
Abstract
In this photovoice study, we explored how people with multiple sclerosis (MS) experience living with and managing invisible symptoms in daily life. Twelve people with MS produced digital images over a 2-week period to capture their experiences of invisible symptoms. Participants then discussed their images in semistructured interviews. We thematically analyzed the interviews and developed three main themes that encompass the difficulties around conceptualizing invisible symptoms and the conflicts of legitimacy this presents for people with MS, in which the reality of their invisible symptoms is invalidated by others and sometimes for themselves. Participants navigated these issues in dynamic ways, choosing to fit their symptoms to their lives or make space for their symptoms depending on the context, often influenced by a desire to “stay invisible” or to “be seen.” We highlight clinical implications for supporting people with MS around the legitimacy conflicts they experience and how they negotiate living with invisible symptoms.
Multiple sclerosis (MS) is a multifaceted, chronic, and often progressive disease of the central nervous system, characterized by an abnormal immune-system response and damage to nerve fibers and myelin sheaths. The demyelination of axons causes cognitive, affective, sensory, and motor impairments for people with MS, which significantly affect their lives (Yorkston et al., 2001). These impairments are classified into symptoms that are “visible” (e.g., easily discernible issues, such as mobility problems) and “invisible” (Fenu et al., 2018).
Invisible symptoms of MS are largely defined in the research literature as symptoms that are difficult for others to notice as debilitating and appear “hidden” to the onlooker (Stuke et al., 2009; Werfel & Trettin, 2020; White et al., 2008). Invisible symptoms commonly cited in the literature include cognitive impairment (e.g., memory problems), fatigue, pain, bladder and bowel dysfunction, sexual problems, and sensory dysfunction such as numbness, tingling, and issues with vision (Fenu et al., 2018; Kratz et al., 2016).
Fatigue is the most common invisible symptom (experienced by up to 75% of people with MS) and is reported to have significant detrimental effects on daily functioning (Induruwa et al., 2012; Kos et al., 2007). Fatigue is also the most commonly researched invisible symptom of MS (Krupp et al., 2005). Pain, neurogenic bowel dysfunction, and cognitive impairment are also among the most commonly reported; the latter affects up to 60% of people with MS (Amato et al., 2013; Norton & Chelvanayagam, 2010; Svendsen et al., 2005).
Research articles, journalistic pieces, and patient accounts highlight the various ways that invisible symptoms affect the lives of the people who experience them. Green et al. (2017) investigated the relationship between symptom severity and perceptions of health (physical, mental, and social) in 1,865 outpatients. Invisible symptoms of MS (i.e., pain, fatigue, and cognitive impairment) were predictive of negative health perception. Pain was the most predictive even when compared with visible symptoms. The authors concluded that invisible symptoms of MS are as important to the individual’s sense of well-being as visible symptoms and that given the association between negative health perception and mortality rates in people with MS (Assari, 2016), the long-term impact of living with invisible symptoms should not be underestimated. Another study found that invisible symptoms were more predictive of health distress than visible symptoms, and the authors suggested that people with invisible symptoms required adequate support with these (White et al., 2008).
The UK MS Society (2017) published an edition of their periodical Research Matters that focused on invisible symptoms of MS and their distinct impacts that differed from the experience of visible symptoms. A patient-produced brochure from the United States titled But You Look So Good! included a selection of quotes from people with MS communicating the psychological distress of living with invisible symptoms (National MS Society, 2016). Both publications referred to patients’ experiences of stigma related to their invisible symptoms, including perceptions of not having a “real” illness, social isolation, reduced confidence in own perception of symptoms, and discouragement from help seeking. Qualitative studies have emphasized stigma in MS in general; specific themes have described a lack of understanding and validation from others around invisible symptoms (Cadden et al., 2018; Grytten & Måseide, 2006; Turpin et al., 2018). In one study, participants reported purposefully concealing or disclosing their MS to influence judgment in their social encounters, although this was a study inclusive of but not specific to invisible symptoms (Grytten & Måseide, 2005).
Our metasynthesis of 17 qualitative studies relating to lived experience of “invisibility” in MS revealed numerous negative impacts (Parker et al., 2021). The invisible nature of people’s symptoms was highlighted as distressing and for some, the most challenging part of having MS. People with MS often did not feel understood or believed by others in relation to their invisible symptoms and felt their social, physical, and emotional needs were often invisible, too, as a result (Parker et al., 2021). The metasynthesis showed that invisible symptoms, by nature, offered people a choice of strategies to navigate the invisibility but confronted them with a burdensome dilemma of disclosing their symptoms to others and making their needs known or remaining invisible and maintaining a sense of control over their illness identities (Parker et al., 2021). Although the metasynthesis uncovered some understanding about the notion of invisibility in MS, the studies included did not primarily focus on the experience of invisible symptoms. The metasynthesis highlighted a need for focused exploration of people’s experiences of living with invisible symptoms and to better understand the ways in which people with MS manage these.
Studies suggest that many people living with invisible MS symptoms strive to find adaptive ways of managing them through developing strategies and using available resources (Norton & Chelvanayagam, 2010; Stuifbergen & Rogers, 1997). Many of these studies have focused on practical management of symptoms rather than elucidating the way in which people navigate the psychological and social impacts that are a prevalent part of living with invisible MS symptoms.
The majority of studies investigating the impact of invisible symptoms of MS have focused on individual symptoms in isolation (Kratz et al., 2016; Olsson et al., 2005). There is a dearth of original empirical research offering an in-depth exploration of lived experience of a cluster of invisible MS symptoms (which often is the case because people with MS experience multiple symptoms; Kratz et al., 2016). Furthermore, previous qualitative research in this area has solely used interview and focus-group methods, with limited participant cocreation and interpretation of data. There appears to be an absence of participatory visual approaches to MS research—an approach that has been reported to create a rich understanding of the experiences present in health populations (Topcu, 2015). No studies have used visual methodologies with people with MS despite evidence to suggest the benefits of these approaches (Glaw et al., 2017).
Our main aim was to obtain an in-depth understanding of people’s holistic experiences of living with invisible symptoms of MS and gain insight into the ways people manage and navigate their lives in the context of their invisible symptoms, offering a rich account of this through visual methods. In addition, we aimed to determine to what extent the data fit with Parker et al.’s (2021) conceptual framework around the notion of invisibility in MS.
Transparency and Openness
Preregistration
This study was not preregistered.
Data, materials, code, and online resources
The anonymized final study data will be available from the corresponding author on reasonable request.
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Ethical approval
Ethical approval was obtained from L.-S. Parker’s academic institution and the National Health Service (NHS) Research Ethics Committee for East Midlands-Derby (19/EM/0196).
Method
Design
We used a visual method commonly referred to as “photovoice,” whereby participants produced their own digital images to capture their (typically in-the-moment) experience of invisible symptoms of MS. In photovoice, photographic images are created during the research process by the participants and used as a point of discussion in interviews to uncover corresponding and related narratives (Foster-Fishman et al., 2005). “Photovoice” no longer is one specific method, but more akin to a general approach to providing a voice to different groups of people while simultaneously providing a means for collecting research data. We used the photovoice method developed by Wang and Burris (1994), which does not involve analysis of the photos themselves but only of the narratives of the people who took them. Therefore, analyzing the photos themselves is not a typical feature of photovoice because they are a means to discuss a particular event, feeling, or thought expressed through a participant’s photo. This is sometimes referred to as “photo-elicitation.” Photovoice offers the means for participants to capture and reflect on their experiences and for key messages related to health issues to be communicated to health-care providers, stakeholders, and policymakers (Wang, 1999). Visual methods are considered complementary to participatory approaches, allowing researchers to become immersed in the world of the participants through the production of real-time, real-world data (Schwartz, 1989).
Indeed, in a condition like MS with attendant cognitive problems (especially memory problems), in which “un-cued” recall is a challenge, a method like photovoice offers participants a means to compensate for their cognitive difficulties—especially when it comes to recall of what can sometimes be vague, diffuse, or esoteric symptoms. The process of taking the photographs would cue them to think about their invisible symptoms, and the photographs themselves would facilitate recall, which is often affected in MS (Collier, 1957; Rao et al., 1993). Photovoice has been successfully used in MS research to explore carers’ experiences in relation to quality of life (Topcu et al., 2021) and as an exploratory tool to elicit experiences of invisibility in Parkinson’s disease (Roger et al., 2018).
