
Abstract
In this epidemiological investigation, we assessed the prevalence of depression and anxiety symptoms during the COVID-19 pandemic. A total of 10,061 adults participated in the study. Symptoms of depression and anxiety were 2 to 3 times higher compared with prepandemic samples. Participants who predominantly socially distanced themselves revealed substantially higher symptoms than their counterparts. Females, ethnic and sexual-orientation minorities, younger adults, unemployed individuals, and participants with a psychiatric diagnosis reported higher prevalence of psychological symptoms. Worry about prolonged duration of physical-distancing protocols and frustration of autonomy was associated with elevation in symptoms of depression and anxiety. Increased competence to deal with the pandemic crisis was associated with fewer adverse symptoms. Physical exercise, experiencing nature, and distraction with activities were associated with reduced depressive symptoms but not anxiety. The extent of information access about the pandemic was associated with reduced anxiety symptoms. Furthermore, adherence to mitigation protocols was investigated. Younger adults and males reported lowest adherence. Altruistic attitudes, in addition to mandatory as opposed to voluntary adherence, were associated with higher adherence rates. Worrying about the health of significant others was associated with higher adherence rates, whereas worry about duration of pandemic protocols was associated with lower adherence rates.
The spread of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), known as the coronavirus disease (COVID-19), has accumulated into an ongoing pandemic with profound impacts on global public health. On January 30, 2020, the outbreak was declared an international public health emergency by the World Health Organization (WHO). As of October 1, 2020, 34 million confirmed cases had been reported, accompanied by more than 1 million coronavirus-related deaths (WHO, 2020). While awaiting the implementation of an efficacious vaccine into routine health care, countries around the globe have employed disease-containment strategies aimed at impeding viral transmission chains. These strategies are collectively referred to as nonpharmacological interventions (NPIs; Ferguson et al., 2020). NPIs are mitigation strategies designed to decrease physical contact among individuals in a community with the goal of reducing the reproduction number R0, the average number of secondary cases generated by each positive case (Ferguson et al., 2020). The term NPI is commonly used interchangeably with physical-distancing or social-distancing protocols. Note that a variety of NPIs are contemporaneously in practice worldwide, and many countries have implemented strategies including lockdowns (e.g., physical closure of schools and universities), social distancing from peers and public activity, quarantine, and isolation.
Consequently, accompanied by the realization that the end of the crisis is not yet in sight, a different dimension of public health that requires urgent attention has emerged. This concerns the associations between mental health symptoms and the NPIs implemented during the COVID-19 pandemic (e.g., Holmes et al., 2020; “Keep mental health in mind,” 2020). Given that many of these NPIs are concurrently in operation globally, their potentially detrimental associations with the health status of the general public have now become a prime concern of clinicians, scientists, and health policymakers. This matter is further reflected by numerous calls for papers urging that mental health be taken into consideration (e.g., Brooks et al., 2020; Galea et al., 2020; Holmes et al., 2020; “Keep mental health in mind,” 2020; “Science in the time of Covid,” 2020; Pfefferbaum & North, 2020; Venkatesh & Edirappuli, 2020; Yao et al., 2020).
Among the psychological symptoms highlighted for investigation in the general population, depression and anxiety are critical (Brooks et al., 2020; Galea et al., 2020; “Keep mental health in mind,” 2020; Venkatesh & Edirappuli, 2020; Yao et al., 2020). Depression and anxiety are two prevalent domains of mental health symptoms; the former primarily encompasses persistent feeling of sadness and loss of interest, whereas the latter mainly comprises extensive and persistent apprehensive expectation about a number of events and activities (American Psychiatric Association, 2013). Note that previous findings have indicated that acute life events, bereavement, and financial crises often precede the onset and maintenance of depression (Herman et al., 2019; Lund et al., 2018; Paykel, 2003). Likewise, anxiety disorders have been revealed to be aggravated by stressful events (Tyrer & Baldwin, 2006). An increase in depression and anxiety is concerning given the disorders’ tendencies to persist following termination of the eliciting situation, relapse rates, economic and societal costs, quality-of-life impairments, as well as associated mortality rates (Herman et al., 2019; Lund et al., 2018; Patel et al., 2016; Tyrer & Baldwin, 2006).
Thus, large-scale screenings of these mental health symptoms using specific validated instruments including the Patient Health Questionnaire (PHQ-9) and the Generalized Anxiety Disorder 7 scale (GAD-7) have been urgently called for, providing an overview of the current prevalence estimates of mental health symptoms during the pandemic (e.g., “Keep mental health in mind,” 2020). In addition, large-scale assessments are imperative for identifying groups of individuals vulnerable to unfavorable mental health outcomes. Insight into specific symptom-level increases and the factors associated with such changes provides a foundation for knowledge concerning the treatment needs of the population as well as the ground on which the development of context-specific preventive and interventive measures are to be based (e.g., Brooks et al., 2020; Galea et al., 2020; “Keep mental health in mind,” 2020; Venkatesh & Edirappuli, 2020; Yao et al., 2020). Such an investigation further provides an initial evaluation of the mental health symptoms associated with the globally omnipresent NPIs. Moreover, the issue of adherence to NPIs is noteworthy because lockdown and social-distancing strategies are ineffective if individuals do not adhere to them (e.g., Brooks et al., 2020). This accentuates the importance of investigating factors associated with adherence to NPIs, which is deemed vital in the current time-sensitive battle against the pandemic.
In recent calls for papers (e.g., Brooks et al., 2020; Galea et al., 2020; Holmes et al., 2020; “Keep mental health in mind,” 2020; Pfefferbaum & North, 2020; “Science in the time of COVID-19,” 2020; Venkatesh & Edirappuli, 2020; Yao et al., 2020), numerous factors have been suggested to be associated with the potential increases in mental health problems, and other variables are hypothesized to be related to adherence difficulties. In nonpandemic settings, factors associated with increases in depressive and anxiety symptoms include female gender (McLean et al., 2011; Nolen-Hoeksema, 2001), younger age (Molarius et al., 2009), being single (Scott et al., 2010), lower education (Bjelland et al., 2008), and involuntary job loss (Linn et al., 1985). Furthermore, several other factors have been deemed important to investigate regarding depressive and anxiety symptoms in pandemic settings. These include frustration of autonomy, commonly observed as a result of imposed behavioral restrictions during pandemics, as well as perceived lack of competence, which is of increased relevance in novel uncertain situations and has been previously associated with detrimental psychopathological symptoms (e.g., Tindall & Curtis, 2019). In addition, calls have been made (e.g., Brooks et al., 2020) for investigations into the relationship between these symptoms and the extent of information access and worry about the duration of implemented pandemic protocols because these cognitive variables are hypothesized to be associated with detrimental mental health symptoms. Furthermore, it remains unclear whether protective behaviors such as physical activity and distraction with other positive activities (a common emotion-regulation technique) are beneficial for mental health during pandemics and whether such factors may alleviate the symptoms of depression or anxiety alone or benefit both symptoms.
Likewise, a great deal remains unknown concerning which factors are associated with adherence to NPIs. Considering the mixed evidence concerning demographic characteristics associated with adherence in previous pandemics (Webster et al., 2020), the role of gender, age, and educational level remains unclear. Access to information and altruistic attitude have been theorized to increase adherence (e.g., Brooks et al., 2020; Webster et al., 2020). Likewise, worry about the duration of pandemic protocols (e.g., Brooks et al., 2020; Webster et al., 2020), the role of fear for one’s own and significant others’ health, and the relationship between psychopathology and adherence remain uninvestigated. Because individuals with considerable depressive and anxiety symptoms reveal higher risk aversion (e.g., Maner et al., 2007), both symptoms could be associated with increased adherence to pandemic protocols. However, considerable depressive symptoms have previously been linked with lower adherence in other settings (e.g., DiMatteo et al., 2000), indicating that such problems could also likely be associated with reduced adherence to pandemic protocols, thus requiring empirical investigation. Furthermore, situational variables such as one’s employment status and the ability to work from home, which is highly relevant for maintaining quarantine orders, and suspicions of having contracted the virus are potentially relevant factors that may influence adherence behavior. These aforementioned factors not only require empirical examination in the context of the COVID-19 pandemic but also, more importantly, are of increased utility when examined with a multifactorial approach that takes into account the relative strength of each variable while controlling for other relevant variables.
In the present research, we thus aimed to empirically clarify the relationship between these theorized and called for variables in terms of (a) central psychological symptoms (i.e., depression and anxiety) and (b) adherence. The presented findings are of utility toward identification of important factors that may aid in reducing the mental health burden of pandemics while increasing adherence to NPIs.
