
Abstract
Race-based traumatic stress (RBTS) refers to the emotional and/or physiological responses associated with a racist or racially discriminatory occurrence experienced as traumatic, injurious, and/or emotionally painful. Race-based traumatic stress is predictive of adverse mental health outcomes such as anxiety, depression, and psychological distress, however, less is known about how Black emerging adults encounter and manage RBTS. We conducted 30 in-depth, individual interviews with a community sample of Black emerging adults living in St. Louis, Missouri. Reflexive thematic analysis guided the analysis of the interview data. Three broad themes emerged from the participants’ lived experiences: (1) experiences of everyday racism (2) hypervigilance as an adaptive coping response, and (3) the mental and physical symptoms of RBTS. Study findings illustrate how the mundane and unpredictable experiences Black emerging adults encounter operate on an individual and structural level to lead to manifestations of race-based traumatic stress and adverse mental and physical health outcomes.
Introduction
Emerging adulthood (18–29 years of age) represents a distinct developmental period comprised of gains in independence, identity exploration, periods of instability, and transitional milestones in education, employment, and relationships (Arnett, 2000; Hope et al., 2015; Syed & Mitchell, 2013). While Black emerging adults experience the same developmental markers as their White peers, they do so while encountering both day-to-day and institutional forms of racism. As Black emerging adults enter higher education or the workforce, for example, they often encounter racially hostile environments where racial stereotyping and workplace discrimination are commonplace (Arnett et al., 2014; Hope et al., 2015; Lee et al., 2020).
Navigating racism while transitioning to adulthood, has been linked to harmful health outcomes such as anxiety, depressive symptoms, and racism-related stress – all of which can have a damaging impact that reverberates into later life (Hurd et al., 2014; Lee, Hope, et al., 2020).
A growing body of work has identified race-based traumatic stress (RBTS) as a key mechanism influencing the relationship between experiences of racism and poor health outcomes (Dieujuste et al., 2023; Pieterse et al., 2024; Roberson & Carter, 2021). Race-based traumatic stress is a severe trauma-based stress response to occurrences of racism and racial discrimination that are sudden, unexpected, and emotionally distressing (Carter, 2007). Conceptualizations of race-based traumatic stress recognizes encounters of racism and racial discrimination as potentially traumatic and stressful events linked to a cluster of adverse psychological and physical symptoms (Carter, 2007; Carter et al., 2020; Dieujuste et al., 2023; Pieterse et al., 2024). Interdisciplinary research examining how RBTS impacts emerging adults primarily focuses on college attending emerging adults and their racialized experiences on campus (Rosenbaum, 2001; Syed & Mitchell, 2013). This work leaves significant gaps in our understanding of how RBTS affects Black emerging adults outside of academic settings and within the broader population (e.g., at work and in public spaces). Moreover, most of this work has relied on quantitative approaches—capturing how RBTS affects the development and severity of adverse mental health outcomes. We know comparatively less (based on qualitative research) on how the underlying mechanisms associated with various manifestations of RBTS shape lived experience in community settings. Using qualitative methods, this study seeks to explore how RBTS manifests in the lives of a community sample of Black emerging adults and outline why it is imperative to gain a better understanding of how RBTS operates as a threat to the health and well-being of Black emerging adults.
Emerging Adulthood, Racism, and Race-based Traumatic Stress
Emerging adulthood represents the developmental period between adolescence and adulthood (Arnett, 2000; Arnett & Brody, 2008). Emerging adulthood consists of five distinct pillars: the age of instability, the age of possibilities, the age of self-focus, the age of feeling in-between, and the age of identity exploration. Each pillar is introduced as an “age” to denote the importance of the developmental concerns that take primacy during the distinct phase (Arnett, 2000). Race is a significant social construct that has the power to stratify an individual’s life from crib to coffin (Jones et al., 2020). Racism, a product of racial stratification, represents a ubiquitous reality for Black Americans, regardless of their stage of life (Harrell, 2000; Lewis et al., 2015). Exposure to racism, experienced directly or vicariously, poses an irrefutable hazard to the health, well-being, and livelihood of Black emerging adults (Lee, Anderson, et al., 2020).
Racism is a permanent psycho-social stressor in the lives of Black Americans (Williams, 2018). Experiences of stress occur when an individual encounters an unwarranted event perceived as negative and burdensome that severely taxes or exceeds their ability to cope or adapt (Lazarus & Folkman, 1984). Race-based traumatic stress (RBTS), as theorized by Robert T. Carter (2007) provides insight into the injurious and traumatogenic nature of racism and racial discrimination, regardless of the form experienced. Utilizing Carlson’s (1997) and Carlson and Dalenberg’s (2000) theory of traumatic stress as a theoretical foundation, Carter’s conceptualization of RBTS aids in elucidating the pathways through which experiences of racism lead to the manifestations of unique trauma responses. Race-based traumatic stress is defined as the recurring psychological and emotional stress reactions evoked by a racist and/or racially discriminatory experience (Carter, 2007). According to the race-based traumatic stress model, racist incidents, events, or encounters are understood as forms of emotional and psychological injury, and the stress associated with these injuries may become traumatic (Carter, 2007). As Carter (2007) further articulates, for race-based traumatic stress to be present, one must view the racist event(s) as “negative (emotionally painful), sudden, and uncontrollable (pg. 90)”. Episodes of RBTS also manifests when an individual perceives a racist or racially discriminatory encounter as a threat to their integrity or safety. Experiences such as, but not limited to, police brutality, racial profiling, or being called a racial epithet may evoke manifestations of RBTS. Experiences of RBTS have been empirically linked to anxiety, psychological distress, dissociation, and low self-esteem (Pieterse et al., 2023). The psychological and emotional injury caused by such an episode can also lead to the manifestation of intrusive and repeated recall of the experience.
While scholars and clinicians who work with racially minoritized populations have long linked racism to trauma through the lens of Post-Traumatic Stress Disorder (PTSD), they also argue that race-based traumatic stress constitutes a distinct, nonpathological phenomenon that captures forms of sociocultural and identity-based injury not encompassed by PTSD (Bryant-Davis & Ocampa, 2005; Butts, 2002; Williams, 2018). First, unlike PTSD—which is a diagnosable mental disorder that typically requires psychiatric treatment—Carter (2007) conceptualizes the racist encounters and experiences that give rise to RBTS as an “external violation,” a “psychological injury” and a “situational factor outside of the control” of those who suffer the harm (pg. 16). Other scholars, such as Thema Bryant-Davis (2007) characterize race-related traumatic stress as a “normal response to an abnormal experience” and a “sane response to an insane stressor” (pg. 137). This framing positions the injured person as someone whose rights have been violated and shifts the blame of responsibility away from the individual experiencing RBTS and onto the racialized nature of institutions, environments and individuals that produce the harm.
