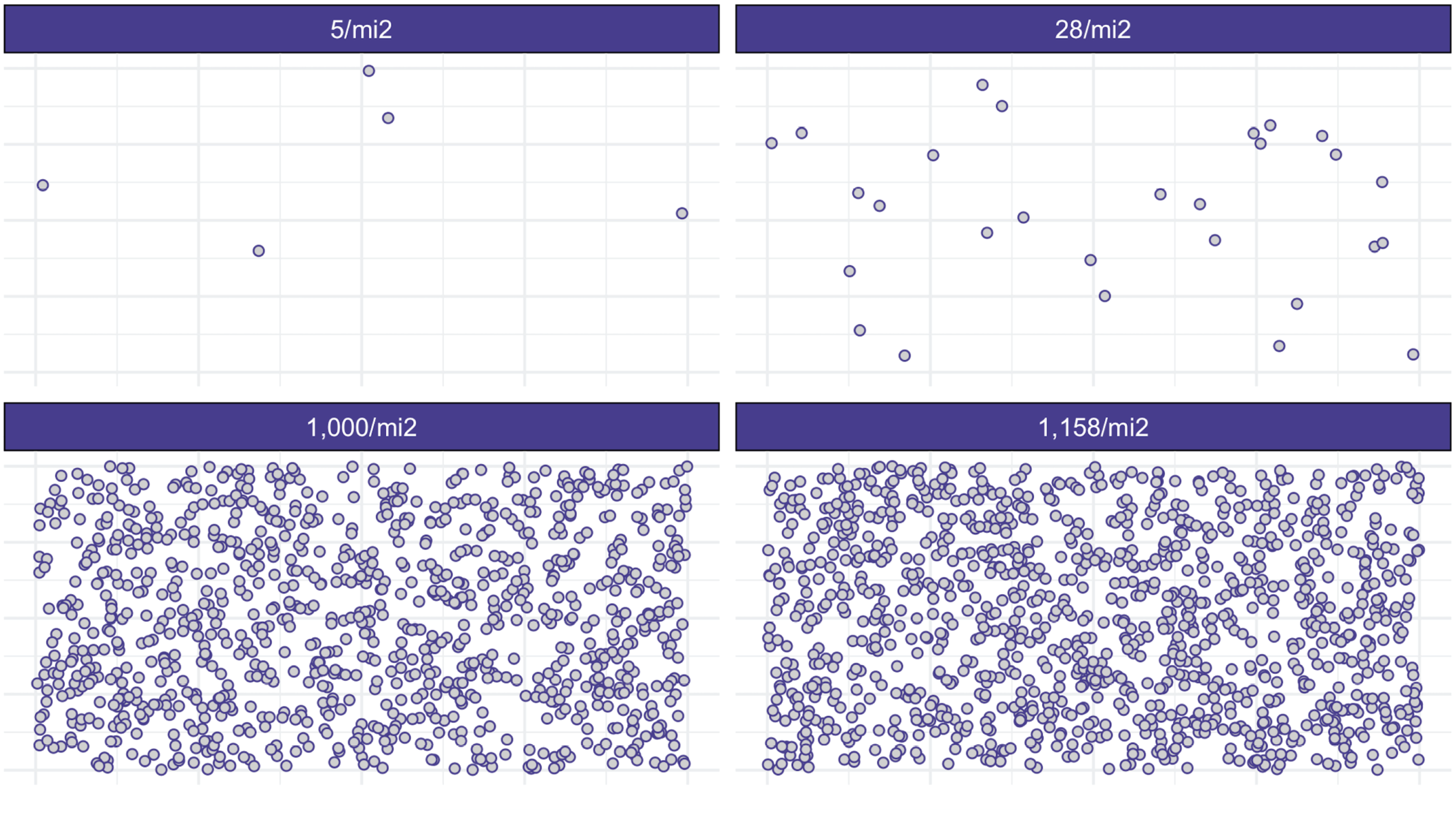
Comparing simulated population densities. We converted km2 to mi2.
