
Abstract
Stigma related to drug-resistant tuberculosis (DR-TB), one of the world's most severe infectious diseases, is a major barrier to TB elimination particularly for women living in settings of gender inequity. Drawing on the participatory action research (PAR) framework of photovoice, we explored lived experiences of DR-TB stigma among nine affected women in Mumbai, India. Consenting women took, shared, and contributed to the critical interpretation of 37 non-identifying images and associated narratives with one another and with PAR researchers. The study surfaced vivid, untold stories of trauma and life-altering encounters with enacted, anticipated, and internal stigma, that were characterized by loss (of self, voice, status, mobility), abuse (mental, social) and deep internal distress (shame, isolation, suffocation, peril). The study also revealed how stigmatized women found means to build resilience and resist the impacts of stigma. We further witnessed the building of their collective resilience through study participation. Photovoice proved to be a uniquely compelling method of data capture and interpretation, with potential to develop meaningful engagement and solidarity among women affected by DR-TB.
Keywords
One-by-one, TB took everything away from me. I used to love to sew and make clothes for my children, nieces, and nephews. I used to enjoy sitting with my husband and chat with him, on hours, about my dreams and aspirations. I used to get so much pleasure from walking barefoot, feeling the softness of the earth and grass underneath my feet. My physical movements by now are restricted. Due to the drugs I have to take, my feet have swelled up and I can barely feel them anymore. My husband avoids me. My children no longer live with me. My mother-in-law has taken away my sewing machine, which used to be my sole companion. (Zeenat)
This is Zeenat's story, a 26-year-old woman living with drug-resistant tuberculosis (DR-TB) in Mumbai, India. Her world is colored with hopelessness, anguish, loss of control, and stigma, most strikingly from her loved ones. Physical debilitation and mental anguish are expected outcomes of DR-TB, the severest form of tuberculosis (TB) affecting nearly half a million people globally each year (WHO, 2021). Stigma and discrimination, however, are particularly harsh and avoidable consequences (Macintyre et al., 2017) (Figure 1).

Zeenat: the sewing machine.
Before COVID-19, TB was the leading cause of death from a single infectious agent. India has approximately a quarter of the world's burden, reporting 24 million new diagnoses each year and 1,400 daily deaths from TB (Chakravarty et al., 2019; WHO, 2021). Mumbai, the country's financial and urban center, has a particularly high incidence of DR-TB that is resistant to the most common anti-TB drugs and is substantially more complex to diagnose and treat compared to its drug-susceptible counterpart (Isaakidis et al., 2014). Historically, patients received 2 years’ multidrug therapy that is associated with debilitating adverse events and requires prolonged social and clinical isolation. Shorter, more effective regimens are now emerging but they remain especially difficult to access in lower-resourced settings such as India (Isaakidis et al., 2013). Research in other settings also suggests that pharmaceutical advancements do not ameliorate the social hardships of DR-TB (Daftary et al., 2021).
Given the complexity of DR-TB, diagnostic delays, misdiagnoses, and poor prescribing practices are commonplace (Isaakidis et al., 2014; Shringarpure et al., 2016). These challenges are exacerbated by fear and negative perceptions about the disease, that fuel stigma and discrimination towards affected people, not only in the community but additionally in the health care system and within households (Courtwright & Turner, 2010; Isaakidis et al., 2013; Macintyre et al., 2017; Shringarpure et al., 2016). In many settings, TB stigma can be compounded in women due to their unequal social and economic status (Daftary et al., 2020). There has however been very limited inquiry into stigma facing women affected by DR-TB in India (Atre et al., 2004; Shringarpure et al., 2016; Thomas & Stephen, 2021). Using a novel methodology, we uncovered the meaning and experience of DR-TB stigma through photos and narratives curated by women living with the illness in Mumbai. We identified complex constructions of stigma in DR-TB, and the potential role of photovoice to engage affected women.
Background
Tuberculosis in India
TB is a quintessential social disease. It is most prevalent in people who live or work in poor conditions where the risk of exposure to airborne infections is high, and in people with compromised immune systems such as people who are malnourished or living with HIV (Farmer, 1996; Lonnroth et al., 2009). A megapolis of 20 million people, Mumbai is a major TB “hot-spot” (Chakravarty et al., 2019). Poverty, malnutrition, and over-crowding create a perfect habitat for the disease to spread.
As in many settings, the TB epidemic in India has a strong gender dimension connected to deep rooted patriarchies and gender-based inequalities that face women more generally (Atre et al., 2004; Daftary et al., 2020; Krishnan et al., 2014; Mason et al., 2015). Women face inequalities of mortality, natality, employment, ownership, special opportunity, basic-facility, and the household (Sumanjeet, 2017). They are often blamed, shunned, and mistreated, including when unwell and, precluded from accessing health care services. To avoid additional marginalization and to protect their social identities, women with TB are found to hide their symptoms and diagnosis, avoid seeking treatment, or leave treatment midway (Daftary et al., 2020; Krishnan et al., 2014). When inquiring on the situation of women with TB in settings such as India, scholars have pointed out first, that women's health-seeking behaviors can be compromised due to deep-set gender roles and expectations that center around and prioritize marriage, child care, and family care; second, that women's access to health services are shaped by socioeconomic inequities, especially poorer financial autonomy and relatedly, poorer agency and mobility; third, TB poses risks to women's reproductive health, which especially threatens their social identities and status in the family; and fourth, given these inherent inequities and threats, women with TB may encounter disproportionate levels of stigma (Atre et al., 2004; Daftary et al., 2020; Krishnan et al., 2014; Somma et al., 2008). These insights are crucial to unpacking experiences of TB and TB stigma among women in countries with poor public health spending, high levels of poverty and gender inequity, and where the health needs and priorities of women can be overlooked. India is a case in point (Bhan et al., 2016).
Stigma in Tuberculosis
Disease-related stigma is not natural or inevitable. It exists because it is enabled and nurtured via social, legal, ideological, and cultural norms and rhetoric which, over time, hallmark systematic exclusionary practices through conscious and subconscious pathways (Pearce et al., 2012; Pescosolido & Martin, 2015). TB is a deeply stigmatized disease (Courtwright & Turner, 2010; Macintyre et al., 2017). Studies from Zambia, South Africa, India, and Kenya, among other high burden settings, show that people with TB are discriminated by family members, neighbors, and health care workers for fear of contracting TB (Mason et al., 2015; Nyblade et al., 2019; Somma et al., 2008; Thomas & Stephen, 2021).The fear of contagion is a leading driver of TB stigma. Those with TB become marked as dangerous, often through an amplified perception of risk, and categorized as worthy of exclusion. Stigma then manifest in overt and covert ways, reflecting established typologies such as enacted stigma (a discriminatory act), perceived stigma (an anticipation or fear of discrimination), and self-stigma (an internalization of others’ negative perceptions and discriminatory acts) (Campbell & Deacon, 2006; Macintyre et al., 2017). People facing other forms of social disadvantage and oppression, such as women living in patriarchal settings, are more vulnerable to TB stigma (Daftary et al., 2020; Macintyre et al., 2017).