Patient and public involvement and engagement
We consulted members of a local MS patient and public involvement and engagement (PPIE) group on the initial study protocol and incorporated their feedback into the study design. A PPIE member became a part of the research team and was involved at every stage of the research process.
Epistemological position
We adopted a critical-realist position, which assumes that underlying unobservable processes cause real effects (Harvey, 1990). When applied to the present project, we assumed that there is an objective and physical reality to invisible symptoms but that participants’ experience of their symptoms is interpreted subjectively and is constructed by the participant in collaboration with the researcher. Our critical-realist position therefore has influenced the way in which we have understood or interpreted the data and how we have approached our analysis of these data. For instance, we began with a view (based on our knowledge of previous research, Parker et al., 2021) of this issue under investigation but were able to shape and reshape this view in light of the data and the subsequent analyses we performed. Our critical-realist position is also evident in our explicit articulation of our theoretical framework and how we were able to critically appraise (and reformulate) this with the data and the analyses this study afforded.
Participants and recruitment
Advertisements were placed in local MS Society newsletters and social media pages, in a UK NHS MS outpatient service, and in a local MS PPIE newsletter. Opportunistic sampling was used with a maximum variation sampling frame in an attempt to increase diversity across the sample in relation to age, gender, ethnicity, and MS subtype. A recommended number of participants for using photo production and elicitation is seven to 10 (Wang, 1999). For qualitative research using thematic analysis, it was found that 12 interviews were enough to reach 92% saturation of the data, in which subsequent analysis generated no new themes (Guest et al., 2006).
We required participants to be age 18 years and over, have a diagnosis of MS and experience or have experienced one or more invisible symptoms of MS, have access to an electronic device with a camera function (e.g., smartphone, tablet) or digital camera, and be able to use this device to take an image. Once eligibility to participate was confirmed, participants were informed of all aspects pertaining to participation and were sent an “information pack” before giving consent to participate. Participants were made aware of their right to withdraw from the study.
Procedure and data collection
Participants met with L.-S. Parker for an orientation meeting and were provided with further guidance about the study processes. The information they received included a list of common invisible symptoms of MS, however, participants were advised that they could self-define invisible symptoms based on what this term means to them individually. Participants were asked to use their own electronic devices to take a minimum of five images that they felt captured their experiences of living with and/or managing their invisible MS symptoms. We set this minimum because we felt it would give us sufficient scope to discuss various aspects of daily life without making the process too burdensome for our participants.
Participants were asked to send their images to L.-S. Parker by their choice of multimedia message (e.g., text message), email, or secure encrypted WhatsApp message as soon as they could after taking the pictures. They were also requested to send a short narrative about what the image captured or represented. Participants were asked to take and send all images within a 2-week period. One week after the orientation meeting, L.-S. Parker telephoned each participant to offer support if needed and to identify any issues with participation. Two weeks after the orientation meeting, participants were invited to a semistructured interview with L.-S. Parker and to select five images to discuss at their interview.
The semistructured interview included inductive questions to elicit discussion about each image and its meaning for the participant. Once the five selected images had been discussed, all participants were given the opportunity to talk about any additional images they had taken. Interviews were audio recorded and transcribed verbatim by L.-S. Parker. The participants received a gift voucher with a well-known retailer for the value of £10 as an expression of gratitude toward their contributions.
Fourteen adults with MS volunteered and consented to participate, but two withdrew in the early stages, leaving 12 participants (age range = 30–57 years; 10 women). The mean time since diagnosis was 10 years (SD = 5.06), and 67% of participants had relapsing remitting MS. All participants were of White British origin, except one with White British/Swiss background (for demographic details of each participant, see Appendix A). Participants were asked for their preferred pronouns, which are used throughout this publication. Participants took 73 images; these were not used as data per se but, rather, to elicit discussion during the interviews.
Ethical considerations
Ethical approval was obtained from L.-S. Parker’s academic institution and the NHS Research Ethics Committee for East Midlands-Derby (19/EM/0196). Some participants opted to be referred to by their real names in the study, and others chose their own pseudonyms.
Data analysis
Analysis of the data (audio recordings, written narratives, and transcriptions) from semistructured interviews was led by L.-S. Parker in collaboration with the other authors, using an inductive-deductive thematic analysis (TA; Proudfoot, 2023). Guidelines provided by Braun and Clarke (2006, 2013) were used for the TA, outlining five phases of the process. First was familiarization with the data sets. L.-S. Parker read and reread the transcripts and made initial notes summarizing key ideas covered in specific phrases, sentences, or paragraphs, and these were shared with other members of the team for feedback on the initial analytic observations. Second was coding, which was completed by L.-S. Parker and second-checked by the other members of the research team. Third was generating initial themes. L.-S. Parker completed this initially by organizing the codes into broader features that represented patterns of meaning across the data. L.-S. Parker printed out each code, color-coded them for each participant, and organized them into piles according to similarities, overlaps, and salient features. These clusters of codes were then further grouped conceptually into areas of overlap, eventually developing themes, which were again discussed with the authorship team. Fourth was refining, defining, and naming themes. The initial set of themes was laid out on a large thematic map, which enabled the whole team to examine the “robustness” of each theme in terms of whether each conveyed a specific idea, the degree to which there was “spillover” between themes, and how the different themes related with each other. At this stage, the initial thematic structure that was being developed in the earlier stages was further tested in terms of completeness of the synthesis of the data related to the aims of the study and the narrative flow that the thematic structure afforded. Fifth and finally was writing. The authorship team worked together to determine how to convey the “story” we captured from the analysis, identifying specific illustrative quotes and contextualizing the analysis in terms of the extant literature. Data were first approached inductively (data driven and open to discovery of new knowledge) and secondarily using a deductive (theoretically driven) framework. The deductive framework (see Appendix B) was developed by drawing on the key themes and conceptual framework highlighted by Parker et al.’s (2021) systematic review of experiences of invisibility in MS.
We applied to this study Yardley’s (2000) guidance for good qualitative research. To improve rigor and credibility of the analysis, a third of the transcripts were cross-checked by other members of the research team for consistency of coding. In addition, the themes generated by L.-S. Parker were checked by all other authors in terms of the plausibility of all interpretations made. We discussed and resolved any discrepancies or queries in regular meetings. To ensure quality and transparency of study reporting, we used the Critical Appraisal Skills Programme (CASP; 2018) for qualitative research.
Reflexivity
We maintained an active process of critical reflection throughout this research. L.-S. Parker used a reflective diary to record and manage their subjective expectations, assumptions, and personal stances in relation to the research processes and data. This diary was shared with other members of the research team for further reflection and discussion of potential biases.
Positionality statement
L.-S. Parker is a 30-year-old White British woman whom at the time of the study was employed as a trainee clinical psychologist. They do not have a diagnosed disability or chronic illness. They have worked therapeutically with people who have long-term chronic physical-health problems and disability, some of whom described their symptoms as being invisible. Therefore, they approached the study with prior assumptions about the potential impacts of invisible symptoms more generally (e.g., people not being believed by others and the debilitating impact on daily living). L.-S. Parker had not worked with people with MS and held no specific assumptions about their experiences, but their expectations based on previous work could have influenced their interpretations, and reflexivity was important in monitoring and responding to this. L.-S. Parker had also spoken to people with MS and gathered anecdotal evidence around the impact of invisible symptoms and had expectations in terms of the output from their metasynthesis around invisibility and MS (Parker et al., 2021). They strove to attend to these assumptions throughout the research process through discussions with the research team. The research team comprised three White women and one Asian man. One of the women (C. Bale) lives with MS and was the PPIE lead for this project. The others had no lived experience of having a chronic illness or disability but had experience of working (as psychologists) with people with MS and other disabilities. C. Bale reflected on her own experiences in relation to the data, which helped us contextualize and interpret the data, but we ensured that her experiences were not included as part of the data itself.
Results
The inductive-deductive analysis led to the development of three main themes and eight subthemes. Inductive codes contributed to the construction of all themes, as did deductive coding, and these were synthesized. The resulting themes provided substantial support for our deductive framework and allowed us to uncover richer detail and explicate the processes that exist within the experience of living with and managing invisible symptoms. The themes outlined below are those that developed the framework further. The data were an almost perfect fit with the deductive frame, and one inconsistency is highlighted in this section of the article.