Third, 32 (22.53%) of the reviewed studies used a form of group coding system to classify people or regions as rural. Specifically, Rural-Urban Continuum Codes (n = 5); Australian Standard Geographical Classification (n = 4); Rural, Remote, and Metropolitan Area Classification (n = 4); Accessibility/Remoteness Index of Australia (n = 2); quantiles of deprivation (n = 2); Australian Local Government Areas (n = 1); Australian Statistical Geography Standards (n = 1); Household Registration Management System (n = 1); New Zealand Urban-Rural Profile (n = 1); Metropolitan and Census Agglomeration Influenced Zones (n = 1); National Socioeconomic Classification Criteria (n = 1); and Urban Influence Codes (n = 1) were used to classify rural and nonrural regions. Eight studies did not clearly state the method of group coding.
Finally, three (2.11%) studies used other methods that did not clearly fit into one of the classification systems. A study by Lee et al. (2018) sampled from the Gangwon, Jeonnam, and Gyeonggi provinces in South Korea but provided no additional information regarding rurality. Another study used ZIP/Crosswalks (Britton et al., 2017), and a final study (Dai et al., 2011) used a composite of considerations without operationally defining the criteria. The final 14 (9.86%) studies did not clearly outline any classification method. Figure 6 presents a visualization of the distribution of classification types.
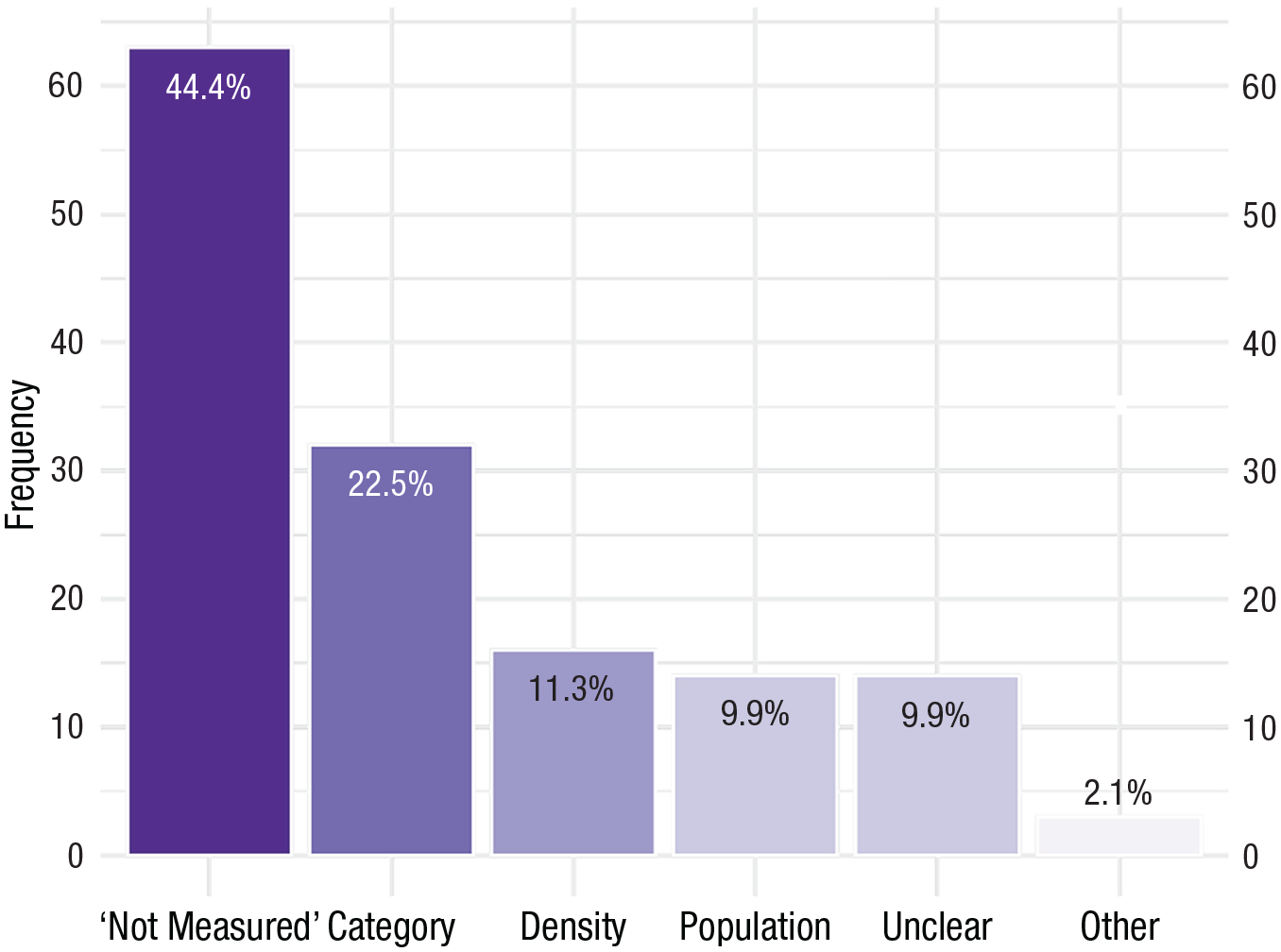
Frequency of rural classification types (n = 142).
Direct-suicide constructs
In order of frequency, the reviewed studies investigated death by suicide (n = 110; 77.46%), suicide attempts (n = 23; 16.20%), suicide ideation (n = 19; 13.38%), suicidal behaviors (n = 12; 8.45%), and suicidal thoughts (n = 3; 2.11%).
Of the 110 studies investigating suicide deaths, 80 (56.34% of total sample) compared rural with a nonrural counterpart. Within this subset of studies, 22 reported that rural suicide deaths were higher and statistically significant than those occurring in nonrural regions. However, there was a larger subset for which the results suggest a more complex relation between rural living and death by suicide or had missing information (n = 58). For example, five studies reported that rural deaths were