Second, another key distinction between RBTS and PTSD lies in the role of avoidance. Under DSM-5 diagnostic criteria, avoidance of trauma-related thoughts, feelings, or external reminders is required for a PTSD diagnosis. With RBTS, however, while avoidant thoughts and feelings may be common, overt avoidant behaviors (e.g., avoiding places, events, people) are far less so, in part because the social and environmental conditions that produce racial trauma (and race-related traumatic stress) are not reasonably avoidable. For example, whereas a combat veteran who survives a car bombing on a bridge during deployment may subsequently avoid bridges as a way of managing trauma while home on leave, individuals subjected to racial violence or race-based mistreatment—whether from White strangers, coworkers, or police—cannot feasibly avoid all White people or law enforcement. Finally, severe forms of RBTS may be precipitated not only by discrete violent incidents that result in exposure to actual or threatened death, serious injury, or sexual violence (as per Criterion A for PTSD) but also by the cumulative or ongoing impact of racist encounters across the life course. As Carter (2007) argues, “one seemingly innocuous or minor event could be the last straw [or trigger] in a series of accumulated racial incidents, causing a person to feel he or she can no longer manage the stress and pain” of the recurrent nature of racialized harm (pg. 90).
Over the last decade, the Race-based Traumatic Stress Symptoms (RBTSS) scale—which includes a cluster of seven unique traumatic symptoms: depression, intrusion, anger, hypervigilance, physical reactions, low self-esteem, and avoidance—has been employed to examine the presence and severity of traumatic symptoms associated with a racist or racially discriminatory encounter (Carter et al., 2013). The RBTSS scale has demonstrated significant associations with validated and commonly used symptom and racial discrimination measures (Cohen et al., 1983; Harrell, 2000). Quantitative studies of race-based traumatic stress, across different populations, have shed light on the complex ways in which racism and racial discrimination affect various aspects of health through the manifestation of race-based traumatic stress (Dieujuste et al., 2023; Pieterse et al., 2023; Roberson & Carter, 2021). Research centered on older Black Americans’ has revealed a relationship between experiences of RBTS and depressive symptomology (i.e., low mood, persistent sadness, and loss of pleasure in normal activities), injurious physical manifestations linked to the experience (i.e., trembling extremities, persistent racing heartbeat and, pervasive recall of the encounter) and general trauma symptoms (Dieujuste et al., 2023; Roberson & Carter, 2021). Among Black emerging adults, exposure to racism is also correlated with markers of race-based traumatic stress (depression, anger, physical reactions, hypervigilance, intrusive thoughts, and low self-esteem) (Tausen et al., 2023). Quantitative data also illustrates a significant relationship between race-based traumatic stress and deleterious mental health outcomes such as dissociative symptoms (Polanco-Roman et al., 2016), and suicidal ideation/suicide-related risks (attempts) (Polanco-Roman et al., 2019). Less is known about the pathways through which occurrences of RBTS may manifest and how Black Americans, specifically Black emerging adults, detail how experiences of RBTS adversely impacts their health and well-being.
While the theory of emerging adulthood is beginning to cross disciplinary boundaries and provide novel insight into the developmental processes that occur within this life stage, it is not without critique. Existing work in this area presents a myopic view of emerging adults’ lived experiences (Syed & Mitchell, 2013, 2016). Scholarship within this body of work is also noted to overwhelmingly focus on the experiences of college-attending emerging adults (Polanco-Roman et al., 2016; Rosenbaum, 2001; Tausen et al., 2023). This hyper-focus on college-attending emerging adults does not interrogate issues surrounding social class and has created a forgotten half (Rosenbaum, 2001) of nearly 59% of emerging adults who do not attend college (National Center for Education Statistics, 2023). This exclusion constitutes a form of epistemic injustice (Fricker, 2007), whereby non-college-attending emerging adults are systematically denied recognition as knowers, and their lived experiences are omitted, albeit not intentionally, from the construction of public health and clinical knowledge. When stratified by race, the percentage of the forgotten half of emerging adults increases, as only 40% of Black emerging adults enroll in a 2- or 4-year college meaning much of existing research ignores the experiences of 60% of Black emerging adults (National Center for Education Statistics, 2023). Moreover, non-college attending emerging adults experience distinct social determinants of health and structural exposures that shape their developmental trajectories and health behaviors/outcomes differently from their college-attending peers (NeMoyer et al., 2022; Wynn & Hood, 2025). Emerging adults who do not attend college are at an increased risk for debilitating and long-term mental health disorders, are more likely to engage in substance use, and experience housing instability and uninsured status (Lau et al., 2013; Lu et al., 2022). Likewise, they are also less likely to benefit from preventive health care and/or the structured interventions that are often tailored to academic settings which have ramifications for healthcare usage in later life (Wynn & Hood, 2025). In addition to the aforementioned hyper-focus on college-attending emerging adults, the theory of emerging adulthood severely lacks an analysis of the impact of race and racism (Arnett & Brody, 2008; Syed & Mitchell, 2013, 2016). If emerging adulthood is a sensitive developmental period, as psychologist Jeffrey Arnett and colleagues (Murray & Arnett, 2018) imply the impact of exposure to social systems (i.e., racism) during this developmental stage can potentially have a profound effect on health that reverberates into later life.
Current Study
Race-based traumatic stress, a psychological by-product of racism, represents a significant mental health concern for Black emerging adults (18–27 years of age) (Bryant-Davis, 2007; Carter, 2007) given that they are 40% less likely to utilize professional mental health services than their White counterparts (Williams & Cabrera-Nguyen, 2016). Exposure to potentially traumatizing race-based incidents and a lack of engagement with professional mental health services can significantly disrupt this developmental period and trigger severe mental health deterioration and accelerated aging in later adulthood (Williams & Cabrera-Nguyen, 2016). Qualitatively investigating how Black emerging adults make meaning of RBTS and how it influences their health in a community setting, can provide evidence that illustrates how their environment shapes their lived experiences and the adverse mental and physical health outcomes they encounter. Qualitative research provides the methodological tools to investigate complex social phenomena in ways that help us understand how and why, rather than how many or how much—which is paramount when exploring sensitive topics such as experiences of racism, racial discrimination, and trauma (Silverio et al., 2022). The present qualitative study seeks to explore how RBTS manifests and illustrate why it is imperative to gain a better understanding of how RBTS operates as a threat to the health and well-being of Black emerging adults. More specifically, using qualitative methods, our study reveals how Black emerging adults make sense of race-based experiences they perceive as traumatic, and how they connect those experiences to their mental well-being. The following research questions guided this study: (1) How does race-based traumatic stress emerge within the daily lives of Black emerging adults living in St. Louis County, Missouri? (a) How do Black emerging adults make meaning of experiences of race-based traumatic stress? (2) How does experiences of race-based traumatic stress impact Black emerging adults’ mental and physical health?