Method
The present cross-sectional study is part of the Norwegian COVID-19, Mental Health and Adherence Project and is conducted in accordance with the guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology statement (STROBE; Von Elm et al., 2007). Health estimates were reported in accordance with the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) statement (Stevens et al., 2016). The study was registered on Clinicaltrials.gov (Identifier: NCT04356365) before any examination or analysis of the data and after the data-collection period. All elements of the submitted study adhere to its preregistered protocol.
Study design and participants
In this cross-sectional and epidemiological study, we investigated the mental health status of the general adult population and adherence to NPIs aimed at impeding viral transmission chains across all regions in Norway during the ongoing COVID-19 pandemic. These regions serve a geographically defined area of approximately 5.3 million individuals, the population of Norway, all serving under identical nationally initiated NPIs. The study design involved the inclusion of a proportionate number of participants from each region of Norway compared with the population of the region. Eligible participants were all adults 18 years and older currently living in Norway and thus experiencing identical NPIs who provided informed consent to participate in the study. The period of data collection was from March 31, 2020, through April 7, 2020. This encompasses a time frame during which all NPIs were in place and held constant during the 2 weeks before data collection as well as during the data-collection week. Furthermore, no new information was provided by the government during this period concerning changes of NPIs, keeping expectation effects constant.
The stopping rule for data collection was designed to ensure that the NPIs were held constant across all counties for 2 weeks before and during the week of the data-collection period and controlled for expectation effects by stopping data collection instantly once information concerning modification of NPIs was provided.
Ethical approval of the study was granted by the Regional Committee for Medical and Health Research Ethics and the Norwegian Centre for Research Data (reference numbers 125510 and 802810, respectively), who approved the study protocol and analysis plan before data collection.
Procedure
The dissemination of the online survey was systematically conducted through six platforms to obtain a probability sample. Because of infection guidelines concerning viral transmission and the time-sensitive nature of a study with the aim of measuring mental health during a period with identical NPIs, we could not disseminate the survey through conventional methods such as access to postal services. Consequently, the survey was disseminated online through various national, regional, and local platforms. The target population (i.e., Norwegian adults) consisted of approximately 4.2 million individuals. To give the adult population an equal opportunity to participate in the study, the survey was disseminated in six ways.
The majority of the sample (i.e., 70%) was obtained randomly using a Facebook Business algorithm, and imputed parameters reached a population of 3.6 million adults, proportionately targeting each region compared with its relative size. The final number of individuals reached through this method encompassed a random selection of 174,885 of these 3.6 million individuals. Because Facebook includes 85% of the Norwegian adult population (i.e., 3.6 million of 4.2 million), five other methods were used to maximize the probability of reaching the residual 15% of the adult population (i.e., 600,000 individuals): (a) through broadcasting on the national news channel of Norway, with approximately 1.1 million viewers at the time of broadcast and (d) through national radio stations, (c) regional and local radio stations across the country, (d) national newspapers, and (e) regional and local newspapers across the country as well as additional local and regional media and social media sources. These national, regional, and local advertisements contained brief messages about the possibility to partake in a study at the University of Oslo about mental health in the adult population. Consequently, among the 10,061 participants in this study, close to 70% were obtained randomly among the pool of Norwegian adults on Facebook (3.6 million; 85% of the adult population), whereas 30% were obtained through the other methods to reach the residual 15% of Norwegian adults. The sampling procedure and the population distribution used for the calculation of the poststratification weights (elaborated in the Statistical Analyses section) are portrayed in Figure S1 in the Supplemental Material available online.
Measurement
The survey consisted of a list of items elaborated below, administered in a random order. The demographic variables included sex, self-reported identification with sex, age, education, ethnicity, marital status, and employment status.
In terms of psychological symptoms, validated screening measures routinely used in practice to assess symptom levels suggestive of psychological diagnosis were used. The PHQ-9 and GAD-7 were specifically chosen because of the limited overlap of the items in each respective measure with regard to symptoms of depression and anxiety, allowing the examination of unique risk factors associated with each symptom group, as called for in the literature (e.g., “Keep mental health in mind,” 2020), and how such variables may be divergently related to them. The PHQ-9 (Kroenke et al., 2001) consists of nine items scored on a 4-point Likert scale (0–3); the total possible score ranged from 0 to 27. Higher scores on the PHQ-9 indicate greater depression severity, and scores 10 and above are considered to indicate a depressive diagnosis with a sensitivity and specificity of 88% (Kroenke et al., 2001). The internal consistency of this scale was good in this sample, with a Cronbach’s α of .88.
The GAD-7 (Spitzer et al., 2006) consists of seven items measuring anxiety on a 4-point Likert scale (0–3); total possible scores ranged from 0 to 21. For GAD-7, internal consistency was good, with a Cronbach’s α of .88. Higher scores indicate greater anxiety severity. A commonly used cutoff for GAD-7 scores includes 8 or above, which has been further validated as the cutoff for determining the presence of an anxiety disorder in Norwegian samples (Johnson et al., 2019). Another commonly used cutoff for GAD-7 includes 10 and above (Spitzer et al., 2006). Consequently, we report the results for both these cutoffs, presenting the one appropriate for Norwegian samples in the Results section and the results for the cutoff value of 10 in Table S1 in the Supplemental Material. Symptoms of health anxiety were measured with two items from the validated Health Anxiety Inventory (HAI; Salkovskis et al., 2002), one item measuring specific fear of being infected by coronavirus (“I fear being infected by the coronavirus”) and an item measuring fear of dying because of the coronavirus (“I fear dying through contracting the coronavirus”) on a 4-point Likert scale (0–3). Internal consistency was good for health anxiety, with a Cronbach’s α of .79.
Adherence to NPIs was measured by asking the participants how well they managed to follow each of the specific NPIs employed by the Norwegian government (for a full list of the NPIs in place during the measurement period, see Table S2 in the Supplemental Material; for the full list of the items measuring adherence, see Table S3 in the Supplemental Material). Internal consistency was acceptable for this scale, with a Cronbach’s α of .66. Scores range from 0 to 32, measuring the degree of adherence on a 5-point Likert scale (0 = no days at all, 1 = some days, 2 = half of the days, 3 = almost every day, 4 = every day), operationalized regarding the approximate number of days during which participants managed to follow each NPI during the preceding 14 days.
Situational variables included two dichotomous variables, involuntary job loss related to the COVID-19 pandemic and voluntary adherence compared with mandatory adherence to social-distancing measures. Other situational variables included extent of access to information related to the coronavirus and NPIs, frustration of autonomy, perceived competence to deal with the pandemic (“I feel confident in in my abilities to deal with the challenges related to the pandemic crisis”), and difficulty to work from home, all measured on 4-point Likert scales (0–3). Finally, participants were asked the number of days out of the preceding 14 days that they had socially distanced themselves from peers and public activity. Participants who reported to have socially distanced themselves for at least 10 of the preceding 14 days were coded as having predominantly followed distancing protocols.
Cognitions, fears, and worries related to the pandemic were measured, including worry about significant others being infected by the virus (“I worry about those close to me contracting the coronavirus), worry about transmitting others with the coronavirus (“I worry about transmitting others with the coronavirus”), and worry about prolonged duration of the implemented NPIs (“I worry that the implemented pandemic protocols may be extended further in duration”), all measured on 4-point Likert scales (0–3). Suspicious of being infected by the coronavirus was measured dichotomously (i.e., on a yes or no scale) with a single item (“Have you suspected having contracted the coronavirus during the past two weeks?”). Altruism was measured with the single item, “It is important for me to follow the pandemic mitigation protocols (i.e., NPIs) to help my fellow human beings and society,” measured on a 4-point Likert scale (0–3). Three protective variables were assessed: (a) experiencing nature; (b) distraction with positive activities one would otherwise not have the time for during nonpandemic everyday life, measured on a 4-point Likert scale (0–3); and (c) frequency during the preceding 2 weeks of physical activity, defined as lasting at least 30 min and leading to at least light sweat or increased pulse. Finally, the presence of a preexisting psychological diagnoses was queried; the participants were asked to report whether they currently have a formal psychiatric diagnosis given by a health care professional.
