
Abstract
Trauma survivors often report experiencing temporal disintegration (e.g., time slowing down, the present feeling disconnected from the past and future) during and after trauma, yet how these distorted time perceptions relate to psychological adjustment and views of the future is poorly understood. We examined the relationships between prior adversity, temporal disintegration, distress, and fear of future trauma following two collective traumas: cross-sectionally among college students following a university-based active shooter event and longitudinally using data from a national sample following the September 11, 2001, terrorist attacks. Temporal disintegration was significantly associated with elevated distress, which was related to greater fear of future trauma. Individuals who experienced prior adversity were especially likely to report temporal disintegration following collective trauma, suggesting that prior adversity may render individuals vulnerable to subsequent deleterious response patterns. Trauma-related temporal disintegration may have lasting implications for psychological adjustment and for how people perceive their futures, especially among individuals with a history of adversity.
I felt like time slowed down. Everything was in slow motion.
It felt like forever . . . long enough to last a lifetime.
Just as time governs the exterior world, so too does it rule our inner ones. Indeed, the subjective experience of time has long been considered the basis for human consciousness, thought, and action (e.g., James, 1890; Kelly, 1955; Lewin, 1942); without it, our lives would consist of isolated momentary experiences with no logical flow or meaning (see Zimbardo & Boyd, 2008). Through the window of time, we see our lives unfolding, as our sense of time underlies and connects who we have been (past) with who we currently are (present) and who we aspire to be (future). Given the fundamental role that time perception plays in shaping our thoughts, feelings, and behaviors (see Stolarski et al., 2015, for reviews), understanding the predictors and consequences of losing a coherent sense of time may be particularly meaningful for psychological functioning and health, especially in the aftermath of trauma.
Traumatic experiences can fundamentally alter one’s understanding of the world and precipitate a host of cognitive and emotional processes to cope with the event (e.g., Janoff-Bulman, 1992; R. L. Silver et al., 1983). These experiences can also alter our perception of time (Terr, 1983). That is, during and immediately following a traumatic experience, the uncertainty and threat of imminent danger may distort individuals’ perceptions of time such that time seems to slow down or stop, and individuals find themselves focusing only on the present moment with little awareness of the past and future (e.g., Holman & Silver, 1998; Melges, 1982). In so doing, trauma can isolate people in a stressful moment, interrupting the subjective linear flow of time that weaves the past, present, and future together into a coherent life story that anchors and supports personal identity (Holman, 2015).
This trauma-related distortion of time has been coined temporal disintegration (Melges, 1982) and has been linked to long-term psychological adjustment following exposure to disasters, in part by rendering some people vulnerable to becoming stuck in past traumas long after the traumatic events have passed (Holman & Silver, 1998). Indeed, individuals who experienced acute symptoms of temporal disintegration in the wake of a trauma remained focused on past negative events months later, and this exaggerated focus on the past was linked to diminished subsequent well-being (Holman & Silver, 1998; see also Fortunato & Furey, 2011; R. L. Silver et al., 1983; Tait & Silver, 1989). These findings suggest that experiencing temporal disintegration may increase susceptibility to long-term deleterious cognitive and emotional responses by keeping individuals fixated on prior trauma, increasing the odds for experiencing distress over time. However, there is a paucity of information about how these trauma-related distortions in perceived time may be associated with our perceptions of the future, presenting a critical gap in our understanding of their lasting impacts.
To the extent that trauma-related temporal disintegration leaves individuals focused on past trauma, it may color individuals’ views of the future by filtering them through the lens of a painful past (see Karniol & Ross, 1996). That is, trauma-related temporal distortions and related distress may color future expectations and stoke fear that the past will repeat itself and similar events will occur in the future (Blum et al., 2014). Prior work on past orientation provides indirect support for this hypothesis—people who orient more toward negative parts of their pasts may be more fearful and anxious and see themselves at greater risk of being victimized (Boniwell & Zimbardo, 2004; Chadee et al., 2019). Studies that have examined stress responses to collective traumas also lend support for this proposed link. They demonstrate how distress, at the time of the trauma and years later, is related to greater worry about future negative events (Basoglu et al., 2005; Garfin et al., 2018; Piotrkowski & Brannen, 2002). Together, this work suggests that trauma-related distress may partially explain why individuals who exhibit temporal disintegration during and after trauma may experience fear or worry about future events. Yet we know little about what makes people susceptible to experiencing temporal disintegration.
Evidence suggests that individual factors and lived experiences may increase vulnerability to temporal disintegration and the response pattern that follows. For example, individuals who have experienced chronic adversity are more likely to report temporal disintegration following a disaster, as are people who suffered a greater loss or felt that their identities had been threatened (Holman & Silver, 1998). However, prior exposure to adversity may be particularly likely not only to exacerbate temporal disintegration but also to perpetuate a cycle of adverse responding (Thompson et al., 2019). Given that individuals with a history of greater adversity perceive themselves to be more likely to experience future negative events (Blum et al., 2014; Burger & Palmer, 1992) and respond more strongly when such events do occur (Garfin et al., 2015), it is possible that these individuals are more prone to distress and, thus, fear about similar events occurring again.
In the context of trauma, we hypothesized that experiencing temporal disintegration may precipitate greater emotional distress and, in so doing, heighten fear and worry about the reoccurrence of similar events. Individuals with a prior history of adversity may be especially prone to temporal disintegration and may therefore be vulnerable to exhibiting this pattern of responding, with implications for long-term adjustment. We evaluated this theoretical model using data collected in response to two distinct collective traumas. As proof of concept, we began by testing this path model using cross-sectional data collected from students in the aftermath of a university shooting (Study 1). To examine the durability of these effects, we then evaluated this model using an existing longitudinal dataset from a multiwave study that tracked psychological responses to the September 11, 2001 (hereafter, 9/11), terrorist attacks over time among a representative national sample (Study 2). All data and code for both studies are available on OSF (https://osf.io/y4dsc/). The studies were not preregistered.