Methods
Participants and Setting
Participant Demographics, n = 30
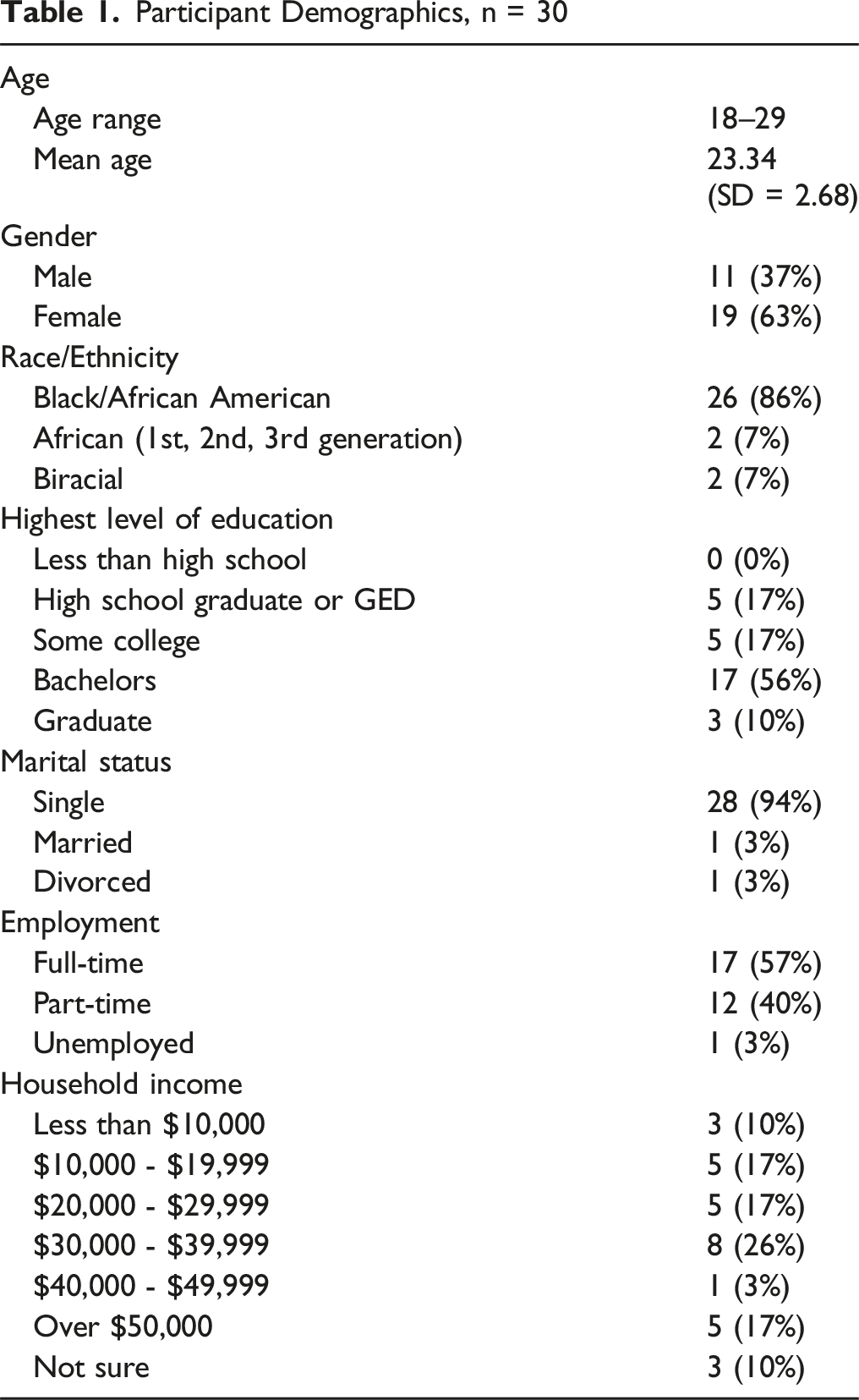
Historically rooted racial divisions within St. Louis have created a contemporary environment where health outcomes are also stratified by race (Purnell et al., 2018). Black St. Louisans, for example, are disproportionately affected by chronic conditions such as obesity, diabetes, and gun violence. Black children under the age of 15 are significantly more likely to develop asthma and live in deteriorating public housing with limited access to medical care (Harris, 2019). Thus, St. Louis serves as a powerful case study given both its history of racial oppression and contemporary manifestations of anti-Black racism, offering a compelling backdrop for studying the dynamics of race-based traumatic stress and its impact on the mental health of Black emerging adults.
Procedure
The data explored within this article are drawn from a larger qualitative methods study that investigated how experiences of race-based traumatic stress manifested within the lives of a community sample of Black emerging adults and how it impacted their mental health help seeking behaviors. The current study diverges in its focus on exploring how manifestations of RBTS negatively impacts Black emerging adults’ health and well-being. Purposive and criterion sampling techniques were used to recruit participants. We utilized the qualitative principle of data saturation and informational power to ensure we collected rich data and were able to reach data saturation (Malterud et al., 2016; Vasileiou et al., 2018). Informational power, as articulated by Malterud et al. (2016), is a theoretical model guided by the core concepts of richness, relevance, and depth of the data that helps researchers establish an appropriate and realistic sample size for a qualitative research study. Malterud et al. (2016) outlined five key factors that determine the informational power of a qualitative sample: (1) the study aim, (2) sample specificity, (3) application of established theory, (4) the chosen analysis strategy, and (5) the quality of dialogue obtained during data collection. Guided by their model, we conducted in-depth interviews with 30 participants. The final sample size reflects both the depth of data needed to adequately explore our study’s research questions and capture the variability of the participants lived experiences.
Collaborations with the University of Missouri (MU) Extension sites located in St. Louis County aided in recruiting participants located across St. Louis County and St. Louis, City, the most densely populated county and city in Missouri. Participating MU Extension staff were equipped with IRB-approved research flyers and a brief informational paragraph to recruit potential participants. The brief informational paragraph used by MU Extension introduced the principal investigator of the research study (the first author) and described the purpose of the study, the projected duration of the interview/how the interview will be conducted (i.e., via Zoom) and compensation ($25 gift card). Potential participants were informed that the purpose of the study was to explore how experiences of race-based traumatic stress manifest within the lives of Black emerging adults and how it impacts their mental health help seeking behaviors. Inclusion criteria were limited to self-identified Black or African American emerging adults between the ages of 18–27 who resided St. Louis County or St. Louis City, Missouri. Individuals who did not (1) self-identify as Black or African American and an emerging adult, and (2) reside in St. Louis County or city were not able to participate in the study. Extension employees were asked to collect demographic data (e.g., name, phone number, and email address) of individuals eligible and interested in the study. To ensure participant confidentiality, MU extension employees were instructed to abide by the IRB mandated requirements and store all sensitive participant information on a password protected computer and permanently delete all information once recruitment was completed. We received a list of 21 eligible participants. The first three authors contacted these individuals to reassess eligibility criteria and schedule interviews. Five participants were excluded because they did not reside in St. Louis County or city. Snowball sampling was utilized to recruit additional participants and ensure we met data saturation and informational power. Utilizing all our recruitment strategies, a total of 30 individuals participated in the interview.
