
Abstract
The current two-wave longitudinal study aimed to investigate changes in stress, anxiety, depression, and positive mental health (PMH) during the first COVID-19 pandemic outbreak in the sample of emerging adults. Data were collected before the COVID-19 and within the first month of the outbreak. The study sample consisted of 775 university students from Lithuania (n = 450, Mage(SDage) = 19.45 (0.93), 79.3% female) and Germany (n = 325, Mage(SDage) = 23.08 (2.94), 78.2% female). The results of multivariate Latent Change Analysis revealed that Lithuanian and German emerging adults demonstrated a decrease in stress and anxiety at the COVID-19 outbreak. Lithuanians also showed a decrease in depressive symptoms and an increase in PMH. Three groups with different change patterns were identified: resilient (82%) demonstrating positive changes, high-symptom (8%) with stable high rates of stress and depression and stable low rates of PMH, and vulnerable (10%) with an increase in depressive symptoms as well as a decrease in PMH over time.
The outbreak of COVID-19 affected the lives of millions of people worldwide. Many countries introduced measures of everyday life restrictions in the first months of 2020 to mitigate the spread of coronavirus amid the global pandemic outbreak (Flaxman et al., 2020; Hsiang et al., 2020). In the face of the pandemic-related crisis, World Health Organization alerted that the level of experienced stress was rising rapidly and expressed concerns regarding its possible impact on mental health (World Health Organization, 2020). Based on findings from previous epidemics (e.g., Hall et al., 2008; Perrin et al., 2009), as well as initial studies of the COVID-19 pandemic, it has been demonstrated that the COVID-19 may have a significant negative impact on mental health across various countries (e.g., Cullen et al., 2020; Kumar & Nayar, 2020; Rajkumar, 2020; Torales et al., 2020).
Initial findings of cross-sectional population studies emphasized that many people reported moderate to high subjective negative impact of the COVID-19 on their mental health. Moreover, a significant proportion reported high levels of stress, anxiety, and depression symptoms (Wang, Pan, Wan, Tan, Xu, Ho, & Ho, 2020). However, at least one longitudinal population study conducted over the course of the COVID-19 pandemic failed to identify significant changes in stress, anxiety, and depression over time, indicating that positive changes in mental health symptoms are also possible (Wang, Pan, Wan, Tan, Xu, McIntyre, et al., 2020). This may indicate that in face of the COVID-19 pandemic, people may also demonstrate resilience, as conceptualized through the ability to bounce back to adversity and adapt positively in face of challenges and difficulties (Luthar & Cicchetti, 2000). Nevertheless, experiences from previous crises (e.g., Bacigalupe et al., 2016) show that there may be a short-term decline in clinical anxiety, depression, and suicide rates immediately after a disaster, and a significant increase in psychological problems can be expected in the medium and long term. These effects are observed in different segments of the population at varying degrees, as they may depend on the levels of negative socioeconomic consequences. Moreover, an increase in psychological problems may be mediated by the psychological processing of the stress experiences, that is, higher levels of personally experienced distress may result in worse mental health over time (Zivin et al., 2011).
It is known that emerging adults, due to high levels of stress, face an increased risk for developing mental disorders (Arnett et al., 2014). Research evidence suggests that life stressors during student years may diminish mental well-being and may contribute to the enhanced risk of the development of mental disorders, such as depression, anxiety, and adjustment disorder (Schönfeld et al., 2016; Truskauskaite-Kuneviciene, et al., 2020). Moreover, emerging adults may be among those who have been the most affected by the COVOD-19-related restrictions and lockdown measures, as they tend to be more sociable and more outgoing, compared to older adults (Brook & Schmidt, 2020). Nevertheless, it has been found that during the early months of the COVID-19 pandemic, higher resilience was associated with going outside more often, more exercising, and higher perceived social support (Killgore et al., 2020), indicating that being more active may work as an important protective factor for youth to demonstrate resilience in face of the pandemic.
In the previous COVID-19 related studies, concerns were raised that the mental health issues in youth could rise and should be studied and monitored during the COVID-19 pandemic (Cao et al., 2020; Li et al., 2020; Liang et al., 2020). Additionally, a high proportion of emerging adults from various countries reported high levels of stress and anxiety during the outbreak of COVID-19 (Browning et al., 2021, Kaparounaki et al., 2020; Liu et al., 2020; Odriozola-González et al., 2020). A longitudinal study of youth with the pre-test 2 years prior to the outbreak of pandemic reported an increase in perceived stress, but not depressive and anxiety symptoms (Shanahan et al., 2020). When the study with the pre-test 7 months before the pandemic reported a decrease in stress, anxiety, and depressive symptoms among university students during the first months of the COVID-19 outbreak (Elmer et al., 2020).
As the COVID-19 crisis is a new global issue, it is highly challenging to robustly measure its impact on mental health. The currently available findings on the effects of the pandemic on mental health are mostly based on cross-sectional data or data collected during the pandemic outbreak without previous or non-recent baseline measures. To better understand the effects of the pandemic, there is a high need for more high-quality data and international collaboration to have a global perspective on this issue, as well as to address the impact of the pandemic on different populations (Holmes et al., 2020). Longitudinal research is needed to address the question of whether the mental health of youth changes during the outbreak of pandemics (Wade et al., 2020).