The challenges of conceptualizing the invisibility of symptoms
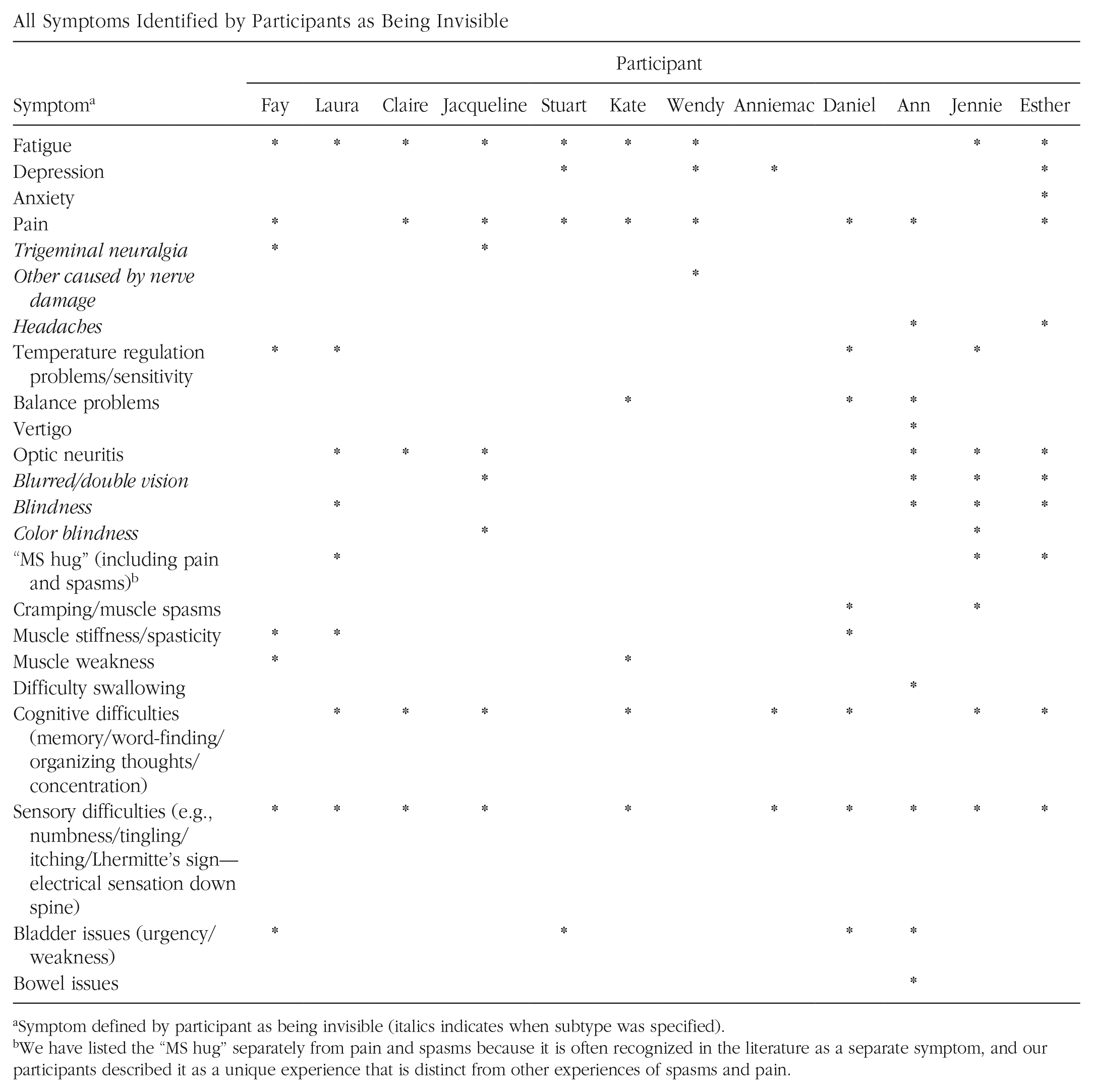
All participants described experiencing multiple symptoms of varying severity that they defined as being invisible in nature (outlined in Appendix C) and the challenges faced with when conceptualizing and discussing their symptoms because of their invisibility (Fig. 1).
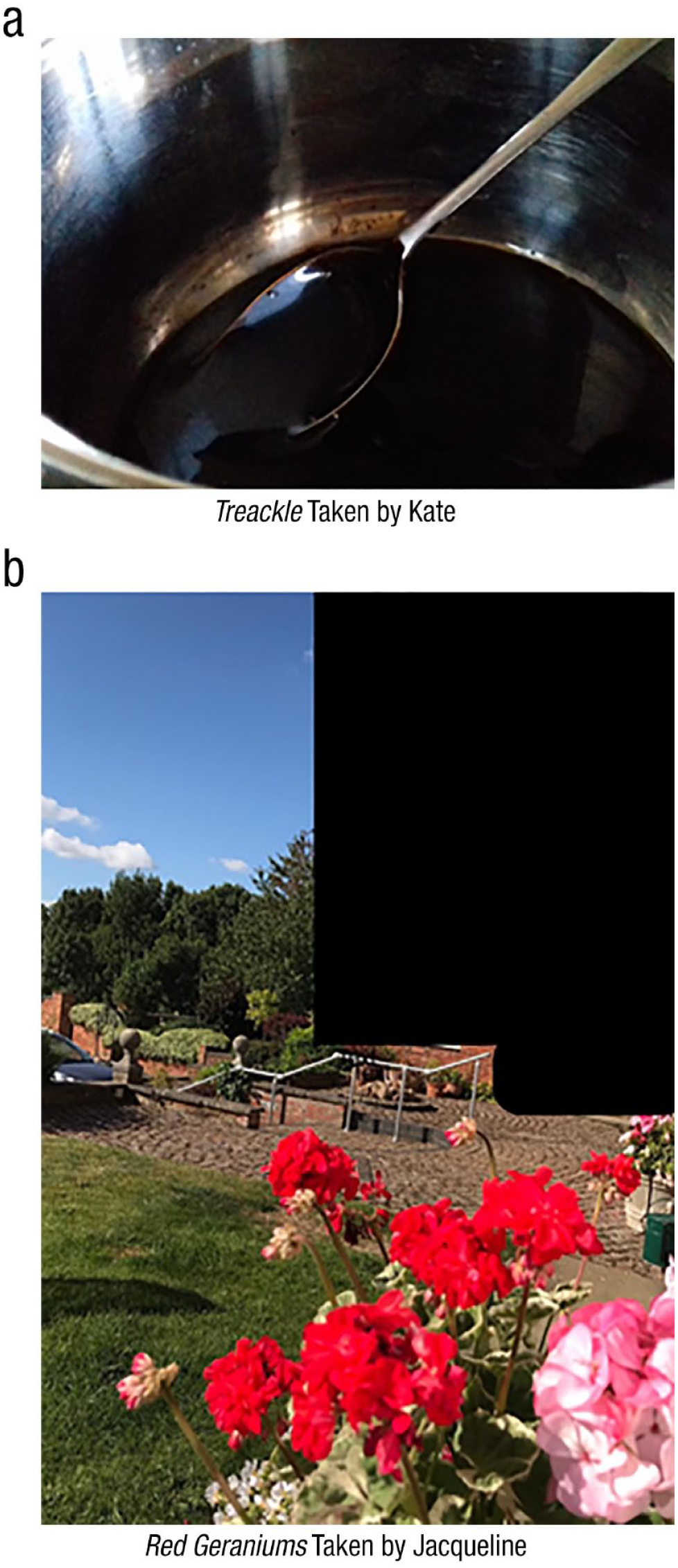
Photographs taken by participants denoting the challenges of conceptualizing the invisibility of symptoms.