Data Collection
Individual, in-depth interviews guided by a semi-structured interview protocol directed data collection for this study. Verbal consent and demographic data were collected before the commencement of each interview. Individual, in-depth interviews were the selected method of data collection given their flexibility (questions can be adjusted in real time and/or probing questions can be used to gain additional data) and ability to capture rich and nuanced data. The semi-structured interview guide was written and refined within three phases. The first draft of the interview guide was created by the first author (phase one). The second phase of the interview guide development involved peer reviews by content (race, racism, and mental health) and subject matter (Counseling Psychology) experts. The content and subject matter expert review were integral in ensuring theoretical and conceptual alignment and improving the clarity and flow of the interview questions (identifying leading questions and enhancing the sequences of the questions). The final phase consisted of pilot testing the interview guide.
The semi-structured interview protocol consisted of three sections that explored how RBTS manifested within the participants’ environments and impacted their health and well-being. The first section of the interview guide sought to learn more about the participants’ experiences with racism and racial discrimination within their community. Participants were asked questions such as, “What was your first memorable experience with racism?”, and “How has that experience impacted you later in life?”. The second section explored and prompted participants to conceptualize race-based traumatic stress. Questions such as “How do you define trauma?”, “What comes to mind when you think of a traumatic experience?” and “Have there been times when you feel like your experiences of trauma are associated with your race?” comprised this section. Lastly, the final section investigated participants’ perceptions of the intersections of race-based traumatic stress, mental health, and mental health help-seeking behaviors. Within this section, participants were asked questions such as “What do you think are barriers to people seeking mental health treatment in STL?”, “To what extent do you believe a therapist would be able to understand your experiences and concerns?” and “What changes would you like to see within STL to improve mental health service utilization among black people?”. Each interview was conducted via a secure and password-encoded Zoom link and ranged from 45–60 minutes. Each participant self-selected a pseudonym to use throughout the interview process.
Data Analysis
NVivo qualitative data analysis software was used to analyze the professionally transcribed interview data. The first three authors analyzed the interview data using a reflexive thematic analysis approach. Reflexive thematic analysis is an iterative analytical strategy that supports reflexive and cyclical engagement with data as the researchers critically interrogate how their positionality shapes the data analysis process (Braun et al., 2022). This approach enabled the first three authors to explore and generate nuanced insight into the intersections of racism, RBTS, and health that was grounded in and supported by the lived experiences of Black emerging adults. The first phase of reflexive thematic analysis consisted of several individual sessions of closely reading each transcript and immersing ourselves in the data. As we immersed ourselves in a close reading of each transcript, we also began the process of open coding and creating individual analytic memos. Analytic memoing was integral during this phase as it provided an opportunity for us to write down and explore the thoughts, reflections, emotions, and early interpretations that emerged as we completed the close readings. The second phase of data analysis involved individual sessions of opening and axial coding. Open coding during this phase of data analysis enabled us to individually generate inductive codes. Axial coding allowed us to explore and refine the relationship between the thematic concepts and categories we developed during our individual open coding sessions (Corbin & Strauss, 1990). The third phase of data analysis involved developing the codes refined through phases one and two into an initial set of themes. As the last phase of data analysis that we completed individually, we used that time to develop meaningful patterns and actively explore the story the codes tell about our data (Bager-Charleson & McBeath, 2022). The fourth phase of data analysis consisted of meeting as a team to discuss our analytic memos, establish inter-rater reliability, and participate in several deep discussions about our initial coding framework. Preliminary codes such as How Trauma Gets Conditioned, Feelings Associated with RBTS and Experiences of Trauma emerged during this phase of data analysis. For example, the second theme, Mental and Physical Health Symptoms of RBTS, originally titled Feelings Associated with RBTS, emerged through discussions that happened within this phase of data analysis. Minor coding disagreements were resolved through discussions until we reached a consensus (Belur et al., 2021). The fifth phase of data analysis consisted of refining and defining our themes as we developed a unified code book. The final phase of data analysis was completed through our (first three authors) combined efforts in writing our findings section (i.e., producing the report). Selective coding completed our analysis of the interview data.
Positionality
Reflexivity is the cornerstone of a reflexive thematic analysis approach (Bager-Charleson & McBeath, 2022). Being reflexive throughout the research process, especially data collection and analysis, provided us with the space to critically reflect on and interrogate how our identities, values, and assumptions/actions influenced how we engaged with the data. The first three authors identify as Black cisgender women and wrote analytic memos to ensure trustworthiness of the data. The first author (assistant professor) used her analytic memos as a tool to remain cognizant of how her status/shared racial identity and lived experiences could influence how she engaged with the data. For example, writing analytic memos throughout the data analysis process helped the first author position the participants’ narratives at the center of inquiry (rather than the margins) as she worked to actively confront any assumptions that arose during the data collection and analysis process. The first author also participated in peer debriefing (trustworthiness technique) with the last coauthor. Peer debriefing with the last coauthor, who shared expertise in Critical Race Theory and sociological understandings of race and racism, during the data analysis and manuscript development process helped her challenge assumptions, refine interpretations of the data, and ground the research study’s commitment to centering the experiential knowledge of the participants. The second and third co-authors are Counseling Psychology doctoral students and aided in data collection and analysis. Given their multicultural psychology and racial trauma focused training, the second and third authors wrote analytic memos to document their decisions, feelings, and assumptions. Moreover, their analytic memos helped them remain mindful of how their training and worldview could shape their interpretation of the data. The final co-author identifies as a Black cisgender man. He made significant contributions to writing and revising the manuscript as he engaged in multiple sessions of peer debriefing with the first author. Each coauthor contributed to the manuscript’s development by helping shape and strengthen its theoretical framework, central findings, and study implications.