To address the lack of longitudinal research utilizing pre-test data collected close to the onset of the COVID-19 and to address the lack of studies on the impact of the COVID-19 on mental health in European countries, the aims of the current study were as follows. First, we sought to investigate the change in mental health indicators, in particular, stress, anxiety, depression as well as positive mental health after the onset of the COVID-19 outbreak in a sample of emerging adults. Second, we aimed to estimate whether the patterns of change in mental health indicators are comparable across two European countries, in particular, Lithuania and Germany. From the cultural perspective, more similarities than differences may be observed between Lithuania and Germany (e.g., Balcytiene, 2012). Similar levels of mental health problems were observed in both countries during the school years (Kovess et al., 2015). Similar behavioral and mental health patterns were reported by university students across two countries (Brailovskaia et al., 2021). Similar measures of the lockdown and moving study process online were taken in the initial months of pandemic. Nevertheless, mental health care is way more developed in Germany (Margraf et al., 2021), compared to Lithuania (Kazlauskas & Grigutyte, 2020), that is, mental health support for university students may be more accessible in Germany than in Lithuania. Also, by the time of the first outbreak of the pandemic, relatively fewer COVID-19 cases were observed in Lithuania, compared to Germany (https://covid19.who.int/). Therefore, some differences in mental health response toward the pandemic could be anticipated among the two countries. Finally, we sought to identify emerging adults with possibly different patterns of change in mental health indicators when facing the COVID-19 pandemic, as previous studies indicated that mental health response to the crisis may vary in association to, for example, the levels of personal distress (e.g., Zivin et al., 2011).
Method
Participants
The final study sample consisted of 775 emerging adults studying at universities (78.8% female; Mage (SDage) = 20.97 (2.71), age range: 18–29) in the two European countries, Germany (n = 325) and Lithuania (n = 450). Participants’ characteristics in each country separately are presented in Table 1. The data from two waves (T1 and T2) were used in the current study, by including only the participants currently studying at university, who are within the age range of emerging adulthood (18–29), and who filled relevant measures both times.
Sample Characteristics (N = 775).
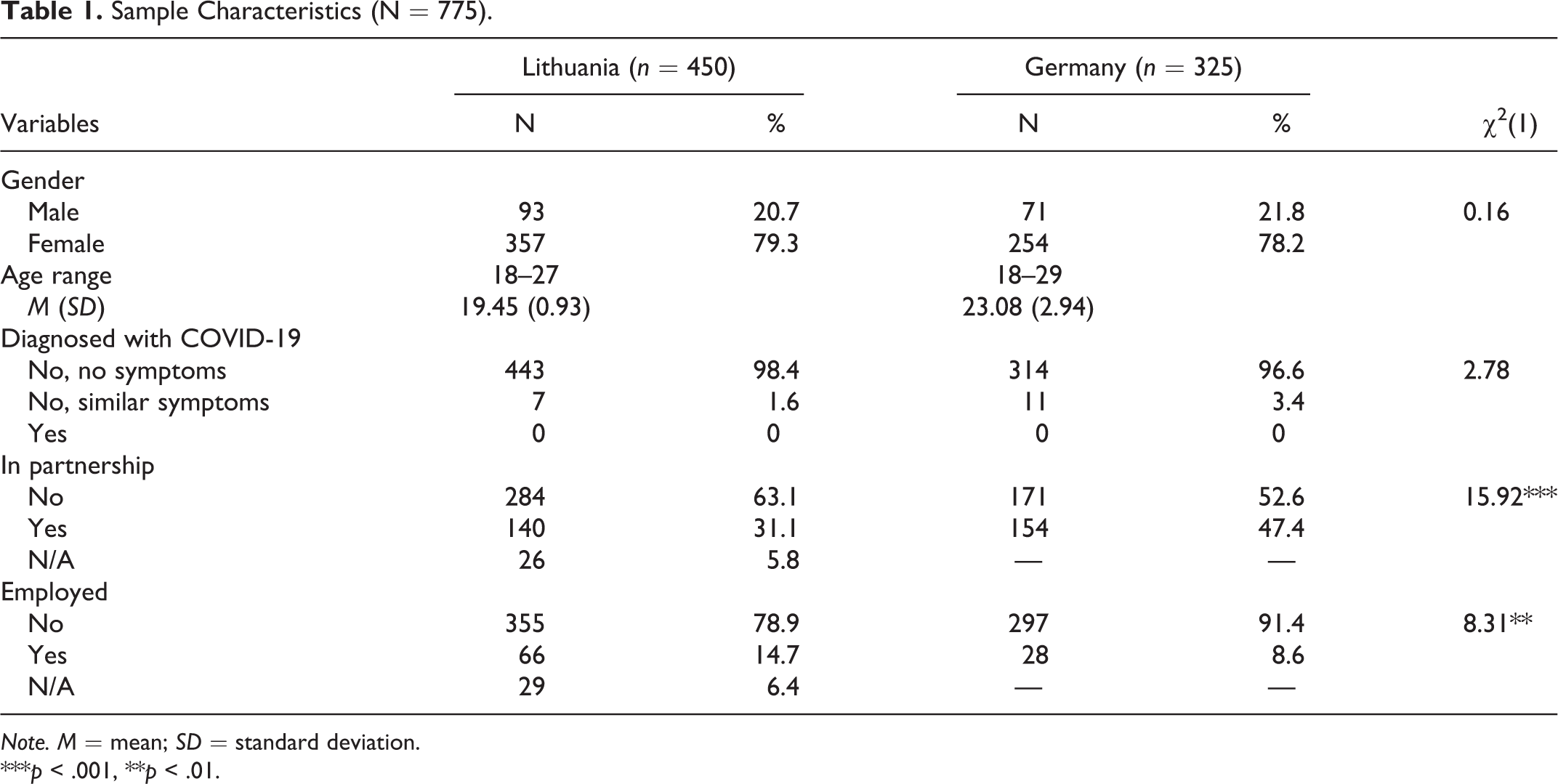
Note. M = mean; SD = standard deviation.