Statistical analyses
All statistical analyses were performed using the R software environment (Version 4.0.2; R Core Team, 2020). Descriptive analyses were reported using means and standard deviations, and difference tests between subgroups were conducted using χ2 tests. In calculating the percentage of participants who met the cutoffs for PHQ-9 and GAD-7, 10,000 bootstrap simulations were conducted to generate 95% confidence intervals (CIs). Three multiple linear regression analyses were conducted, one for each dependent variable: (a) depressive symptoms, (b) anxiety symptoms, and (c) adherence to NPIs. The inference criteria (i.e., p < .001) for all analyses was predefined taking into consideration the large sample size and the number of investigated relationships to account for multiple testing and further minimize the risk of Type I errors. In total, 45 relationships were investigated (i.e., three regressions including 15 predictors each), thus yielding a Bonferroni-corrected α level of .05/45 = .001. Adjusted R2 was used instead of R2 because it accounts for the number of predictors in the model, increasing explained variance only if the added variables improve the model than what is expected by chance.
To investigate the relative importance and strength of the different factors compared with one other, we calculated effect sizes using part correlations (semipartial correlations), which provide easily interpretable effect estimates and represent the least biased estimates of the strength of a predictive relationship (Dudgeon, 2016). They reveal the correlation between the dependent variable and the aspects of the predictor variable that are unique when accounting for all other predictors. As correlation estimates, they are evaluated in accordance with the standards provided by Cohen (1988): Values above .10 were regarded as small effects; values above .30 were regarded as medium effects; and values above .50 were regarded as large effects. The assumptions of multiple regression were checked, and multicollinearity diagnostics were conducted in accordance with common guidelines (variance inflation factor < 3; tolerance > .20; Hocking, 2013). Each model assesses the joint and unique contribution of the included predictors and accounts for possible correlations between them. Outliers were examined using Cook’s distance statistics, which allows for the detection of data points that can bias the results.
The survey involved voluntary participation and is thus susceptible to oversampling and undersampling of certain subgroups. To deal with this problem and take the most conservative and accurate approach concerning inference to the adult population, we assigned all overrepresented and underrepresented subgroups appropriate weights proportionate to the exact distribution of each subgroup in the Norwegian population. More weight was assigned to underrepresented units and less weight to overrepresented units. Specifically, age, sex, education, geographic region, ethnic distribution proportionate to each ethnic group, and the percentage of health care and social workers were all weighted to represent their exact distributions and frequencies in the population. The precise distributions used for the calculation of these poststratification weights are portrayed in Figure S1 in the Supplemental Material. Poststratification weights were assigned using the R package survey (Version 4.0; Lumley, 2020) The weighting procedure involved simultaneously matching under- and oversampled variables to the population distribution, so that matching one variable’s distribution would not result in unmatching other variables’ distributions. To that end, we used an iterative algorithm (i.e., raking ratio estimation). This iterative algorithm poststratifies factors by turn, leading to a converging set of weights for each factor that matches the population distribution. All three regression models involved the use of this weighted and adjusted sample. This weighted sample was additionally used in descriptive estimations to assess the replicability of the results revealed by the main unadjusted sample.
Sensitivity analyses involving only the randomly obtained participants
Approximately 70% of the participants in the present study were randomly obtained, leaving 30% of the participants in the main analysis nonrandomly reached. Consequently, we selected a random and poststratified proportion (i.e., subsample) of only those participants who were obtained by the random selection technique through the Facebook Business algorithm. This was used in sensitivity analyses to further assess the robustness and the replicability of the main results stemming from the original sample. These sensitivity analyses were additionally conducted following matching of demographic variables proportionate to the adult population of Norway. In sum, the robustness of the original results was assessed twice; sensitivity analyses consisted solely of randomly obtained individuals as well as with a weighted and adjusted sample involving poststratification weights proportionate to the population distribution.
Comparison of concurrent symptom levels with prepandemic samples
Although we did not employ a prospective design and could not directly assess changes in the same subjects, we were able to investigate differences in symptom levels by acquiring data from the same population as the population of the present study (i.e., Norwegian adults) from 2015. This prepandemic sample consists of 1,944 representative and randomly sampled Norwegian adults who had responded to the PHQ-9 before the COVID-19 pandemic (i.e., 2015), including 1,051 females and 893 males (Krogstad et al., 2020). In addition, using the same instruments and cutoff values, we compared the prevalence rates of depression and anxiety in the current pandemic sample with representative prepandemic samples from similar populations as well as more distinct cultures encompassing similar population characteristics.
Results
Sample description
National NPIs aimed at reducing viral transmission were employed in Norway on March 12, 2020. The data collection of this study was conducted between March 31, 2020, and April 7, 2020. Consequently, at the time of measurement, the duration of NPIs experienced by respondents ranged from 19 to 26 days. Overall, a total of 10,061 adults participated in the study. All 10,061 participants (100% of the sample) were included in all descriptive reports and prevalence estimates. A total of 10,035 participants (99.75% of the sample) were included in the regression analyses because two levels of the sex variable (i.e., intersex and transgender) included too few participants to be included as separate categories in the regression analyses (four and 22 participants, respectively). The age of participants ranged from 18 to 86 years, with a mean age of 36 years (SD = 13.46). The percentage of preexisting mental health conditions in this sample was 17.11%, which reflects the lower end of the known rate of psychological disorders in the adult population of Norway, which is between 16.66% and 25.00% (Norwegian Institute of Public Health, 2016). Participants’ demographic information is provided in Table 1. The sample was also geographically representative of Norway, and the ratio of individuals from each region was proportionate to the population parameter. Specifically, 63.02% of the sample (vs. 58.32% in the population) were from eastern Norway, 24.87% of the sample (vs. 20.28% in the population) were from western Norway, 10.50% of the sample (vs. 15.95% in the population) were from mid-Norway, and 3.60% of the sample (vs. 5.45% in the population) were from northern Norway.
Demographic Information of the Participants in the Present Sample (N = 10,061)
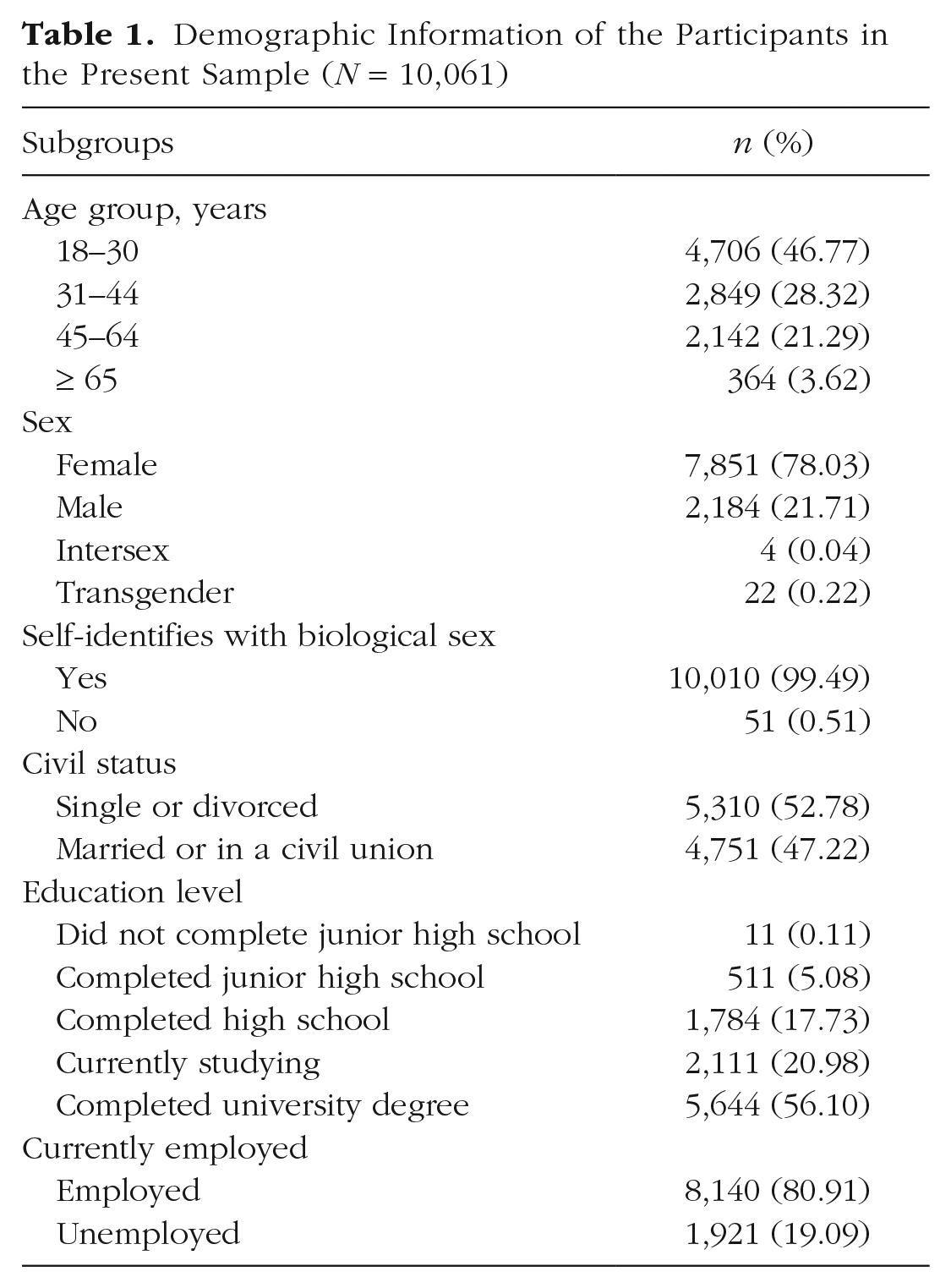
Out of the 10,061 participants, a total of 3,583 (35.61%) reported suspicions of having been infected by COVID-19 during a 2-week period. Of these individuals, 1,090 respondents (30.42%) reported visiting the health care system for this problem specifically. Furthermore, a total of 4,846 (48.17%) of all respondents reported difficulties working from home for more than half of the days during which they experienced NPIs, whereas 4,963 (49.33%) of all participants reported that the NPIs affected their productivity related to their job or schoolwork. More than 59% of the 10,061 participants reported financial concerns. The Norwegian government held press conferences on national television, providing clear and transparent information updates concerning the pandemic situation. These press conferences were well received by the adult population; only 4.97% of the 10,061 participants reported being negatively affected by them.
