
Abstract
Introduction
Globally, 800,000 people die by suicide every year – one death every 40 seconds (World Health Organisation, 2019). According to the most recent published data in England and Wales in 2019, there were 5691 registered suicides, 11 deaths per 100,000 population (Office for National Statistics, 2020).
The Centre for Mental Health’s ‘Zero suicides’ report suggested that “the economic and social cost of one suicide is estimated at £1.5 million” (Centre for Mental Health, 2015). For every suicide, it has been estimated that 135 people are directly affected (Cerel et al., 2019). It is thought that exposure to suicide is on a continuum with some people directly exposed or witness to a suicide, some directly or indirectly affected, and some bereaved (Cerel et al., 2014). The continuum defines individuals exposed to suicide as “anyone who knows or identifies with someone who dies by suicide,” and stresses that this no longer merely just focuses on kin or those who were exposed to the trauma of the death itself but focus on all of those who may be affected by a suicide (Cerel et al., 2014, p. 4).
Pitman et al. (2016) found that people bereaved by suicide are 65% more likely to attempt suicide than people who are bereaved by natural causes, increasing the absolute risk to 1 in 10. Furthermore, regardless of whether the participants were blood-related to the deceased, the effects of suicide bereavement were similar. These findings suggest that bereavement by suicide is a risk factor for a suicide attempt and its effects are not confined to immediate family members and thus, suicide bereavement effects wider support networks.
A study investigating suicide deaths in 10–19-year-olds (n = 595) between 2014-2016, using inquest information found that 9% (n = 51) had been bereaved by suicide (Rodway et al., 2020). Bartik et al. (2020) study of 18-year-olds who had experienced a friend’s suicide in rural Australia found that young people exposed to a friend’s suicide experienced significantly high levels of depression, anxiety and maladaptive coping strategies such as alcohol use. Those identifying themselves as “close friends” were at less risk of suicide but displayed increased mental health concerns as a result of their friend’s death. Those identifying themselves as “peripheral friends” were at a greater risk of suicide. However, the limitations of this study suggest that the sampling was open to selection bias, there was a distinct lack of randomisation and the small sample size had insufficient statistical power to meet requirements of quantitative method deduction, and the sample were not re-tested and therefore, results only capture participant’s experience from one point in time. Pitman et al. (2014) found an increased risk of psychiatric admission for parents bereaved by the suicide of their child. Additionally, the suicide of a child places parents at greater risk of psychological morbidity and physical health problems such as poor diet and smoking, compared to other causes of death (Erangsen & Pitman, 2017; Pitman et al., 2014).
The process of an intervention post-suicide was acknowledged by Edwin Schneidman, as “postvention is the prevention for the next generation” (Cain, 1972, pg. x). Postvention is a process which alleviates the effects of stress and aids in coping with a death by suicide. Professionals working with people bereaved by suicide noted that people they characterise their grief as a unique experience requiring specific intervention (Schuyler, 1973; Batzler, 1988; Knight, 1992). Harwood et al. (2002) reported that individuals bereaved by suicide felt highly distressed by legal procedures, specifically the coroner’s office and the inquest. Similar levels of distress were caused by the media reporting on the suicide, therefore postvention services should address these experiences. Dyregrov (2011) recommended that postvention support should adapt to meet each individual bereaved person’s needs.
Andriessen et al. (2017) suggested that postvention research should focus on increasing intercultural collaboration and theory-driven research whilst encouraging relationships between research and practice. Furthermore, Campbell et al. (2004, p. 31.) suggested that “an essential ingredient for successful implementation... is acceptance or buy-in by various police departments... and coroners”, therefore it is crucial that services collaborate with statutory services that are involved in suicide bereavement. McGeechan et al. (2018) compared police and coroner-led postvention strategies and found that coroners were more consistent at identifying suspected suicides however cases were filed quicker by the police. Bereaved individuals were more willing to share contact details and consent to referrals with police, which led to increased referrals. This research highlighted a need to look at components of successful postvention services, such as referral sources and collaboration.
McDaid et al. (2008) conducted a systematic review into the interventions for adults and children bereaved by suicide. They included support groups, self-help, volunteer-led groups and therapeutic interventions led by health professionals. This study exclusively included randomised controlled trials and studies with a control or comparison group such as cohort studies. Eight studies were identified, none being UK-based. Findings suggested that when compared with no intervention, there was evidence of effectiveness for four sessions of cognitive-behavioural family interventions with a psychiatric nurse. They also found that a psychologist-led 10-week bereavement group intervention was beneficial for children. Finally, an 8-week group therapy delivered by a mental health professional or volunteer was beneficial to adults. They concluded that all but one study had “substantial methodological limitations”.
More recently, Andriessen et al. (2019) conducted a systematic review into the effectiveness of interventions for people bereaved through suicide. The studies included (n = 11) were controlled studies of grief, psychosocial and suicide-related outcomes. The inclusion criteria included: study population consisting of people bereaved by suicide, studies needed to provide empirical data on grief, mental health and/or suicide-related outcomes, studies involving a controlled intervention and finally, studies needed to have been published in a peer-reviewed journal. This review excluded studies without a control group, case studies and review papers. No qualitative studies met the inclusion criteria. Location of origin included USA (n = 8), the Netherlands (n = 3), Australia (n = 3) and Belgium (n = 3). Across the studies, intervention modalities vary. The quality of studies was weak as evidence of the effectiveness of complicated grief interventions was lacking. The diversity of intervention settings, populations and measures used contributed to the overall quality of the studies. Furthermore, the studies had limited replicability and none of the studies looked at suicidal behaviour as an outcome. Studies that did have an interview follow-up period utilised short time points. Studies had small sample sizes, were female dominated samples, and it is unknown if studies controlled for effects of other treatments. This review highlighted concerns of selection bias, blinding and high withdrawal and dropouts as the weakest components across the studies. However, there was some evidence of the effectiveness of interventions for uncomplicated grief (Andriessen et al., 2019).