higher but did not present information regarding the statistical significance of the difference. In addition, within the complex/unclear group, studies sometimes reported mixed results, or findings that were qualified by significant interactions of demographic or other variables. These interactions were not purported to be the mechanisms responsible for rural suicide and thus are not included in the section on the indirect-suicide construct (see below). Other studies did not report enough information to determine the exact metric of rural/nonrural death and/or if the results were statistically significant. In addition, there was variability in the metrics used to report deaths (e.g., hazard ratios, prevalence) and in the timeline of data collection.
A total of 11 studies (7.75%) compared suicide attempts across rural and nonrural regions. Of these, one reported higher and statistically significant attempts in rural regions (Karami et al., 2018). Another three reported statistically significant lower attempts in rural regions (Davaasambuu et al., 2017; Goldman-Mellor et al., 2017; Harriss & Hawton, 2011). Finally, another seven studies did not compare rural and nonrural regions using significance testing, did not report enough information to draw a conclusion, or reported unclear information.
Nine studies (6.34%) compared suicidal ideation between rural and nonrural regions. Of these, four reported statistically significant higher suicidal ideation in rural regions (Chiang et al., 2013; Dou et al., 2015; Lee et al., 2018; Meng et al., 2013). Conversely, two studies reported statistically significant lower suicide ideation in rural regions (Abel et al., 2012; Goldman-Mellor et al., 2017). Three studies did not provide enough detail or did not compare through significance testing.
Three (2.11%) studies compared suicidal behaviors across rural and nonrural regions. One reported a statistically significant higher rate of suicidal behaviors in rural regions compared with urban counterparts (Alaghehbandan et al., 2011). One study reported a statistically significant lower rate of suicidal behaviors among rural regions (Davaasambuu et al., 2017). Last, another study reported a moderated association between rurality and suicidal behavior (Williams et al., 2015).