Prevalence of psychological symptoms in the general population
Descriptive statistics of depressive and anxiety symptoms across different subgroups in the present pandemic sample are provided in Table 2, along with the percentage of participants meeting the validated cutoff points on PHQ-9 (≥ 10) and GAD-7 (≥ 8) for clinically significant depressive and anxiety symptoms. The level of depressive and anxiety symptoms is much higher in the present sample of participants experiencing the NPIs aimed at mitigating viral transmission during the COVID-19 pandemic compared with obtained data from the same population before the pandemic in 2015 in addition to similar samples from other countries during nonpandemic periods. These results are presented in Table 3. Specifically, the prevalence of depression estimated by PHQ-9 (cutoff ≥ 10) in the present pandemic sample is 30.78% (95% CI = [29.88%, 31.70%]). In the obtained data from the same population in 2015 estimated by PHQ-9 (cutoff ≥ 10), the prevalence of depression was 10.24%. Consequently, the prevalence of depression in the present pandemic sample is 3 times higher than estimations from the obtained data of the same population (i.e., Norwegian adults) before the pandemic (30.78% vs. 10.24%) as well as approximately 3 times higher than similar representative samples from other countries in nonpandemic periods (8.20%–14.70%), all using the same instrument and cutoff value (Johansson et al., 2013; Kauffman et al., 2021; Krogstad et al., 2020; Maske et al., 2006). In addition, there was a significant difference (p < .001) in depressive symptoms between participants who predominantly socially distanced themselves and participants who did not. Of adults who predominantly socially distanced themselves, 32.81% met the cutoff for clinically significant depression (PHQ-9 ≥ 10), in contrast with 23.14% among adults who did not predominantly socially distance.
Levels of Psychiatric Symptoms in a General Adult Population (N = 10,061) After 2 Weeks of Nonpharmacological Interventions Aimed at Impeding Viral Transmission Chains During the COVID-19 Pandemic.
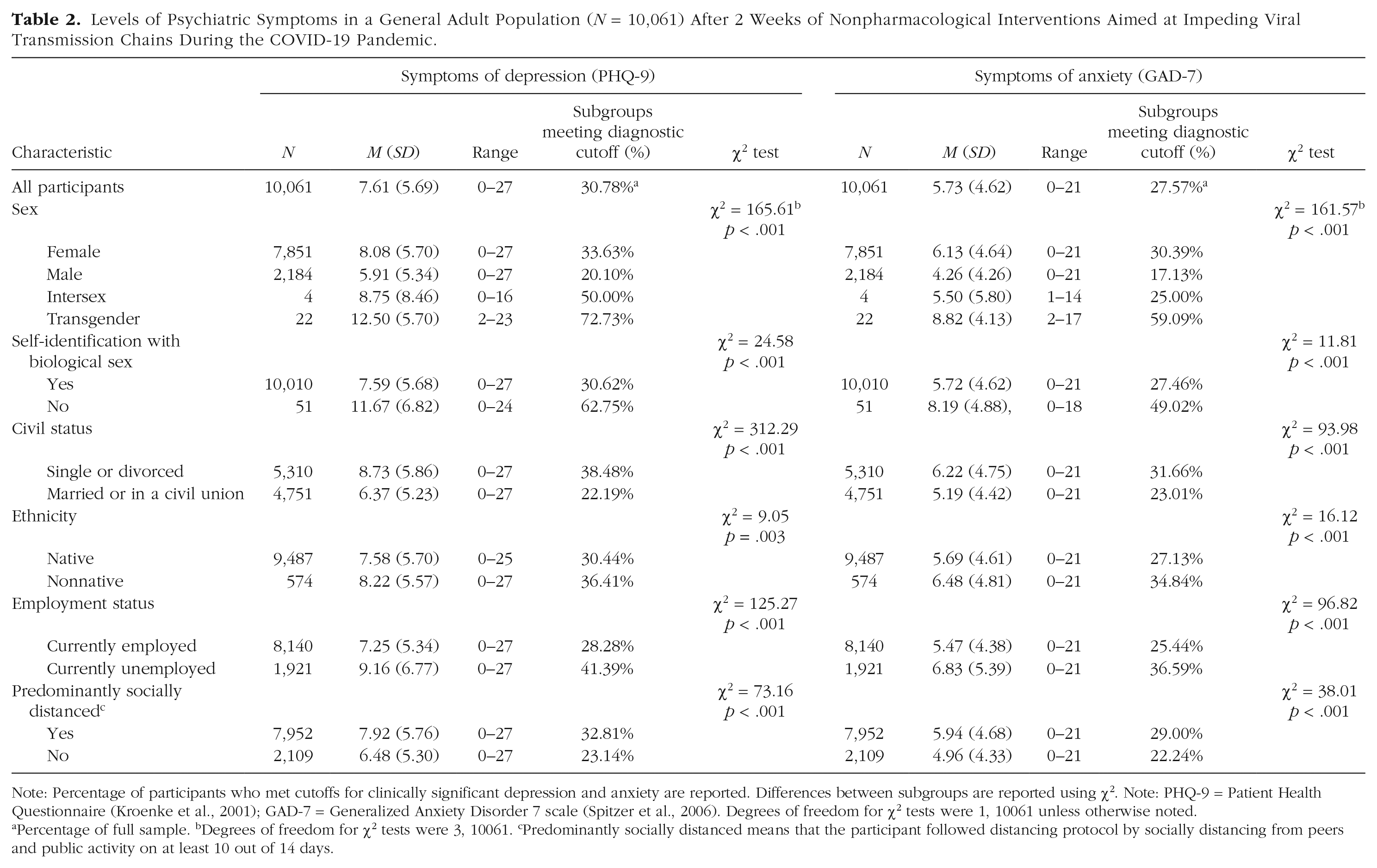
Note: Percentage of participants who met cutoffs for clinically significant depression and anxiety are reported. Differences between subgroups are reported using χ2. Note: PHQ-9 = Patient Health Questionnaire (Kroenke et al., 2001); GAD-7 = Generalized Anxiety Disorder 7 scale (Spitzer et al., 2006). Degrees of freedom for χ2 tests were 1, 10061 unless otherwise noted.
Percentage of full sample. bDegrees of freedom for χ2 tests were 3, 10061. cPredominantly socially distanced means that the participant followed distancing protocol by socially distancing from peers and public activity on at least 10 out of 14 days.