The majority of postvention research is conducted elsewhere in the world, and rarely conducted in the UK despite multiple postvention services supporting people bereaved by suicide in the UK, suggesting a need for postvention research in the UK. Two studies highlighted that mixed methodology studies were more effective in identifying insights through qualitative interviews that cannot be discovered using quantitative methods (Jordan, 2001; Jordan & McMenamy, 2004). Quantitative methods are limited in teasing out how contexts of postvention impact the outcomes. Qualitative methods, specifically the phenomenological approach, which seeks to understand the lived experience of the respondents, are inherently designed to assess a phenomenon in its natural setting and context (Moustakas, 1994). Andriessen & Krysinska (2012) posed essential questions on suicide bereavement and postvention and conclude that “the voice of survivors should be included in public health policies related to suicide prevention as well as involved in design and implementation of postvention programs and studies” (p. 29). Therefore, conducting a systematic review that considers non-controlled studies that assess the effectiveness of suicide bereavement support interventions is crucial. This will help to determine whether a non-controlled approach yields stronger quality of studies that also allow us to gain insight into the experience of being bereaved by suicide, creating services that provide a good standard of support. No recent reviews have included non-controlled and qualitative studies.
This systematic review has two aims, firstly to assess research which evaluates postvention services supporting those bereaved by suicide and secondly it aims to assess the acceptability of methods of postvention in terms of community support, peer support, group support and internet support.
The objectives in this review are to: 1. Identify and assess international research which evaluates postvention services and methods of postvention 2. Examine evidence for suicide postvention services that aim to prevent suicide 3. Examine and identify outcomes used to evaluate the effectiveness of suicide postvention services 4. Identify components of effective suicide postvention services
Method
Review Questions
1. How do suicide postvention services support those bereaved by suicide? 2. What outcomes are used to assess the effectiveness of postvention services? 3. How effective are suicide postvention services in supporting those bereaved by suicide? 4. Can effectiveness of these services be measured and quantified?
Literature Search
Electronic databases were searched to identify relevant published studies that met the inclusion criteria for this systematic review. The databases included were: PSYCINFO, CINAHL, MEDLINE, Scopus, Web of Science, Science Direct, EMBASE, TRIP, Cochrane Library, AMED and Google Scholar.
General searches were then supplemented with more specific searches for postvention services or interventions. Lateral search techniques were then implemented to search through citations used in primary studies and other systematic reviews.
Search Terms
(1) Suicid* OR “taking your own life” (2) Postvention OR support OR counselling OR counseling OR “peer support” OR “support service*” OR “self-help group” OR “postvention liaison service*” OR liaison (3) Bereave* OR grief OR mourning (4) Effectiveness OR impact OR acceptability
Inclusion Criteria
Qualitative and quantitative peer-review studies. This included interviews, focus groups, intervention studies, and experimental designs and process evaluations. Studies focusing on suicide postvention were included. No geographical restrictions were applied. Postvention services offering support to adults and children were considered. Any relationship to the deceased was included, such as studies that evaluate services that offered support to any relative or friend. As those accessing support services may be experiencing mental health issues, studies including those individuals as participant groups were included. Studies were included if they reported on suicide postvention services and their effectiveness and the acceptability of a method of postvention. As the goal of most suicide postvention services is to prevent suicide, suicide-related outcomes were the primary outcome of interest, postvention studies will also be included if they measure other mental health or well-being change such as self-harm, psychological factors. Peer support groups were also considered.