Study 1: Cross-Sectional Data From a School Shooting
We first tested our conceptual model using a sample of students whose university experienced an active shooter event in 2016. At the time of the incident, a campus-wide lockdown alert was issued, and individuals on campus sheltered in place without any official update for 90 min. Using data comprising psychological responses to this collective trauma, we evaluated the relationships among prior adversity exposure, temporal disintegration, acute stress, and fear of future violence.
Method
Sample and design
One week after the school shooting and lockdown, 40,339 undergraduate and graduate students received a campus-wide email inviting them to participate in an anonymous, online survey; a reminder email was sent 1 week later to encourage participation during the 3-week fielding period. The participation rate was approximately 18% (n = 6,540), and most participants (92%) completed the survey within 16 days. Twenty-four participants were excluded during data cleaning because they were under the age of 18, leaving a total of 6,516 participants for the analyses. The sample identified as 62% female, 36.1% male, and 1.9% trans/genderqueer/other; ethnicity was reported as European American (39.8%), Asian American (30.2%), Latino American (13.5%), multiracial/ethnic (8.6%), African American (2.7%), or other (6%). Most of our participants (72.7%) identified the United States as their country of origin; of those from outside of the United States, country of origin varied widely, but the most reported countries were China (28.8%), India (8.3%), and Mexico (7.1%). The majority of the sample (64.7%) was undergraduates, and roughly 61% of the sample reported having been in the lockdown. Participants were not compensated for survey completion; all procedures for this study were approved by the institutional review board of the University of California, Irvine.
Measures
Prior adversity exposure
Prior exposure to adversity was assessed using five items asking whether participants had personally experienced a previous school shooting, natural disaster (e.g., flood, fire), community violence (e.g., shooting, civil unrest), combat during war, or any other form of violence prior to the shooting. Responses were dichotomously coded and summed with a range of 0 to 5; roughly three fourths (72.3%) of the participants reported exposure to at least one prior event.
Temporal disintegration
Acute shooting-related temporal disintegration was measured using six items used in previous research (e.g., Holman et al., 2016; Holman & Silver, 1998). Participants were asked to what extent they had experienced each of six reactions during the campus shooting/lockdown, including feeling as though “time had stopped,” “nothing was real,” they “were in slow motion,” they “had no future,” they were “unsure about what time or day it was,” and they found themselves “forgetting what just happened or feeling unclear about the order of events [they] just experienced.” Responses were provided using a 5-point scale ranging from 0 (never) to 4 (all of the time). The scale had very good reliability (α = .89); items were averaged (M = 0.71, SD = 0.86) to create an index.
Event-related acute stress
Acute stress responses to the school shooting were assessed using the Acute Stress Disorder Scale-5, a validated measure of acute stress symptoms (Bryant et al., 2000). Using a 5-point scale from 0 (not at all) to 4 (very much), participants indicated the extent to which they experienced 14 possible reactions “since the shooting and lockdown” (e.g., “Do you try to avoid thinking about the shooting/lockdown?”). Responses demonstrated excellent reliability (α = .91) and were averaged (M = 0.67, SD = 0.68) to create an index.
Fear of future violence
Worry about future violence was measured using two items that were adapted from a scale used in previous research on collective traumas (e.g., R. C. Silver et al., 2002; Thompson et al., 2019). Participants reported on a 5-point scale from 0 (never) to 4 (all the time) how often in the past week they had fears about the possibility of violence in their community and whether they worried that an act of violence would personally affect them or a family member in the future. Responses had good reliability (α = .83) and were averaged (M = 1.66, SD = 1.02).
Covariates
Demographic information and days since lockdown
Participants provided demographic information, including their age, gender, and ethnicity, and received a score to indicate how many days after the school shooting their survey was completed, with values ranging from 7 to 29.
Affiliation with affected department
Participants indicated whether they were affiliated with the department in which the shooting occurred; responses were dichotomously coded such that no affiliation was scored as 0 and any affiliation (e.g., being a department major/minor, have taken classes in the department) was scored as 1. Of the 6,197 participants who responded to this item, 26.9% were affiliated in some way with the affected department.
Exposure to lockdown and related events
Participants reported whether they were in the campus lockdown and whether they experienced each of 12 different exposures to the lockdown (e.g., “I heard live gunshots”). All items were dichotomously coded; the 12 exposure items were summed to create an index of lockdown exposure ranging from 0 to 12.
Traditional and social media exposure
Given the abundant evidence that exposure to traditional and social media coverage of collective traumas is linked to adverse psychological responses (e.g., Garfin et al., 2015; Hopwood & Schutte, 2017; Jones et al., 2017; Thompson et al., 2019), we sought to account for its contribution in this model. Participants indicated on a 3-point scale from 0 (not at all) to 2 (most or all of the time) how often they received information regarding the event from three traditional media sources (radio, television, online news sites) and five social media platforms (e.g., Twitter, Facebook, Snapchat) during the shooting and lockdown. Responses were dichotomously coded (0 = not at all, 1 = at least some of the time) and summed, respectively, to create two continuous counts for traditional media sources (range = 0–3) and social media sources (range = 0–5) used.