Percentage Meeting Validated Cutoff of Depression and Anxiety in the Current Pandemic Sample, the Same Population Before the Pandemic (Data From 2015), and Similar Representative Populations of Adults
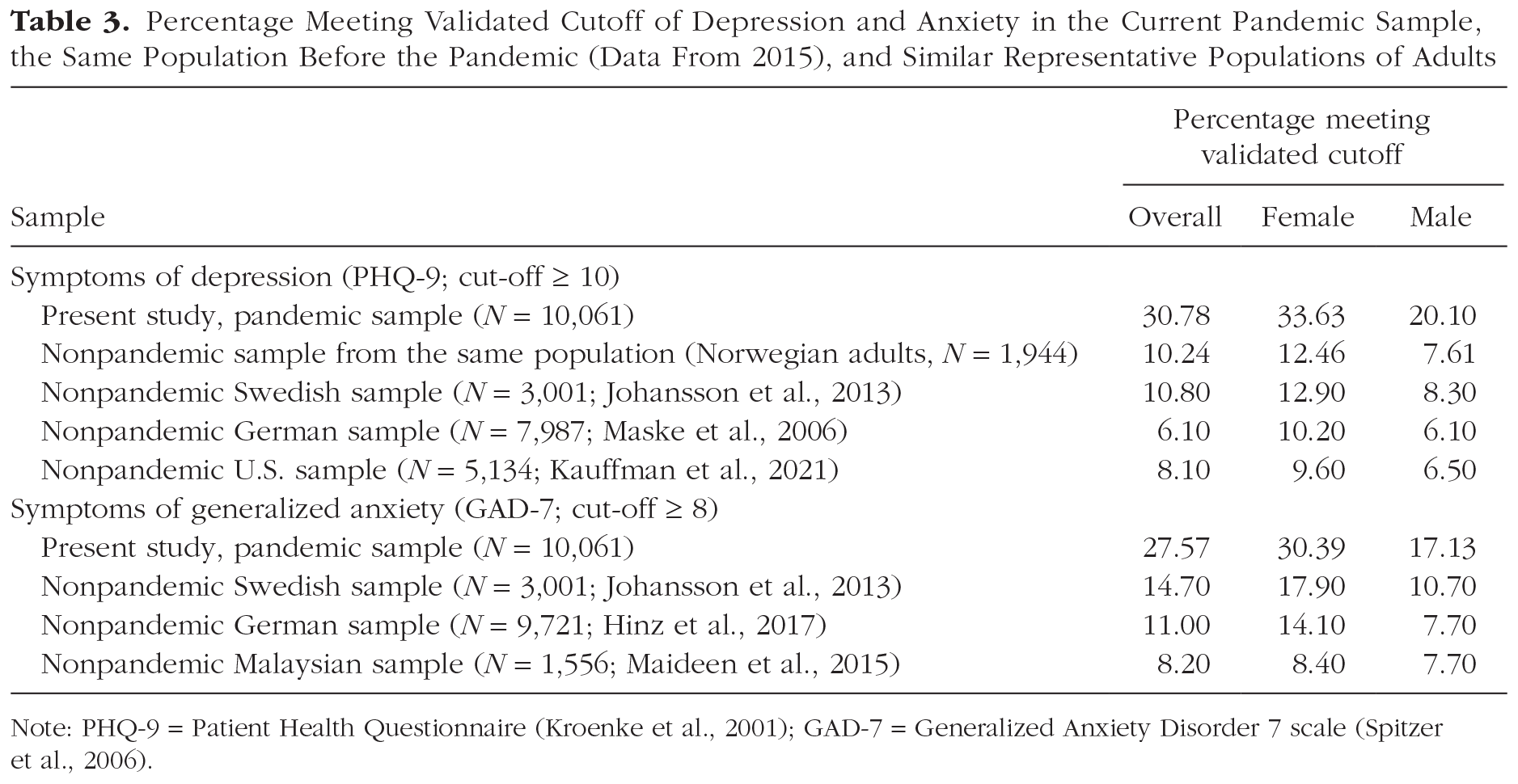
Note: PHQ-9 = Patient Health Questionnaire (Kroenke et al., 2001); GAD-7 = Generalized Anxiety Disorder 7 scale (Spitzer et al., 2006).
The prevalence of clinically significant anxiety estimated with GAD-7 (cutoff ≥ 8) is 27.57% (95% CI = [26.70%, 28.43%]), 2 to 3 times higher than estimations using the same instrument and cutoff from similar samples in nonpandemic periods (Hinz et al., 2017; Johansson et al., 2013; Maideen et al., 2015). In the present pandemic sample and all mentioned nonpandemic samples, a larger proportion of women met the cutoff criteria of both GAD-7 and PHQ-9, revealing more severe symptoms of depression and anxiety. Note that there was a significant difference (p < .001) in anxiety symptoms between participants who predominantly socially distanced themselves and participants who did not. Of participants who predominantly socially distanced themselves following protocols, 29.00% met the cutoff for clinically significant anxiety (GAD-7 ≥ 8), in contrast with 22.24% among participants who did not predominantly follow these protocols.
In the current pandemic sample, single or divorced individuals, individuals who did not identify with their biological sex, nonnatives, and unemployed individuals represented other vulnerable demographic groups, yielding higher levels of depressive and anxiety symptoms (see Table 2).
To further control for the robustness of these results, we repeated the same analyses using the weighted and adjusted sample. The original findings were replicated in this representative sample, revealing an overall prevalence of 29.56% (vs. 30.78%) for depression and a prevalence of 26.26% (vs. 27.57%) for anxiety. In addition, sensitivity analyses were conducted using a random subsample of the randomly obtained portion of participants, further matched in accordance with population parameters. These sensitivity analyses involved a random subsample including 3,098 of the participants. Once again, the results showed identical prevalence estimates for depression (30.89%) and anxiety (26.66%) compared with the original sample (30.78% and 27.57%, respectively), replicating the original findings for the second time and providing further support for the robustness of the presented results.
Factors associated with depressive symptoms
The multiple regression examining the variables associated with depressive symptoms is presented in Table 4. Overall, the regression model accounted for 52% of the variance in depressive symptoms. Female gender associated with more depressive symptoms than male gender. Increased age was associated with less depression. People who were single or divorced as well as people with lower education were associated with more depressive symptoms. Regarding situational variables, being employed was associated with less depression, whereas job loss related to the pandemic was unrelated to depressive symptoms. Frustration of autonomy was associated with greater depression severity. Mandatory social distancing versus voluntary social distancing (p = .009) and extent of access to information (p = .011) were unrelated to depressive symptoms at the prespecified p < .001 level, whereas perceived competence to deal with the crisis was associated with less depression. Worry about prolonged duration of the implemented NPIs predicted more depressive symptoms. Physical activity, distraction with positive activities not performed otherwise during nonpandemic everyday life, and experiencing nature were protective factors against depression; more involvement in these activities was associated with fewer depressive symptoms. Having a preexisting mental health condition was controlled for in the multiple regression model, and this variable was associated with greater depression severity.