Others’ blindness to my internal struggles
Invisible MS symptoms were conceptualized by all participants as a discrepancy between what they experience internally and what is observable externally. All described experiencing symptoms and internal struggles related to their symptoms that cannot be seen by others: It’s the invisible-ness of MS. Because most of it is internal . . . I can feel it, I know it’s there, but to anybody else, they can’t see it. (Fay)
For some, invisible symptoms were felt to be the most challenging aspect of their MS, even for individuals who experienced visible symptoms: The invisible symptoms that people just don’t know about. . . . They’re the ones that really get you . . . I struggle, as you can see with mobility. . . but it’s the invisible that I really struggle with. (Jacqueline)
Cannot be seen, cannot be spoken about
Participants described their symptoms as “strange,” “odd,” “weird,” “bizarre,” and “abstract” experiences and sensations, which are difficult to describe. Ten participants spoke about not having the language to communicate their invisible symptoms or explain them to others despite a desire to do so. This further compounded their sense of invisibility and the discrepancy between what is felt internally and what can be said about it: It’s trying to find ways to explain to people how you feel. That can be quite challenging. (Laura) Trying to put it into words sometimes can be a bit awkward. . . . Trying to explain to people, you just can’t. (Daniel)
Participants relied on a range of linguistic methods, including similes, metaphors, use of word emphasis, and sound effects, to attempt to communicate their experiences yet maintained a sense of being unable to translate their symptoms accurately and in a form accessible to others. Some images taken by participants represented their symptoms in abstract and metaphorical ways. For example, Kate demonstrated the heaviness and stiffness in her legs in her image (Fig. 1a): I often feel like I’m wading through treacle . . . your legs are really heavy. I feel like I’ve got big boots on and it’s real hard work. (Kate)
Jacqueline’s experience of trigeminal neuralgia pain was “indescribable,” so she made use of color in her image (Fig. 1b) to communicate this: The invisible is visible because that red . . . my goodness me . . . I just cannot describe the pain of neuralgia, I really can’t. It is so excruciating . . . like having electric shocks down your face. . . . And then [explosion noise] it really hits your face . . . Zzzz just going down, and it’s a raw red. (Jacqueline)
Participants’ accounts indicate that their invisible symptoms are not only experiences that cannot be seen but also ones that cannot be spoken about.
Conflicts of legitimacy
All participants discussed issues of conflict in relation to the perceived legitimacy of their invisible symptoms, grounded in the fact that they are not observable. We have understood these issues of legitimacy conceptually as epistemic and experiential such that participants struggle to validate the “realness” of their invisible symptoms to both themselves and to others and feel invalidated as a result (Fig. 2).
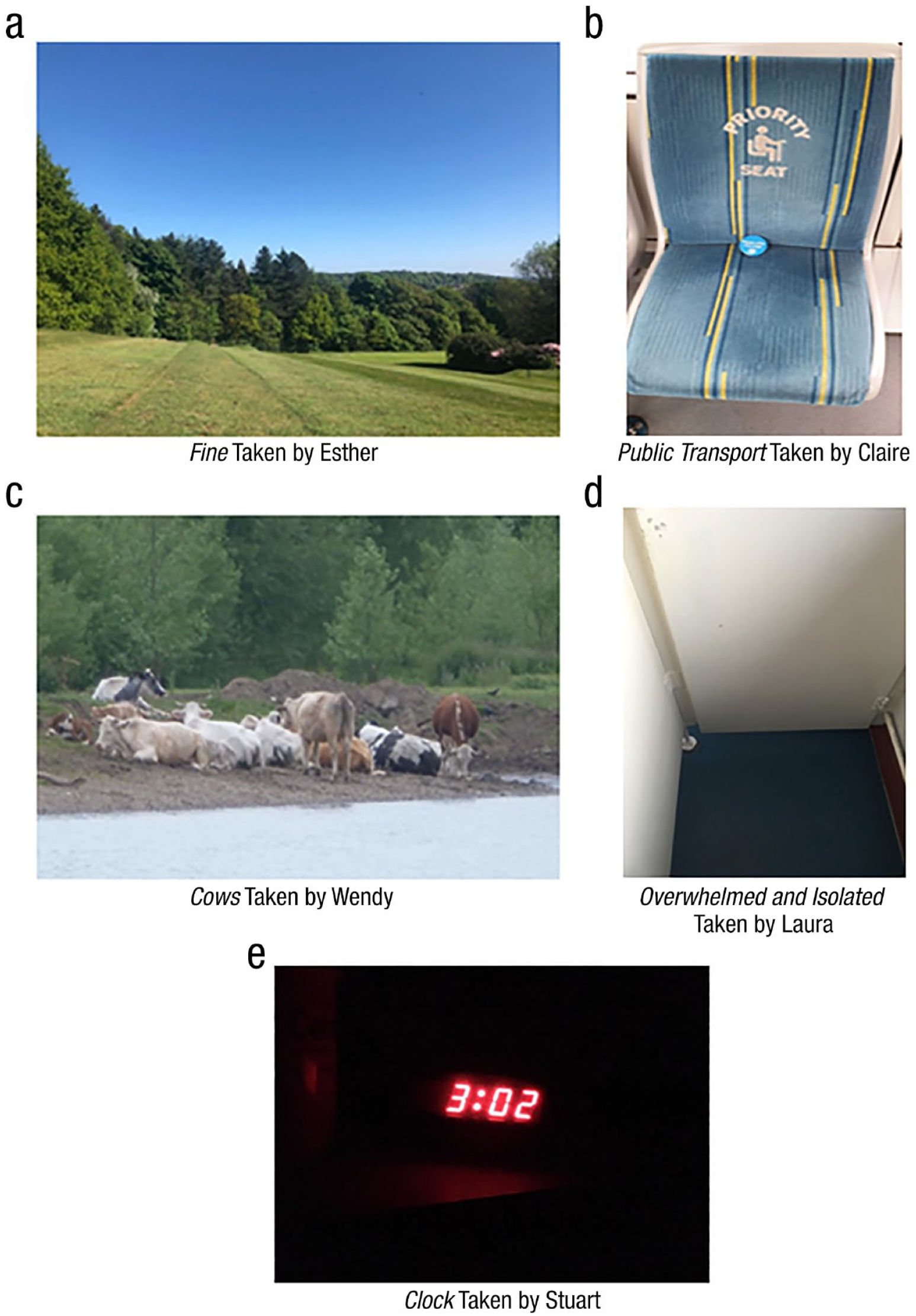
Photographs taken by participants denoting the conflicts of legitimacy.
An invisible reality (epistemic issues of conflict)
Participants highlighted epistemic issues created by the fact that their invisible symptoms cannot be clearly seen or communicated and the difficulty of validating the realness of their symptoms without external evidence of them to both themselves and others. Some participants spoke of the importance of their MRI scans in validating their symptoms by providing “objective” evidence of their reality. Esther felt it was important for clinicians to help people with MS to understand their MRI scans to validate their invisible experiences and believed the absence of MRI evidence could lead her to question the reality of her symptoms: It might help the patient to feel less like they’re going mad. . . . “Here it is, your MRI scan shows that yes you do have these symptoms.” . . . Because otherwise it’s just my word against anyone else’s . . . whilst I’m not making it up, it can feel like because it’s all hidden that it’s all just a figment of your imagination. (Esther)
Some participants described longing for a physical indicator of their symptoms to verify their invisible reality and resolve the legitimacy conflict: Why couldn’t I have just lost a leg or something? Because then if somebody asks what’s wrong with you, you just go “That’s what’s wrong with me” and it’s something you can see. (Stuart)
Laura discussed the difficulties of quantifying her invisible symptoms to others, which had an impact on deciding whether to “call in sick” for work. She worried that others would question the reality of her symptoms at work because she could not provide evidence of it as she would with “a snotty nose”: It’s so hard to measure [invisible symptoms]. . . . You can’t quantify how tired you are . . . I just couldn’t ring up and say, “I can’t come into work today because I’m fatigued or exhausted.” I would just make up an excuse and say I’d been [physically] sick. (Laura)
External invalidation (experiential issues of conflict)
Experiences of feeling dismissed, misunderstood, and invalidated by others in relation to their invisible symptoms were described by 11 participants, which brought the reality of their symptoms into question and worsened the legitimacy conflict. Esther spoke about people telling her that she did not look unwell, capturing this in an image of a seemingly “fine day” (Fig. 2a): People say to me “Oh you look fine though, even though you’ve got MS,” “Oh, but you look so well!” . . . People actually forget that I have MS . . . it can make people feel misunderstood and that you may even be fabricating the whole thing. (Esther)
Some participants believed invalidating reactions from others most often occurred in the absence of physical evidence for their symptoms. Claire spoke about her tram commute to work and her experience of others assuming that she does not need to use a disabled seat despite her internal struggle with fatigue. She denoted this with an image (Fig. 2b) of the disabled seat she often arrives deliberately early at her tram stop to ensure she can sit on: Anyone getting on the tram when it’s packed doesn’t see me as needing to sit in those seats . . . I sit in a disabled spot, but I don’t look disabled . . . you just hear people talking. . . . That picture’s showing someone with a stick needing a stick . . . whereas people need to sit on there that don’t have sticks. (Claire)
Claire observed that the “disability” image includes a representation of an “aid,” which clearly marks a disability, serving to further invalidate her hidden disability.