Analytic strategy
In Stata (Version 14.2; StataCorp, 2015), we used a structural equation modeling framework to conduct a path analysis examining whether prior adversity exposure and temporal disintegration were associated with acute stress responses and fear of future violence, as hypothesized. This strategy estimates multiple regression equations simultaneously, which allows a more comprehensive evaluation of model fit. The path model was tested using a full-information maximum-likelihood approach with bootstrapped standard errors, which retains cases with missing data. Covariates included days since lockdown, age, gender, ethnicity, affiliation with the affected department, presence in the lockdown, exposure to lockdown events, and exposure to information via traditional and social media.
Results
Table 1 displays the zero-order and point biserial correlations among all variables in the model for Study 1.
Correlations Among Key Variables and Covariates for Study 1 (N = 6,516)
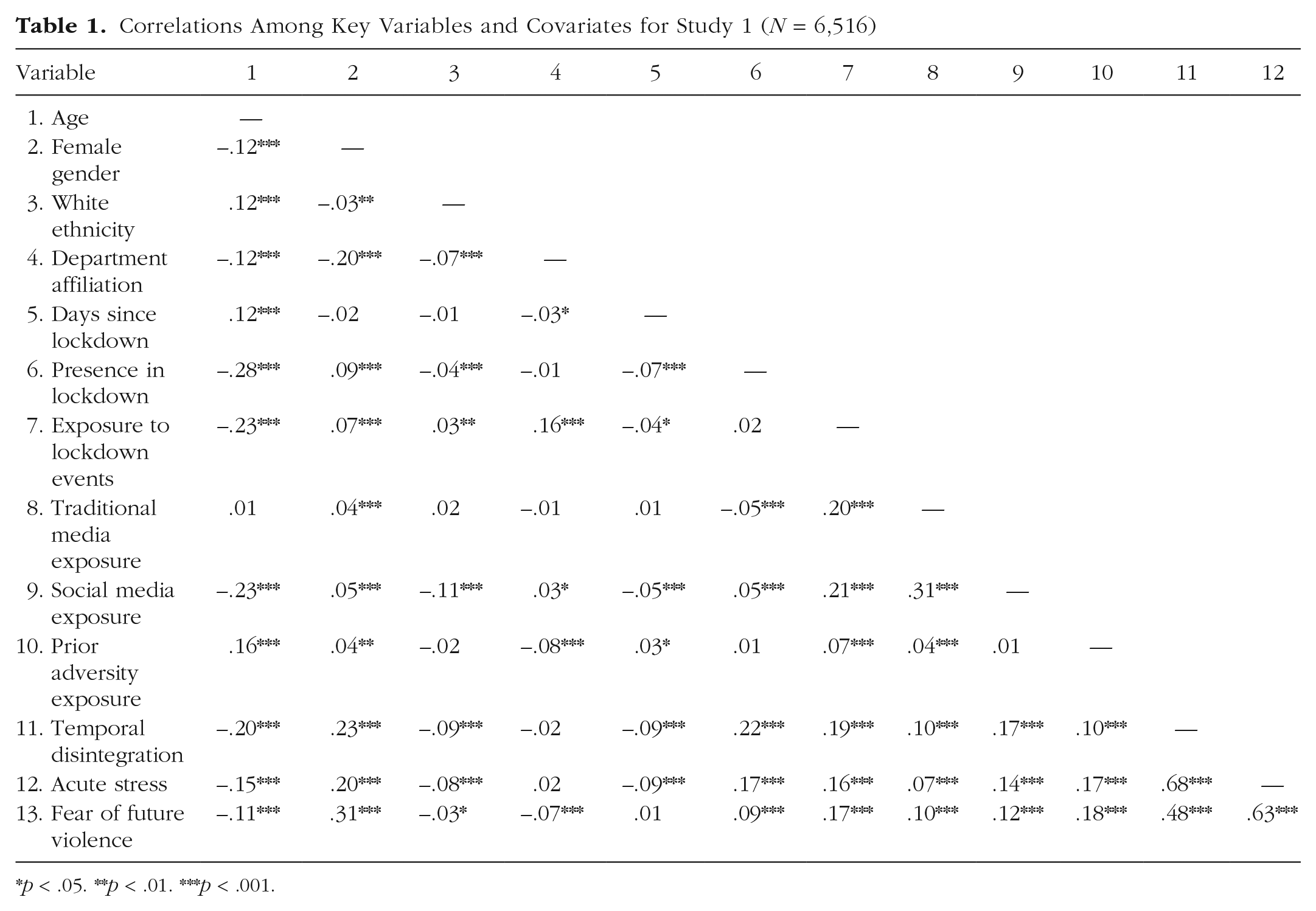
p < .05. **p < .01. ***p < .001.
Model fit
We assessed goodness of fit using the root-mean-square error of approximation (RMSEA) and the comparative fit index (CFI). For the RMSEA, acceptable values are below .08, and for the CFI, acceptable values are above .95 (Bollen, 1989; Schermelleh-Engel et al., 2003). Results for the χ2 goodness-of-fit test are also reported, although this index is not considered an appropriate indicator of model fit for large sample sizes (Kline, 2015). Using these guidelines, we found that the model fitted the data quite well, χ2(1) = 48.34, p < .001; RMSEA = .08; CFI = .99 (see Fig. 1).