Three Multiple Regression Models (N = 10,035) Presenting the Predictors of Depressive Symptoms, Symptoms of Anxiety, and Degree of Adherence to NPIs Employed Against COVID-19
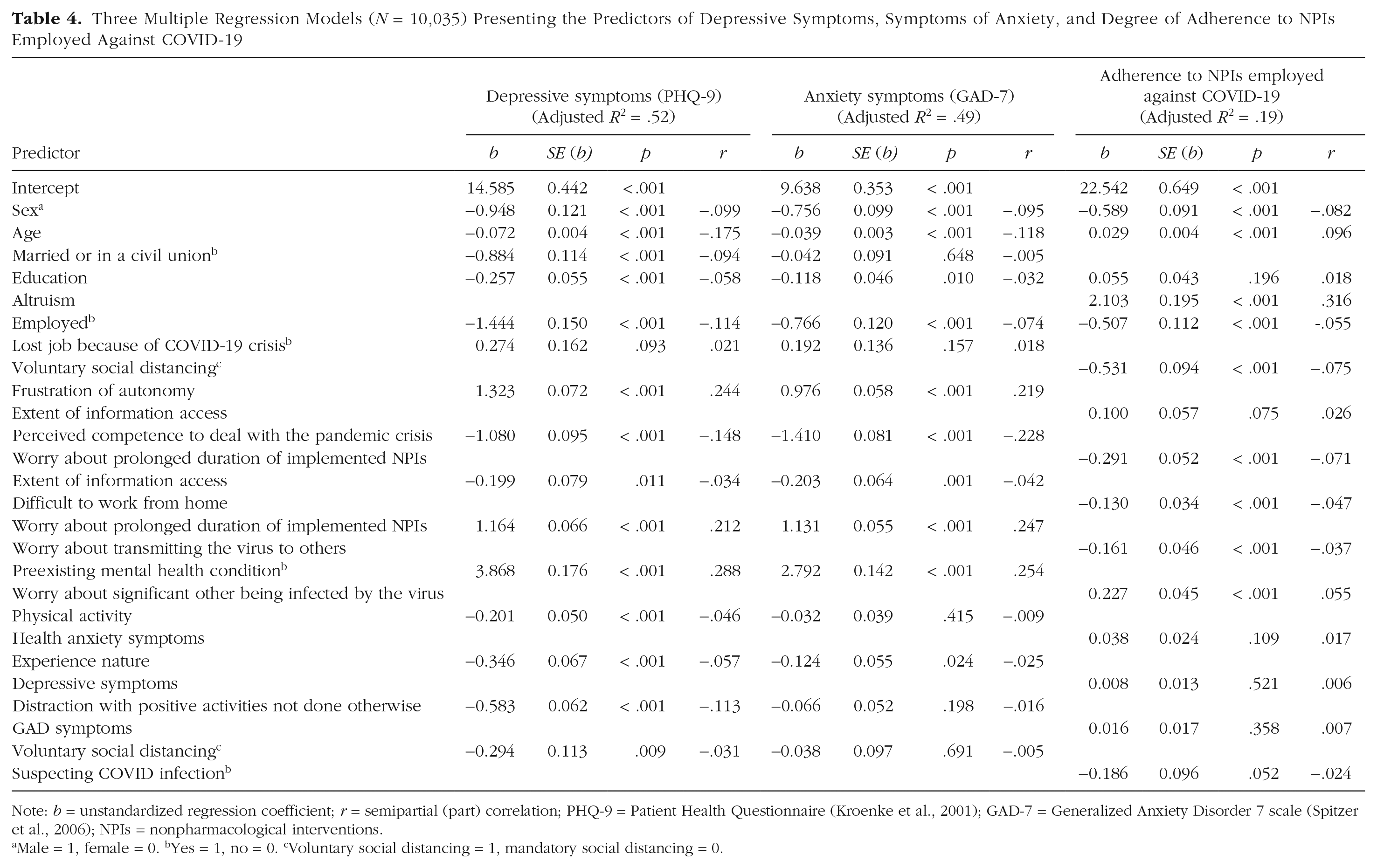
Note: b = unstandardized regression coefficient; r = semipartial (part) correlation; PHQ-9 = Patient Health Questionnaire (Kroenke et al., 2001); GAD-7 = Generalized Anxiety Disorder 7 scale (Spitzer et al., 2006); NPIs = nonpharmacological interventions.
Male = 1, female = 0. bYes = 1, no = 0. cVoluntary social distancing = 1, mandatory social distancing = 0.
Among these associations, part correlations revealed the factors most strongly associated with depressive symptoms while accounting for all other variables. The strongest factors associated with depressive symptoms included worry about prolonged duration of the implemented physical distancing protocols (part correlation = .21), frustration of autonomy (part correlation = .24), preexisting mental health conditions (part correlation = .29), age of the participants (part correlation = −.18), sex (part correlation = .10), being employed (part correlation = −.11), distraction with positive activities not done otherwise (part correlation = −.11), and perceived competence to deal with the crisis (part correlation = −.15), all revealing small to medium effects (see Table 4).
Factors associated with anxiety symptoms
The multiple regression model examining the factors associated with anxiety symptoms are provided in Table 4 and explains 49% of the variance in anxiety symptoms. Females were associated with more severe anxiety. Higher age was associated with fewer anxiety symptoms. Employment was associated with lower anxiety severity. Extent of information access was borderline significant (p = .001) and served as a protective factor associated with less anxiety symptoms. Perceived competence to deal with the crisis was another protective factor associated with less anxiety symptoms. Worry about prolonged duration of the implemented NPIs was associated with more anxiety symptoms. History of mental disorder was controlled for in this model, and people with mental disorders reported more anxiety symptoms.
Among these associations, part correlations revealed the factors most strongly associated with anxiety symptoms while accounting for all other variables. These included perceived competence to deal with the pandemic (part correlation = −.23), worry about prolonged duration of implemented physical distancing protocols (part correlation = .25), age of the participant (part correlation = −.12), sex (part correlation = −.10), preexisting mental health conditions (part correlation = .25), and frustration of autonomy (part correlation = .22), all revealing small to medium effects (see Table 4).
Factors associated with adherence to mitigation strategies
In addition, we fitted a multiple regression model to investigate the factors associated with adherence to the NPIs employed aimed at impeding viral transmission chains. The model explained 19% of the variance (see Table 4). Females revealed higher rates of adherence than males. There was a significant association between increased age and higher adherence rates, whereas education was unrelated to adherence. Increased altruistic attitude was associated with higher adherence, whereas being employed was associated with lower adherence. Voluntary social distancing was associated with less adherence compared with mandatory social distancing. Extent of information access was unrelated to adherence to NPIs. Difficulty working from home was associated with lower adherence. Worry about transmitting the virus to others was associated with lower adherence, whereas worry about significant others being infected by the virus was associated with higher adherence to NPIs. Worry about prolonged duration of the implemented NPIs was associated with lower adherence rates.
Among these significant associations, part correlations revealed the factors most strongly associated with levels of adherence while accounting for all other variables. Adherence was most strongly associated with altruistic attitude (part correlation = .32) and the age of the participants (part correlation = .10); the former yielded a medium effect size, and the latter yielded a small effect.
Discussion
Prevalence of psychological symptoms
Level of current psychopathology was markedly (i.e., 3 times) larger during the period with implemented NPIs compared with an obtained prepandemic sample from the same population in 2015 and similar representative samples in Sweden (Johansson et al., 2013), Germany (Maske et al., 2006), and the United States (Kauffman et al., 2021) during nonpandemic periods. Overall, nearly one third of the present sample met the cutoff for clinically significant depressive symptoms. These findings correspond to a previous study in which levels of depression during an NPI-active period during the SARS pandemic in Canada were examined (Hawryluck et al., 2004) and a recent meta-analysis by Salari et al. (2020), which revealed a prevalence of 33.70% for depression during the present pandemic across 14 studies (N = 44,531). In addition, a recent prospective study by Ettman et al. (2020) followed participants from before to after the pandemic and revealed threefold increases in depressive symptoms. Consequently, the findings reflect the consistent associations between exposure to stressful life events and greater severity of depressive symptoms in the literature (e.g., Hammen et al., 1992; Kendler et al., 1999; McGonagle & Kessler, 1990; Tennant, 2002), revealing the heavy psychological burden that accompanies pandemics. Note that in the present sample, there was a substantial (i.e., 10%) difference in the prevalence of clinically significant depressive symptoms among participants who predominantly socially distanced themselves compared with participants who did not (33% vs. 23%, respectively). Social-distancing protocols were thus associated with higher depressive symptoms. Such differences have been found for anxiety symptoms during the present pandemic, revealing that quarantined individuals reported significantly higher symptoms of anxiety than nonquarantined participants (Zhao et al., 2020). The present results extend to the literature by revealing these associations with regard to depressive symptoms.
For anxiety symptoms, comparisons with similar representative samples from Sweden (Johansson et al., 2013), Germany (Hinz et al., 2017), and Malaysia (Maideen et al., 2015) during nonpandemic periods reveal that the prevalence of anxiety symptoms is 2 to 3 times higher during an NPI-active period in the current pandemic. These results are comparable with a study that found that more than one third of participants experienced high levels of psychological distress during a period of equine influenza outbreak in Australia (Taylor et al., 2008) and coincide with a recently published meta-analysis by Salari et al. (2020) that revealed a prevalence rate of 31.90% for anxiety during the present pandemic across 17 studies (N = 63,439). Moreover, in the present sample, there was a substantial (i.e., 7%) difference in the prevalence of clinically significant anxiety symptoms among participants who predominantly socially distanced themselves compared with participants who did not (29% vs. 22%, respectively). Social-distancing protocols were thus associated with higher anxiety symptoms, consistent with a recent study revealing that quarantined individuals reported significantly higher symptoms of anxiety than nonquarantined participants (Zhao et al., 2020).