Any commitment to addressing TB stigma needs deep inquiry into and bold representation of its lived experience and legacy. Deconstructing the drivers (causes), domains (aspects) and manifestations (types) of stigma, and situating them in context, can enable forethought into meaningful interventions (Macintyre et al., 2017; Pescosolido & Martin, 2015). Traditional research methods may however risk reducing or missing the layered and nuanced voices of those who are marginalized. What can be availed in these contexts are approaches and tools that place the subjects of inquiry, in our case women with DR-TB, at the nexus of the research process.
Methods
Study Objectives
Our primary objective was to understand how women with DR-TB understand and characterize their experiences with stigma. Secondarily, we explored the impact of photovoice on patients’ engagement with stigma mitigation. As part of the secondary objective, we explored how women challenged stigma and could be engaged as advocates of change or discussants of solutions.
Framework
Using a feminist approach, we drew on the methodology of PAR, or participatory action research, as is described here and subsequent sections. We explored TB stigma through the perspectives of women with TB, and many of our research activities (data collection methods, analysis, knowledge mobilization) combatted normative processes in which oppression may be embedded (Cosgrove et al., 2020; DeVault, 1999). The one area in which we deviated from the feminist inclination, underlined by Lewin's influence that, “communities identify their issues” (Darroch & Giles, 2014, p. 23) was in our decision to preconceive stigma as the subject of inquiry (Darroch & Giles, 2014; Lewin, 1946). Activities thereon, however, were in deliberate partnership with participants including planning what to do in the study, executing those procedures, evaluating the results, and taking action. In this way, we drew on the ideologies of Freire and challenged the hierarchical model of research and knowledge production and, as detailed ahead (Darroch & Giles, 2014; Freire, 1970). At each stage of data collection, interpretation and dissemination, we made concerted attempts to balance power relationships in research processes and outcomes by surfacing and prioritizing knowledge from the perspectives of people with lived experience, that is otherwise often “subjugated” (Mountz, 2016) and supporting their motivations and directions (Parpart, 1995). This included paying explicit attention to the language, tone and gestures used, and apparel worn during by team members (TM, TM) who directly engaged with participants.
Under PAR, our choice of method was photovoice, that combines photography with a Freire (1970) approach to critical dialogue, and where local and emic knowledge and concerns of utmost priority to research participants, that could be especially complex and difficult to verbalize, may be privileged (Cosgrove et al., 2020; Freire, 1970; Wang & Burris, 1997). Participants were accordingly encouraged to take photographs to uncover their experiences, co-create solutions, and contribute to critical interpretations of their lived realities (Gervais & Rivard, 2013). Stigma lent itself well to be studied through a feminist, PAR and photovoice approach because it is intimately connected to a marginalized lived experience that may be difficult to share or reflect upon through traditional methods. Photovoice has been applied in India, including among women and girls (Shah, 2015; Srinivasapura Venkateshmurthy et al., 2021). However, despite its ability to create compelling evidence supporting public interest and policy reform, it has very seldom been used to interrogate the experiences, norms, and practices underlying TB stigma or stigma mitigation, and not widely at all in the context of India (Catalani & Minkler, 2010; Mohammed et al., 2015).
Study Site
The study was undertaken at a TB clinic in Mumbai operated by the international non-governmental organization Médecins Sans Frontières (MSF). Staffed with three physicians, six nurses, and three adherence counselors, the site is a referral point for patients in and around the city who have especially complex drug-resistant profiles and are in need of drug regimens that may be harder to access in the traditional public health sector. At the time of the study, there were 61 women in DR-TB care. Stigma was a common complaint raised during patient counseling sessions and program managers were keen to learn more about it. They were also interested in supporting a more active approach to inquiry that could meaningfully engage their patients.