Does rural definition affect direct outcomes?
Chi-square tests of independence were used to determine if the results (i.e., potential differences in rural and nonrural regions) of the included studies were dependent on the operational definition of rural. Results were separated into three groups: (a) higher risk in rural regions, (b) lower risk in rural regions, and (c) unclear/mixed/no difference in risk in rural versus nonrural regions. These were further separated based on risks for four specific suicide-related constructs: suicide death, attempt, ideation, and behavior. Rural definitions were separated by density, cutoff, category, other method, or unclear. Thus, four chi-squares of a maximum 8 df were used with an adjusted alpha of .01. Given the low expected cell counts for all these analyses, they should be interpreted with caution. First, the results of studies that compared suicide deaths between rural and nonrural regions (n = 80) were not associated with the operational definition of rural, χ2(8) = 8.14, p = .420, Cramer’s V = .23, 95% confidence interval [CI] = [.00, .29]. Second, the results of studies that compared suicide attempts between rural and nonrural regions (n = 11) were not associated with the operational definition of rural, χ2(6) = 4.19, p = .651, Cramer’s V = .44, 95% CI = [.00, .63]. Third, the results of studies that compared suicide ideations between rural and nonrural regions (n = 9) were not associated with the operational definition of rural, χ2(4) = 2.10, p = .717, Cramer’s V = .34, 95% CI = [.00, .61]. Last, the results of studies that compared suicide behaviors between rural and nonrural regions (n = 3) were not associated with the operational definition of rural, χ2(2) = 3.00, p = .223, Cramer’s V = 1.00, 95% CI = [.00, 1.00].
Indirect-suicide constructs
Fourteen (9.86%) studies investigated the following indirect SIB factors: limited access to health and mental-health services (n = 2), alcohol availability/risky alcohol consumption (n = 2), firearm ownership/availability (n = 2), civic engagement/sense of community (n = 2), bullying/social isolation/social-support unavailability (n = 2), depression (n = 2), deprivation/proportion of middle-class presence (n = 2), residential stability (n = 1), agricultural employment (n = 1), altitude (n = 1), religiosity (n = 1), masculine ideals (n = 1), and male unemployment (n = 1). Of these, four studies compared a rural and a nonrural counterpart on the indirect construct.
Several articles highlighted differences in rural and nonrural regions regarding indirect-suicide constructs; however, there were no clear patterns in these results. For instance, owning a handgun was a risk for suicide, but only in urban areas (Brent et al., 1993). Moreso, although rural residents may have been more likely to own a long gun than their urban counterparts, the relation was not statistically significant (Brent et al., 1993). Deprivation has also been suggested to be an indirect construct that implicates rural-suicide risk (Levin & Leyland, 2005). Specifically, deprivation—a composite of car ownership, lower social-economic class, male unemployment, and overcrowding—was proposed to explain higher rates of suicide in urban areas.
Access to physical or psychological health services may also account for some of the rural-suicide relationship. Although rural and urban residents did not differ in the rates of contacting general physicians in the month or year before dying by suicide, rural-suicide decedents were less likely to have had a prior-year admission to a hospital than urban counterparts (Stark et al., 2012).
Differences in communication patterns between rural and urban residents were also highlighted as a potential mechanism for differences in rural and urban suicidality. Specifically, McPhedran and De Leo (2013) reported that despite having less contact with mental-health professionals before dying by suicide, rural men were no less likely to communicate suicide intent than urban counterparts. Thus, ensuring adequate resources are available and offered for men who communicate intent is imperative for suicide-prevention efforts.
The association between operational definition of rural and differences in indirect outcomes between rural and nonrural regions was not investigated given the low prevalence of included studies. Ultimately, no conclusions could be made given the low sample size in a potential analysis.