***p < .001, **p < .01.
In Lithuania and Germany, 27.5% and 41.3% of study participants, respectively, who filled the relevant measures at T1, were reached at T2. Possible attrition bias (Miller & Hollist, 2007) was tested to identify whether the characteristics of retained participants were comparable to drop-out participants who were not reached at T2. MANOVA analysis revealed that in the Lithuanian sample there was a statistically significant but small difference of baseline mental health indicators between retained and drop-out participants (F(4) = 4.51, p = .001, Wilks’ Λ = .989, partial η2 = .011). Retained participants had higher levels of stress (η2 = .003) and anxiety (η2 = .007) as well as lower levels of positive mental health (η2 = .004) in comparison to the drop-out group at T1. We found no significant drop-out effects in the German sample.
Procedures
Ethical approvals from the relevant Institutional Review Boards (IRB) in Germany and Lithuania were obtained prior to data collection. Additionally, ethical approval amendments to include the COVID-19 specific items in the study were granted by the IRB’s in both countries. The T1 data were collected in October–December 2019; the T2 data were collected in March–April 2020, within the first month after implementing national social distancing measures due to the COVID-19 in both countries. Some data from the German sample were published previously (Brailovskaia & Margraf, 2020) by including stress, anxiety, depression, and positive mental health at T1 as predictors of burden related to COVID-19.
In both countries, data were collected online on a secure survey platform. Participants were recruited via e-mail or face-to-face invitations with a link to an online survey using the national language by sending invitations to individuals who were studying at a large university in the Ruhr region (Germany) or Vilnius (Lithuania). All participants were properly instructed and provided informed consent online to participate in a longitudinal study. No financial incentives were provided for participation. For the German sample only, participation in the study was compensated by course credits.
Measures
Depression, anxiety, and stress symptoms
The 21-item Depression Anxiety Stress Scales (DASS-21; Lovibond & Lovibond, 1995) was used to measure mental health issues. The DASS-21 consists of three subscales, comprising of seven items each and measuring symptoms of depression (e.g., “I couldn’t seem to experience any positive feeling at all”), anxiety (e.g., “I was worried about situations in which I might panic and make a fool of myself”) and stress (e.g., “I found it difficult to relax”). Participants indicated frequency on each of the symptom items over the past week on a 4-point Likert scale ranging from 0 (= “never”) to 3 (= “always”). The DASS-21 score for each of the three symptoms ranges from 0 to 21, with a higher score indicating a higher level of symptoms. The Cronbach’s alpha coefficients for the Stress, Anxiety, and Depression Scales in a full study sample at T1/T2 were .88/.88, .83/.81, and .90/.89, respectively. In the Lithuanian sample, the Cronbach’s alpha coefficients for the Stress, Anxiety, and Depression Scales at T1/T2 were .87/.89, .82/.83, and .90/.89; in the German sample, .87/.87, .79/.73, and .88/.88, respectively.
Positive mental health
The Positive Mental Health Scale (PMH-Scale; Lukat et al., 2016) is a unidimensional scale that consists of nine items, measuring emotional, psychological, and social aspects of positive mental health (e.g., “I am in good physical and emotional condition”). Each item was rated on a 4-point Likert scale ranging from 0 (= “do not agree”) to 3 (= “agree”). The total PMH-Scale score ranges from 0 to 27, with a higher score indicating a higher level of positive mental health. The Cronbach’s alpha coefficient in a full study sample at T1/T2 indicated a high internal consistency (Cronbach’s α = .91/.92) of the scale. In the Lithuanian sample, the Cronbach’s α coefficients of PMH-Scale at T1/T2 were .90/.92; in the German sample, .92/.92.
Resilience
The Resilience Scale 11 (RS-11; Schumacher et al., 2005) was used to measure psychological resilience. The RS-11 is a unidimensional measure containing 11 items (e.g., “I usually manage one way or another”). Each item was rated on a 7-point Likert scale ranging from 1 (= “do not agree”) to 3 (= “agree”). The total RS-11 score ranges from 11 to 77, with a higher score indicating a higher level of resilience. In the current study, resilience was measured at the COVID-19 outbreak (T2) only. The Cronbach’s α coefficient in a full study sample indicated a high internal consistency (Cronbach’s α = .85) of the scale. In the Lithuanian and German samples, the Cronbach’s alpha coefficients of RS-11 were .84 and .87 respectively.
In the current study sample, the metric longitudinal measurement invariance of both the DASS-21 scale and the PMH-Scale were established, including country invariance. The metric country invariance was also established for the RS-11 scale. The changes in model fit indices are provided in the Supplementary Table S1.