Participants discussed feeling validated about their invisible symptoms when speaking to others with MS, who have an understanding that people without MS cannot evoke. When Wendy’s friendships became strained because of their lack of understanding around her symptoms, she created new friendships with people she felt understood by (to see how Wendy conceptualizes her friends as a supportive “herd,” see Fig. 2c): I set out to make new friends through the MS society . . . you have quite a lot in common with them and can talk to them. It’s quite reassuring. (Wendy)
Some participants commented that their closest loved ones have tried to understand and have made conscious efforts to validate their experiences. Often, they have more of an understanding than the general public and at times even notice when the participants are struggling with symptoms. Although this does not fit with the deductive framework, these accounts were also accompanied by the commentary that despite the efforts of loved ones, participants still did not feel understood because of the invisibility of their symptoms. We therefore considered this to be inconsistent with the deductive framework to a degree but not refutational.
Participants questioned their own symptom legitimacy in response to their experiences with others, such as wondering whether their symptoms are “psychosomatic” and “mind over matter.” Participants described self-questioning whether they were “lazy” (when experiencing fatigue and depression), “dim” (cognitive issues), “fabricating” their symptoms, and “making excuses” for not doing things because of their symptoms.
The negative emotional impact of invalidation was highlighted, which could exacerbate the symptoms themselves. Laura captured an image (Fig. 2d) on a particularly challenging day at work, where she felt dismissed by her colleagues while struggling with invisible symptoms. She went to the staff toilets to cry when she took the image: I just found it really overwhelming . . . that lack of understanding from other people . . . when you’re trying your best and you’re trying to manage a condition, if someone says something quite out of turn and not very kind it has such a big impact. (Laura)
Stuart captured an image of his alarm clock (Fig. 2e) one night during which he lay awake worrying about his ordeal of being disbelieved by benefits assessors to grant him personal independence payments.
1
Others highlighted similar difficulties, compounded by the invisibility of their symptoms and pressure to “prove” the symptoms’ existence: They [benefit assessor] assessed me and said “That’s fine, we believe you.” . . . And then they reassess and go “Oh there’s nothing wrong with you.” . . . They go “Nah, there’s nothing wrong with you. Go back to work.” (Stuart)
Navigating life with invisible symptoms
We found that all participants negotiate their lives with invisible symptoms in dynamic ways dependent on their contexts and needs (Fig. 3). We identified that participants’ styles in doing so differed and were characterized by “pushing through” their invisible symptoms and trying to make the symptoms fit around their perceived lives, roles, and responsibilities. We also uncovered narratives around “making space” for and “accepting” their invisible symptoms, with participants organizing their lives around their symptoms. The approaches of pushing through and making space not only help participants to manage living with their invisible symptoms more generally but also have implications for the invisibility of their symptoms and the control the participants have over whether their invisible symptoms are made known to others (“being seen”) or kept hidden (“staying invisible”).
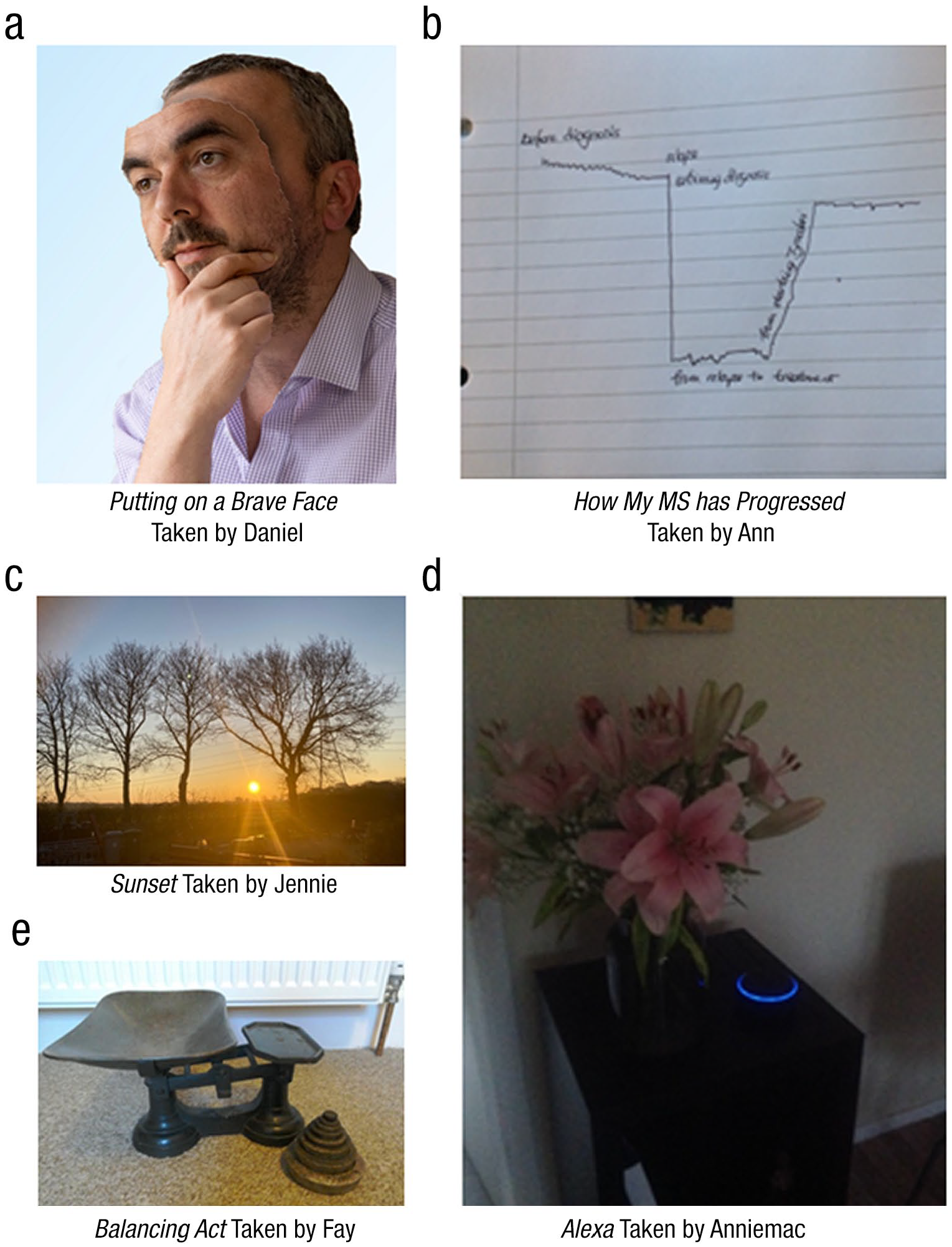
Navigating life with invisible symptoms. The participant gave written consent for this photo with their face in it (Fig. 3a) to be published, and it was covered in our ethics application.