Discussion
The goal of this study was to review the variability in the operational definition of rural in rural suicidology and differences in direct- and indirect-suicide constructs in rural and nonrural regions. Although other reviews in this area have been published (Hirsch & Cukrowicz, 2014), this review provides a needed update on the literature and extends prior reviews by accounting for variability in the operationalization of rurality in the field of suicidology and how this operationalization may play a role in the findings of studies concerning direct- and indirect-suicide risk in rural settings.
Rural definitions in suicidology
Of the studies examined, there is much variability in the operational definitions of rurality. Some studies used population cutoffs, population densities, and classification systems, whereas other studies implemented unclear or unstated measurement methods for classifying people or places as rural. Given the heterogeneity of the characteristics of determining rurality (e.g., population cutoff, categorical systems), it is imperative to pinpoint the rural features that are relevant to suicide and to consider these features when operationally defining rural in suicide research. Further to this point is the consideration that rural features relevant for suicidology versus other public-health concerns may vary (Hart et al., 2005). It has been noted that “depending on the study context, certain rural definitions may be more relevant than others” (Hawley et al., 2017, p. 32). The current review highlights an apparent lack of consistency and thus, no clear consensus when defining rural in suicidology. Furthermore, there seems to be little evidence for the justification of how and why particular conceptualizations of rural are used, and thus, it is unclear whether they account for suicide-specific considerations.
Approximately one quarter of the reviewed studies used some categorical classification system to define and measure rural. A benefit of this approach is the possibility of avoiding a dichotomy of urban and rural, which amalgamates differing rural regions and people into one group. For example, Rural-Urban Continuum Codes differentiate rural regions (populations below 2,500) by their proximity to nearby metro regions (U.S. Department of Agriculture, 2020). Although this indicator is applied strictly to the United States, similar classification systems exist for other countries (Metropolitan Influenced Zones in Canada; Statistics Canada, 2017). Despite this, many researchers employed a “rural or not” approach to classification based on population cutoffs, which varied by a factor of 25, or densities, which varied by a factor of 232. It is common knowledge, but perhaps not practice, to avoid dichotomization of continuous variables for myriad reasons, such as a loss of information about individual differences (MacCallum et al., 2002). However, avoiding dichotomization would be required only should there be quantitative differences in rural (i.e., a continuous variable). Further exploration into potential quantitative and qualitative differences in the definition of rural may be integral to furthering rural suicidology.
Differences in direct and indirect risks
The results of this review paint a murky picture regarding differences in rural and nonrural regions in suicidal ideations and behaviors. Indeed, for suicide deaths, attempts, and behaviors, most studies presented a complex or nuanced association with rurality. Despite this murkiness, about a quarter of the reviewed studies compared suicide deaths in rural versus nonrural regions, and most studies concluded that rural living is a risk factor for suicide death. However, rural living may be a risk factor for suicide death in some cases (Dresang, 2001; Sankaranarayanan et al., 2010) yet not for others (Middleton et al., 2003). A recent meta-analysis indicated that rural living, as indicated by lower population density, distance to urban centers, and distance to health services, may be a particular risk for suicide among men, but not women (Barry et al., 2020). Looking ahead, teasing apart such potential moderators and mediators is necessary to further the understanding of rural suicidology.