In sum, prevalence of clinically significant depression and anxiety symptoms measured during the NPI-active period was 2 to 3 times larger than estimates of these symptoms in the same population from 2015 and other comparable populations during nonpandemic periods without NPIs. These symptom increases were further comparable with prevalence estimates from previous pandemics and a meta-analysis assessing the same symptoms during the present pandemic. Moreover, in the present sample, social-distancing protocols were associated with significantly higher proportions of depressive and anxiety symptoms. Our results suggest that female respondents, individuals belonging to sexual-orientation minorities, nonnatives, single individuals, individuals with preexisting mental health conditions, and unemployed individuals are associated with higher risk of meeting the cutoff for clinically significant depression and anxiety symptoms, suggesting that these groups may be more susceptible to requiring interventive measures in the present pandemic as well as preventive measures in forthcoming pandemics employing similar NPIs. Taken together, the presented results suggest that the present pandemic and its implemented mitigation protocols are associated with detrimental mental health symptoms. Although the strict NPIs employed in Norway successfully managed to reduce R0 from 2.4 to 0.7 during the survey period, these findings suggest that such intensive lockdown strategies and social-distancing interventions, which are presently ubiquitous across all continents, are likely to include detrimental psychological costs. Although some respondents will experience immediate relief of symptoms once NPIs are lifted, other individuals may continue to experience these symptoms for long durations even after NPIs are discontinued. Indeed, several studies from previous pandemics have suggested long-term effects of NPIs on mental health and behavior (Brooks et al., 2020). Consequently, the markedly larger prevalence rates of clinically significant depressive and anxiety symptoms may have adverse implications for respondents’ future mental health states, a cause for concern that will be crucial to monitor over the forthcoming period.
Factors associated with depression and anxiety
Several factors associated with depression were also associated with anxiety, which is not surprising given their correlation in this sample (r = .76, p < .001). However, important differences emerged among both risk factors and predictors of depression and anxiety, requiring attention from clinicians and health policymakers. Females, younger adults, and individuals with a preexisting psychiatric disorder had greater symptom severity for both depression and anxiety. In terms of relationship status, being married or in a civil union was a significant protective factor of depressive symptoms but not anxiety. Furthermore, lower education levels were associated with more depressive symptoms but unrelated to anxiety. Job loss related specifically to the COVID pandemic was unrelated to depression and anxiety severity, although being employed (vs. unemployed) in general served as a protective factor against these symptoms. This finding is consistent with the economic stress hypothesis, in which unemployment has been related to increased symptoms of psychological disorders (Catalano & Dooley, 1983).
Furthermore, given that employment has been robustly associated with reduced symptoms of depression and anxiety (Lund et al., 2018), this finding encourages government officials to find solutions that make use of individuals’ skills to keep them employed. These findings further particularly highlight the vulnerability of single individuals with regard to depressive symptoms during pandemic periods; twice as many (in contrast with participants in relationships) and nearly 40% of single individuals experienced clinically significant depressive symptoms. This seemingly reflects the importance of social contact, which has been reduced to a greater extent for single individuals by the strictly employed social-distancing protocols. Appropriate action to incorporate mitigation strategies that may alleviate these symptoms while simultaneously maintaining viral transmission control is warranted. A utile intervention toward both these causes may include the use of social support bubbles, allowing single individuals to have a few contact points during strict lockdown and curfew periods. In addition, other important differences between depression and anxiety included that higher engagement in coping behaviors such as physical activity, distraction with positive activities not done otherwise, and experiencing nature were protective factors associated with reduced burden of depression but not anxiety. To further advance the literature on coping strategies that are effective during pandemic periods, forthcoming studies should investigate other coping behaviors that could reduce the burden of anxiety.
Frustration of autonomy and worry about prolonged duration of the implemented social-distancing measures (i.e., NPIs) were associated with greater severity, whereas perceived competence to deal with the pandemic crisis was an associated protective factor for both anxiety and depressive symptoms. Worry about prolonged duration of implemented NPIs had an equally large effect on anxiety symptoms as a preexisting psychiatric disorder, suggesting the strength and importance of this variable in its association with anxiety symptoms. The extent of access to information was unrelated to depression but significantly associated with anxiety symptoms. It would thus seem that for depression, it is more the content of information rather than its frequency that is associated with symptoms. Thus, competence-enhancing public health messages combined with provision of predicable estimates concerning the duration of implemented pandemic measures may be a utile strategy with regard to combating depressive symptoms, a strategy of possible utility to health policymakers. For anxiety, both worry about prolonged duration of implemented NPIs as well as extent of access to information are of importance. This finding is meaningful given empirical findings that have revealed that anxiety is mainly driven by worry and an intolerance of uncertainty (e.g., Grupe & Nitschke, 2013; Rosser, 2019), both of which seem to be alleviated through availability of information and predictable information concerning the length of NPIs. Although the causal directions of this relationship are not certain, there is a possibility that providing credible and accurate information concerning the pandemic situation may be beneficial in reducing symptoms of anxiety, a finding that should be investigated in forthcoming studies. This is in line with the uncertainty and anticipation model of anxiety (Grupe & Nitschke, 2013) in which uncertainty of possible future events may result in anxiety. Consequently, preparing the population for plausible upcoming scenarios in an open and transparent manner may have the potential to reduce such uncertainty and in turn protect against detrimental mental health outcomes.
Moreover, diverting efforts toward supporting individual autonomy and perceived competence may be beneficial given that it is associated with reduced symptoms of both depression and anxiety, which could possibly be achieved by providing individuals with information fostering a sense of self-efficacy in their own ability to cope with the present crisis. It may be possible that the shock accompanied by the early pandemic phase resulted in a state of perceived helplessness, which has been previously associated with depressive symptoms arising from environmental factors (e.g., Miller et al., 1977). The initial shock arising from the pandemic also may have led to increased worry about the future, which has previously been associated with increased anxiety symptoms (e.g., Wells, 2009). Investigations of such potential underlying mechanisms of increases in depressive and anxiety symptoms should be a priority for forthcoming studies because they can provide important insights concerning treatment targets.
Factors associated with adherence to mitigation strategies
Adherence levels were generally high in Norway; most individuals reported having followed the NPIs for more than half of the days to nearly every day. These findings are consistent with Google Mobility reports during the measurement period (see the Supplemental Material). The Google Mobility report portrays a sharp decrease in social and physical activities, with large decreases in overall national mobility in Norway, further reflecting that individuals adhered to the NPIs requiring physical and social distancing. Female gender and older age were associated with higher adherence. This finding suggests that males and younger individuals may take pandemic risks less seriously, revealing that alternative strategies are necessary to increase the adherence of these subgroups of individuals. Indeed, previous studies have indicated that older adults tend to see more risk in matters of health compared with younger adults (i.e., Bonem et al., 2015). One possible strategy to increase adherence in these groups may include the adaptation of risk perception in public health messaging, given that previous findings (e.g., Brewer et al., 2004) on Lyme disease indicated that individuals with greater awareness of its associated risks were more likely to engage in adaptive adherence behavior.
Current employment was associated with lower adherence levels, which could be explained by the fact that many of the NPIs concern socially distancing oneself and staying at home, guidelines that certain groups of employed individuals may have to violate for work-related purposes. People instructed to socially distance themselves (i.e., mandatory or rule-enforced social distancing) had higher adherence levels compared with people who voluntarily socially distanced themselves. This finding may be explained by the fact that people who were instructed to engage in mandatory social distancing were either carriers of the infection (being instructed to isolate) or had been in contact with infected others (being instructed to enter quarantine). Consequently, it may seem that these individuals were more likely to adhere to NPIs involving social distancing because they were either infected and/or had increased risk of infecting others, possibly taking the NPIs more seriously. Extent of access to information was unrelated to adherence, suggesting that it is the content rather than the frequency of information that is relevant to adherence. Given the current overload of available information about the pandemic (i.e., an overload termed an infodemic by the WHO), these findings have important implications suggesting that public health officials may more reliably focus on the clarity and content of messaging rather than increasing its frequency when informing the public about pandemic mitigation protocols.
Worry about significant others being infected by the coronavirus was associated with higher adherence to NPIs. However, we found that worry of transmitting the virus to others was associated with lower adherence to NPIs. Because the presented data are correlational, it may seem more plausible to consider the other direction in interpreting the latter association, in which it may be that individuals who at first did not adhere to NPIs subsequently experienced worry about transmitting the virus to others rather than the other way around. Finally, worry about prolonged duration of implemented NPIs was associated with lower adherence. Taken together with the other findings of this study, the latter association seems to reflect an emotional burden of adhering to NPIs, as is evident from the severely high prevalence rates of depression and anxiety in this sample. However, the direction of this association is uncertain because it may be that individuals first worry about extended duration of NPIs after having violated them, instead of this worry itself being primary and subsequently leading to lower adherence. Such directional associations are important to investigate in forthcoming studies involving multiple time points, which have the potential of moving closer to causal understandings given temporal precedence in data structures. In any case, it appears that strategies aiming to reduce worry about prolonged durations of implemented mitigation strategies, such as the provision of information concerning how long they will be implemented, is associated with decreases in anxiety and depressive symptoms and increases in adherence to NPIs.