Making symptoms fit to life
Eleven participants described trying to make their invisible symptoms “fit” to their lives, often characterized by pushing through and attending to daily tasks despite feeling unwell. Symptom invisibility often allowed participants to push through daily life undetected by others. Fay talked about needing to put her invisible symptoms “on the back burner” when she has responsibilities to consider: There are days where you have to forget the MS and really fight through things to get them done and be as normal as you can . . . times where being a mum has to take priority over how you feel physically . . . you have to do things that put you in discomfort because they are really important. (Fay)
Daniel is responsible for his team of employees and spoke about the “brave face” he puts on when he is struggling with invisible symptoms to maintain his managerial persona and avoid worrying others (Fig. 3a): I almost have to sort of put a brave face on . . . even when I am struggling I do have to come across as being my normal self, almost as though there’s nothing wrong . . . I’ve got to project to my staff that there’s nothing to worry about. . . . You don’t want people to see that you’re hurting. (Daniel)
For some, pushing the invisible symptoms from their minds was a way of managing the symptoms to get on with life: I try and push it away most of the time because I don’t want it to be there. It’s an annoyance, it’s an irritation, so why would I think about it more than I have to? (Jennie)
Making space for symptoms in life
All participant accounts supported this subtheme, describing how they have “made space” and adjustments in their lives for their invisible symptoms. Wendy spoke about being a “career girl” before being diagnosed with MS and having to adjust her lifestyle to accommodate her invisible symptoms: I figured I had to leave my old life behind and start a new one, because I couldn’t possibly have continued at the rate, the pace that I was living my life . . . I had to put my life into perspective and think about how I was going to manage. (Wendy)
Ann talked about how she changed her working patterns, stepped away from unhelpful relationships, changed her medication, and made conscious decisions to reduce the impact of various stressors on her invisible symptoms. She illustrated this in a graph (Fig. 3b) depicting her MS journey and how this steadily improved after making changes: I did various things to change the way I lived my life, and that really helped. (Ann)
Jennie described feeling as though “the sun was going down” on her life when she was diagnosed with MS (depicted in Fig. 3c); however, she has made and continues to make changes to her life to manage her invisible symptoms in a way that offers her a sense of agency. She reflected that this has helped her to manage the impact of her symptoms. I kind of preempted and got into a slightly different role . . . that was the main change I made. I wanted it to be my choice, and not something that was pushed on me or decided by the illness . . . that was my way of exerting control over it. . . you need to know how to plan around it. (Jennie)
As well as making larger life changes, participants also described a plethora of practical strategies they use to manage daily living with invisible symptoms. Anniemac spoke about the technology she uses to support her with invisible symptoms, including using an Alexa Dot device (depicted in Fig. 3d) to help manage cognitive difficulties: Alexa makes life so much easier. My MS brain struggles to organize! (Anniemac)
There was evidence for participants arranging their day-to-day lives around their invisible symptoms and of making mental space for the symptoms and accepting their impacts: It’s much better to embrace it . . . there’s no point ignoring it because it’s not gonna go away . . . let it be part of you but not the whole thing . . . it doesn’t define you . . . it doesn’t consume me like it used to. It’s part of me, I’ve accepted that. (Stuart)
Implications of navigation styles on symptom invisibility
This subtheme was supported by all participants. We found that the choice to either make space for invisible symptoms or fit them into life often had consequences for the invisibility of participants’ symptoms in terms of whether these remain hidden to others and stay invisible or are made known and result in being seen. These consequences were sometimes intentional and at times unintentional for the participants. Claire described her reluctance to stay home from work when she struggles with fatigue, instead choosing to push through undetected by others. This sometimes results in the exacerbation of her symptoms, and then her struggle becomes apparent to her colleagues: I wasn’t letting my team leader know that I was struggling . . . I was trying and trying and seeing how far I could go . . . I’ve been known to fall asleep at work . . . and the woman I usually sit next to, she’s like “I know when you’re ill.” And I’m like “Oh dear.” (Claire)
Making space for the symptoms by participants making their needs known sometimes had the outcome of helping their invisible symptoms to be acknowledged and understood to a degree by others. However, despite participants’ efforts to make others aware of their symptoms, sometimes, the legitimacy conflict keeps them feeling invisible and unvalidated.
Finding a balance on a double-edged sword
This subtheme explicates how participants choose the way they navigate their invisible symptoms by taking account of their context, needs, wishes, potential consequences for the invisibility of their symptoms (i.e., being seen or staying invisible), and the advantages and disadvantages of these outcomes. Participants described striving to strike a balance in life between pushing through symptoms and making space for them. Fay depicted this “balancing act” in Figure 3e by capturing a set of scales. The ability to be flexible in her approach across different situations helped with this balance: Everything is a balancing act . . . knowing what you can and can’t do . . . on some days the MS is gonna make the scales drop really low . . . and there’s gonna be days where you have to forget the MS and really fight through things to get them done and be as normal as you can. (Fay)
For many participants, their choices were influenced by the desire to maintain a sense of identity and not be defined by their MS and trying to balance this against their other needs and the impacts of their invisible symptoms. Stuart said his desire for others to be aware of his symptoms varied according to the situation: Sometimes you don’t want people to see but sometimes you just want to go “Look, that’s what it is” . . . depending on the situation . . . with my dealings with the DWP [UK Department of Work and Pensions] I’d like to be able to say “That’s what’s wrong with me” . . . but not necessarily day-to-day for meeting [other people]. (Stuart)
Although being able to choose a navigation style offered a sense of control for people over their invisible symptoms and how they present to others, many participants experienced this choice as a double-edged sword in which each choice has both costs and benefits. Jennie discussed this choice and the conflicts she experiences in daily life. By pushing through, she keeps her symptoms hidden from others; however, this puts her in a very “lonely place.” However, making space for the symptoms and making them known can lead to unwanted input and worry from those around her: I don’t know that I’d want everybody to see. Because you don’t want that feeling sorry for you. . . . But it can be quite a lonely place to be. Sometimes you want people to know what’s going on inside but other times you think “Actually no I don’t.” . . . That’s a bit of a frustration, not knowing where you want people to be in the situation. What do you want from them, what you want from yourself. . . . It’s sometimes really hard to know what you want . . . I don’t want people to judge me by what I’ve got, not what I am. (Jennie)
Participants were often caught in a conflict of their wish for the reality of their invisible symptoms to be validated and a desire to be treated as “normal” and no different to others.
Discussion
This photovoice study allowed us to explore and uncover people’s experiences of living with the invisible symptoms of MS and the ways they manage and navigate their daily lives in relation to these invisible symptoms. To our knowledge, this is the first study to use visual methodology to unpack the lived experience of invisible MS symptoms. Our findings were consistent with those of the recent metasynthesis (Parker et al., 2021) and provided us with rich information that allowed us to further elucidate and understand the implications of living with invisible symptoms and how people negotiate this. We have integrated our original framework (see Appendix D) with the findings from the present study and have outlined this as a conceptual framework in Figure 4. This is not intended as a theoretical model but, rather, an arrangement of the themes to better conceptualize them in relation to our research aims. The dashed lines in the framework represent links rather than implying linearity or causation.
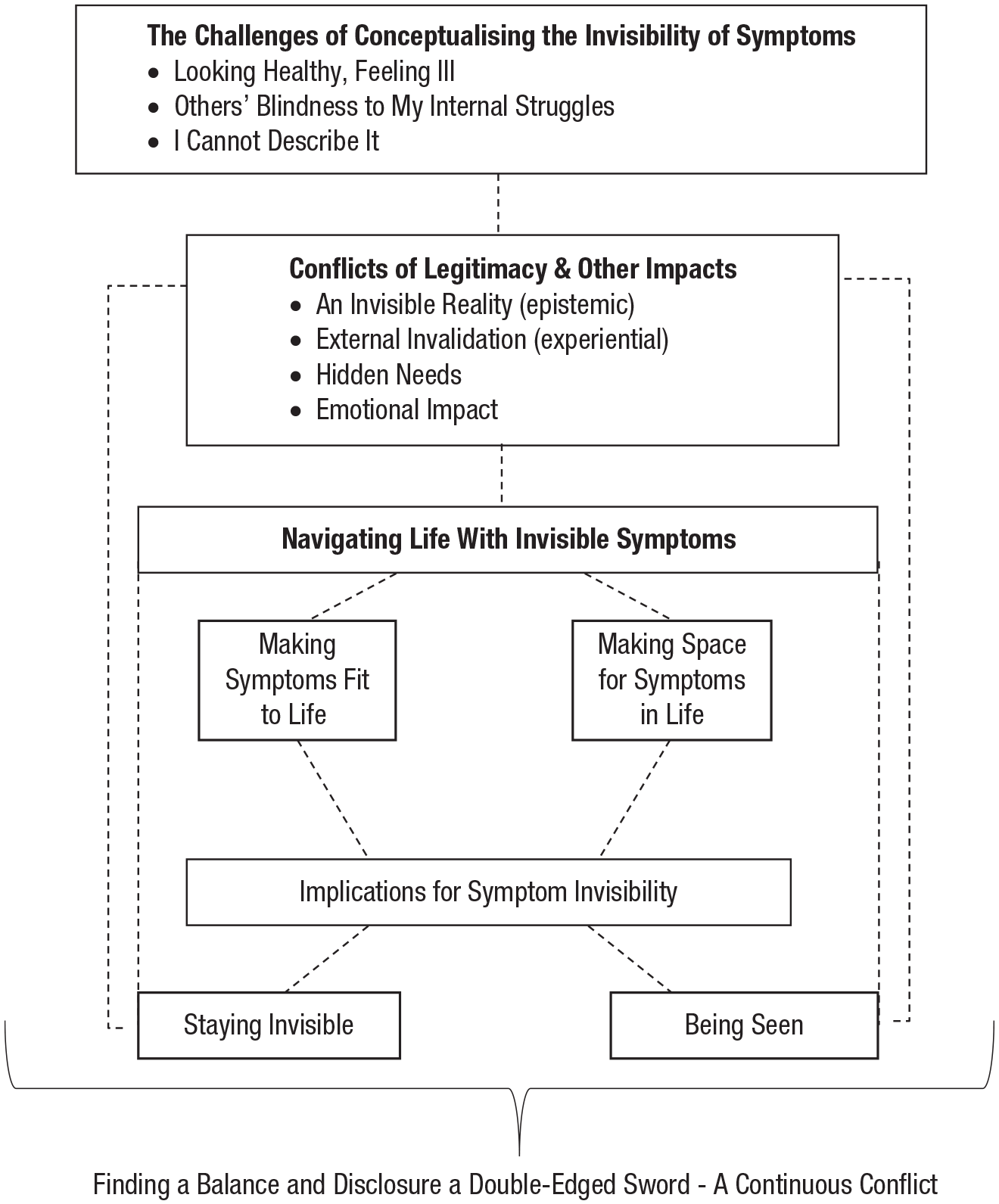
Conceptual framework to represent the relationship between themes identified from the analysis and the deductive framework from Parker et al. (2021). The dashed lines in the framework represent links rather than implying linearity or causation.