Participant Recruitment
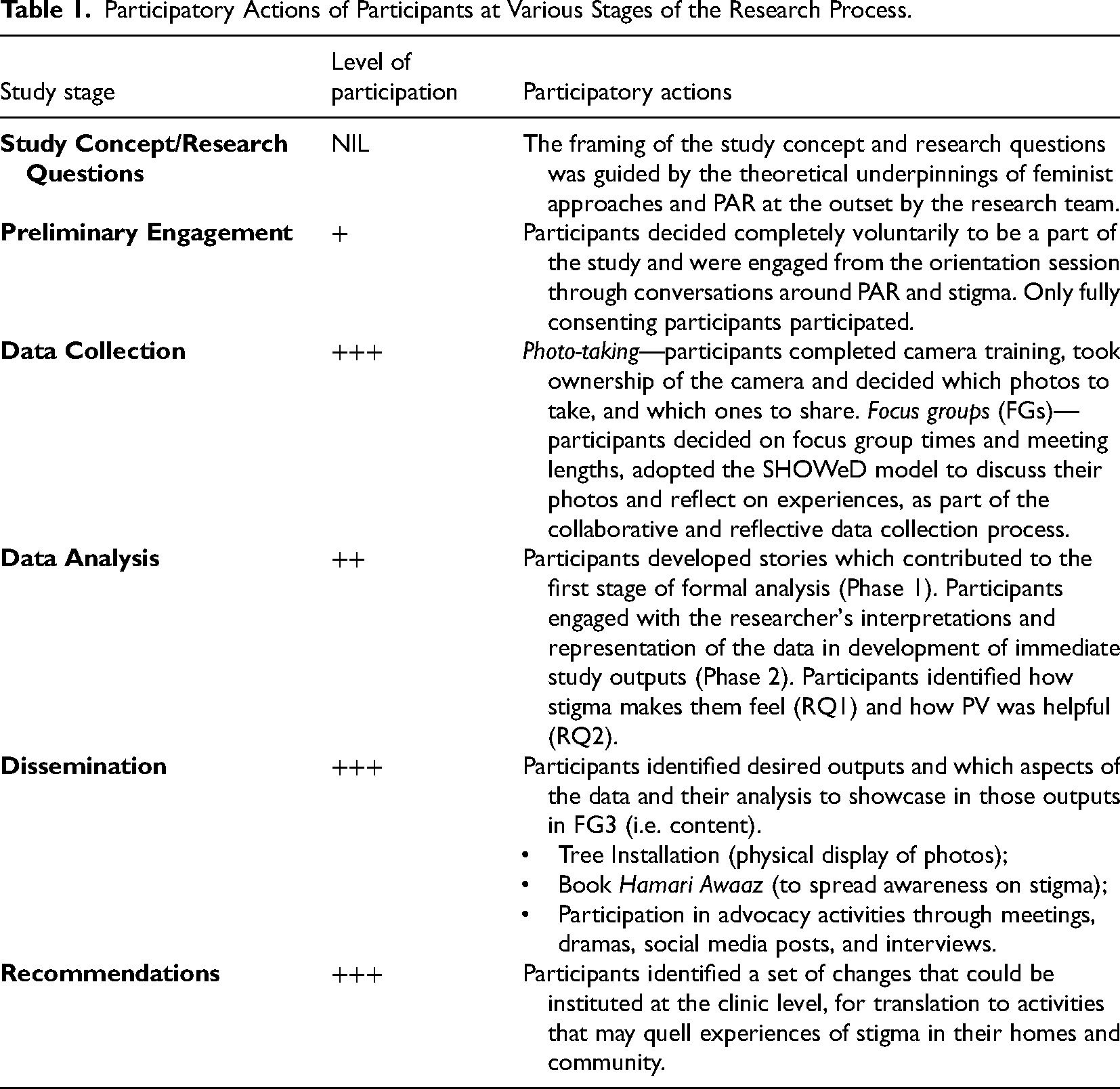
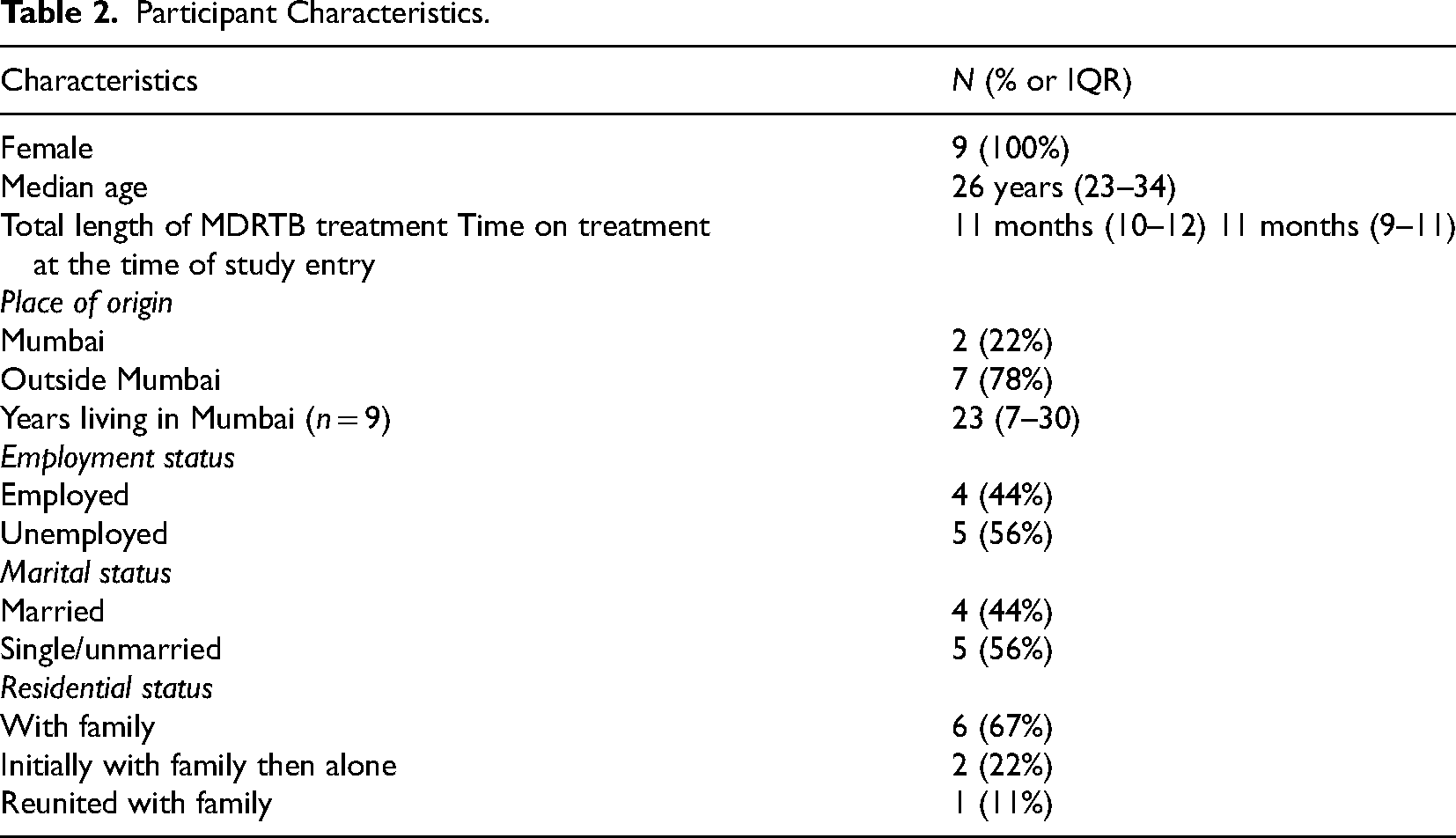
The study took place between November 2019 and May 2020. A contextually appropriate PAR approach was applied from the point of participant recruitment (Table 1). Participant eligibility criteria included (1) female adults diagnosed with DR-TB, specifically multi- extensively or pre-extensively DR-TB); (2) completed minimum 4 months treatment and/or are culture-negative (whichever was later); (3) in active care at the study site; (4) physically able to carry a camera (i.e. free of pic lines or catheters and assessed to be clinically stable); and (5) capable of informed consent. Eligible women identified by clinic staff over a 1-month period were invited to a group orientation session to learn about the study; 21 women attended one of two sessions. We first discussed the study purpose, activities including the photovoice process and group discussions, potential risks and benefits, and time commitment; that is, attendance at an introductory workshop and three focus groups (FG), each spanning 1.5–2 hours and held in a private area at the clinic over the following 4 weeks. We spoke individually with attendees to gauge their understandings and motivations related to the study and potential participation, and responded to questions. Their engagement and collaborative spirit, including availability and willingness to take photos, attend discussion sessions, share thoughts and listen to others, were understood to be crucial to the research process. In the ensuing formal consent process, nine women gave written, informed consent to engage in the study (Table 2). Others did not express interest or did not foresee being able to attend multiple sessions due to conflicting responsibilities of child or home care, being uncomfortable traveling to MSF more often than required for medical care despite transport assistance, and/or feeling unconfident about taking pictures.
Participatory Actions of Participants at Various Stages of the Research Process.
Participant Characteristics.
Ethical Considerations
Institutional ethics approval was received from the MSF Research Ethics Board and the Indian Foundation for Medical Research Ethics Committee. Individual informed, written consent was obtained from all participants prior to participation in any research activity. Emphasis was placed on voluntariness, especially that their decision to participate or not, or early withdrawal, would have no impact on their medical or related care, and confidentiality. Distinct consent for photo release was sought and obtained from each participant after the images were taken and shared; participants were trained to take non-identifying images as described ahead. Given the advocacy angle of feminist-rooted work, we also built in opportunities for participants to self-select pseudonyms, disclose participation, and/or link photos to their identity (Cosgrove et al., 2020). All participants received transport reimbursements and refreshments.
Data Collection
At an introductory workshop, consenting participants met each other and research team members comprising of a PAR researcher (TM, lead author) and patient support worker (TM, second author), learned more about the study activities, and decided collectively on processes of group engagement (e.g. agreement on planned study activities, meeting times, pseudonyms, respect for others’ opinions and contributions, means of communication and decision-making, audio-recording). They learned how to operate a FUJIFILM INSTAX WIDE 300 polaroid camera, and each received a camera to take home. They were asked to take photos of moments, issues, subjects, artifacts, stills, persons (in an unidentifiable manner) or anything else that represented to them some form of stigma they had experienced, regardless of whether it was a tangible encounter or something they thought or worried about. The term ‘stigma’ was unpacked by participants to arrive at a shared understanding of what their images could potentially capture; it was decided to be something that made them feel very sad, worried, afraid, badly, and especially that made them feel different (with a negative connotation), discriminated, or less worthy. It could represent an emotion or event since having been diagnosed with TB, the present time, or an expected future. That stigma was a salient feature of all of their lived experiences was evident in the discussion.