Findings
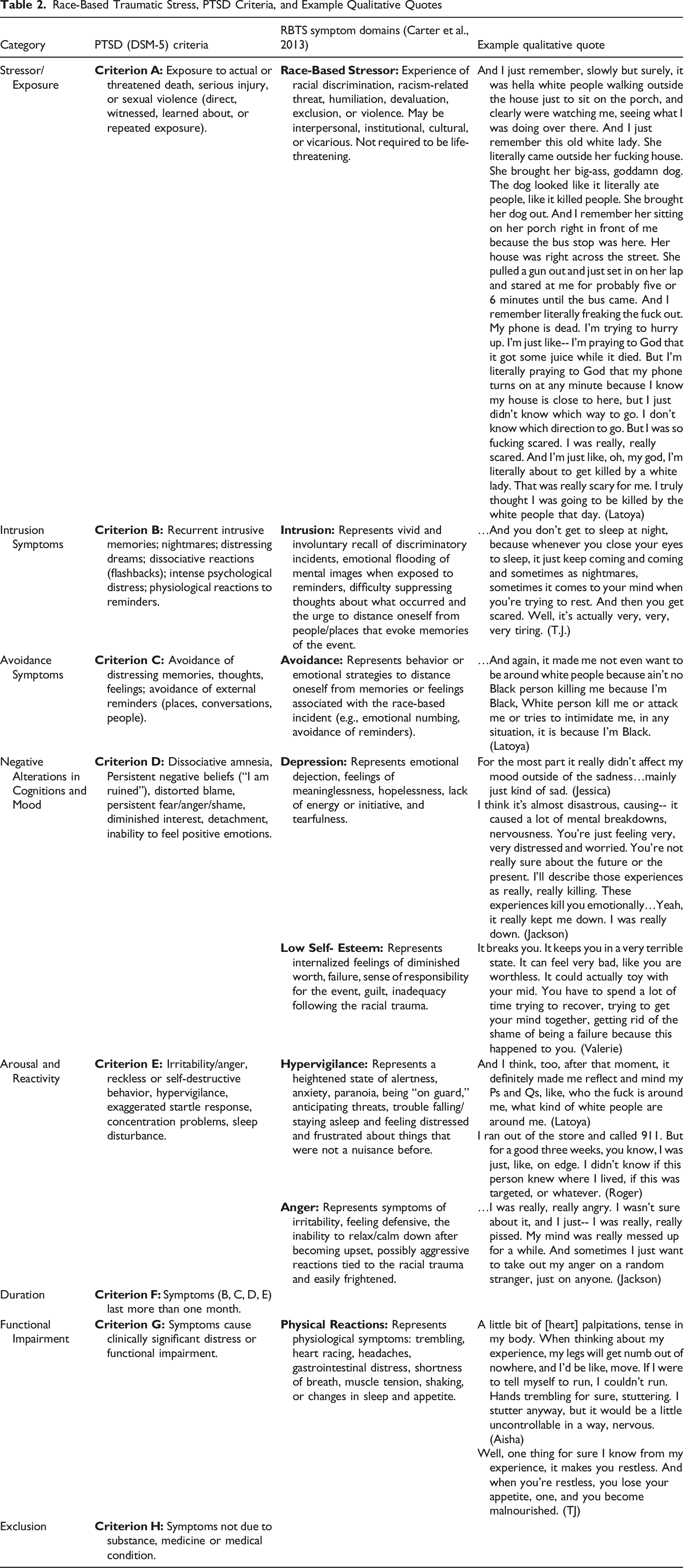
Race-Based Traumatic Stress, PTSD Criteria, and Example Qualitative Quotes
Experiences of Everyday Racism
The experiences of everyday racism theme provide personal context that illustrates how RBTS manifests in the participant’s environment. Within this theme, we explore various experiences that evoke the traumatogenic nature of race-based traumatic stress (i.e., hyperarousal and hypervigilance symptoms, cognitive worldview changes, intrusive thoughts, and anger). Among all participants, 80% (n = 24) of the sample were able to identify a race-based experience or racially discriminatory experience and 70% (n = 21) identified an event or set of events that were traumatogenic in nature. Spurred by questions that prompted participants to think about their most memorable experience of racism, their narratives provide rich detail and insight that illustrates the mundane nature of RBTS and how it manifests. For example, Jackson (25, male, speech language pathologist) shares an incident on a local train that was unexpected, emotionally traumatic, and taxed his capacity to respond when experiencing a potentially life-altering situation. There was some call for medical assistance, and some people came rushing by. Believe you me, I could actually do CPR. But I just stood there. I didn’t know what to do. I felt if I touched that [White] woman, it might just not turn out right. Maybe I was trying to give her CPR, and someone comes to the scene-- they say, yeah, a Black man is trying to choke her. He’s trying to kill her. I didn’t want something like that happening. I don’t like bad things happening around me. I don’t like being shouted at. I don't like being scolded at. I don’t like things I don’t have control over. So, I just stood there. And you could be surprised that-- while standing there… Someone came and was like, hey, what happened here? And before they could explain, she looked right into my eyes, like, yo, you did this? What did you do? You’re the only Black person in this area. What did you do to this woman?
Jackson's recollection of his experience reveals both the insidiousness of racism (being blamed for harming a white woman during a medical emergency because of one’s race) and the psychological turmoil such encounters can trigger. While he openly stated, “Believe you me, I could actually do CPR,” he ultimately did not intervene, saying, “…I just stood there. I didn't know what to do.” This hesitation was most likely fueled by past experiences and reflects a deep fear that any action he took might result in personal harm: “if I touched her, it might not turn out right. Maybe I was trying to give her CPR, and someone comes to the scene—they say, yeah, a Black man is trying to choke her. He's trying to kill her.” A concern that Jackson felt was justified given that he perceived that another bystander wrongfully assumed that he hurt the woman. The candid experience Jackson shared illustrates how experiences of race-based traumatic stress are unexpected, outside the locus of their control, and painful. Latoya (23, secondary school teacher) shared a recollection of utter fear and safety for her life when she accidentally gets off at the wrong bus stop. It was like summer of my senior year of high school. And I used to-- I caught the bus to work every day. I caught the bus and the train to work. And so I remember one day my phone died. I got on the wrong fucking bus, or I got off at the wrong stop. And it was close to my house, but it wasn't close enough to be walking from. And I remember getting off in this neighborhood-- first, you could tell like all the people in this neighborhood were White. They were truly, very scary. And I had never, ever, ever seen this on the South Side. I've actually never seen it in my life. Y’all got Confederate flags up in y’all windows. I just had never seen anything like that before so blatantly, in my face. So, I remember like getting off the bus. And I'm like, oh, this is not the right bus stop. Obviously, the bus pulled off and I realized, I would have to stand there for about five or 10 minutes for the next bus to come.
After a brief, palpable, silence she continued by stating, And I just remember, slowly but surely, it was hella white people walking outside the house just to sit on the porch, and clearly were watching me, seeing what I was doing over there. And I just remember this old white lady. She literally came outside her fucking house. She brought her big-ass, goddamn dog. The dog looked like it literally ate people, like it killed people. She brought her dog out. And I remember her sitting on her porch right in front of me because the bus stop was here. Her house was right across the street. She pulled a gun out and just set in on her lap and stared at me for probably five or six minutes until the bus came. And I remember literally freaking the fuck out. My phone is dead. I'm trying to hurry up. I'm just like-- I'm praying to God that it got some juice while it died. But I'm literally praying to God that my phone turns on at any minute because I know my house is close to here, but I just didn’t know which way to go. I don't know which direction to go. But I was so fucking scared. I was really, really scared. And I'm just like, oh, my god, I'm literally about to get killed by a white lady. That was really scary for me. I truly thought I was going to be killed by the white people that day.