Data Analyses
To examine the changes in mental health indicators at T2, we used the multivariate latent change modeling approach that provides more robust estimates of change over time (Duncan et al., 2013). In latent change models with two measurement points, the intercept represents the mean level of the measure at T1 and the slope represents the change from T1 to T2.
Measurement invariance
As a preliminary step, we tested longitudinal measurement invariance for each measure used in the study. First, we compared the configural model (Confirmatory Factor Analysis (CFA), allowing the correlations between errors of the same items across the two-time points) with the metric model, in which the factor loadings were constrained to be equal across time, and the scalar model, in which item intercepts were also constrained to be equal across time. Model comparisons were conducted by examining the changes in fit indices (e.g., Chen, 2007). In all invariance models, we allowed the residual correlations of the same items across the time-points. We then extracted the factor scores (Yang & Hoyle, 2010) from scalar models of the DASS-21 and the PMH scales that were subsequently used for the multivariate latent change model estimation.
Latent change analysis
In the current study, we conducted the latent change model of four parallel processes, specifically, change in stress, anxiety, depression, and positive mental health (PMH), controlling for possible gender effects on intercepts and slopes. To have the latent change model identified, first, we fixed the residuals to zero; second, we fixed non-significant gender effects to zero one by one until we obtained the final model with the significant links only. In addition, to identify whether the change processes in mental health indicators were linked with each other and whether the initial levels of stress, anxiety, depression, and PMH were associated with the changes, in the final model, we correlated all intercepts and slopes.
Multi-group analysis
After running the multivariate latent change model in the full study sample, we conducted multiple group analysis by including the country of residence as the moderator. To determine possible differences between groups, we assessed differences between the models with fixed versus free parameters of slopes, indicating the same versus different levels of change in mental health indicators across countries. To determine significant differences between the models with fixed versus free parameters, at least two of these three criteria had to be matched: Δχ2 significant at p < .05 (Satorra & Bentler, 2001), ΔCFI ≥ .01, and ΔRMSEA ≥ .015 (Chen, 2007). To test for the differences in mental health indicators at T1 as well as to compare the change parameters across countries, we ran the Wald χ2 tests.
Latent class change analysis
To identify groups of participants with possibly different patterns of change in mental health indicators, we used the latent class change approach (Jung & Wickrama, 2008). We classified the study participants based on the change in all four mental health indicators and used several criteria to decide on the number of latent classes. First, the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) statistics for a solution with k classes should be lower than for a solution with k–1 classes. Second, a statistically significant p-value of the adjusted Lo, Mendell, and Rubin test, which compares improvement in fit between neighboring class solutions after the inclusion of an additional class. Third, Entropy score, with relatively higher values equal to or above .70 indicative of more accurate classification. After the data-driven classification of the study participants regarding their mental health indicators, we have validated the groups by comparing the levels of resilience in the resulting subsamples. To do that, we compared the latent means of resilience among the groups by constraining the mean in the reference group to 0 and freeing the mean in the comparison groups. When comparing the latent means, a significant mean in a comparison group indicates a significant difference among groups.
The model fit in all analyses was evaluated by using the Comparative Fit Index (CFI), the Tucker–Lewis Index (TLI), the Root Mean Square Error of Approximation (RMSEA), and the Standardized Root Mean Square Residual (SRMR), following the goodness of fit recommendation provided by Kline (2006). Namely, CFI/TLI values higher than .90 indicated an acceptable fit and values higher than .95 represented a very good fit; RMSEA and SRMR values below .08 indicated of an acceptable fit and values less than .05 suggested a good fit. The analyses were conducted with Mplus 8.2 (Muthén & Muthén, 1998–2017).
Results
Means and standard deviations of the study variables at T1 and T2 are presented in Table 2. The results of preliminary analyses indicated higher levels of Stress, Anxiety, and Depression as well as lower levels of Positive Mental Health and Resilience in Lithuania, compared to Germany, both at the Baseline and the COVID-19 outbreak. Correlations among study variables are reported in Supplementary Table S2. The results of correlation analysis yielded that in Lithuania and Germany, Stress, Anxiety, and Depression were positively linked with one another as well as negatively linked with Positive Mental Health both at the same time-points and across two measurement points.
Descriptive Statistics of Mental Health Indicators in Lithuania and Germany.
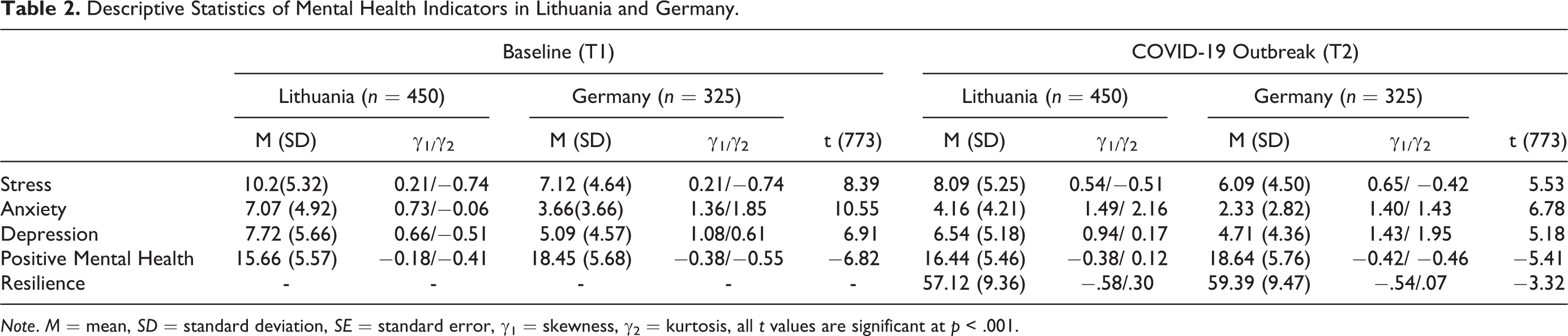
Note. M = mean, SD = standard deviation, SE = standard error, γ1 = skewness, γ2 = kurtosis, all t values are significant at p < .001.