Data were then formally collected via three audio-recorded FGs. In the first two FGs, participants shared and discussed their photos (3–5 each, total 37), gently prompted by the research team. The SHOWeD model was used; a springboard for dialogue creation where participants are sequentially prompted to help them “dig beyond the surface of the image to discuss causes and potential solutions” (Strack et al., 2004, p. 51) through the questions: "(1) what do you
Analysis
Common to photovoice studies, the first phase of analysis was a group-based interactive process involving researchers and participants, and coinciding with data collection during FGs (Wang & Redwood-Jones, 2001). As participants took turns sharing photos and responding to questions in the SHOWeD model, they were given the opportunity to independently reflect on their own and their peers’ photos. Some opted to collect thoughts in silence while others used a notepad. The floor was then opened to return to each photo, receive others’ comments, and hone out similar and dissimilar experiences. This part was facilitated by the researchers, as the goal was to identify diverse themes. A whiteboard was used to list ideas, with examples and reasons. Participants made the final decision on which ideas would best address the primary research objective to learn how women experienced and understood TB stigma. Each participant selected and entitled two of their most compelling photos and gave researchers clearance to craft preliminary story lines around each drawing on what they had shared in FGs. The quotes and final stories were then reviewed by participants; the research team attempted to use participants’ words verbatim wherever feasible (including this paper).
The journey of photographing and co-analyzing made the first phase of data analysis a lived experience in its own right, as became apparent in four crucial ways. First, the activity of photographing enabled women to reconstruct experiences with their illness. Photography was an active process and led to a tangible output; it was cognitively stimulating and immediately gratifying as repeatedly suggested by the engaged conversations amongst participants. Rather than relay a static story, each participant had to plan and reflect on what photographs they would take to illustrate their particular experience with stigma related to TB. As has been recorded by other photovoice researchers, we saw that “participants had creative control and freedom to produce a storyboard of [visuals] that could subsequently be narrated … these preliminary processes were generally enjoyed, and participants were eager to view, explain, and talk about their photographs” (Oliffe & Bottorff, 2007, p. 851). Photo-taking allowed past as well as current experiences to be placed in participants’ consciousness, and their stories explicitly became situated in the focus of the research. At first, as explained by the participants, the process was painful, discomfiting, and confronting. By the end, it was transformative and therapeutic. For example, Khushi, stated, In this project, we the TB patients, who are in actuality survivors, were treated as “experts” on our lives and through our photos that represented our voices, hence “photo-voice,” we explored and shared what it feels like to live with TB in safe-space settings and came up with potential advocacy suggestions and hope for change in our communities.
In the second phase, research team members (TM, TM, PI and AD) further analyzed the photos and related discussions away from the FG setting, engaging with the literature on stigma and resilience that emerged as most relevant to the data emergent from FGs (Campbell & Deacon, 2006; Courtwright & Turner, 2010; Eshel et al., 2018; Link & Phelan, 2014; Macintyre et al., 2017; Nyblade et al., 2019; Pescosolido & Martin, 2015; Zimmer-Gembeck & Skinner, 2016). Audio-recorded materials were de-identified, and professionally transcribed and translated. Thematic analysis created space for inductive as well as deductive approaches to meaning making (Braun & Clarke, 2006; Nowell et al., 2017). Descriptions of living with stigma helped to develop a critical analysis of stigma experiences and manifestations that were grounded in participants’ voice and the study context and supported by the literature. In this phase, the potential relevance and impact of participants’ engagement in photovoice was also more deliberately assessed. The following procedures were discursively practiced: (a) active familiarization with the data by two coders (TM, TM); (b) coding separately at first using the code-is-your-mantra scheme popularized by Braun and Clarke (2012), wherein each analyst coded for semantics, expressions, and descriptions mainly focusing on the point “how does stigma make the participant feel?”; (c) meeting on concept and early theme development by comparing and contrasting developed codes between coders and consulting with other research team members (PI, AD); (d) meeting on thematic refinement and critical interpretive engagement with the literature related to stigma and resilience (as shared above); (e) triangulating participants’ ideas as raised during FGs, with typologies of stigma and resilience that were reflected in the literature (e.g. Campbell & Deacon, 2006; Macintyre et al., 2017); (f) member checking themes with three willing and available participants; and (g) writing up themes to ensure participants’ perspectives were reported in ways that centered around the connectedness of their experiences as well as the heterogeneity among them.
Findings
We interpreted two parallel results linked to our participatory action methodology. First was the capture of the lived experience of TB stigma, and second was the building of resilience as a consequence of having partaken in the photovoice enterprise. Typologies of stigma and resilience, which emerged during analysis and are integrated into the themes ahead, helped us to delineate ways by which participants encountered these phenomena.
Lived Experience of TB Stigma
Enacted stigma
Enacted stigma or overt discriminatory acts are considered to be the most visible and visceral form of stigma. In TB, it has encompassed name-calling, distancing, apathy, abandonment, and violence (Daftary et al., 2021; Macintyre et al., 2017). Enacted stigma was expressed in all participants’ stories, and manifested in diverse ways. Mahera's story for example depicts a “Mickey Mouse Bench” (Figure 2) and tells of discrimination and disrespect that she encountered from her health providers. The bench brings us into the patient waiting area of a (different) health facility where she spent hours waiting to be seen. Upon arrival, she was spoken to rudely and told to sit at one end, far removed from other patients because of her TB diagnosis. Though she arrived early, and saw others being attended to on the basis of their arrival, she was not seen until all the other patients left. She had felt paralyzed with the discrimination, yet unable to question it. So, they said, you are TB patient, right? Go out. Go out. They shouted at me very loudly in front of a lot of people and that was not right. So, I went and sat at the end until all the patients got done. It is important to share this visual because this is how people treat TB patients…like they have committed some crime. Even the doctors there say to your face, “you will die, you will die.” (Mahera)

Mahera: Mickey Mouse bench.
Several participants had been reprimanded, removed from common waiting areas, moved to the end of a line, and required to wait for extended periods within various health facilities that they had been referred to for tests or procedures. One participant was told by her provider that she should “not hope to live” with this diagnosis, making corresponding acts of exclusion all the more unbearable. The TB literature is replete with examples of institutional or structural stigma, enabled through the restrictive or exclusionary policies of established institutions such as government bodies (Macintyre et al., 2017; Pescosolido & Martin, 2015). Nyblade et al. (2019) reviewed health facility stigma to “[range] from outright denial of care, provision of sub-standard care, physical and verbal abuse, to more subtle forms, such as making people wait longer or passing their care off to junior colleagues” (p. 1). This is a particularly egregious dimension of stigma, as it emanates from a system that is expected to support, protect, and enable people who need and seek care when they are at their most vulnerable. Institutional stigma has undermined diagnostic and treatment outcomes in TB (Daftary et al., 2018; Nyblade et al., 2019).