Latoya’s candid account underscores how the white woman’s actions—bringing out a large dog and visibly placing a gun on her lap, both symbols of racial power and territorial control—provoked intense panic and fear of physical harm or even death. Her encounter stands as a palpable and deeply felt threat to her safety and life. Roger (22, legal assistant) shared an experience that occurred at a local gas during the height of the COVID-19 pandemic. The gas station was just two blocks from my house probably 11:00 at night or so. I'm the only one in the gas station that I see so far and I get some drinks and I get to the counter. There's no one at the counter, but there is someone else in the gas station that I didn't see before. It's just this bigger white guy with a beard. And he looks drunk. So, I'm just thinking to myself, well, he's probably just walked here from the bar or whatever. Maybe he needs the bathroom. I'm just going to try to not look at him. But then he kind of like wanders over to me. And he mumbles something to himself. And then he says, “Do you think we bleed the same?” And I was like, “I don’t know.” And so, I kind of turned away and then the cashier comes eventually. He’s checking me out and the guy-- he’s mumbling to himself louder. And then he says louder-- he's like, “Hey, do you want to bet that we bleed the same?” And he starts approaching me. He takes a box cutter from his pocket and cuts himself. And I look at the cashier. And they’re looking at me. And he’s, like, still walking towards me so, I ran out of the store and called 911. But for a good three weeks, you know, I was just, like, on edge. I didn't know if this person knew where I lived, if this was targeted, or whatever.
Experiences of this nature, either personally or vicariously experienced, spanned across the interviews. Roger’s recollection of his experience illustrates the manifestation of unwanted intrusive thoughts (“I didn't know if this person knew where I lived, if this was targeted, or whatever”) and hypervigilance/avoidance (“for a good three weeks, you know, I was just, like, on edge”) which represent core psychological symptoms associated with race-based traumatic stress.
The race-based experiences described by Jackson, Latoya, and Roger, were marked by overt acts of intimidation and threats to their safety within presumably “safe” public spaces (e.g., gas station, bus stop, and local train). These encounters were also sudden, unexpected, outside of their locus of control, and painful (Carter, 2007). The participants’ narratives also reveal how the emotional injury correlated with their experiences induced episodes of intrusive and repeated recall (e.g., Roger’s admission of being on edge for three weeks after his encounter in the gas station). The narratives within this theme reveal the mundane and extreme nature of racism embedded within the participant’s environment that operates as a conduit for RBTS to manifest.
Hypervigilance as an Adaptive Coping Response
Hypervigilance is a heightened state of behavioral, emotional, and physiological arousal that manifests when an individual perceives an element of their environment to be a threat to their safety. Hypervigilance is also a significant marker of RBTS (Carter et al., 2013; Carter & Muchow, 2017; Carter & Sant-Barket, 2015). As evidenced by their narratives, manifestations of hypervigilance were a daily and depleting occurrence that seemed to unduly burden the participants. Moreover, their experiences also reveal how hypervigilance shaped how the participants comported their bodies when attempting to navigate their environment. The narratives within this theme emerged from questions that asked participants to describe, in detail, how their most memorable experience with racism (Experiences of Everyday Racism theme) made them feel. Equally as important, the participants, unprompted, integrated race (i.e., being Black) into their response to the interview question. For example, Tyler (24, personal trainer) discussed how regardless of social standing, Black Americans must always be on guard. So, I feel like by default, every Black person, regardless of your stature, regardless of your status, regardless of your position, you are bound to be harassed for no reason at all. And I think that is really traumatizing because you have to be on watch every time. You are conscious of the things you do. You're conscious of the things you see. You try not to get in anybody's way, especially people of different skin colors, so they don't use it against you. And stuff like that is difficult for you.
Similarly, Teshell (25, software engineer) shared, My experiences and encounters with trauma is, like, it already makes me feel like it's something that I should expect [as a Black person], because it's everywhere, racism against Black people, discrimination. So, it's always there. It's lingering. Anything could happen. You could project it. You could be suspected for things you didn't do just because of color. So, it’s this never-ending feeling that makes me feel like anything could happen at any moment. So, I kind of expect trauma relating to my race.
Tyler and Teshell’s narratives illustrate an explicit connection between experiences of racism/racial discrimination and hypervigilance a coping response. They both describe hypervigilance as something one “should expect, because it’s everywhere” because as a Black person “you are bound to be harassed for no reason at all”. Tyler points out a lack of safety that is omnipresent for Black Americans regardless of their social position. Teshell states that Black people can “project it” and “be suspected for things you didn't do just because of color” which points to an internalization of racism and race-based traumatic stress. When asked how her encounter at the bus stop made her feel, Latoya stated, And I think, too, after that moment, it definitely made me reflect and mind my Ps and Qs, like, who the fuck is around me, what kind of white people are around me. And again, it made me not even want to be around white people because ain’t no Black person killing me because I’m Black, White person kill me or attack me or tries to intimidate me, in any situation, it is because I’m Black. You don’t know me. You never seen me a day in your life.
In line with current research, Latoya’s mention of reflecting and “minding her Ps and Qs” or her lack of desire to be around people is indicative of operating in a hypervigilant state as a means to control one’s environment and curtail potential encounters or threats to safety. Similarly, Camille (21, college student) shared, It is not easy, because the underlining fact is that you never know. It made me feel that if you’re Black you could be minding your own business and still be harassed or killed. You know, illegally detained. So, I feel like my experience heighten my awareness and it gives us a sixth sense, which isn’t healthy, because you feel like you always have to be on guard.
Likewise, Kelvin (25, grad student) stated, It has made me realize that when others see you as a Black person, their first instinct isn’t oh, hey, how are you doing? It’s like, man, what are they trying to do to me? Or let me watch them. But on the other hand, you see a white person, an Asian person, an Indian person, Hispanic person and you really might not have that same thought. They’re just walking around. I’m not tripping off nobody. But if you see a Black person walking, even being Black, your Blackness would be like, I mean, watch and see what they don’t know, which I do now too. If they’re trying to do something, I want to be able to do something before them.
Camille and Kelvin’s narratives reveal the insidiousness of RBTS and as a result of their experiences with RBTS how they developed a “sixth sense” of hypervigilance. Kelvin is also one of many participants who explicitly interrogated how their Blackness is seen as a marker of criminality that does not translate for White or non-Black POC individuals, which heightens the need to question “what are they up to” and “let me watch them”. Evident within all of the narratives shared within this theme hypervigilance operates as a protective mechanism to provide assurance of mental and physical safety.