Exclusion Criteria
Studies reporting on prevention services and therapeutic interventions were not included, as this review focuses on postvention services. Studies and grey literature written in other languages that had not been translated into English were not considered.
Comparator/Control
Some studies included within this review compared intervention outcome with a control group or treatment-as-usual, another intervention or no intervention group.
Screening
Electronic search results were downloaded into Microsoft Excel (n = 2808). Duplicates were then removed (n = 890). Titles and abstracts were screened against the inclusion criteria (n = 1918). Systematic reviews and policy/practice guidance documents were screened for primary studies. One researcher then screened full papers, with the rest of the research team screening 1/3 of the full papers each. Any disagreements at this stage were blindly assessed by a different member of the research team and discussed. Full papers were then screened (n = 315). The final number (n = 36) of studies included were then agreed upon, rejecting studies which were not written in English, evaluated counselling interventions and prevention services, and did not evaluate postvention support services (See Figure 1). At this stage, results were divided into papers which were evaluations of a specific postvention service, and papers which looked at the acceptability of methods of postvention. Flow diagram depicting the flow of information through the different phases of a systematic review.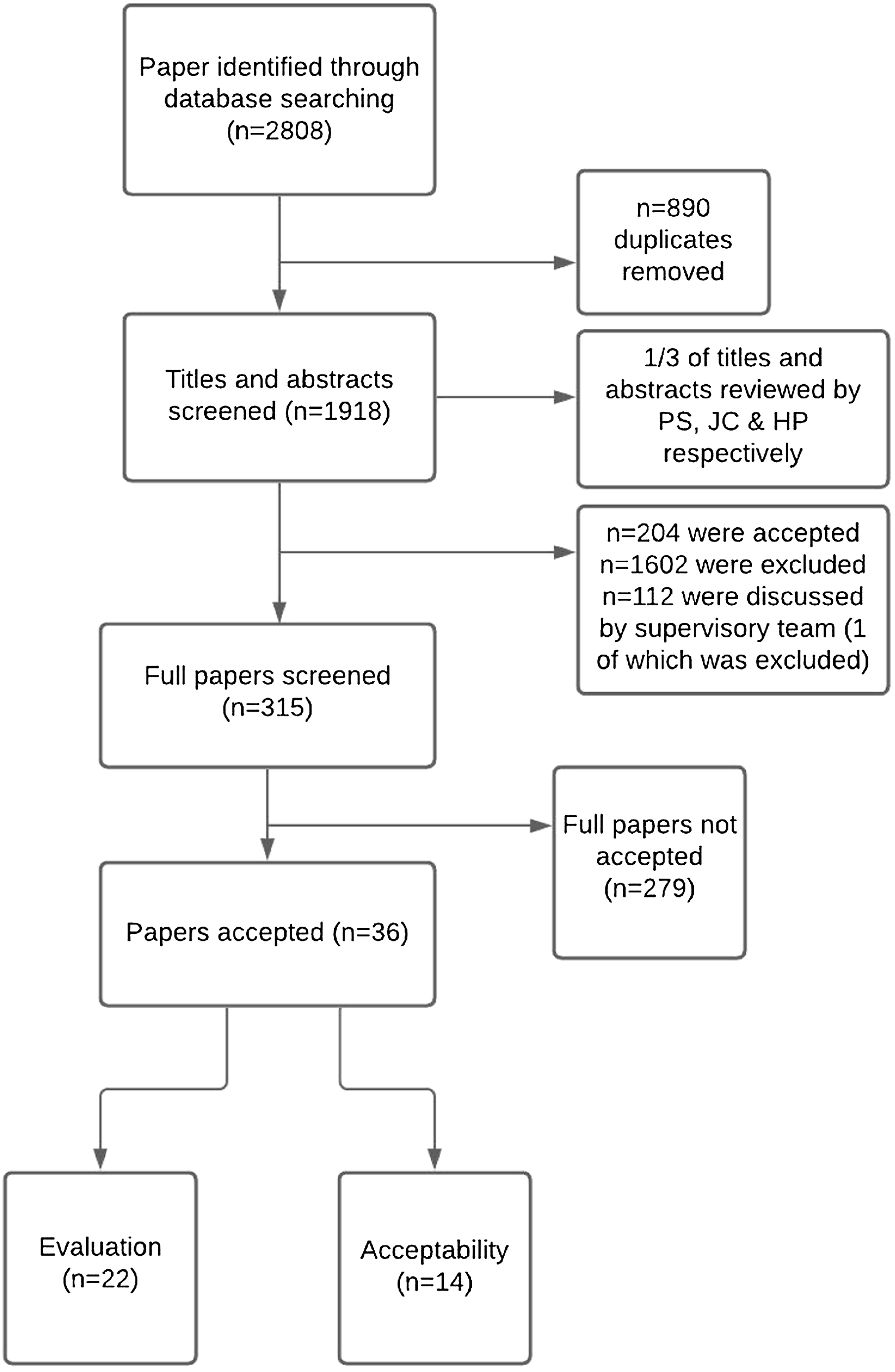
Data Extraction
Data extraction from all studies were conducted by the primary author to a Microsoft excel database. Study types were classified as: outcome evaluation, process evaluation, economic evaluation, methodological evaluation, intervention development, protocols, descriptive, qualitative studies, and systematic or literature reviews. The research team conducted a data extraction quality assurance check and 2/3 of the research team blindly rated 10% of evaluation papers and 10% of acceptability papers.
The data which was extracted from each study is highlighted below: 1. Study characteristics: Author, publication year, location of study, study design, age range of participants, gender of participants, time since bereavement and relationship to deceased 2. Intervention characteristics: Type of intervention, setting, characteristics of intervention, duration/frequency of contact 3. Study outcomes: Outcome measurement approach used (e.g., qualitative and/or quantitative), baseline mean (SD) for intervention group and any comparison group if used (e.g., control), endpoint mean (SD) for intervention group and comparison group if applicable (e.g., control group) and intervention effect as reported within the paper. Outcome measures and timepoints. 4. Secondary study outcomes/process outcomes: acceptability, feasibility and satisfaction
Strategy for Data Synthesis
Data was collected and analysed according to type of study design and outcomes. A narrative synthesis was conducted which included ‘evidence statements’ as this summarised the results of the studies taking into account the key issues relevant to the review questions.
Risk of Bias Quality Assessment
Methodological quality was evaluated by the primary researcher using guidelines stipulated in the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018). Two members of the research team then blindly assessed 10% of the papers in each group. Discrepancies from independent screening, data extraction, and quality assessment were resolved through discussion and where appropriate by a third reviewer within the research team.
Results
Thirty-six studies were included. These studies were then divided into (1) research evaluating specific postvention services (n = 22) and (2) research evaluating the acceptability of models of postvention (n = 14). From this point onwards, we will discuss the results of each of these categories separately.
Studies Evaluating Specific Postvention Services
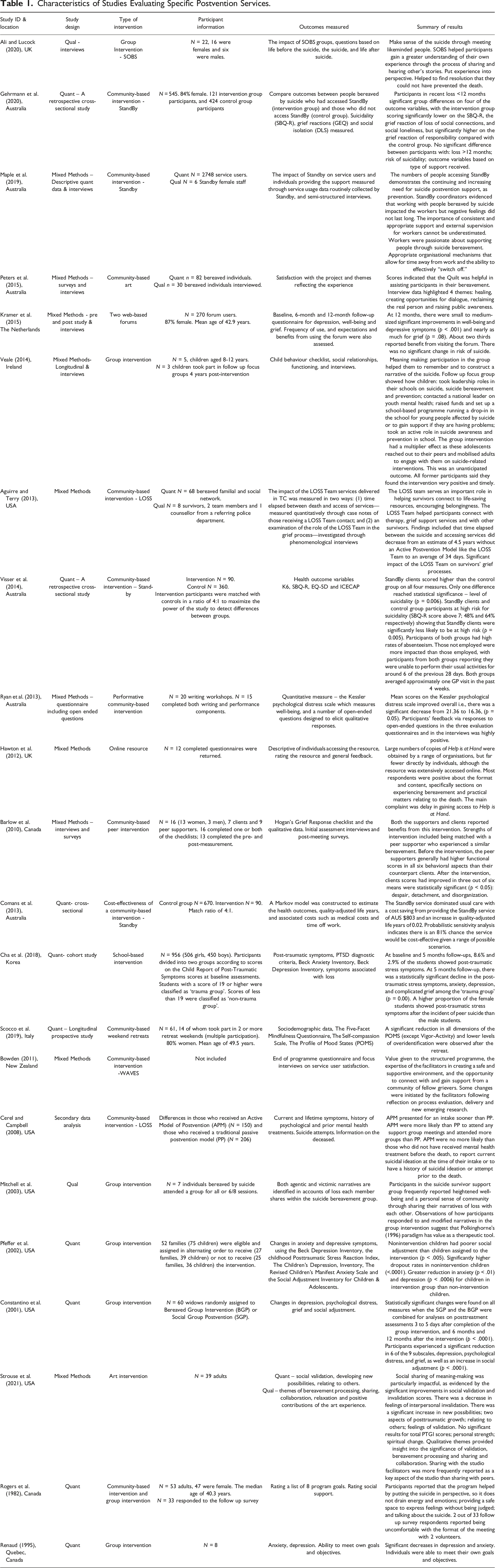
Characteristics of Studies Evaluating Specific Postvention Services.