Overall, the current body of literature precludes any clear conclusions regarding how rurality is associated with suicide ideations, attempts, and behaviors. There is some indication that suicide deaths are higher in rural regions, but this is a tenuous conclusion given the definitional issues concerning rurality reflected in this review. Although we noted that a study’s definition of rural did not moderate a rural-suicide death relationship, this finding should be interpreted with caution because of the abundance of studies without a clear definition of rural. Note that there were fewer studies directly comparing nondeath suicide outcomes among rural and nonrural people or in rural versus nonrural places. Here, comparing whether rural definitions were associated with differential rural versus nonrural outcomes was not feasible given the few available studies. A possible explanation for fewer studies investigating these constructs may be that many of the studies we examined were epidemiological in nature; thus, examining suicide deaths may represent the most readily available data (e.g., public death records) for these researchers. It may also be that death by suicide is a more consistently and easily defined behavior (i.e., consisting of agency, intent, and outcome; Posner et al., 2014) compared with ideations and attempts, although vagueness in the suicide taxonomy is a long-standing issue (Klonsky et al., 2016). The lack of focus on the breadth of SIBs (i.e., not just suicide death) is a limitation in rural-suicidology research. Suicidal ideations are more frequent than suicide attempts, which are more frequent than deaths by suicide. Thus, death by suicide is only the tip of the iceberg when it comes to gaining a full understanding of suicide in rural regions, and researchers and clinicians cannot underestimate the potential impairments and distress associated with frequent suicidal ideations (Jobes & Joiner, 2019). Furthermore, contemporary suicide theory, often referred to as ideation-to-action frameworks (e.g., three-step theory; Klonsky & May, 2015), highlight the importance of understanding the progression from ideations to attempts. Thus, it is not surprising that differences may exist in the relations between rurality and suicide ideations, behaviors, attempts, and deaths. Grounding rural suicidology in contemporary theory is imperative in understanding suicide to advance suicide-prevention efforts.
Limitations
This review has limitations that should be considered when interpreting its findings. First, we investigated indirect-suicide-related factors that the authors purported to be responsible for differences in direct-suicide factors for rural and nonrural living versus every moderator or interaction that researchers incorporated into their analytic models, which would have obfuscated our results and likely rendered them uninterpretable. It is concerning (Wysocki et al., 2022) that researchers often include moderators or control variables without specifying causal pathways of independent, dependent, moderating, and control variables. In line with this, only a small number of studies in this review examined indirect factors as causal mechanisms within the context of the association between rurality and suicide. However, without accounting for the totality of relevant moderators or interaction terms, this link remains opaque. Second, our search terms may have excluded some search terms that would have captured additional studies. A future review may consider expanding the search strategy to account for potentially excluded work. Third, we did not investigate potential age-related differences in the rural-suicide associations in the reviewed studies. Indeed, some rural regions tend to have aging and older populations (Statistics Canada, 2018). Furthermore, suicide may be higher in midlife to late life, particularly for men (Centers for Disease Control and Prevention, 2022), marking a potential confound in the rural-suicide association. Only a direct investigation of age as a moderating variable in the rural-suicide relationship could determine the residual effect of rurality on suicide risk.
Recommendations
Building on our overall findings, we present several recommendations (for a brief overview, see Table 1) to propel research on rural suicidology. We first recommend additional attention to, justification of, and transparency with the definition of rural in suicidology. At a minimum, researchers should present how rural is measured in their studies. Although this may seem obvious, our results suggest that assuming measurement transparency is unwarranted. A more comprehensive approach would be to consider rural as a social construct and potential latent variable (Congdon, 2011) comprising various contextual indicators. For example, researchers can model various psychosocial (e.g., belongingness, cultural dissonance), geographic (e.g., population density), cultural (e.g., normalized risky alcohol consumption), and systemic factors (e.g., availability of mental-health services) to determine their suitability as indicators of rural. This rural latent factor can then be tested for associations with SIBs or other relevant variables. Although the current practice of using extant metrics (e.g., densities, government-created categories) is likely practical and analytically efficient, the results of this study highlight consequences, such as a murky evidence base with few conclusions, of such practice. We recommend authors refer to Flake and Fried (2020) for detailed recommendations on measurement practices.