Mental and Physical Health Symptoms of Race-Based Traumatic Stress
A large body of knowledge has documented how racism operates as a social determinant of mental and physical health for Black Americans (Williams, 2018). Experiences of RBTS have been empirically linked to anxiety, depression, hypervigilance, low self-esteem, and negative somatic symptoms (Carter, 2007; Carter et al., 2013). The experiences the participants shared provide conceptual clarity about the mental and physical health symptoms of race-based traumatic stress and a deeper awareness of the mechanisms that undergird the relationship between racism and poor health outcomes. In what follows, participants describe the emotional/physical symptoms they experienced as a result of an event that they perceived as traumatic. The narratives highlighted within this theme are guided by participant responses to a series of questions that prompted them to think about how their most memorable encounter with racism and racial discrimination impacted facets of their health. Admissions of anger, sadness, detachment, fear, and the urge to isolate were disclosed across multiple interviews. The depth to which the participants candidly discussed their mental and physical health symptoms not only revealed the pathways that connect the environment and race-based traumatic stress but also the resulting deleterious health outcomes. For example, when asked how the experience on the local train impacted him, Jackson stated it made him feel, …undesirable, not friendly. I think it’s almost disastrous, causing-- it caused a lot of mental breakdowns, nervousness. You’re just feeling very, very distressed and worried. You’re not really sure about the future or the present. I’ll describe those experiences as really, really killing. These experiences kill you emotionally. Yeah, I was angry for a while. I was really, really angry. I wasn’t sure about it, and I just-- I was really, really pissed. My mind was really messed up for a while. And sometimes I just want to take out my anger on a random stranger, just on anyone. Yeah, it really kept me down. I was really down.
Jackson candidly speaks about the emotions he felt ranging from nervousness, anger, distress, and worry associated with his experience. Abundantly clear within his recollection was his anger, “I was really, really pissed. My mind was really messed up for a while”. Jacksons recollection aligns with the anger and low self-esteem markers of RBTS. Similarly, in her interview, Jessica (25, barista) recounted how an experience overt racism at work impacted her negatively, namely through bouts of sadness. For the most part it really didn’t affect my mood outside of the sadness. Now if I would see other things happening to other people then I would get upset, because my main thought was you could just, could just leave us alone. Like you really don’t have to go out of your way to bother us. So mainly just kind of sad.
Jessica’s admission also illustrates how intrusive and repeat recollection (an important component of RBTS) further perpetuates the adverse symptom she experiences (Carter & Sant-Barket, 2015). She also conveys an emotional response to a direct experience of racism—sadness—paired with stronger feelings of anger or frustration when witnessing the same harms enacted on others. The emotional pattern evident with her admission reveals a normalization of her own exposure to race-based trauma, while still reacting intensely to the broader implications of such treatment for her community. Valerie (22, postal worker) shared how experiences of racism at work and within her neighborhood, …breaks you. It breaks you. It keeps you in a very terrible state. It can feel very bad, like you are worthless. It could actually toy with your mid. You have to spend a lot of time trying to recover, trying to get your mind together, getting rid of the shame of being a failure because this happened to you.
Valerie’s quote maps strongly onto the low self-esteem domain of race-based traumatic stress. She openly attributes failure and shame not to personal shortcomings, but to an experience imposed on her, revealing how racism creates conditions in which she began to see herself as deficient. In addition to the mental and emotional ramifications of race-based traumatic stress, participants also discussed the physical implications they experienced. For example, after recounting her negative experience involving a White male police officer within a well-known local sundown town, Aisha (24, non-profit) confessed how during this experience she felt, A little bit of [heart] palpitations, tense in my body. When thinking about my experience, my legs will get numb out of nowhere, and I’d be like, move. If I were to tell myself to run, I couldn’t run. Hands trembling for sure, stuttering. I stutter anyway, but it would be a little uncontrollable in a way, nervous.
For Aisha, the physical symptoms of race-based traumatic stress manifest as heart palpitations, trembling hands, and numbness that can become incapacitating. She also shares that such experiences exacerbated her stuttering. Within his interview Jerry (25, insurance agent) shared how attempting to make sense of the stress he felt when he heard of the death of George Floyd. But that’s a good question. Because I never really thought about how it affected me. I guess like I just kind of said exhausted. I guess that’s-- for me, the extent it’s been for me physically. Because when you feel exhausted, you feel it. It’s not a mental thing all the time. You don’t want to leave the house sometimes when -- when George Floyd thing happened. It was the early beginning of the COVID, but I didn’t feel like doing anything. Just seeing that video and just kind of like literally feeling drained for watching an officer kill a man on camera. I physically felt drained. So, I guess that’s the farthest to go for me physically.
Jerry highlights the physical health symptoms of race-based traumatic stress, such as feeling physically exhausted and drained and how it made him feel like he “didn’t want to do anything or “leave the house sometimes”. Building upon the sentiments expressed by Jerry, T.J. (24, mechanic) adds how RBTS impacted him physically. Well, one thing for sure I know from my experience, it makes you restless. And when you're restless, you lose your appetite, one, and you become malnourished. And you don't get to sleep at night, because whenever you close your eyes to sleep, it just keep coming and coming and sometimes as nightmares, sometimes it comes to your mind when you're trying to rest. And then you get scared. Well, it's actually very, very, very tiring.
As stated by T.J., experiences of race-based trauma can evoke restlessness, which he posits can (trickle down) to other physical symptoms of poor health such as a lack of appetite and malnutrition. Equally as important are the notions around nightmares which is a core psychological construct of race-based traumatic stress. TJ’s discussion of nightmares and the physical inability to rest/sleep evoke the same aligns with current research which illustrates that racial microaggressions and daily stress have harmful effects on Black emerging adult’s sleep quality and onset duration (Davenport et al., 2021; Maher et al., 2022). Also noteworthy, the description of the experiences he articulates also align with some physiological symptoms of depression (e.g., losing appetite, restless, feeling like everything is an effort, fearful). Race-based traumatic stress is a unique and insidious emotional response to racism that has adverse physical and mental health outcomes. The participants’ narratives provide a nuanced insight that aids in our understanding of the symptoms that comprise RBTS.
Discussion
Emerging adulthood is a critical and dynamic period of the lifecourse where the development of health behaviors shapes later life (Gee et al., 2012; Taggart et al., 2023). Understanding how Black emerging adults make meaning of RBTS and its impact on their health can have significant therapeutic implications (Dieujuste et al., 2023). Our analysis of the participants lived experiences and experiential knowledge revealed how RBTS manifests and why it is imperative to gain a better understanding of how race-based trauma operates as a threat to the health and well-being of Black emerging adults. The study findings attend to gaps in knowledge by illustrating how the social forces, ideologies, and processes embedded within the participant’s environment led to and reinforced the adverse mental and physical health outcomes they experience.