Nishi's story, “Bathroom I Can’t Use” (Figure 3), tells of the dehumanizing experiences she faced from her family, who denied her from using the toilet at her discretion for fear of contracting TB. She spent months holding herself every morning, unable to meet a basic need. This left her feeling helpless, exposed, and humiliated. Naturally everyone goes to the bathroom in the morning but no matter what happened, I did not have the permission to go to the bathroom until everyone's breakfast was done. Once everyone had eaten and gone out for work, I could go to the bathroom. After that, I would have to put 3–6 buckets of water and Detol [cleaning agent] properly and only after I washed the bathroom that way, was I permitted to enter the hall or my room…[so, my urge, I had to] keep controlling it from 6 am to 11 am. Anyhow, I had to control it. So much that I would have health issues with my stomach. But what to do, I had to adjust. (Nishi)

Nishi: the bathroom I can’t use.
These encounters had little clinical consequence, but they stripped participants’ identity, dignity, and sense of belonging and worth. They affirmed widely held views that TB is a ‘dirty’ disease and illustrated how fears about risk, contagion, and death could erode people's inclination to offer respite and support (Juniarti & Evans, 2011). Participants were especially traumatized that their stigmatizers were people whom they rather expected would bestow empathy and comfort. Reports from India have shown that women can be locked in rooms, hidden from relatives, rejected by husbands and in-laws, returned to their natal households, and disconnected from their children after receiving a diagnosis of TB (Mehra & Udwadia, 2016).
Anticipated stigma
Anticipated stigma is the worry that one will be devalued and discriminated. It is the perception or feeling of stigma (i.e. what could happen), fuelled by exposure to negative attitudes including one's own beliefs, or witnessing overt discriminatory acts. Anticipated stigma can have visible consequences in TB. People are known to delay or refuse seeking TB care, access their test results, or begin (or complete) treatment in order to keep their diagnosis hidden (Macintyre et al., 2017). Very early in treatment, and often after experiencing some overt discrimination, all participants recognized that they could be mistreated by others, including those whom they would have normally trusted. They adopted various strategies to deflect these difficult situations. For example, Zee's photo, “My Shameful Face” (Figure 4), represents the effort she took to prevent neighbors from recognizing her as the “girl with TB.” In conveying its significance, Zee explained that in her community, TB was considered a grave offence with religious connotations. It marked people as careless or so carefree as to acquire TB, as if it were a result of cognitive behavior. Women became “non-marriageable material.” The fear of suffering these judgments compelled Zee to hide her face in public. While masking is a viable infection control measure, and could invite stigma itself, Zee simply wanted to become unrecognizable so she could avoid inviting contact or conversation with anyone outside of her home, and hence avert harsh questions or mistreatment at the hands of others. She veiled herself up until her reports returned negative.
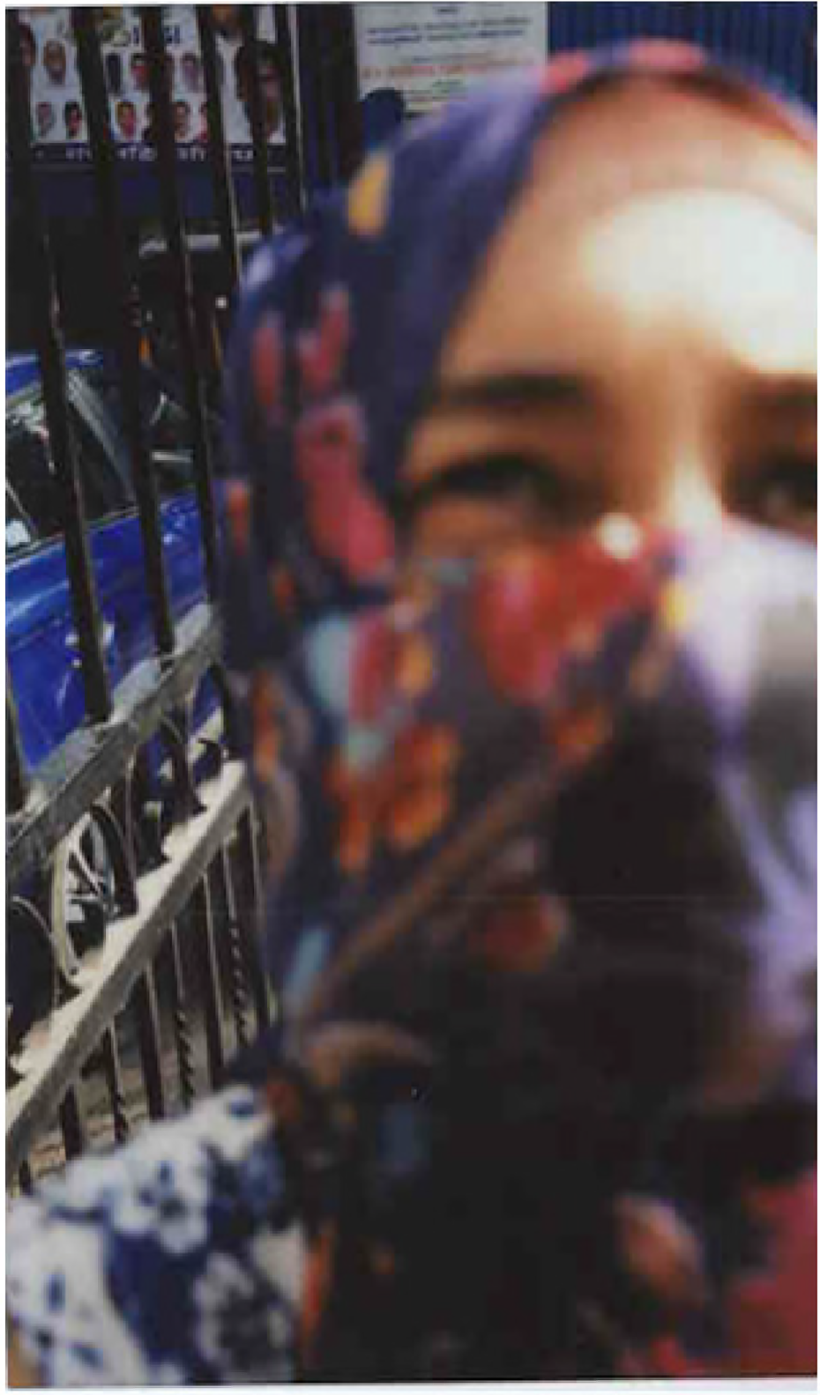
Zee: my shameful face.
Khushi photographed “The Empty Office Desk” (Figure 5) to tell us about her crushed dreams: “I want to work like in this environment. I want to do job. But I cannot.” She wished to work in the Indian foreign or administrative service that would have been highly valued in her community. In her view, TB took away the chance to fulfill her dream. Given her medical quarantine recommendations, she could not appear for the in-person government exam. She also feared the examiners would label her as having “unfit health.” The anticipation of a life interrupted and dreams destroyed from such disqualification was substantiated by statements made by other participants who had also been labeled by their relatives and acquaintances as weak and unfit for any “excursion” outside their homes. The distress of how poorly interactions with the outside world could go, during and in the aftermath of their diagnosis, fed into participants’ sense of worthless, and threatened to affect them well beyond treatment.