Note that increased altruistic attitude was a potent factor associated with higher adherence, revealing a medium to large effect size. This finding adds to the literature by providing support for a previously uninvestigated hypothesis by Brooks and colleagues (2020) suggesting that appealing to altruism during pandemic periods may foster favorable effects. Previous studies (e.g., Tajfel & Turner, 1979) have highlighted possible ways through which altruism may effectively be increased, including the formation of a collective identity via establishing shared interests that may further be enhanced through public health messaging campaigns involving framing such as “our united battle against the virus.” In addition, researchers (e.g., Bendapudi et al., 1996; Gouldner, 1960) have found that presenting helping behaviors as norms may enhance altruistic attitude. This is revealed to happen through the mechanism of reinforcement (i.e., peers in society reinforce newly established norms) and through the presentation of cues for how to behave in novel situations (e.g., Bendapudi et al., 1996; Gouldner, 1960). Consequently, public health officials may find it useful to provide clear guidelines on specific behavioral etiquettes and norms in pandemic situations, provide suggestions on how to best conduct these behaviors, stress the importance of helping behavior, and provide a collective cause and establish common interests to motivate individuals to adhere to mitigation protocols.
Magnitude of investigated associations
We now point to the magnitude of the associations between the examined predictors (i.e., Table 4) and depression, anxiety, and adherence. Because these regression analyses involve high-dimensional and multifactorial models (i.e., involving numerous and diverse sets of variables) with all variables controlling for the influence of one another, the relative effect size per predictor is naturally lower in contrast to unidimensional models and models examining few predictors. Thus, models including more relevant variables naturally reveal smaller effect sizes for each included variable given that each added relevant factor competes for the same pool of variance. Consequently, in interpreting the effect sizes, we point to the unstandardized regression coefficients and the relative part correlations between variables, which provide more accurate representations of the magnitude of associations. For instance, the association between worry about prolonged duration of NPIs (part correlation = .25) is equal in size to that of having a psychiatric diagnosis (part correlation = .25). Such comparisons are also available for depression (i.e., frustration of autonomy, worry about prolonged duration of NPIs), revealing the substantial associations between these factors and the criterion variables (see Table 4).
Strengths and limitations
A major strength of the present study is the existence of prepandemic data for the same population in comparison with the large pandemic sample. Another substantial strength of this study involves the multifactorial investigations of factors related to depression, anxiety, and adherence. Moreover, the main results were replicated across the main sample and two cross-validations, including an adjusted and representative weighted sample, and the entirely randomly selected and adjusted subsample of participants in the sensitivity analyses, attesting to the robustness of the findings. Furthermore, this study has momentarily captured the effects of NPIs as they happen and while they are identical and held constant across the measurement period. It involves an investigation of commonly used NPIs, providing the grounds for the evaluation and modification of such strategies when similar approaches are taken in the present and forthcoming pandemics. Self-selection bias was further accounted for in multiple ways, including through a subsample sensitivity analyses involving the randomly selected participants with matched characteristics to the population parameter in addition to following assignment of poststratification weights on the entire sample that matched the demographic groups to the exact distributions known in the population. In both analyses, the original findings of the present study were further replicated.
A limitation of the present study includes its cross-sectional design, which impairs the ability to draw conclusions concerning directional and causal effects. This highlights the importance of future research to investigate such directional effects in studies involving multiple time points. Clever experimental designs that may imply causal effects are warranted. Another limitation concerns the self-reporting of symptoms and the presence of a psychiatric diagnosis rather than the use of diagnostic interviews. Moreover, one of the predictors in the regression concerning anxiety (i.e., worry about prolonged duration of NPIs) slightly overlaps with the process of worry and its uncontrollability in this measure. Although the predictor represents a pandemic-specific worry and is distinct from this general process of worrying and its uncontrollability, this minor overlap should be noted as a limitation. As with traditional sampling techniques involving voluntary participation, potential self-selection of participants may be present. However, analyses were conducted to reduce the influence of such effects; these analyses replicated the main findings and thus suggesting lowered likelihood of such effects.
Future directions
Research on the mental health impacts of the current global crisis is in its infancy, and there is an urgent need for more studies on the topic. Among other areas, future studies should investigate the general mental health and posttraumatic symptoms of vulnerable groups, such as health care workers, individuals in critical positions susceptible to burnout (e.g., politicians and teachers), parents, children in vulnerable homes, individuals with special needs, public service providers at increased risk of contracting the virus, individuals with preexisting mental and physical health conditions, and minority subgroups. Investigating adherence as well as mental health symptoms in immigrants may also be important because language barriers have the potential effect of causing anxiety symptoms in addition to problems with adherence. Examining the impact of information sources on adherence and psychiatric symptoms would further greatly benefit the literature. An investigation of posttraumatic symptoms, parental stress, and other mental health symptoms in both parents and children in unfavorable home situations is warranted, which may be amplified by closure of schools and quarantine measures. Investigations of other symptoms of psychopathology are warranted, including insomnia and disturbances to circadian rhythms that have been amplified because of the large changes in daily routines around the world. Studies involving complex systems approaches such as network methodology are warranted and have the potential to reveal specific symptom relations during pandemic periods and to investigate the mechanisms underlying emergent detrimental mental health states. It would be of great utility to the pandemic research literature if there were studies comparing the network structure of psychopathological symptoms in prepandemic sample compared with pandemic samples, which may reveal structural differences and mechanisms especially relevant during pandemic periods. Finally, studies investigating time trends and psychological symptoms across multiple time points during different phases of the pandemic will be imperative, allowing for the monitoring of subgroups requiring interventive measures, revealing more resilient groups requiring less attention, and further assessing the possible long-term effects of pandemic protocols.
Concluding remarks
The present study reveals a twofold to threefold increase in depressive and anxiety symptoms in the adult population compared with prepandemic samples. Although these symptoms increased for all individuals, there was a large difference between individuals who were predominantly exposed to pandemic mitigation protocols and individuals who were not, suggesting unfavorable associations between these strict physical-distancing measures and mental health symptoms. Several risk factors, pandemic-specific situational factors, and psychological factors associated with mental health symptoms were investigated in addition to factors associated with adherence to pandemic protocols. Cumulatively, the presented results have implications for approaches that may be favorable in the efforts of increasing adherence to pandemic mitigation protocols while simultaneously protecting the population from the detrimental mental health correlates of these implemented strategies. Appropriate action must be taken by government officials, researchers, and clinicians to minimize mental health risks accompanying pandemics and its burdensome mitigation protocols and to monitor the development of these symptoms during the course of the pandemic and after its termination.
Supplemental Material
sj-pdf-1-cpx-10.1177_2167702621994545 – Supplemental material for Physical Distancing and Mental Health During the COVID-19 Pandemic: Factors Associated With Psychological Symptoms and Adherence to Pandemic Mitigation Strategies
Supplemental material, sj-pdf-1-cpx-10.1177_2167702621994545 for Physical Distancing and Mental Health During the COVID-19 Pandemic: Factors Associated With Psychological Symptoms and Adherence to Pandemic Mitigation Strategies by Omid V. Ebrahimi, Asle Hoffart and Sverre Urnes Johnson in Clinical Psychological Science
Footnotes
Acknowledgements
The present research would not be possible without the immense efforts of multiple individuals and organizations behind its logistics. We owe our gratitude to the Regional Committee for Medical and Health Research Ethics and the Norwegian Centre for Research Data for processing and approving the study protocol and analysis plan in a swift manner. We further thank Marianne Jensen Hjermstad, who provided us with access to prepandemic data on the Norwegian adult population. We are grateful for these efforts, which were imperative in making this time-sensitive project possible.
Transparency
Action Editor: Kenneth J. Sher
Editor: Kenneth J. Sher
Author Contributions
The project was designed by all of the authors, and the study concept of the manuscript was developed by O. V. Ebrahimi under the supervision of A. Hoffart and S. U. Johnson. All of the authors contributed to the data collection process. Writing of the manuscript, data analysis, and interpretation of the findings was performed by O. V. Ebrahimi under the supervision of S. U. Johnson and A. Hoffart. The manuscript and its subsequent revisions were drafted by O. V. Ebrahimi with input from S. U. Johnson and A. Hoffart. All of the authors contributed to and approved the final manuscript for submission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.