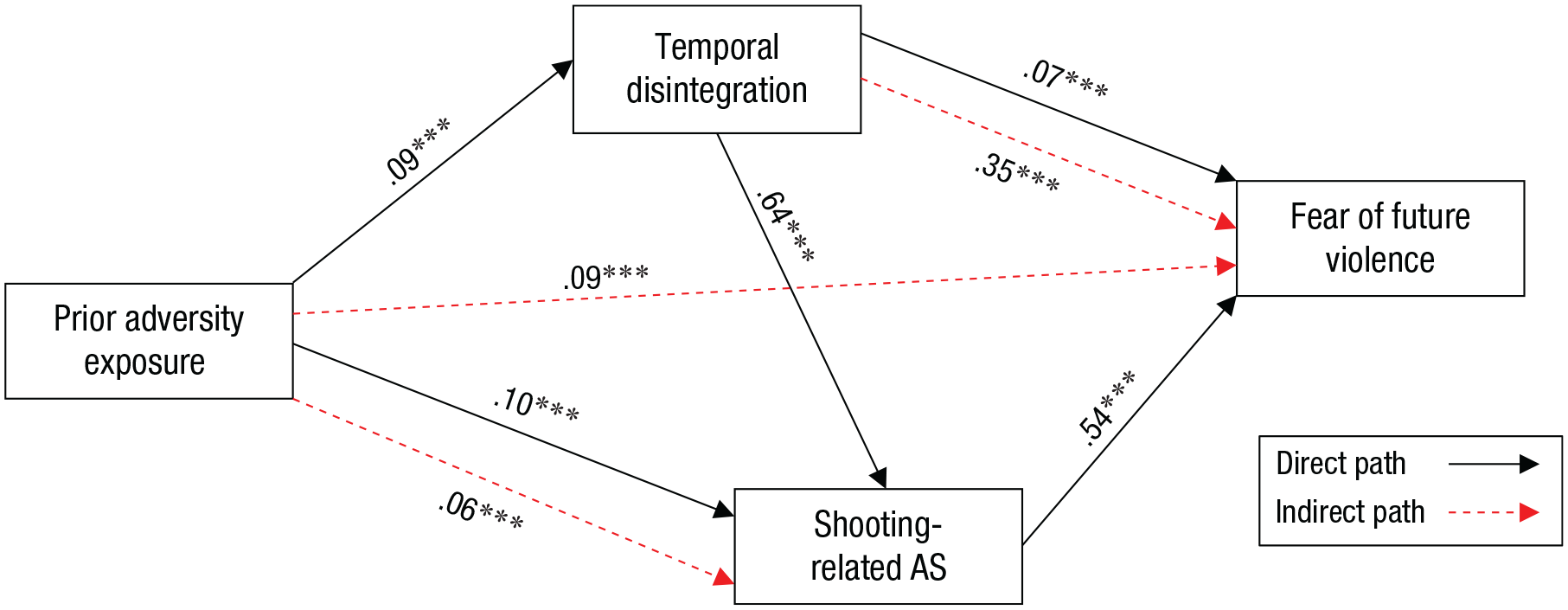
Path model of relationships between prior adversity exposure, temporal disintegration, shooting-related acute stress (AS) symptoms, and fear of future events for Study 1 (N = 6,516). Standardized coefficients are shown. Asterisks indicate significant paths (***p < .001).
Model results
We found that when analyses controlled for covariates, temporal disintegration was associated with acute stress (b = 0.51, SE = 0.01, β = 0.64, 95% confidence interval [CI] = [0.62, 0.67], p < .001), which, in turn, was associated with fear of future violence (b = 0.81, SE = 0.02, β = 0.54, 95% CI = [0.51, 0.57], p < .001). Temporal disintegration was also significantly related to fear of future violence directly (b = 0.09, SE = 0.02, β = 0.07, 95% CI = [0.05, 0.10], p < .001) and indirectly via acute stress (b = 0.41, SE = 0.01, β = 0.35, 95% CI = [0.33, 0.37], p < .001). Preshooting trauma exposure was related directly to temporal disintegration (b = 0.08, SE = 0.01, β = 0.09, 95% CI = [0.06, 0.12], p < .001) and acute stress (b = 0.07, SE = 0.01, β = 0.10, 95% CI = [0.08, 0.12], p < .001) and indirectly to fear of future violence (b = 0.10, SE = 0.01, β = 0.09, 95% CI = [0.08, 0.11], p < .001) through temporal disintegration and acute stress.
Discussion
The results of this study demonstrated that, as hypothesized, individuals who had been previously exposed to more adversity were more vulnerable to experiencing temporal disintegration at the time of the shooting and expressed greater acute stress and fear of enduring similar violent events in the future. Findings from this cross-sectional study provide initial support for our theorized model and the crucial role of temporal disintegration in understanding responses to collective traumatic events. However, the cross-sectional design of this study limits our ability to draw firm conclusions about the nature of these associations.
Study 2: Longitudinal Data Following the 9/11 Attacks
Because Study 1 demonstrated cross-sectional support for the model and the associations between prior adversity exposure, temporal disintegration, psychological distress, and fear of future trauma, we examined these relationships longitudinally in Study 2 to test their accuracy over time. Using an existing dataset from a national longitudinal study that examined short- and long-term responses to the 9/11 terrorist attacks (R. C. Silver et al., 2002), we tested whether temporal disintegration experienced during and shortly after the event predicted posttraumatic stress (PTS) symptoms 1 year after 9/11 and fear of future terrorism 2 years later, as well as whether individuals with a history of adversity were more likely to experience these responses over time.
Method
Sample and design
We used an existing dataset from a prospective longitudinal study of a nationally representative sample of Americans following the 9/11 terrorist attacks that began within days of the attacks. Knowledge Networks (KN), a Web-based survey research company, used stratified random digit dialing (RDD) telephone sampling—the standard probability sampling method at the time—to create a large, nationally representative panel of American adults. Individuals received a free Web-enabled device and Web access in exchange for completion of three to four surveys monthly. The original study sample (N = 2,729; R. C. Silver et al., 2002) was randomly drawn from the KN panel; a random sample of 1,069 panelists residing outside New York City was drawn from the original study sample to complete a second survey approximately 2 months after 9/11 (n = 933, 87% completion rate). This was the sample used for the present research. These participants subsequently received follow-up surveys at 12 (82% retention; n = 762) and 24 (76% retention; n = 582) months after 9/11 (R. C. Silver et al., 2006). The sociodemographic composition of the KN panel closely tracked that of the U.S. census counts on several variables, such as age, gender, race, Hispanic ethnicity, and geographical region, among others. Participants who had left the panel completed the surveys via paper and pencil and received the equivalent of $10 for completing each survey.