Studies Evaluating the Acceptability of Models of Postvention
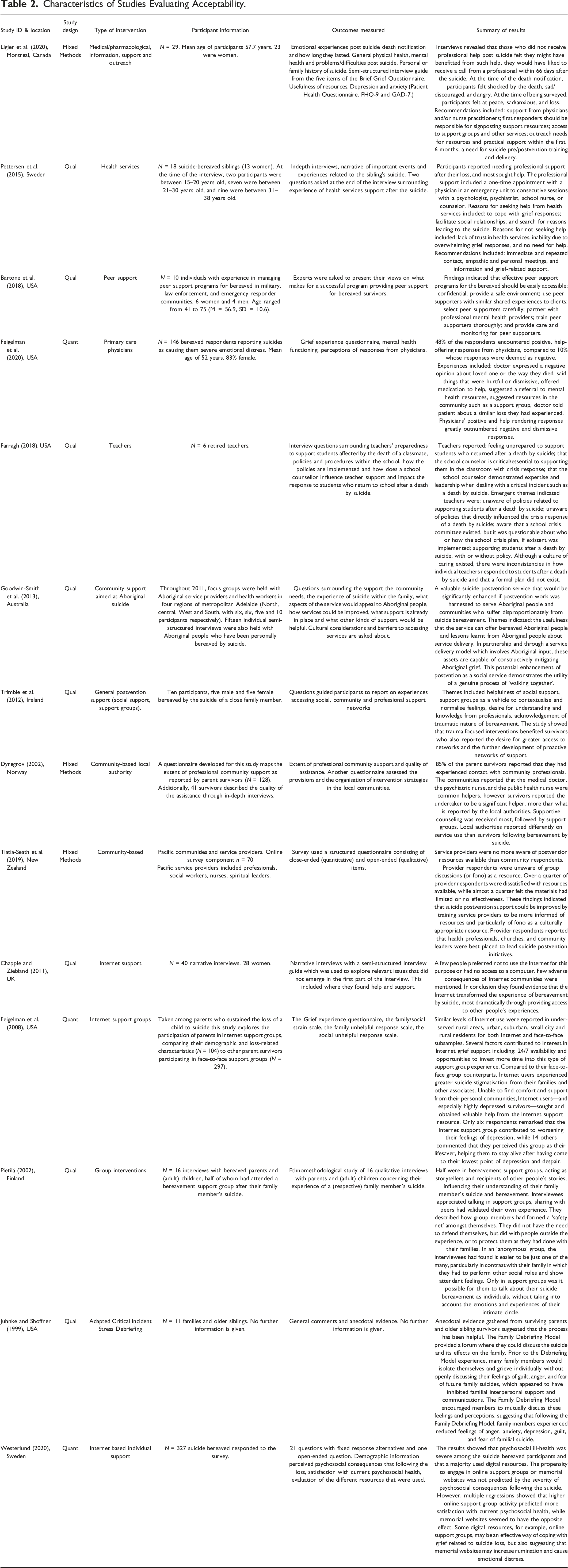
Characteristics of Studies Evaluating Acceptability.
Quality Assessment
Evaluating Specific Postvention Services
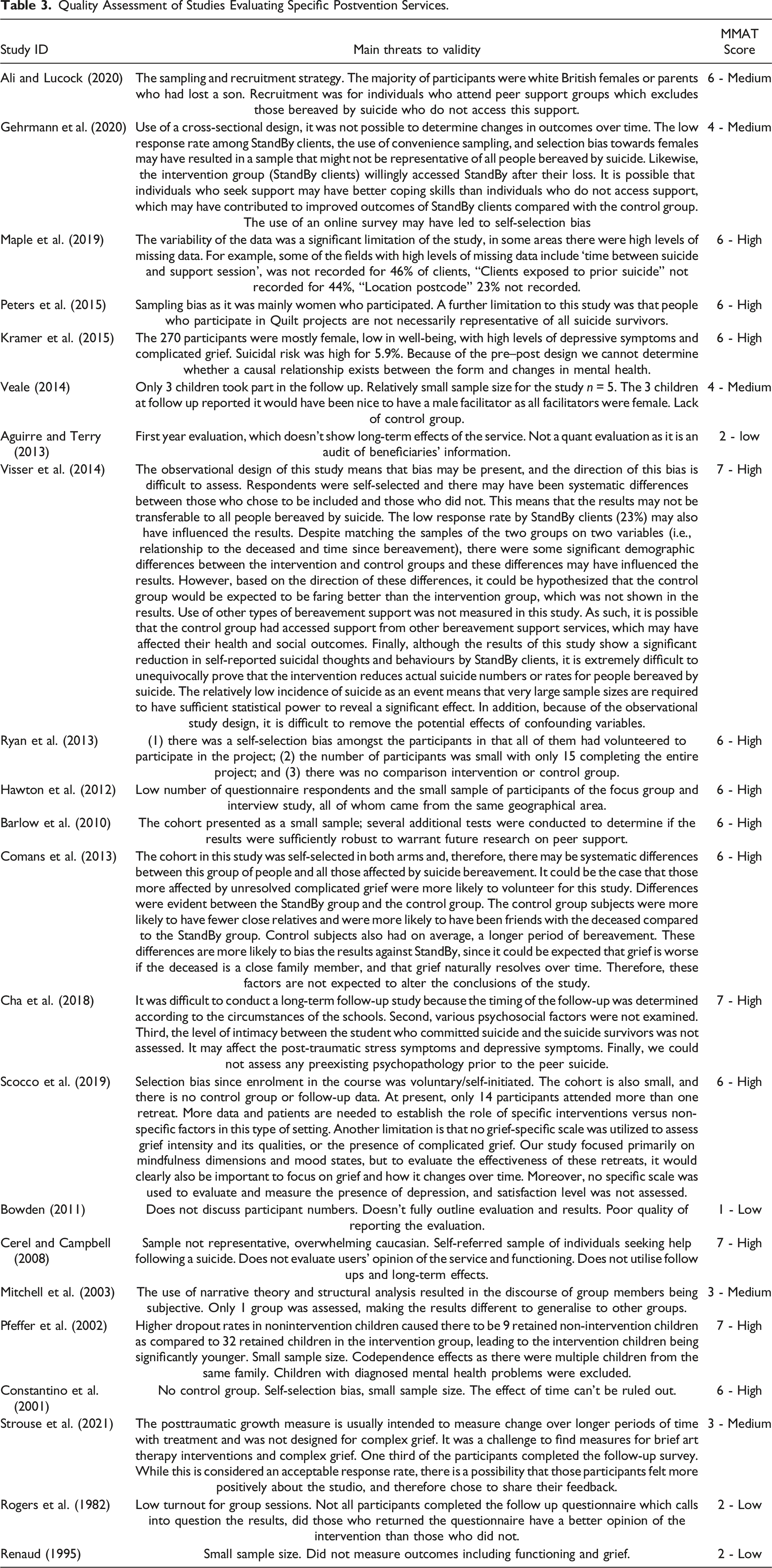
The quality of all the 22 studies was assessed using the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018), using the corresponding tool for the methodology of each study. Studies scoring 1 or 2 out of the 7 questions were rated as low quality. Studies scoring 3, 4 and 5 out of 7 questions were rated as medium quality. Finally, studies scoring 6 or 7 out of the 7 questions were rated as high quality (Hong et al., 2018).
Of the 22 studies evaluating a postvention service, four were rated as low quality (Aguirre & Terry, 2013; Bowden, 2011; Renaud, 1995; Rogers et al., 1982). This was due to studies not having explicit research questions and not clearly stating how the collected data addressed the research questions. The mixed methods study (Aguirre & Terry, 2013) did not adhere to the quality criteria for each tradition of the methods involved. Furthermore, it was difficult to assess whether there was an adequate rationale for using a mixed methods design and whether each component of the study was effectively integrated to answer the research question. The research questions were also unclear. The qualitative study (Bowden, 2011) was unclear in all questions relating to the qualitative methodology as it did not clearly state the evaluation aspect of the paper but was more of a descriptive paper on the service. The two quantitative papers rated as low (Rogers et al., 1982; Renaud, 1995) did not have a sample that was representative of the target population and had high nonresponse rates. There were five studies that were rated as medium quality. Two were mixed methods (Veale, 2014; Strouse et al., 2021) and they had issues in reporting on the risk of nonresponse bias, addressing the rationale for using a mixed methods approach and integrating the different components of the study effectively. Furthermore, inconsistencies between the quantitative and qualitative results were not discussed and the quality criteria for the qualitative methods was not wholly adhered to. One qualitative study was rated as medium quality (Mitchell et al., 2003) due to not clearly stating the research questions and whether the data collected would address the research questions. There was a lack of clarity as to whether the qualitative approach chosen and data collection methods were appropriate to answer the research question. One quantitative study was rated as medium quality (Gehrmann et al., 2020) due to incomplete outcome data, low response rate and the intervention group (n = 121) being significantly smaller than the control group (424). Finally, there were 14 studies assessing a postvention service that were rated as high quality; Six were mixed methods (Maple et al., 2019; Peters et al., 2015; Kramer et al., 2015; Ryan et al., 2013); Hawton et al., 2012; Barlow et al., 2012). They were rated because they had adhered to the quality criteria of both the qualitative and quantitative methods and integrated these aspects to address the research questions. There was also explicit and adequate rationale for using a mixed methods approach. Seven studies