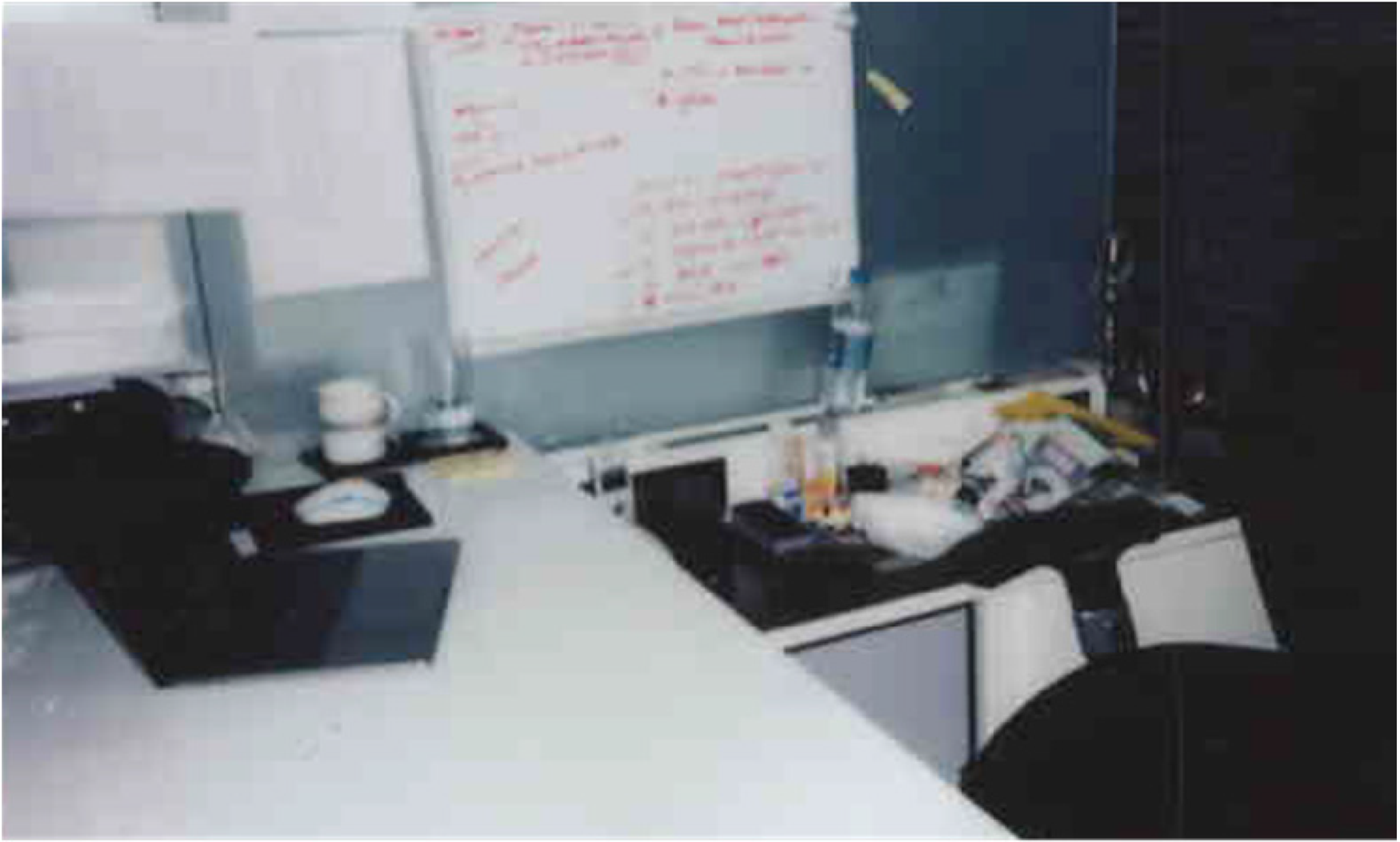
Khushi: the empty office desk.
Internalized stigma
Internalized or self-stigma is when individuals come to endorse negative stereotypes and discriminating attitudes, and think or act according to those negative portrayals (Macintyre et al., 2017). It is typically derived from people's experiences with enacted and anticipated stigma, but the manifestations are often invisible to anyone except the person who experiences it. “The Lonely Bench” (Figure 6) photographed by Khushi, for example, reflects the deep erosion of her identity and self-worth that came about with her prolonged isolation. When a person is, or I am treated, less favourably on the grounds of illness and fear of becoming the subject of gossip, I often isolate myself. To avoid infection of others and to avoid uncomfortable situation, I just like to keep myself separate. I feel this is self-discrimination where I feel unworthy, leading to a lack of self-worth, depression and abnormal behaviour. Although my family tried to pull out me from this situation but because of my TB and treatment, high consumption of drugs makes me… I am more comfortable with isolating myself. (Khushi)

Khushi: the lonely bench.
While self-isolation and reclusiveness may be a way to accept TB and follow health providers’ sanctions (and develop resilience, as discussed later), it is arguably triggered by the embodiment of negative sentiments perceived and received from others. As another participant stated, being seen as a “nuisance, a topic of discussion” fed into her sense of unworthiness and she felt increasingly disinclined to interact with others.
In “My Feet” (Figure 7), we see Zee's loss of mobility and agency. On the surface, the photo represents a treatment side effect, but beneath it carries the weight of her devaluation. Peripheral neuropathy (experienced as nerve pain in the limbs) and skin dyspigmentation (experienced as skin darkening) are common side-effects of the DR-TB drugs linezolid, cycloserine, and clofazimine. Participants internalized the undue negative attention invited by these effects, which triggered feelings of disablement, unattractiveness, and inadequacy, especially because a high social value was placed on having light skin in their community and there was virtually no infrastructure to support people with physical disabilities. For Zee, as with several other participants, physical changes compounded the impact of restrictions already placed on her by her providers and relatives. The [pills] make you darker than what you were before. So, it makes you feel like you are not you. And sometimes you feel like when will I get back to myself. Because you don’t like what you see. And it brings down your whole self-confidence as well. Because you don’t like to see yourself in the mirror. When you look at yourself in the mirror, you will be reminded of the darkness you know, that has taken over. This particular medicine that we take, it affects the feet. And the chances are that it has damaged 70% of the nerves of the feet which makes it difficult to walk. I felt like uhh you know my world is like collapse in a way because I felt like I wasn’t like myself the way I was before. I felt like I am different now. I felt like almost like half disabled. (Zee)
Zee: My feet.
Internal TB stigma thereby butchered participants’ self-confidence, leaving them disempowered and helpless. They gradually relinquished whatever decision-making agency they may have enjoyed within their families or households. Apathy set in for participants who saw their opinions become less important, and hence also started to see themselves as inferior. They came to believe one of two things: that they deserved to be devalued, blamed, and mistreated, and must accept it, or that they needed to overcome this trauma and find a way to move forward.