The sample was 48.2 years old on average (SD = 16.5), the gender distribution was roughly even (50.1% female), and slightly more than one quarter of the sample had completed a BA/BS college degree (26.4%). Ethnicity was reported as White, non-Hispanic (74.1%); Black, non-Hispanic (8.4%); Hispanic (10.3%); or other, non-Hispanic (7.2%). Participants were geographically located primarily in the southern United States (37.7%), followed by the western United States (22.5%), midwestern United States (20.4%), and northeastern United States (19.4%).
Measures
Prior adversity exposure
Lifetime exposure to stressful and traumatic events was assessed approximately 2 months after the attacks (see Seery et al., 2010). Participants reported whether they had ever experienced any of 37 events (e.g., personal losses, natural disaster, physical violence). Responses were summed to create a continuous score representing the number of adversities experienced in their lifetime; scores ranged from 0 to 24, with most participants (88.2%) reporting exposure to at least 1 prior event.
Temporal disintegration
9/11-related temporal disintegration was assessed 2 months after the attacks using the same six items from Study 1. Participants indicated the extent to which they had experienced various reactions during and immediately after the attacks, such as time slowing down or stopping and feeling “unsure of what day or time” it was. Items were scored on a 5-point scale from 1 (never) to 5 (all of the time) and averaged (M = 1.78, SD = 0.79), with very good reliability (α = .87).
9/11-related PTS symptoms
9/11-related PTS symptoms were assessed 12 months after the attacks using the Posttraumatic Stress Disorder Checklist-Civilian Version (PCL; Weathers et al., 1993). The PCL is a valid and reliable 17-item measure of intrusion, avoidance, and arousal symptoms. Using a 5-point scale from 1 (not at all) to 5 (extremely), participants reported how distressed and bothered they were by symptoms pertaining to the 9/11 attacks over the prior month. Items demonstrated excellent reliability (α = .93), so responses were averaged (M = 1.32, SD = 0.49) to create mean PTS scores.
Fear of future terrorism
Fear and worry about future terrorism were assessed 2 years following the attacks using a modified version of the same two-item measure from Study 1. Specifically, participants were asked how often in the past week they had fears about the possibility of a terrorist attack (e.g., bioterrorism, hijacking) and to what extent they worried that an act of terrorism would personally affect them or a family member in the future. Responses were made on a 5-point scale ranging from 1 (never) to 5 (all the time) and were averaged (M = 2.08, SD = 0.87) to form an index with good reliability (α = .83).
Covariates
Demographic information and mental health history
In a separate survey administered by KN prior to the 9/11 attacks, participants provided demographic information, such as their age, gender, ethnicity, income, and education, which were included as covariates given prior work documenting sociodemographic differences in trauma-related stress responses (Kilpatrick et al., 2017). They also reported whether a physician had ever diagnosed them with a depressive or anxiety disorder; these responses were scored dichotomously and summed to range from 0 to 2 (0 = none, 1 = either anxiety or depression, 2 = both).
Exposure to the 9/11 attacks
Exposure to the attacks was assessed using several items drawn from prior work (Koopman et al., 1994) that reflected the degree of proximity a participant had to the attacks (R. C. Silver et al., 2002). Individuals were categorized as directly exposed (e.g., close enough to hear or feel the attacks, in the World Trade Center or the Pentagon, within a few blocks), indirectly exposed (e.g., witnessed the attacks via live TV coverage as they occurred), and no live exposure (e.g., learned of attacks only after they occurred). Given substantial evidence of the negative psychological impact of exposure to collective traumatic events via media coverage (e.g., Holman et al., 2014; Hopwood & Schutte, 2017), indirect exposure was also assessed as the number of hours per day participants watched TV news coverage of the event in the week immediately following the attacks (1 = < 1 hour, 2 = 1– 3 hours, 3 = 4–6 hours, 4 = > 6 hours).
Analytic strategy
Statistical analyses were conducted in Stata (Version 14.2; StataCorp, 2015). We followed the same analytic practice as discussed in Study 1, using structural equation modeling to conduct a path analysis to examine the relationships in the proposed model. A full-information maximum-likelihood estimation approach with bootstrapped standard errors was used to account for missing data and retain all participants in the sample. Covariates in this analysis were age, gender, ethnicity, educational attainment, household income, pre-9/11 mental health history, and direct and media exposure to the 9/11 attacks.
Results
Zero-order and point biserial correlations for all variables in the model are reported in Table 2.