Recommendations for Future Studies
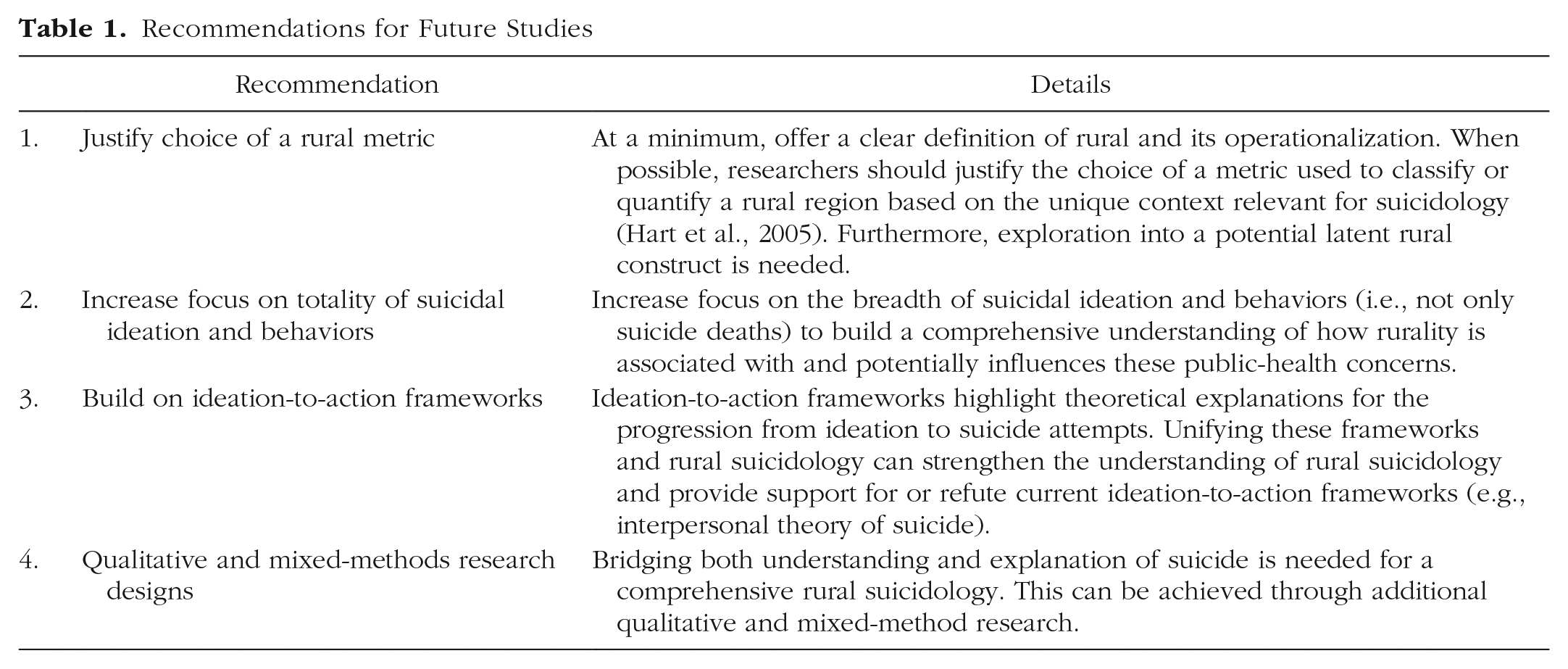
Second, we recommend an increased focus on the breadth of suicidal ideations and behaviors. Most studies seem to investigate suicide deaths; however, a comprehensive rural suicidology requires going beyond researching rural deaths and incorporating the full taxonomy of suicide. Although suicide is no doubt a public-health concern, there is significant distress and impairment associated with frequent passive and active ideations and nondeath behaviors, which occur more frequently than suicide death (Jobes & Joiner, 2019). Ideation-to-action frameworks may provide a useful guide for research involving the completeness of suicidal ideation and behaviors (Klonsky & May, 2015). However, it is important to use theory with a critical lens and acknowledge potential limitations, such as generalizability (Wiglesworth et al., 2023).