rated as high were quantitative (Cerel & Campbell, 2008; Scocco et al., 2019; Cha et al., 2018; Visser et al., 2014; Comans et al., 2013; Pfeffer et al., 2002; Constantino et al., 2001). One study rated as high was qualitative which evaluated the SOBS group intervention (Ali & Lucock, 2020). These studies met six or all the methodological quality criteria. The studies that met six of the criteria had some issues with confounding variables (n = 2; Scocco et al., 2019; Comans et al., 2013) and the sample was not representative of the target population (n = 1; Constantino et al., 2001).
Quality Assessment of Studies Evaluating Specific Postvention Services.
Quality Assessment of Acceptability of Models of Postvention.

Quality Assessments of Components of Effective Postvention Services
Where adequately reported in the studies, components of postvention services are discussed in this section. Group interventions such as Survivors of Bereavement by Suicide (SOBS) in the UK have been supporting people bereaved by suicide, offering peer-led support groups, a national telephone helpline, email support, online virtual support groups and online community forum. Ali and Lucock (2020) evaluated SOBS support group members who reported experiencing difficulties adjusting to the suicide, which motivated them to meet others in a peer suicide bereavement group who had shared a similar experience. This helped them to normalise their grief experiences and share ways of coping with the death. Veale (2014) evaluated a group intervention for children and found that groupwork enhanced connectedness, emotional expression, family communication, memory and meaning making. Groupwork also enabled active coping. Furthermore, measures of emotional and behavioural problems and social competence showed improvements 6 months post-intervention. Mitchell et al. (2003) also evaluated a group intervention for children and found that participants reported heightened well-being and a sense of community through sharing their narratives. These findings suggest that group interventions should attempt to foster the development of agentic narratives, rather than victimic narratives as this empowers the bereaved to feel in control. Pfeffer et al. (2002) studied children’s group intervention and reported that children who received the intervention had significantly lower scores for anxiety (p < .001) and depression (p < .006) than those who did not receive the intervention. Constantino et al. (2001) evaluated a group intervention for widows. When comparing a bereavement group postvention and a social group they found that when these interventions were combined, significant changes were found on all measures, seeing an improvement in 6 of the 9 grief subscales, depression (p < .0001), and psychological distress (p < .0001). There was also a significant improvement in social adjustment. (p < .0001). Another study looking at adults participating in a support group (Renaud, 1995) found that there was a significant decrease in depression (p < .001) and situational anxiety (p < .001). Rogers et al. (1982) evaluated a community and group-based intervention and found that participants reported that the intervention helped by putting the suicide into perspective as it provides a “safe space” to talk about the bereavement without feeling judged.