Change in Mental Health Indicators
The multivariate latent change analysis in a full study sample yielded an excellent model fit (χ2 (17) = 5.59, p = .348, CFI/TLI = 1.000/.999, RMSEA [90% CI] = .012 [.000, .053], SRMR = .015). Overall, we found significant (p < .001) small decrease in rates of stress (Mslope = −.26; d = −.42 [−.52; −.32]), moderate decrease in anxiety (Mslope = −.36; d = −.65 [−.98; −.33]), small decrease in depression (Mslope = −.12; d = −.20 [−.30; −.10]) as well as small increase in positive mental health (PMH) (Mslope = .07; d = .12 [.02; .22]) at T2. For all mental health indicators, we found significant negative links (p < .001) between intercepts and slopes, indicating that higher baseline rates of stress (r = −.52), anxiety (r = −.67), and depression (r = −.53) are associated with higher/stronger decrease in these negative mental health indicators; lower baseline rates of PMH (r = −.37) are associated with higher increase in this positive indicator of mental health. We also found significant gender effects on intercepts of stress (βintercept = −.05, p = .001) as well as intercept and slope of anxiety (βintercept = −.06, p < .001; βslope = .02, p = .022), indicating higher stress and anxiety female baseline rates, compared to male and higher anxiety decrease in male, compared to female.
The Country as a Moderator of Change in Mental Health
The results of multi-group analysis and the comparison between the latent change models with free versus fixed slope parameters across countries indicated that there were significant differences in change of mental health indicators in Lithuania and Germany (Δχ2(8) = 106.05, p < 0.001, ΔCFI = .013, ΔRMSEA = .072). Therefore, further in the current section, we will present the results of latent change model with all free parameters across countries (χ2 (10) = 16.29, p = .09, CFI/TLI = .999/.994, RMSEA [90% CI] = .040 [.000, .074], SRMR = .030). The trajectories of change in mental health indicators in Lithuania and Germany separately with the effect sizes are presented in Figure 1. The results of multiple group analysis indicated that the Lithuanian participants reported significantly higher initial levels of stress (χ2(1) = 33.47, p < .001), anxiety (χ2(1) = 61.68, p < .001), and depression (χ2(1) = 63.48, p < .001), as well as lower levels of positive mental health (PMH) (χ2(1) = 40.66, p < .001) compared to the German participants. However, the Lithuanian sample demonstrated significant (p < .001) moderate decrease in stress and anxiety, small decrease in depression (Mslope (stress/anxiety/depression) = −.34/−.44/−.17) as well as significant (p < .001) small increase in PMH (Mslope = .10). The German sample showed significant (p < .001) small decrease in stress (Mslope = −.15) and moderate decrease in anxiety (Mslope = −.25), while depression and PMH remained stable over time. Moreover, the decrease in stress (χ2(1) = 20.63, p < .001) and anxiety (χ2(1) = 18.86, p < .001) in the Lithuanian sample was significantly higher compared to the German sample. The correlations between intercepts and slopes of the same variables in both subsamples were found to be negative, indicating the higher decrease in negative mental health indicators for higher initial levels of stress, anxiety, and depression as well as a higher increase in PMH for the lower initial level of this indicator (Table 3). In the German sample only, we found a significant gender effect on change in anxiety (βslope = .04, p = .046), indicating a higher decrease in anxiety for male participants compared to female participants. In the Lithuanian sample, female participants demonstrated higher levels of stress (βintercept = −.06, p = .004) and anxiety (βintercept = −.08, p < .001) at T1.