Correlations Among Key Variables and Covariates for Study 2 (N = 932)
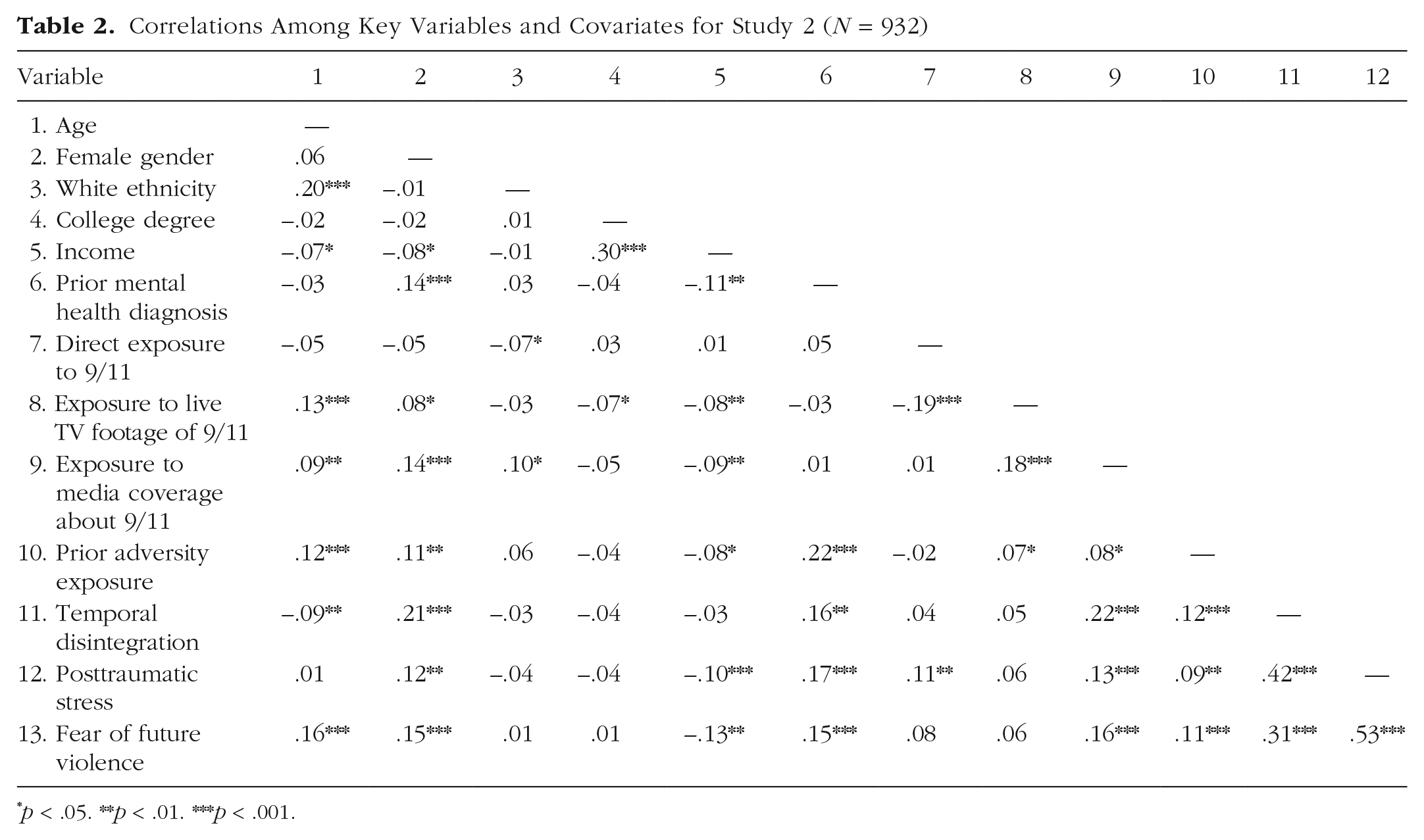
p < .05. **p < .01. ***p < .001.
Model fit
As in Study 1, model fit here was assessed using the RMSEA and CFI, and results from the χ2 goodness-of-fit test are also reported. According to these indices, the model fitted the data very well, χ2(1) = 0.18, p = .671; RMSEA = .01; CFI = 1.00 (see Fig. 2).
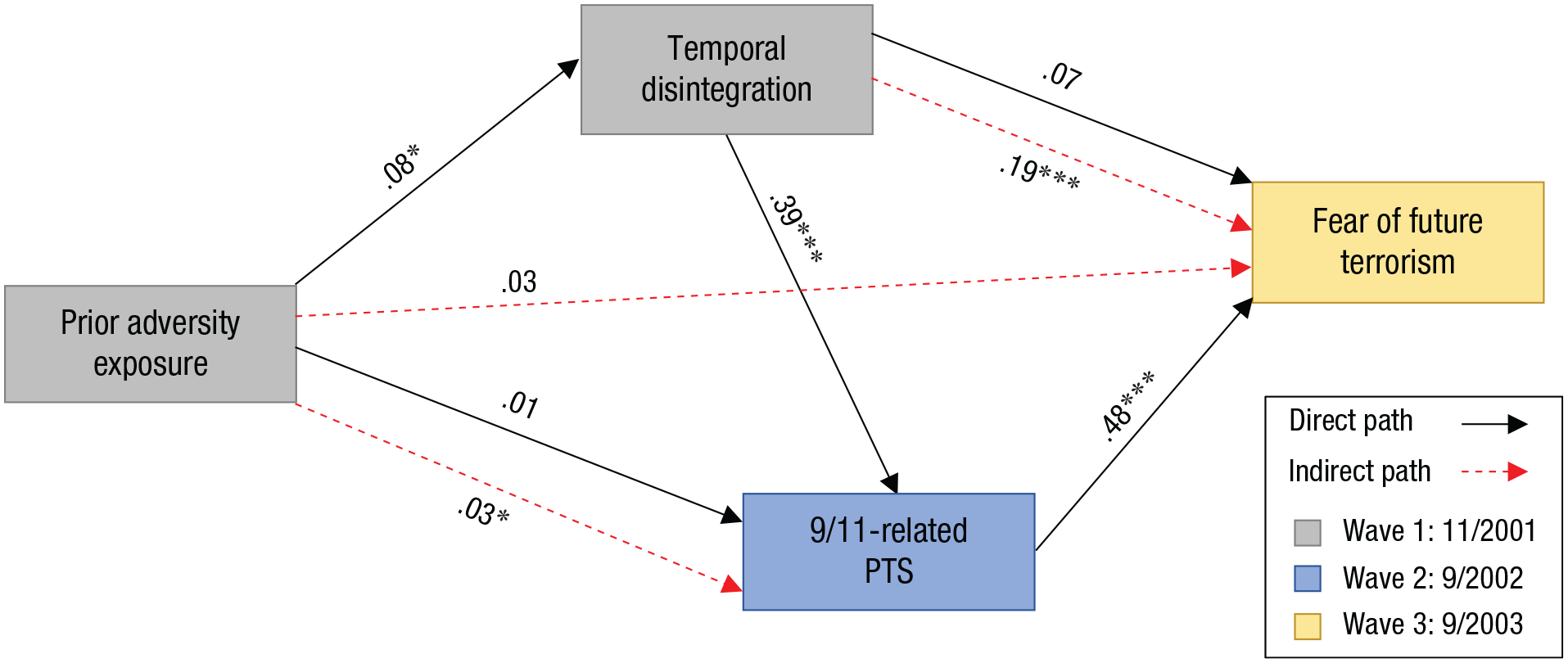
Path model of relationships between prior adversity exposure, temporal disintegration, 9-11/related posttraumatic stress (PTS), and fear of future terrorist events for Study 2 (N = 932). Standardized coefficients are shown. Asterisks indicate significant paths (*p < .05, ***p < .001).