Invisible symptoms were conceptualized as a discrepancy between the struggle people with MS experience internally and what is visible externally to both onlookers and to the sufferers themselves. This is consistent with the available definitions in the literature and what has been expressed previously by people who experience these symptoms (Parker et al., 2021; Werfel & Trettin, 2020). Our findings expand on this and show the complexities of fully conceptualizing the invisible nature of people’s MS symptoms. This is due to the notion that not only can invisible symptoms not be outwardly seen by the person with MS or others but also that the language with which to communicate these symptoms is not available. Participants described sensory experiences without tangible, observable evidence, which feel so abstract that they cannot verbally explain these experiences accurately. This introduces a legitimacy conflict around the perceived realness of people’s invisible symptoms, in which people cannot validate the symptoms for themselves or communicate this to others, and the invalidating responses of others lead the person with MS to doubt the reality of their own experience of their symptoms. The lack of understanding from others compounded the invisibility of the needs of people with MS and the emotional impacts of their symptoms, worsening this legitimacy conflict. Our findings here support the existing evidence whereby people with invisible MS symptoms feel ignored and dismissed and question the validity of their lived realities (Cadden et al., 2018; Parker et al., 2021).
The way people with invisible symptoms navigated daily life had two key functions. One was the management of the physical experience of the symptoms themselves and being able to complete daily tasks more generally, and the other was navigating symptom invisibility and the legitimacy conflict this presents. The invisibility of people’s symptoms afforded them a choice as to how they navigated their lives not accessible for visible disabilities. We uncovered two key navigation styles whereby (a) people with MS tried to make their invisible symptoms fit into their lives and push through, almost as if to ignore their invisible symptoms, and (b) people with MS consciously made space in their lives for their invisible symptoms and reorganized their lives around symptom-related needs. This was true not only of the way they overtly behaved but also how they negotiated living with symptoms psychologically.
We learned that although some participants were more inclined to particular styles of navigating their lives, there was a general sense of striving to find a balance between pushing through and making space for their invisible symptoms, and participants often oscillated between these styles depending on the context and their evaluation of needs in a given situation. Participants weighed up the advantages and disadvantages of navigation styles by considering their perceived roles and responsibilities, personal values, and having a sense of control over the way in which they present themselves to and are perceived by others.
Participants expressed an awareness that their navigation styles in a given situation inherently influenced the degree of invisibility of their symptoms. Many participants described making active choices to directly influence their symptom invisibility and to be seen by making their invisible symptoms known to others or to stay invisible and continue to let their symptoms remain undetected. At other times, participants indirectly influenced their symptom invisibility as a result of pushing through or making space. We learned that the impact of people’s chosen navigation styles at times had both intentional and unintentional consequences on whether their symptoms were seen or remained invisible. For example, sometimes the approach of pushing through invisible symptoms proved effective in concealing an illness identity, but sometimes, it led to participants being unwittingly seen when the impact of their symptoms became apparent to others.
Many participants described trying to stay invisible and push through their invisible symptoms, particularly in workplace settings, which appeared to be motivated by a desire to protect the image they portray to the world and to avoid becoming associated with a pitied illness identity. Goffman (1963) and Charmaz (1983) theorized that people with disabilities inherit a stigmatized “spoiled identity” and loss of self that is shaped by other people’s (and general societal) responses to them. Two societal identities were suggested by Goffman: the “stigmatized,” who are dismissed and discounted, and the “normals,” who appear not disabled and are valued. Our findings are consistent with the conflict people with invisible symptoms of MS find themselves in, torn between being perceived as one of the normals and being insufficiently supported or understood or being one of the stigmatized. This conflict informs their choices as to how they navigate their invisible symptoms in daily life and within this, negotiate their identities.
The choice to try to be seen or stay invisible and to make symptoms fit to life or make space for symptoms while offering a sense of control and agency for people with invisible symptoms of MS was a source of conflict in which people strove to find a balance on a double-edged sword as they navigated their lives. This is consistent with our previous findings and those of chronic invisible illnesses (Parker et al., 2021; Vickers, 1997), in which choosing to be seen in an attempt to be validated also involves the risk of stigmatization but staying invisible can harm people’s psychological well-being through keeping their needs hidden—both compounding the legitimacy conflict that people with MS seek to resolve.
Implications
Our study provides insight into the challenges faced by people living with invisible MS symptoms and the ways they negotiate day-to-day living and their illness legitimacy and identities. It is important that clinicians and health-care professionals are aware of the conflicts created by symptom invisibility so that they can offer appropriate support to people with MS. It may also be helpful, given that many participants reported doubting the reality of their own symptoms, to acknowledge this and discuss the neurological evidence for the symptoms with patients to help them resolve the epistemic issues highlighted in our study.
Hayes et al. (2004) suggested that mental well-being and effectiveness in navigating life and its challenges centers around the ability to demonstrate psychological flexibility, which includes being able to contact the present moment, accept and make space for one’s experience and step away from avoidance of this, and act in accordance with one’s values. These are skills that can be developed to flexibly respond to challenging contexts (e.g., living with invisible symptoms) in a way that is consistent with what is important and meaningful to the individual. Acceptance and commitment therapy (ACT; Hayes et al., 2006) focused on supporting people to increase their psychological flexibility and has yielded some promising results in terms of improving psychological flexibility and reducing symptom distress for people with chronic, long-term health conditions (Graham et al., 2016). More specifically, ACT has been shown in some studies to be effective in improving quality of life and reducing psychological distress for people with MS (Barooti et al., 2019; Brown et al., 2016; Nordin & Rorsman, 2012). Although it is theoretically intuitive to suggest that improved psychological flexibility (through interventions such as ACT) could help people to navigate the invisible symptoms of MS, our study was not designed to explore this. To our knowledge, no research exists exploring the benefits of improving psychological flexibility through ACT with people who experience invisible symptoms of MS. ACT has been shown to reduce perceived stigma around pain as a symptom more generally (Scott et al., 2019); however, further research into how improved psychological flexibility could potentially support people with MS to navigate their invisible symptoms and the legitimacy conflict they present could have important indications for supporting people to live on the double-edged sword.
We found that photography facilitated the communication of invisible symptoms for people with MS and allowed people to voice these experiences, which are often difficult to describe. Using photography in the therapeutic context could possibly support people with MS to express their experiences and make meaning of these. Phototherapy has been linked with increased self-awareness and positive therapy outcomes (Saita & Tramontano, 2018; Stevens & Spears, 2009). Future research could explore the potential of using photo production in therapy with people who have MS.
Limitations and strengths
Although a range of ages between 30 and 57 years and a range of years living with MS were captured, the study has limitations in terms of demographic diversity of the sample, with there being no ethnic or cultural diversity among participants. In addition, we did not collect information on our participants’ income, education, or socioeconomic status. This allows for limited representation of the population group’s perspective and excludes the voices of people from other cultures and ethnic groups for whom the experience of living with and managing invisible symptoms of MS may differ or offer new insights.