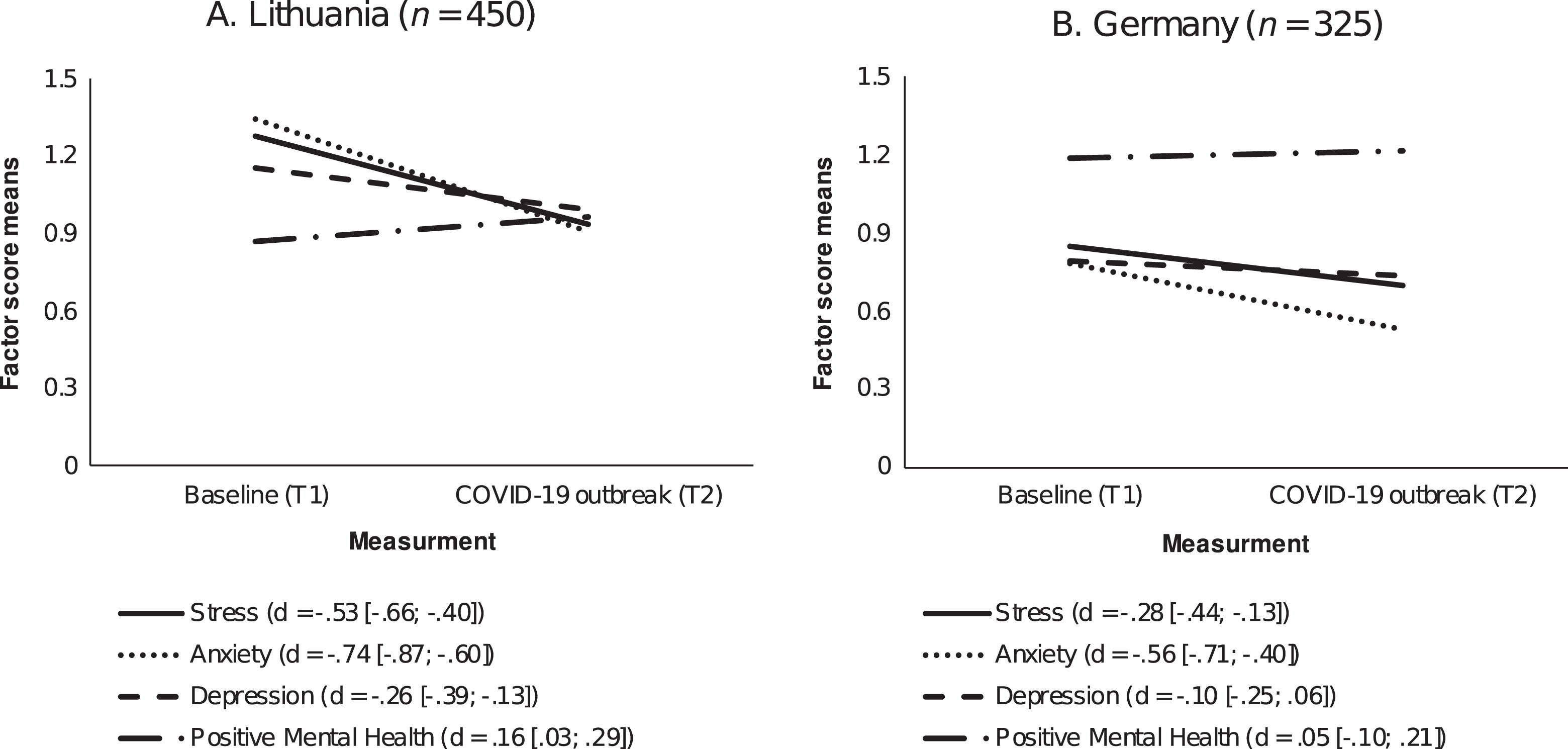
The trajectories of change in mental health indicators in (A) Lithuania and (B) Germany (N = 775). Note. d = effect size with 95% confidence intervals. Negative score indicates decrease, positive score indicates increase.
Pearson r Correlations of Intercepts and Slopes of Study Variables in Lithuania (n = 450)/Germany (n = 325).
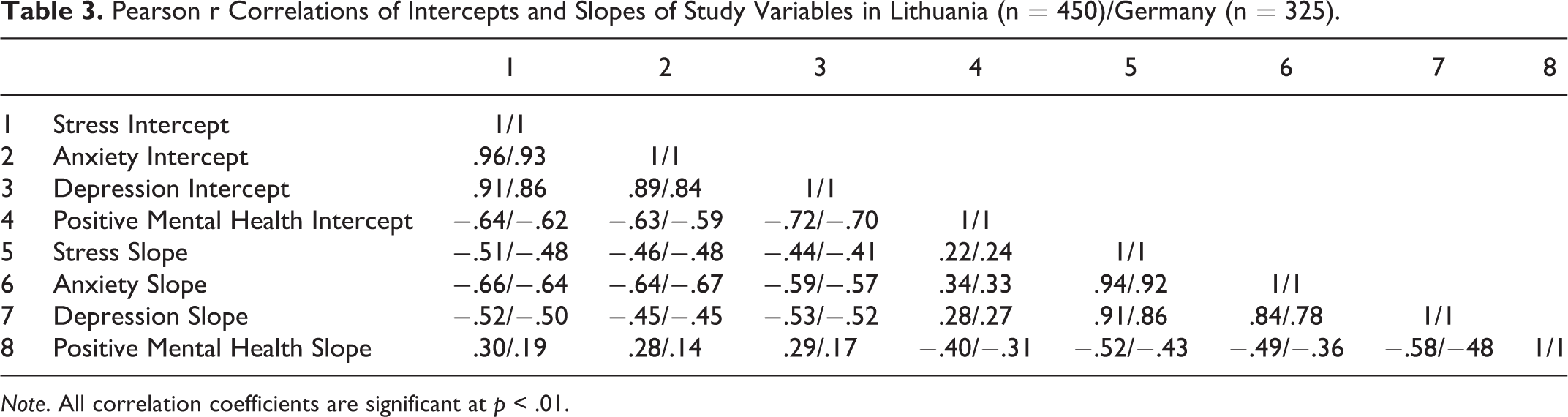
Note. All correlation coefficients are significant at p < .01.