Building Resilience
Individual resilience
All participants experienced enacted, anticipated, and self-stigma since their TB diagnosis. While they felt less in control of countering enacted and anticipated stigma, they had developed ways to alleviate internal stigma; some more successfully than others. We learned how participants built individual levels of resilience through silent and personal introspection, independently processing their life situation, and holding on to encounters that had bolstered their confidence and worth before they became sick with TB.
Personal resilience has been defined as a person's cognitive ability to respond positively to an adversity or stressor (Eshel et al., 2018). In feminist theory, resilience is conceived as an inherently bounded response inextricable from one's family, community, and social systems (McRobbie, 2020). In this study, we saw resilience following a “pull yourself up by your bootstraps” logic (Liegghio & Caragata, 2021, p. 3). Though participants were limited by inequities connected to their gender, social capital, and diminished social status, they all took concerted efforts to shield themselves from negative experiences. Two examples follow: the first of Mahera, who applied positive thinking, and the second of Nags, who withdrew from social interactions.
Mahera worked hard to stay positive and every day devoted some attention to those memories and aspects of her life that helped her feel “normal” and returned her to an identity devoid of TB. Her photo, “My Achievements” (Figure 8) embodies how she directed her focus on the medals and accolades she had won for school competitions and sports achievements. She had been an astute student, and reflecting on her accomplishments helped her to stay positive. She was motivated to work even harder to prove to her friends, family, and school authorities that TB would not prevent her from continuing to reach for her goals and ambitions. Her efforts represented sublimation, a resilience strategy where unpleasant emotions are channeled into socially acceptable modes of expression and new, learned behaviors (Vaillant, 2011). By redirecting her attention to something which inspired her and also resulted in a tangible output, Mahera was able to alleviate the hurt she felt from others. While she continued to face prejudice, she was able to resist internalizing those prejudices. And the day I saw my father crying because of my TB and the stigma I had faced at the hospital, I gathered courage and thought that no matter what problem I have, I will not back out from life. When I would have to take injections and it would be painful and I would vomit due to the medicines, I didn’t show my parents that I was having distress… People generally give up on their studies, hobbies, other activities once they are diagnosed with TB. But I never let this disease stop me from participating in various sports events in school and college… I would participate no matter if I win or lose or no matter what others thought of me. I wasn’t bothered about that. I was participating with my TB condition and that was a big thing for me. (Mahera)

Mahera: my achievements.
Nags’ photo, “The Dining Table I Avoid” (Figure 9), embodies the resilience strategy of withdrawal, or the act of deliberate social and emotional separation from others (Zimmer-Gembeck & Skinner, 2016). Nags was explicit that she did not like to be the topic of gossip, hence disengaged from situations that could place undue attention on her. She kept away from others as a way to reject them before they could reject her. Not only did this allow her to assert agency, she won a degree of independence, as she had to figure out ways to take care of her material needs without seeking help from others. Nags needed support, but knowing that her expectations would be unmet, she rather embraced the opportunity to become self-sufficient. Indeed, it was evident from the stories of several participants that social withdrawal was not their first choice; rather it became a way to deal with the loneliness once separation had already been imposed by others. Gradually, they bought into the idea that staying away was their own decision, and claimed it as a means to and preserve their self-respect, autonomy and, for some, take action against potentially abusive situations. Here we all used to sit and eat food. But since I came to know that I am a patient, I started to sit alone at the table and have dinner. Everyone else started eating together, separately. It was painful for me. But somewhere I understood that it is better for me and for my family members. I tried to take this experience in a positive way. This made me feel less bad. This picture makes me feel pain but it was important for me somewhere, the pain…perhaps, to grow. (Nags)

Nags: the dining table I avoid.
Collective resilience
Photovoice was new for our participants. They experienced it in progressive related stages (Figure 10), beginning with co-creation of a safe space where they could articulate untold stories to one in which collective enablement and resilience was incited. As researchers, we witnessed the powerful imprint the process had on women who faced stigmatizing and or marginalizing encounters in their everyday lives. The non-judgmental, non-evaluative and collaborative approaches to data gathering, sharing, and analysis (Phase 1) were crucial. Photos and their associated stories came to be valued by participants and researchers alike. Participants accepted one another on par—likely also because of their shared socioeconomic conditions, and researchers came to be recognized as learners—possibly because of the efforts taken to mitigate traditional imbalances, allowing some of the asymmetries in control over the research process to be overridden.
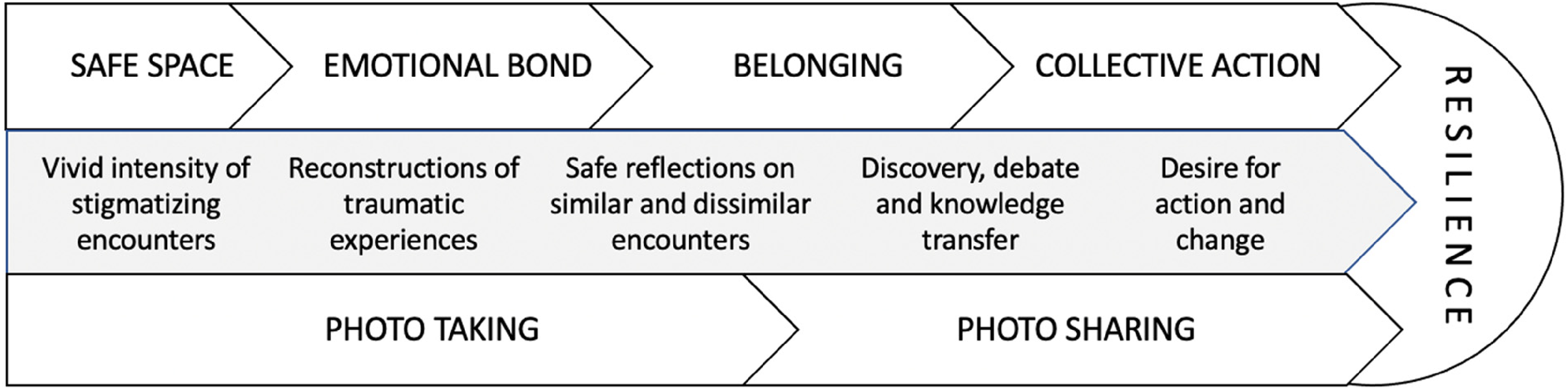
Building collective resilience: the photovoice journey.
This process allowed participants to develop increasing comfort in taking and openly discussing their photos. In one instance, Nikita reflected on a photograph of the utensils that her step-mother kept separate from others. She remembered her deceased mother and began to cry, voicing the disparities she felt and had internalized between her mother's unconditional love and step-mother's resentment. She felt able to share with the group the wounds which fractured her closest relationships, something that she had never previously verbalized. Photovoice was very important because for a year before this project, I felt that I was alone. Who would I go talk to? Who can I talk to? We don’t talk to everyone that this has happened with me or this doesn’t happen with me. But with the help of this project we had a discussion here and that felt good. (Nikita)
Expunging emotions with others who had faced hardships on account of a shared illness enabled participants to process and overcome their grief in a group. This may have happened because participants displayed overt empathy with one another, validating others’ feelings, and making them feel less alone and more safe. For many, this was the first instance of visualizing their pain and assigning it a formation, in other words, a meaning. They were finally able to address emotions which, until then, they had deeply suppressed. Several participants were able to leave their grief behind in the photo, recognizing that they were no longer alone, or at least the pain was no longer theirs alone to have encountered. The ability to assign meaning to another's photo(s), and give it meaning, enhanced their connection to others and built feelings of allyship and solidarity. With time, participants felt emotionally invested in the project and motivated to use their photos to create awareness about TB. This is not to state that photovoice was the singular trigger; rather, it allowed participants to organize their thoughts, revisit their situations in the safety of a peer group, and reflect on their emotions (and those of others) as attached to a particular moment or encounter experienced in a given circumstance. It helped them answer for themselves and their peers ‘how do I/we feel about that situation’, and ‘what does that tell me/us about my relationship with TB’. It also allowed them, for the first time, to value their own stories. It is in this valuation and belief in the power of their own voice that they could consider their photos and reflections thereof as agents of change.