Data in qualitative research are subject to the researchers’ interpretations, which are likely to be influenced by their expectations, experiences, and positions. We acknowledge that L.-S. Parker, who led the analysis, had their own expectations based around previous research they have conducted in the area of MS and invisible symptoms. Although we used a rigorous reflexive process, the interpretation of the data cannot be completely separated from the expectations and position of the researchers. We acknowledge the potential for confirmatory bias in our results as a possible limitation given that there was considerable overlap and fit with our deductive frame. Independent cross-verification of coding and themes and transparent discussions within the research team throughout analysis helped to mitigate potential biases and improved the credibility and reliability of our findings. We evaluated the study against quality criteria to ensure that our research met the standards of good qualitative research and reporting (e.g., CASP, 2018; Yardley, 2000).
Conclusions
Photovoice was shown to be a useful method in exploring people’s lived experience of their invisible symptoms of MS and how they manage these. We found that people with MS navigate their lives with invisible symptoms by managing not only the symptoms generally but also their invisibility. Evidence suggested that people with MS often have to make burdensome choices across a range of situations as to how they manage their symptoms, taking into account their needs and whether they wish for their symptoms to be known to others. Participants experienced conflict around these choices and valued the ability to respond flexibly to each context. Our research highlights the importance of supporting people with MS to validate their invisible symptoms and respond flexibly to the issues they present.
Footnotes
Appendix A
Participant Characteristics
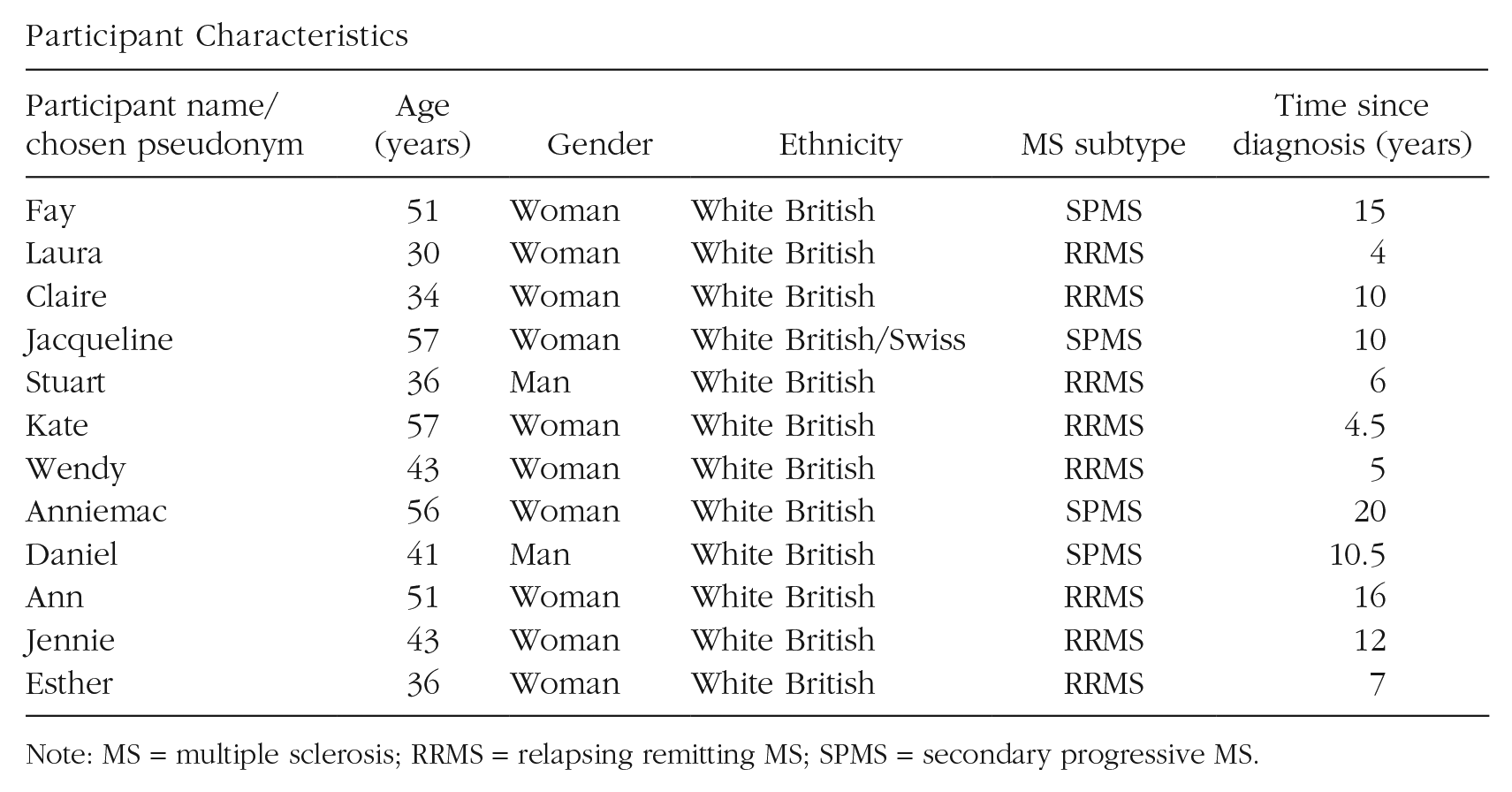
| Participant name/chosen pseudonym | Age (years) | Gender | Ethnicity | MS subtype | Time since diagnosis (years) |
|---|---|---|---|---|---|
| Fay | 51 | Woman | White British | SPMS | 15 |
| Laura | 30 | Woman | White British | RRMS | 4 |
| Claire | 34 | Woman | White British | RRMS | 10 |
| Jacqueline | 57 | Woman | White British/Swiss | SPMS | 10 |
| Stuart | 36 | Man | White British | RRMS | 6 |
| Kate | 57 | Woman | White British | RRMS | 4.5 |
| Wendy | 43 | Woman | White British | RRMS | 5 |
| Anniemac | 56 | Woman | White British | SPMS | 20 |
| Daniel | 41 | Man | White British | SPMS | 10.5 |
| Ann | 51 | Woman | White British | RRMS | 16 |
| Jennie | 43 | Woman | White British | RRMS | 12 |
| Esther | 36 | Woman | White British | RRMS | 7 |
Note: MS = multiple sclerosis; RRMS = relapsing remitting MS; SPMS = secondary progressive MS.
Appendix B
Appendix C
All Symptoms Identified by Participants as Being Invisible
| Participant | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptom a | Fay | Laura | Claire | Jacqueline | Stuart | Kate | Wendy | Anniemac | Daniel | Ann | Jennie | Esther |
| Fatigue | * | * | * | * | * | * | * | * | * | |||
| Depression | * | * | * | * | ||||||||
| Anxiety | * | |||||||||||
| Pain | * | * | * | * | * | * | * | * | * | |||
| Trigeminal neuralgia | * | * | ||||||||||
| Other caused by nerve damage | * | |||||||||||
| Headaches | * | * | ||||||||||
| Temperature regulation problems/sensitivity | * | * | * | * | ||||||||
| Balance problems | * | * | * | |||||||||
| Vertigo | * | |||||||||||
| Optic neuritis | * | * | * | * | * | * | ||||||
| Blurred/double vision | * | * | * | * | ||||||||
| Blindness | * | * | * | * | ||||||||
| Color blindness | * | * | ||||||||||
| “MS hug” (including pain and spasms) b | * | * | * | |||||||||
| Cramping/muscle spasms | * | * | ||||||||||
| Muscle stiffness/spasticity | * | * | * | |||||||||
| Muscle weakness | * | * | ||||||||||
| Difficulty swallowing | * | |||||||||||
| Cognitive difficulties (memory/word-finding/organizing thoughts/concentration) | * | * | * | * | * | * | * | * | ||||
| Sensory difficulties (e.g., numbness/tingling/itching/Lhermitte’s sign—electrical sensation down spine) | * | * | * | * | * | * | * | * | * | * | ||
| Bladder issues (urgency/weakness) | * | * | * | * | ||||||||
| Bowel issues | * | |||||||||||
Symptom defined by participant as being invisible (italics indicates when subtype was specified).
We have listed the “MS hug” separately from pain and spasms because it is often recognized in the literature as a separate symptom, and our participants described it as a unique experience that is distinct from other experiences of spasms and pain.
Appendix D
Transparency
Action Editor: Vina Goghari
Editor: Jennifer L. Tackett
Author Contributions