Patterns of Change in Mental Health
The latent class change analysis in the full study sample indicated that the three classes solution fitted the data best, based on the non-significant LMR-A p-value of the four classes solution (for details see Supplementary Table S3). Three identified change profiles were found to be distinguishable in terms of differences in changes of factor means of mental health indicators (see Figure 2). The vast majority of study participants (82%) were classified into the group that, compared to other groups, reported the relatively lowest levels of negative mental health and the highest levels of PMH at the baseline. This group demonstrated a significant (p < .001) moderate decrease in stress (Mslope = −.32), and anxiety (Mslope = −.38), small decrease in depression (Mslope = −.19), as well as significant (p < .001) small increase in PMH (Mslope = .11) over time; this class was labeled as resilient. The second class (8%) reported the relatively highest levels of negative mental health and intermediate levels of PMH. Participants who were classified into this group demonstrated a moderate decrease in anxiety over time (Mslope = −.26, p = .002) with no changes in other mental health indicators; this class was labeled as high symptom. The third class (10%) reported relatively intermediate levels of stress, anxiety, and depression with the lowest levels of PMH. In this group, we observed a moderate decrease in anxiety (Mslope = −.34, p < .001), but also a moderate increase in depression (Mslope = .34, p = .002) as well as a small decrease in PMH (Mslope = −.25, p = .007); we labeled this group as vulnerable (see Figure 2 for the trajectories of change in three groups as well as the effect sizes). The resulting groups were also distinguishable in terms of the levels of resilience. Specifically, the resilient group reported higher levels of resilience, in comparison to high symptom (latent mean = −0.70, p < .001) and vulnerable (latent mean = −1.25, p < .001) groups; high symptom group reported higher levels of resilience when compared to vulnerable group (latent mean = −0.55, p < .001).
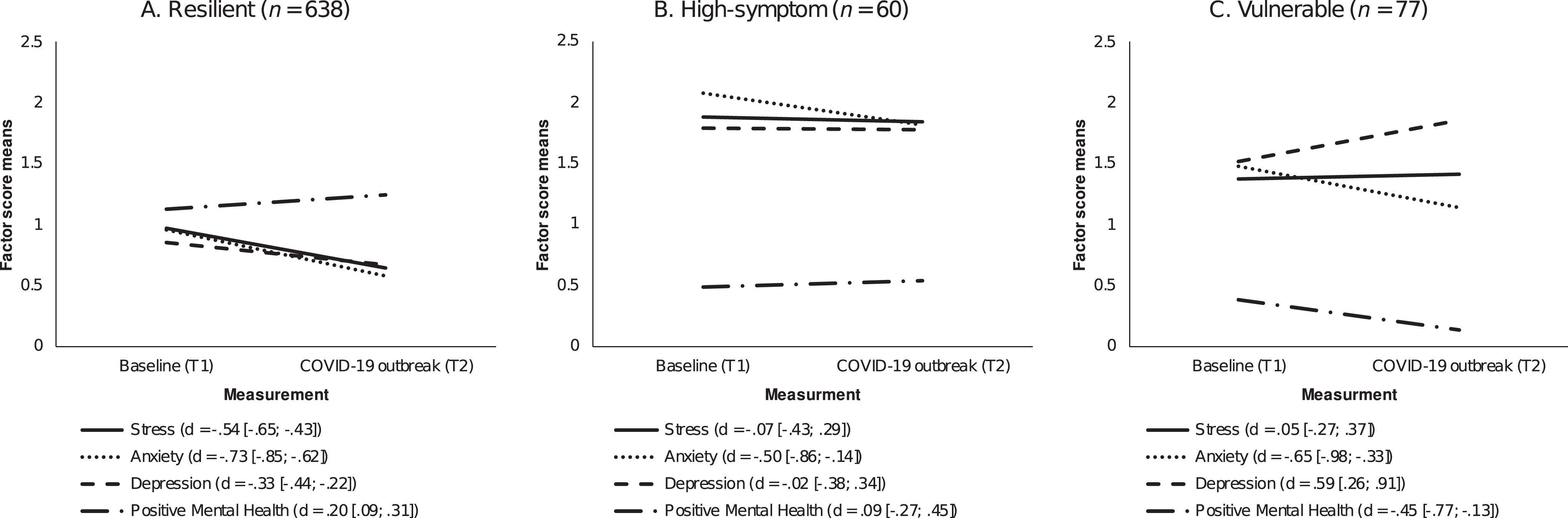
The trajectories of change in mental health indicators in (A) Resilient, (B) High-symptom, and (C) Vulnerable latent change classes (N = 775). Note. d = effect size with 95% confidence intervals. Negative score indicates decrease, positive score indicates increase.
Discussion
The aim of the current longitudinal study was to investigate the initial effects of the COVID-19 crisis on mental health among emerging adults in the two European countries, Lithuania and Germany. Overall, we observed positive initial changes in the mental health of emerging adults in the face of the COVID-19 crisis and these results are in line with recent findings of the initial effects of the previous crisis on mental health (Bacigalupe et al., 2016; Forbes & Krueger, 2019). In particular, we found that the levels of stress and anxiety decreased in both countries. Moreover, there was a decrease in depression, as well as an increase in PMH in Lithuania only. However, we also identified three distinct groups with different change patterns of mental health indicators. The vast majority of youth, who reported relatively good mental health before the COVID-19 outbreak, demonstrated a positive change in all mental health indicators. However, we found that there may be a risk group who reported relatively poorer mental health before the COVID-19 and who may be more vulnerable, as indicated by an increase in their depressive symptoms as well as lower PMH over time. Also, the third group was identified to be possibly in need of clinical-level support. This group demonstrated stable high levels of stress and depression and stable low levels of PMH. Interestingly, anxiety decreased in all three groups over a period of 6 months.