Our last recommendation focuses on observed inconsistencies in the approaches used to examine rural suicidology. Most researchers from the reviewed studies implemented quantitative research methods. Indeed, the fact that quantitative approaches accounted for much of the suicidology research has been a long-standing concern, with many researchers focusing on explanations of suicide (Gili et al., 2019; Murphy, 2014; Van Orden et al., 2010) versus the meaning of suicide (Hjelmeland & Knizek, 2010; White & Stoneman, 2012). The larger number of quantitative studies identified in our review may be due to our approach and the search terms used, which may not have captured the entirety of qualitative work in this field. Looking ahead, future work should explicitly seek qualitative work in the rural-suicide literature to further understanding of suicide. Indeed, in keeping with calls to action in the field (Hjelmeland & Knizek, 2010), multiple approaches to the scientific study of suicide are needed. Researchers may consider approaches that are not as dominant in rural suicidology (e.g., constructivist vs. positivist). As noted by Hjelmeland and Knizek (2010), mixed-method studies may be fruitful avenues that can provide complementary, converging, or contradicting evidence, all of which propel suicidology toward a comprehensive understanding of suicide ideations, behaviors, and deaths. For example, in this review, one article outlined detailed photovoice interviews that highlighted the stigma experienced by rural men with mental illness who later died by suicide and the potential self-medication through drugs and alcohol (Creighton et al., 2017). Understanding the unique processes and complexity within individuals and the general principles that are similar between individuals (Leenaars, 2002) is likely required for a comprehensive rural suicidology and, importantly, clinical practice. Simply stated by Leenaars (2002), “We need both quantitative and qualitative methods in suicidology” (p. 2). Rural suicidology is no exception. It would be concerning, and potentially neglectful, to imagine clinicians not inquiring about or incorporating the unique meaning of suicide for a patient into their work. The meaning of suicide for the individual has important clinical implications (Freedenthal, 2018) and, thus, should be represented in research. Thus, we hope future researchers will consider the usefulness of qualitative and mixed-methods approaches to understanding rural suicide.
Conclusions
Suicide has been a long-standing concern in rural regions given numerous individual (e.g., sex), geographic (e.g., lack of access to services), sociocultural (e.g., stigma), interpersonal (e.g., thwarted belongingness), psychological (e.g., comorbid diagnosis), and environmental (e.g., economic hardship) factors that may be related to an increased risk. The present study provides an updated and novel review of rural suicidology, highlighting several features of rural suicidology, such as the variability in terms used to classify rural people or places, and the unclear link between rural living and suicidal ideation and behaviors. Furthermore, we present recommendations to propel rural suicidology forward. Ideally, researchers can draw on our recommendations to design theory-informed research with the goal of understanding and explaining suicide, ultimately reducing the prevalence and impairments of suicidal ideation and behaviors in rural regions.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026241234319 – Supplemental material for Rural Suicide: A Systematic Review and Recommendations
Supplemental material, sj-docx-1-cpx-10.1177_21677026241234319 for Rural Suicide: A Systematic Review and Recommendations by Tyler R. Pritchard, Jennifer L. Buckle, Kristel Thomassin and Stephen P. Lewis in Clinical Psychological Science
Supplemental Material
sj-docx-2-cpx-10.1177_21677026241234319 – Supplemental material for Rural Suicide: A Systematic Review and Recommendations
Supplemental material, sj-docx-2-cpx-10.1177_21677026241234319 for Rural Suicide: A Systematic Review and Recommendations by Tyler R. Pritchard, Jennifer L. Buckle, Kristel Thomassin and Stephen P. Lewis in Clinical Psychological Science
Supplemental Material
sj-docx-3-cpx-10.1177_21677026241234319 – Supplemental material for Rural Suicide: A Systematic Review and Recommendations
Supplemental material, sj-docx-3-cpx-10.1177_21677026241234319 for Rural Suicide: A Systematic Review and Recommendations by Tyler R. Pritchard, Jennifer L. Buckle, Kristel Thomassin and Stephen P. Lewis in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Pim Cuijpers
Editor: David A. Sbarra
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.