Four studies rated the Standby service in Australia which is a community postvention service. Gehrmann et al. (2020) found that participants with a bereavement in the last 12 months who received the intervention had significantly lower scores in suicidality, experience a loss of social support and social loneliness compared to those who did not receive the intervention. However, participants who received the intervention whose bereavement was more than 12 months showed no significant difference, suggesting that it is crucial for postvention support to be timely. Maple et al. (2019) found that postvention workers believe that appropriate and timely support reduces the negative effects associated with suicide bereavement. They also state the importance of maintaining their own well-being through external supervision. Visser et al. (2014) compared those who received the intervention with those who did not and found that Standby improves well-being across four measures. It also significantly reduced suicidality. Those that received the Standby intervention had significantly less healthcare usage than those in the control group, suggesting that Standby is effective in improving well-being and may also be cost-effective. Comans et al. (2013) found that Standby was far more cost-effective than usual care with a cost saving of $803AUS and an increase in quality-adjusted life years of 0.02. Probabilistic sensitivity analysis indicated there was an 81% chance the service would be cost-effective. However, none of the other studies were evaluated in terms of cost-effectiveness, this is the only cost-effective evaluation included in this review.
The LOSS service based in the US, a community intervention was evaluated by Aguirre and Terry (2013), and they found that the service helped them to feel supported and create a community around themselves, by connecting them with resources and other bereaved people. Furthermore, Cerel and Campbell (2008) found that those receiving the support were more likely to access additional support such as support groups. Bowden (2011) evaluated the Waves service, a community-based intervention in New Zealand and reported that participants find the features of the intervention “highly valued”, however this study was rated as low in quality as it did not outline any participant information, methodology or results.
Barlow et al. (2010) evaluated a Canadian peer support intervention and found that peer supporters can be effective in supporting people recently bereaved. This study also assessed the functioning of the peer supporters as well as the clients. Peer supporters had higher levels of premeasurement functioning compared with the clients, suggesting that peer support can be delivered effectively by trained individuals who have grieved sufficiently in order to support others. Scocco et al. (2019) found that weekend retreats reduced all dimensions in the Profile of Mood states, suggesting that these can be beneficial to individuals bereaved by suicide. School-based interventions may also support younger people bereaved by suicide. Cha et al. (2018) found that at 5 months follow-up there was a significant decrease in post-traumatic stress symptoms, anxiety, depression and complicated grief in the ‘trauma’ group.
Art and performative postvention support were also represented in this review. Peters et al. (2015) found that the quilt project was helpful in assisting participants in their bereavement by giving them an opportunity to reflect and grieve without fear of negative social reactions. Participants rated themselves as having high satisfaction with the project. Ryan et al. (2013) found that a writing and performative postvention improved psychological distress. Participants gave highly positive feedback in interviews. Strouse et al. (2021) found that art can enable meaning-making as supported by significant improvements in social validation and invalidation scores. Qualitative themes highlighted the significance of validation, specifically, bereavement processing and sharing and collaboration. Participants reported that sharing with the studio facilitators was more frequently reported as a key aspect of the studio than sharing with peers.
Non-face-to-face support was also represented in this review. Resources given to those bereaved by suicide to provide information and practical support may alleviate associated anxieties concerning the legal process that occurs when there has been a death by suicide. Hawton et al. (2012) evaluated a UK online resource, Help is at Hand and found that organisations were more likely to access the resource than bereaved individuals. Participants reported that the overall format and content of the resource was appropriate. Web-based forums may also be effective in supporting people bereaved by suicide. Kramer et al. (2015) evaluated two sister forums, one in Belgian and one in Dutch and found that at 12 months there were significant improvements in grief, depression and well-being. Two thirds of participants reported some benefit from using the forums. These studies suggest that online resources can be useful in supporting people bereaved by suicide.
In summary, these findings suggest that postvention support for individuals bereaved by suicide is effective in reducing various health and psychological outcomes associated with being bereaved by suicide. One of the significant findings is that a mechanism that seems to be most effective is for suicide bereaved individuals to have some kind of access to others, creating a sense of community and belonging around themselves. This may be through peer support, group support, contact with those previously bereaved by suicide who are now in a supportive role or indeed through trained postvention support workers. Studies have also shown that postvention can be cost-effective in monetary value but also in psychological facts and life expectancy.
Quality Assessments of Components of Effective Models of Postvention
There is an ongoing debate as to which model of postvention would deliver adequate postvention support. Andriessen et al. (2019) defined suicide postvention service model as a “coordinated approach to providing support to people impacted by the death of a family member, friend or person in a network (such as a school, nursing home, workplace, etc.) through suicide.” Questions surrounding who should deliver and how services should be delivered are discussed. Health services delivering postvention support may be suitable. Ligier et al. (2020) found that individuals bereaved by suicide who did not receive professional help from health care professionals felt that they may have benefitted from such support. On average, participants received a call from a health care professional within 66 days of the suicide. Pettersen et al. (2015) reported reasons for seeking help from health services in Sweden was to cope with grief, facilitate social relationships and search for meaning making. Reasons to not seek help from health services included the lack of trust in health professionals, incapability due to grief responses and no experienced need for help from health professionals. This study concludes that health services should offer immediate and repeated contact, empathy, personal meetings, information and grief-related support. Feigelman et al. (2020) found that nearly half of participants received positive support and responses from physicians. However, a small number of respondents reported doctor expressed a negative opinion about the deceased, doctors expressed a negative opinion about the way they died, doctors said things that they felt were hurtful or dismissive. Over half reported that their doctor offered medication to help deal with the loss. 48% reported the doctor suggested a referral to mental health resources and 34% stated doctors suggested resources in the community such as a support group. These studies suggest that support from health services could be of benefit. However, attempts should be made to improve the experience of those seeking support from health professionals to ensure that suicide bereavement support is sensitive to the needs of those bereaved.