As safety, engagement, and belongingness unfolded during the photo and story sharing process, we observed participants more easily and intensely assemble together; collaboration was naturally inculcated. Not only did they formulate individual stories, they also engaged in dissemination discussions. They built a three-dimensional tree to display their photos, wrote a collective poem on stigma and healing for use as an advocacy tool (through electronic and print media), and decided to bring these outputs together in the form of a coffee table book (which has since been published and widely shared) for clinics, health centers, media professionals, and government bodies ( Hamari Awaaz: uncharted voices, 2021 ).
The participant journey was thus dotted by achievements that illustrate the opportunity for photovoice to create a platform for action and collective resilience building; from taking photos, feeling engaged, opening up to others, forging relationships, and coming together towards a common goal to create change. By way of thoughtful facilitation skills, photovoice was also a vehicle for instances of joy, ownership, and creativity. It can be argued that those moments were short-lived, or that the change offered was small or only to a handful of individuals. It can also be argued that when women come together in a group they automatically feel engaged in sisterhood. We did not seek to measure the impact of photovoice, but we documented several instances of connection and empowerment that may have been engendered by the study framework and process. As stated by Khushi, for example, one of the shyest members of the team. Today I am stronger than I ever was before. Today I am stronger than I was, even before I got TB. For me, photovoice has been a journey, an eye-opener to see how my pain can be a balm for others. Photovoice showed me a way to find others and also not to feel sorry for myself and others like me with TB. I will continue to play my part on changing this society's view towards us, TB survivors. (Khushi)
Khushi has since joined a group of local TB activists. Among other activities, she delivered a speech on TB stigma to commemorate World TB Day across key community sites in her city.
Key Implications and Contributions
Participants’ photos and corresponding narratives revealed rich insights suggesting they had experienced life-altering encounters with TB stigma ranging from loss (of self, voice, status, mobility), abuse (mental, social), and distress, characterized by feelings of shame, isolation, and hopelessness. Their images and stories spoke to diverse forms of stigma encountered at the hands of family members and health providers in their homes and at health facilities, and the ensuing internalization of those devaluing encounters. While material items depicted as representing a loss often had little monetary value, their abrupt removal stripped participants’ of their sense of self and self-worth, and compounded the anguish of living with a life-threatening infection. Our research also revealed how resilience to stigma could be constructed at the individual and collective level. Participants navigated their deepest, most painful experiences of exclusion through introspection, positive thought, sublimation, and withdrawal. Their collective participation in photovoice helped them to connect isolated journeys and build cohesive resilience that was possibly stronger than what they had been able to achieve on their own.
In elucidating explicit shapes of TB stigma in women, this study has several implications for the engagement of families affected by TB, the health workforce, decision-makers and researchers. Many ideas to mitigate the exclusion and stigmatization of people with TB were posed by participants themselves in the final FG. Foremostly, they emphasized the need for gender-relevant education and counseling to help patients combat stigma; a cause that has been gaining momentum in the latest global strategy to end TB. Treatment literacy programs that taught patients about their medications, side-effects, and infection control were important but insufficient. Participants wanted families to be included in counseling sessions so they could be shown how to display overt care and empathy when patients in their households may be especially emotional, helpless, and sensitive to disrespect and apathy. They wanted families to learn how to cohabit with and support someone diagnosed with TB even whilst adhering to infection control practices. They hoped for wider awareness of the needs, vulnerabilities, and unjust stigmatization of women with TB. While many had won empathy and support from at least one household member, they had in parallel encountered negative behaviors from many others. They recommended focused counseling for those relatives who remained uninvested in their wellbeing and who often became the flag-bearers of their stigmatization.
Given that many had been admonished by health providers, participants strongly voiced the need to improve provider communication skills (in their words, “soft skills”), particularly among nurses with whom many patients tended to open up, and doctors, who monitored them for months on end. They raised the idea of setting up a system, in consultation with patients, to celebrate important treatment milestones to build patients’ motivation and self-efficacy.
Three months after the study, following participants’ desire to have their stories shared with those at the helm of TB programming and decision-making, we published their book Hamari Awaaz: Uncharted Voices (
Hamari Awaaz: uncharted voices, 2021
). Three participants presented it to city and state representatives at an MSF public event. It was participants’ hope that their storied photos be used in public campaigns to increase attention to TB stigma, advocate for patient-centered TB care, and establish patient centerism as a distinct objective within TB policy. For TB related stigma, we should build awareness using photos, real photos, because photos remain in people's minds and they can see what stigma actually looks like and does to us…makes all the colours in our lives dark… and maybe change their attitude so that we or other TB survivors can suffer less. (Mahera)
Conclusion
Stigma is a critical social outcome of DR-TB. In this study, we found photovoice to enable the meaningful representation, engagement, understanding, and relief of DR-TB stigma. The assignment of a visual to the experience of living with TB helped women with TB to process the image, and associated memories, and share it of their volition in an environment where those exchanges were accepted without judgment.
A few limitations are worth noting. While we attempted to implement PAR at almost every stage of research, and take concerted actions to diminish power imbalances in the process, deep societal hierarchies that govern health care settings were likely not entirely eradicated and could have affected the data and interpretations. The study was also among women only. Investing in wider approaches to engage men in participatory activities, especially given their likely distinct encounters with TB stigma, could yield rich comparative results (Chikovore et al., 2020). Stigma may also emerge distinctively in rural communities (Somma et al., 2008).
Our study nonetheless makes an important critical contribution to the TB and stigma literature. We saw the effectiveness of visuals, safe spaces, engaged voices, and participants’ capacity for ownership and collaboration in initiating advocacy and change. This may foster opportunities for organizations to support action-oriented pathways to uncover and address struggles encountered by people with stigmatizing illnesses. We also conclude that components of photovoice need not be limited to research endeavors. The framework of PAR is set in a paradigm of social justice given its roots in feminist theory and the works of Lewin and Freire, and within that, photovoice can be used generously and in malleable ways to engage patients, families, and providers to help make sense of, if not alleviate, the trauma of disease-related stigmas.
Footnotes
Acknowledgments and credits
The authors of this paper are grateful to the collaborating patients for their time and insights, clinic staff, as well as the guidance of the Médecins Sans Frontières office in Mumbai and Delhi.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported through an internal funding envelope by Médecins Sans Frontières (grant number NA).