Model results
Study 2 partially replicated the results from Study 1. We found that, controlling for covariates, prior adversity exposure predicted temporal disintegration 2 months after the attacks (b = 0.01, SE = 0.01, β = 0.08, 95% CI = [0.01, 0.14], p = .021), which in turn, was associated with 9/11-related PTS a year later (b = 0.24, SE = 0.03, β = 0.39, 95% CI = [0.28, 0.46], p < .001). Fear of future terrorism 2 years after the attacks was uniquely predicted by PTS (b = 0.84, SE = 0.08, β = 0.48, 95% CI = [0.40, 0.57], p < .001) but, unlike in Study 1, not by temporal disintegration (b = 0.08, SE = 0.04, β = 0.07, 95% CI = [−0.01, 0.14], p = .082). However, although the direct association between temporal disintegration and fear of future terrorism was not significant, temporal disintegration was indirectly associated with fear of future terrorism via PTS (b = 0.21, SE = 0.03, β = 0.19, 95% CI = [0.13, 0.23], p < .001). Adversity exposure prior to the terrorist attacks was not directly associated with PTS (b = 0.01, SE = 0.01, β = 0.01, 95% CI = [−0.05, 0.07], p = .66) as it was in Study 1, but the indirect path via temporal disintegration was significant and was replicated (b = 0.01, SE = 0.01, β = 0.03, 95% CI = [0.01, 0.05], p = .027). Finally, the indirect path from prior adversity exposure to fear of future terrorism 2 years later was not significant (b = 0.01, SE = 0.01, β = 0.03, 95% CI = [−0.01, 0.06], p = .12).
Discussion
The results from Study 2 replicated findings from Study 1, revealing that experiencing temporal disintegration in the immediate aftermath of 9/11 predicted more PTS symptoms 1 year later, which then predicted greater fear and worry about future terrorism 2 years after the attacks. Again, individuals who had a history of greater adversity appeared predisposed to experience temporal disintegration and the pattern of distress and fear it precipitates, putting an already vulnerable population at greater risk for long-term adverse mental health outcomes.
General Discussion
Across two studies, we demonstrated that temporal disintegration experienced during or soon after a collective trauma was associated with elevated distress responses, both in the acute aftermath and over time, and that elevated distress, in turn, was associated with heightened fear of the reoccurrence of another such event in the future. Importantly, the longitudinal findings in Study 2 were robust when analyses controlled for pre-9/11 mental health history, suggesting that they were not an artifact of preexisting mental health problems. Our results further suggest that individuals with a history of exposure to adversity may be particularly vulnerable to this pattern of responding, especially as they continue to experience these events over time. Although not all indirect pathways were significant across both studies, temporal disintegration was consistently linked to greater worry about the reoccurrence of trauma via heightened distress in response to the collective trauma. This convergent finding suggests that acute temporal distortions at the time of trauma may play a role in shaping how people perceive, and what they expect in, the future—even up to 2 years later.
By linking temporal disintegration to future fears, our results also suggest that temporal distortion during the acute phase of a trauma may contribute to an enduring cycle of adverse psychological responding. Ongoing worry about future negative events is a form of perseverative cognition known to exacerbate affective response to stress (Brosschot et al., 2006), including acute stress responses to subsequent collective traumas (Thompson et al., 2019). By prompting fears of future trauma reoccurrence, temporal disintegration may be an entry point for a maladaptive cycle of distress and fear in which trauma-exposed individuals become sensitized to future adversity with adverse consequences for mental health. To the extent that perseverative cognition and worry are associated with physiologic responses to stress (Brosschot et al., 2006), this deleterious cycle of distress could also have implications for physical health, as a growing literature has linked both perseverative cognition and acute stress responses with subsequent physical health problems (Kubzansky et al., 1997; Ottaviani et al., 2016; Song et al., 2019). Future research should explore this potential downward spiral and further examine the characteristics and lived experiences that predispose individuals to this temporal distortion and subsequent patterns of perseverative cognition. By identifying these indicators of risk, health professionals could then more effectively target trauma-exposed individuals most susceptible to these detrimental processes and intervene early to delay or stop their progression.