Peer support models may also be beneficial. Bartone et al. (2018) found that effective peer support programs for the bereaved should be confidential and easily accessible interventions that provide a safe environment. Interventions should employ peer supporters with similar shared experiences to clients but should also select peer supporters carefully and ensure that peer supporters are trained. Professional mental health providers should also be involved in peer support. Peer support should also provide care and monitoring for peer supporters.
Farragh (2018) assessed teachers' ability to support children experiencing the suicide of a classmate or friend within the school community. This study found that teachers feel unprepared to support students and felt that school counsellors were critical or essential in supporting teachers as school counsellors had expertise in this area. Teachers interviewed in this study reported that they were unaware of school policies in dealing with student suicide and were unsure who or how the school crisis plan was implemented. Teachers felt that they supported students as best as they could, suggesting they wanted to be of support but felt that school response plans were inconsistent. Therefore, it may be reasonable to suggest that teachers could be supported by other professionals when a suicide occurs in the school community.
Goodwin-Smith et al. (2013) aimed to understand how postvention could support Aboriginal individuals bereaved by suicide in Australia. Results suggested that Aboriginal people should be involved in service delivery to demonstrate “walking together”. This suggests the importance of models of postvention involving the very community that they support in order to maximise effectiveness and service delivery. Tiatia-Seath et al. (2019) assessed the needs of pacific communities and found that service providers were no more aware of postvention support available than community members. The majority of service providers were unaware of group discussions (known as fono by this community). 25.9% of service providers were dissatisfied with resources and 23% felt the materials had limited or no effectiveness. These findings suggest that communities would benefit from working with service providers who provide culturally appropriate support. Service providers felt that health professionals, churches and community leaders were best placed to lead postvention in this community.
Furthermore, Trimble et al. (2012) found that individuals bereaved by suicide valued the helpfulness of social support and saw support groups as a vehicle to contextualise and normalise feelings. There was a desire for understanding and knowledge from professionals and an acknowledgement of the traumatic nature of bereavement by suicide. This suggests that models of postvention may be most beneficial when they include peer support, group intervention and intervention from professionals. Furthermore, Dyregrov (2002) found that 85% of parents bereaved by suicide had received some kind of support from professionals. Community professionals believed that medical doctors, psychiatric nurses and public health nurses were common supportive professionals. However, individuals bereaved by suicide felt that undertakers were significant helpers, which was not reflected in community professionals’ beliefs. Supportive counselling was most often received and provided for, as reported by 80% of the bereaved and 86% of the local authorities. However, only 26% of the parent survivors had participated in support groups, whereas 40% of the local authorities reported to have such group. The study concluded that local authorities lack the ability to fulfill expectations of those bereaved by suicide.
Web-based models have been evaluated, with Chapple and Ziebland (2011) finding that a minority of people had no access to a computer or preferred not to use the internet in this way. However, few adverse effects of internet support were found and there was evidence that the internet could be beneficial. Furthermore, Feigelman et al. (2008) found that internet support was utilised to similar levels by those in urban, cities and rural areas. Factors which users found to be beneficial were that internet support has no time constraints as it is constantly accessible, there are also opportunities to meet face-to-face. Out of 104 participants, only 6 experienced worsening depression due to internet support. However, internet support users felt greater stigmisation than those accessing face-to-face support. Furthermore, Westerlund (2020) found that higher online support use was related to more satisfaction with psychosocial health. However memorial websites did seem to have the opposite effect as participants had increased rumination. This study suggests that online support groups may be an effective model, however memorial websites may cause further emotional distress.
Pietilä (2002) found that half of participants had participated in support groups which enabled communication about the suicide and influenced meaning-making. Participants reported finding benefit from group participation as it helped to normalise their experiences. Anonymous groups were found to be easier and more accessible than family support, with the ability to be honest and talk openly most valued by users.
Juhnke and Shoffner (1999) evaluated using a model known as Adapted Critical Incident Stress Debriefing. However, as this study uses general comments and anecdotal evidence, there is insufficient empirical data to suggest acceptability of this model of postvention and therefore, we cannot determine whether this model to be effective in supporting those bereaved by suicide.
In summary, models of postvention should involve the community they serve, and be timely and culturally appropriate. Successful models include community-based support which could utilise peer and professional support. Group postvention models may also be effective in creating a community around bereaved individuals, enabling them to talk about their grief without being judged and normalising their experiences. Internet support may also supplement this but may not be suitable for everyone. For young people, school-based models may be effective to address bereavement in the school community.
Discussion
To our knowledge, this review of postvention services is the first to include non-controlled and qualitative studies within the analysis. The aim of this systematic review was to assess research which evaluates postvention services supporting those bereaved by suicide. Secondly it aimed to assess the acceptability of methods of postvention in terms of community support, peer support, group support and internet support.
This review showed that evaluations on specific postvention services were mostly rated as medium or high. Successful evaluations on effectiveness and cost-effectiveness included the Standby service in Australia, SOBS groups, the LOSS service, art projects, online forums and the Help is at Hand online resource. Ongoing evaluation of postvention services would enable the services to continue offering a good standard of care for beneficiaries. This supports Andriessen et al.’s (2017) findings that postvention research should be theory-driven and increase intercultural collaboration. Resources made available to individuals bereaved by suicide may be beneficial to alleviate some of the anxieties caused by the legal process which concurs with Jacoby’s (2002) findings that individuals bereaved by suicide felt highly distressed by legal procedures, specifically the coroner’s office and the inquest. Similar levels of distress were caused by the media reporting of their loved one’s suicide and postvention services should address these experiences. Therefore, providing practical and informative support may be a valuable part of any postvention service.