Although the positive changes we observed in youth in the face of COVID-19 may seem surprising at the first glance, some recent findings provided evidence that initially, mental health may not change or might even improve (Wang, Pan, Wan, Tan, Xu, McIntyre, et al., 2020) in response to the COVID-19 pandemic. Emerging adults, in general, are not among the high-risk group of the complicated course of the COVID-19 disease, and fatality rates after contracting the virus among children and youth are relatively low (Jordan et al., 2020). Therefore, emerging adults may not experience life threats in the COVID-19 pandemic, resulting in an unlikely negative change in mental health. Moreover, it is possible that at the beginning of the lockdown, emerging adults, who are usually exposed to relatively high levels of life stressors (Schönfeld et al., 2018; Truskauskaite-Kuneviciene et al., 2020), may experience reduced demands of academic and social responsibilities in response to the social distancing measures resulting in lower levels of stress. Moreover, the resilient response to COVID-19 is positively associated with spending time outside, more exercise as well as higher social support (Killgore et al., 2020; Süss & Ehlert, 2020), which is characteristic of youth in different cultural contexts (Lin et al., 2018). These characteristics may contribute to emerging adults’ overall resilience in response to the COVID-19 pandemic. Additionally, the current findings contribute to the theoretical conceptualization provided by Bonanno (2005), suggesting that resilience is a quite prevalent response to adversity. Nevertheless, the observed positive effects on mental health might be temporary, as the data was collected in the first month of lockdown, and further studies are needed to investigate the longer-term effects of the pandemic on mental health in youth (Wade et al., 2020).
Although we found positive changes in mental health indicators both in Germany and Lithuania, more positive effects were observed in the Lithuanian context. This difference could at least partially be attributed to the relatively better mental health in German youth, compared to Lithuanian, as we also found that bigger positive changes were linked to worse initial mental health condition prior to the pandemic. Moreover, as shown by the population-comparative COVID-19 statistics (https://covid19.who.int/), relatively more COVID-19 cases, as well as more deaths, were reported in Germany compared to Lithuania. Factors that are associated with a more resilient response during emerging adulthood in times of crisis, such as higher sociability (Germani et al., 2020) should be addressed in future research.
The current study is one of the first prospective longitudinal studies in Europe on the effects of the COVID-19 on mental health. The present findings should be considered with caution, as they rely on self-reported online-collected data. Also, the attrition rates from T1 to T2 were relatively high. Moreover, the changes in mental health observed in the current study may be attributable to other, for example, developmental factors. However, despite these limitations, the current study provided valuable evidence on the resilience of youth during the COVID-19 crisis in two European contexts. In addition, our findings indicated that among youth there may be vulnerable individuals who might need support and access to mental health services in the outbreak of pandemics.
Supplemental Material
Supplemental Material, sj-pdf-1-eax-10.1177_21676968211031120 - Evidence on Resilient Initial Response to COVID-19 Pandemic Among Youth: Findings From the Prospective Study of Mental Health in Two European Countries
Supplemental Material, sj-pdf-1-eax-10.1177_21676968211031120 for Evidence on Resilient Initial Response to COVID-19 Pandemic Among Youth: Findings From the Prospective Study of Mental Health in Two European Countries by Inga Truskauskaite-Kuneviciene, Julia Brailovskaia, Jürgen Margraf and Evaldas Kazlauskas in Emerging Adulthood
Supplemental Material
Supplemental Material, sj-pdf-2-eax-10.1177_21676968211031120 - Evidence on Resilient Initial Response to COVID-19 Pandemic Among Youth: Findings From the Prospective Study of Mental Health in Two European Countries
Supplemental Material, sj-pdf-2-eax-10.1177_21676968211031120 for Evidence on Resilient Initial Response to COVID-19 Pandemic Among Youth: Findings From the Prospective Study of Mental Health in Two European Countries by Inga Truskauskaite-Kuneviciene, Julia Brailovskaia, Jürgen Margraf and Evaldas Kazlauskas in Emerging Adulthood
Footnotes
Author Note
I.T.K. ORCID ID: 0000-0001-6699-6638
J.B. ORCID ID: 0000-0001-7607-1305
J.M. ORCID ID: 0000-0001-5207-7016
E.K. ORCID ID: 0000-0002-6654-6220
Author Contributions
All authors developed the study concept and contributed to the study design. Testing and data collection were performed by I.T.K. and J.B. I.T.K. performed the data analysis and interpretation under the supervision of E.K. and J.M. I.T.K. drafted the paper, E.K., J.B. and J.M. provided critical revisions. All authors approved the final version of the paper for submission.
Data Availability
The data that support the findings of this study are available from the corresponding author, [I.T.K.], upon reasonable request.
Ethical Statement
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees and with the Helsinki Declaration of 1975, as revised in 2008.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Lithuanian Research Council (grant number S-COV-20-12).
Open Practices
The raw data, analysis code, and materials used in this study are not openly available but are available upon request to the corresponding author. No aspects of the study were pre-registered.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.