Although our primary hypotheses were supported and successfully replicated using a national longitudinal sample, not all findings across both studies were consistent. For example, whereas the direct paths from prior adversity exposure to PTS and from temporal disintegration to future fears were statistically significant in Study 1, these paths failed to reach significance in Study 2. One possible reason for this inconsistency is the difference in design: direct effects found cross-sectionally may capture valid relationships that decayed over time or simply be an artifact of the confounding nature of collecting data at a single time point. Alternatively, the lack of replication of this path in Study 2 may be attributable to the inclusion of pre-event mental health as a covariate, as it may predispose individuals to both temporal disintegration and future fears. The bivariate correlations from our second study suggest that this may be the case. Using retrospective data collection in Study 2 to assess whether participants experienced temporal disintegration 2 months earlier may have introduced recall bias and thus contributed to the failure to replicate these paths. Nonetheless, future work should assess the durability of these direct paths longitudinally using more proximal data collection intervals and controlling for preexisting mental health diagnoses to explore possible explanations for the lack of replication of this path’s significance.
Another limitation concerns the potential conceptual overlap between temporal disintegration and other general distressed states. Some items of the temporal disintegration scale describe experiences that are like symptoms of depression (e.g., feeling of having no future) or psychosis (e.g., feeling that nothing is real) when experienced outside the context of trauma. Thus, it is possible that participants’ responses to these items may have captured both the prevalence of symptoms representing trauma-related temporal disintegration and those that, outside the context of trauma, represent other distressed states. To help rule out this possibility, we included prior mental health history as a covariate in Study 2; although this measure was not a comprehensive inventory of prior psychological symptoms or disorders, it helped account for pre-9/11 diagnoses of depression and/or anxiety disorders, which can have overlapping symptoms.
Moreover, we found that, as displayed in Tables 1 and 2, temporal disintegration was related to temporal distance from the event and event-related media exposure such that participants with closer temporal proximity (Study 1) or greater indirect exposure via the news media (Studies 1 and 2) reported greater temporal disintegration, providing some evidence that temporal disintegration scores were indeed tied to the event itself and not simply a reflection of psychological symptoms unrelated to the trauma. Nonetheless, to better differentiate symptoms of trauma-related temporal disintegration from symptoms of psychopathology, future research could assess and control for diagnoses of disorders that share similar symptoms, such as dissociative disorders, when examining the links between temporal disintegration, distress, and worry about the future.
The types of prior adversity examined as a risk factor for temporal disintegration also differed across the two studies: Study 1 focused primarily on community-based violence exposures to match the event under study, whereas Study 2 included a more comprehensive array of 37 adverse events. Evidence suggests that interpersonal violence may be especially detrimental for posttraumatic mental health (Kessler et al., 2017) and that repeated exposure to the same type of adversity, such as community-based collective trauma, sensitizes people to similar subsequent events (e.g., Garfin et al., 2015). Furthermore, prior work has found that people who were exposed to chronic trauma were more likely to experience temporal disintegration than those with a history of acute trauma (Holman & Silver, 1998), suggesting that the chronicity of prior adversity exposure may also impact its relationship with temporal disintegration and subsequent mental health responses. Given that Study 2 did not replicate the role of temporal disintegration as a mediator of the association between prior adversity and worry, future research should compare whether previous exposure to specific types and durations of adversity (e.g., childhood adversity, interpersonal/sexual violence) differentially predispose individuals to experiencing temporal disintegration to a degree that worsens downstream outcomes over time.
We also note that the participation rate was relatively low in Study 1. Because Study 1 was conducted using a nonrepresentative convenience sample of students enrolled at a university at which an active shooter event occurred, it is possible that selection bias affected the findings; to address this concern, we complemented the sample in Study 1 with a nationally representative sample in Study 2 and found consistent results, which suggests that the data used in Study 1 may not have been strongly impacted by selection bias. We also acknowledge another methodological limitation in that there was attrition across waves of data collection in Study 2; consistent with prior work, our results showed that individuals who were older and identified as White were more likely to be retained over time (e.g., R. C. Silver et al., 2002; Thompson et al., 2019). However, by using the full-information maximum-likelihood approach in structural equation modeling and bootstrapping the standard errors, we were able to maintain the full, more diverse sample for these analyses.
For many years, the concept of time received scant empirical consideration in the trauma literature, despite clinical and scholarly evidence suggesting its crucial role in posttraumatic adjustment. However, trauma researchers have begun pushing for greater exploration of time to better understand its significance in the context of coping with and moving past difficult experiences (e.g., Saltzman, 2019), even developing time-based therapies to treat posttraumatic stress disorder (e.g., Sword et al., 2014). Recent collective traumatic events, such as the COVID-19 pandemic, have further highlighted the need for greater research on trauma-related distortions in time perception, especially those such as temporal disintegration that have been connected to detrimental psychological outcomes years later (Holman & Grisham, 2020). Cultivating our knowledge of antecedent and mitigating factors for temporal disintegration may strengthen our ability to effectively prevent this deleterious response pattern and buffer individuals against its long-term consequences.
Footnotes
Acknowledgements
We thank Christine Dunkel Schetter, Maryann J. Gray, and Dana Rose Garfin for their valuable input to Study 1. We also thank Michael Poulin, Virginia Gil-Rivas, Judith Pizarro Andersen, and Daniel McIntosh for their conceptual/methodological contributions to Study 2 and the Knowledge Networks Government, Academic, and Nonprofit Research Team for their support with data collection.
Transparency
Action Editor: Vina Goghari
Editor: Jennifer L. Tackett
Author Contributions
Correction (March 2023):
Article updated to include the Open Data and Open Materials badges and the Open Practices statement.