Postvention research reviewed in this paper rarely included experts, professionals working in suicide and those bereaved by suicide using qualitative methods. It would be beneficial for further research to assess the effectiveness of suicide postvention support services to assess both the professional and peer support provided to those bereaved by suicide. Using qualitative evaluation methods will enable those bereaved by suicide to explore their experiences and needs. This review also reported that models of postvention services should include community-based interventions and group interventions, which could be supported by online interventions. Young people and school communities would also benefit from support within the school environment. Andriessen et al., (2019) recommended that a public health model of postvention can allow for a tailor-made approach to service delivery and meet the needs of bereaved individuals. They suggest that models can range from information and awareness-raising targeting all people bereaved by suicide to specialised psychotherapy for those bereaved people who experience high levels of grief and symptoms of poor mental health. This also supports Ali and Lucock’s (2020) recommendations that services should be tailor-made and flexible in the timing and duration. Furthermore, Campbell (1997) suggested that adequate and early postvention services may normalise the grief process after suicide, identify more at-risk survivors, and reduce the risk of further suicides. Campbell (1997) suggested that an active model of postvention rather than a passive one would improve outcomes for those bereaved by suicide. It concludes that increasing access to support through community postvention services, the impact of postvention services can facilitate the grief process while providing information about resources in the community. The long-term consequences of suicide may be averted if the problems of access to services and awareness of resources could be overcome. Dyregrov (2011) recommended that postvention support should adapt to meet each individual bereaved person’s needs and therefore, any postvention model should include support that meets the needs of the community it supports.
This review highlights the lack of evaluations on UK interventions, with only two services included in this review; one on the effectiveness of the SOBS groups and another on the Help is at Hand online resource. There has been little to no research completed on the effectiveness of postvention services, with Australia and the US leading the way on postvention services evaluations. Furthermore, limited research has been done on the acceptability of models of postvention.
Some issues were highlighted by this systematic review. Firstly, it highlighted n = 4 postvention evaluation studies and n = 1 acceptability paper was poorly conducted and discussed. Studies were rated as poor due to not having clear research questions and it being unclear if the data collected could address the research aims. To address this, the author of this review also considered papers which did not have research questions but did have clear aims. Due to this, one paper was rated high rather than medium (Ali & Lucock, 2020). Furthermore, MMAT ratings indicated a distinct lack of rationale for using mixed-methods design, and where rationale was given, this was often unclear. Furthermore, many mixed methods studies did not adhere to the quality criteria for each tradition of the methods involved. Therefore, many mixed-methods papers were rated lower. One study rated poorly was a debriefing model of postvention (Juhnke & Shoffner, 1999). This study was a qualitative study which did not provide enough of a rationale and outline adequate evidence for the acceptability of such a model. Much research has been conducted on debriefing professionals when they experience a suicide in their professional capacity, however very little research has been done on the acceptability of debriefing suicide bereaved individuals. Therefore, this review cannot conclude that this model would or would not be of benefit and further research would need to be done.
Some services had many evaluations, in the case of Standby, four evaluations of their service were included in this review. This may be simply because they could have the resources or funding to have ongoing evaluation, thus proving their effectiveness. Other services may be just as effective, but we have been unable to evidence this. One reason for this may be due to inadequate reporting, for example, the WAVES evaluation, was rated as poor due to not adequately outlining research aims and methodology. Therefore, it may be that the WAVES service is a successful service, but the paper outlining the service has been rated as poor due to the quality of the research paper. Other services may have found it difficult to access funding or resources for evaluation.
Other issues reported were incomplete data sets and groups being incomparable at baseline. Some studies had low retention rates and small sample sizes. Samples were overwhelming Caucasian women in most of the papers discussed in this review. There was also self-selection bias in many of the studies, as evaluations focused on individuals who were supported by the services and had volunteered to participate. Therefore, individuals who took part may be the most satisfied with their experiences with the service. Some studies had multiple intervention arms but no control groups. (Scocco et al., 2019; Constantino et al., 2001; Ryan et al., 2013). Furthermore, some studies with control groups were matched 4:1 and were significantly different in ages and other factors (Visser et al., 2014: Comans et al., 2013). However, it is important to note that this review aimed to evaluate qualitative and mixed methods postvention evaluations as the author aimed to determine whether a non-controlled approach would yield stronger quality of studies that also allowed us to gain insight into the experience of being bereaved by suicide, creating services which are providing a good standard of support. As such, concerns about quantitative studies were expected.
Studies were rated using MMAT scores, which has different questions for studies with the following methods: qualitative, quantitative randomised controlled trials, quantitative non-randomised, quantitative descriptive and mixed methods. For mixed methods studies, to answer the final question, the rater must complete the questions for both components of the mixed methods (for example, qualitative and quantitative non-randomised). The questions are different for each method. Therefore, some studies may have confounding variables or a sample which is non-representative, if the questions for that method do not feature those criteria, this study will have been rated higher. The researchers have endeavored to discuss that in the reporting of the studies. Furthermore, the ratings were based on three answers; “yes”, “no” and “can’t tell”, for example, if the researchers could “not tell” if confounders were accounted for in the design and analysis of a qualitative non-randomised study, this was rated the same as if the study did not account for confounders. Therefore, studies where there was no clear discussion on the corresponding criteria were rated the same if they did not include this information. The extent to which a study was reported with clarity was crucial. However, it was felt that due to the wide range of methods, using one peer-validated tool to assess the studies would be beneficial.
Future Research
Future research should focus on longitudinal studies to evaluate the services’ longitudinal effectiveness. Studies with appropriately matched control groups would enhance research evaluating postvention services. Finally, more resources should be made available to services to enable them to evaluate effectiveness and ensure the longevity of services that prove to be effective in supporting people bereaved by suicide.
Supplemental Material
Supplemental Material - Evaluating Postvention Services and the Acceptability of Models of Postvention: A Systematic Review
Supplemental Material for Evaluating Postvention Services and the Acceptability of Models of Postvention: A Systematic Review by Laura Abbate, Jennifer Chopra, Helen Poole, and Pooja Saini in OMEGA - Journal of Death and Dying
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.