During emerging adulthood individuals grow into their unique form of independence and grapple with understanding and managing newfound responsibility and social roles, all while negotiating their own, and society’s, interpretation of their identity (Taggart et al., 2023). A sense of safety is crucial for this developmental stage as all emerging adults explore various aspects of their identity (Timmerman & Volpe, 2023). Emerging into adulthood while Black means navigating a developmental landscape marked by persistent and, at times, severe racialized stressors—conditions not typically encountered by many of their White counterparts. Utilizing qualitative methods provided rich, nuanced data that exposes how the mundane, uncontrollable, and unpredictable experiences Black emerging adults encounter operate on an individual and structural level to lead to manifestations of race-based traumatic stress. The first theme (experiences of everyday racism) candidly reveals how encounters with white St. Louis residents precipitated the manifestation of RBTS and provided foundational evidence that illustrates how their environment and everyday racist encounters represent a source of emotional and physical injury that in turn may lead to symptoms of race-based traumatic stress symptoms (i.e., hyperarousal and hypervigilance symptoms, cognitive worldview changes, intrusive thoughts, and anger). Moreover, utilizing qualitative methods aided in approaching the analysis of the participants’ narratives in a manner that moved beyond the individual level to explore how the structures embedded within their environment are harmful to their health. As a result, we were able to produce data that moved beyond a deficit-oriented outlook of Black emerging adults and their health behaviors as we illustrate how the environment the participants navigate actively shape for their socio-emotional well-being. As evident within the participant’s vulnerable admissions, they are attempting to survive, persist, and thrive within an environment that incessantly reminds them of their subjugated social status.
Emerging adults (18–29) endorse higher rates of adverse mental health outcomes, such as suicidal thoughts and planning, depressive symptoms, and dissociative symptoms in comparison to adolescents and adults (Hallensleben et al., 2018; Polanco-Roman et al., 2019). The mental and physical health symptoms of race-based traumatic stress theme provide conceptual clarity about the mental and physical health implications of RBTS and a deeper awareness of the mechanisms that undergird the relationship between racism and poor health outcomes. Quantitative analysis examining how RBTS impacts Black Americans has revealed how everyday racism and racial discrimination are strongly correlated with feelings and emotions that made participants within the study sample question the meaningfulness of their lives and experience reoccurring mental images of the racist event and body tremors (Dieujuste et al., 2023). In line with current research, participants in this study recounted experiencing symptoms that may comprise depressive symptomology (persistent sadness, the urge to detach and isolate) and physical symptoms (inability to sleep, numbness, and trembling of limbs).
Hypervigilance is a hyperaroused mental and physical state of being that is correlated with adverse mental health outcomes such as anxiety, depression, and psychological distress (Carter & Forsyth, 2010). The hypervigilance theme reveals that these reactions were not isolated but instead daily and depleting features of the participants’ lives, shaping how they carried and comported their bodies as they moved through what they often described as racially toxic environments. The participants’ narratives illustrate that encounters with overt racial harassment and hostility were associated with extremely hypervigilant and anxious reactions. Our findings align with existing research showing that Black emerging adults often rely on hypervigilance to manage encounters in their environment that they perceive to be a threat to their mental health (Timmerman & Volpe, 2023). Yet studies also caution that this strategy carries significant costs. For example, Timmerman and Volpe (2023) found that although hypervigilance can help Black emerging adults anticipate and navigate potential threats, it can also carry harmful consequences, including elevated anxiety, depression, and adverse somatic symptoms. In this sense, racial hypervigilance—being acutely aware of living in a society where racism is pervasive, recognizing one’s potential vulnerability to racial harm, and constantly guarding against it—may itself constitute a secondary form of trauma (Bryant-Davis & Ocampa, 2005; pg. 489). Importantly, this secondary trauma is not rooted in individual pathology but in the broader social environment; it emerges from navigating a racially (disordered) society in which vigilance is a necessary response to the systemic nature of—and everyday threats posed by—racism.
Limitations and Future Directions
This study is not without limitations. Data collection was limited to an urban Midwestern city and most of the participants self-identified as cis-gender, heterosexual Black emerging adults. The absence of identities outside the binary may not reflect that of Black emerging adults who are living with multiple oppressed identities. Future studies should approach recruitment from an intersectional perspective to include perspectives and experiential knowledge among Black emerging adults that are often overlooked with regard to gender identity. Although extensive recruitment efforts were implemented to ensure a community sample participated in our study, many of the participants were current or former college students. This is an important limitation given that the goal of the study was to investigate how experiences of race-based traumatic stress manifested within the lives of a community sample of Black emerging adults. It is imperative that future research focused on recruiting a community sample of minoritized individuals engage in more targeted efforts to build trust and partnerships with community leaders. Trusted community leaders can help those who are harder to overcome skepticism about research and increase comfort with study participation. Racism is a multifaceted threat to the overall health and well-being of Black emerging adults. Acts of racism can be subtle and unconscious or overt, injurious, irreconcilable, and result in manifestations of RBTS. To fully capture and articulate the cumulative effect everyday racism and RBTS have on Black emerging adults future research should be guided by theoretical frameworks and methods that can be used to actively identify the mechanisms that perpetuate racism and RBTS while also challenging the root causes.
Conclusion
Our study findings illustrate that race-based trauma is a pervasive, harmful and deeply embodied form of racial injury that manifests in the daily lives of Black emerging adults. Centering the lived experiences of Black emerging adults outside of campus contexts, this study addresses a notable gap in the existing literature. Previous scholarship examining how RBTS impacts emerging adults has primarily focused on college-attending populations and their experiences of campus-based racial discrimination (see citation Polanco-Roman et al., 2016, 2019; Tausen et al., 2023). While important, this body of work leaves significant blind spots in our understanding of how race-based traumatic stress affects Black emerging adults more broadly—particularly in everyday public spaces where racism is often normalized. Participants’ narratives vividly revealed how seemingly mundane encounters in public space—such as waiting at a bus stop, navigating public transportation, or entering a gas station—can suddenly shift into situations marked by psychological threat and emotional injury, later resulting in symptoms including hypervigilance, intrusive thoughts, anger, sadness, and somatic disruptions such as trembling, disrupted sleep, and heart palpitations. These incidents were not isolated or uncommon. Instead, they reflected the normalized racial hostility embedded within the participants’ everyday environments, particularly within the historically racialized context of St. Louis, Missouri.
Drawing upon Carter’s (2007) theoretical framework and supported by existing literature linking racism to adverse mental and physical health outcomes, the present study also contributes critical qualitative evidence illustrating the mechanisms through which racism functions as a persistent traumatic stressor. The findings also offer insight into how race-based trauma is embodied in ways that threaten long-term health and developmental well-being. This is especially consequential during emerging adulthood, a critical period of identity formation and psychosocial growth. As Camille shared, repeated encounters with racism made her feel she had developed a “sixth sense, which isn’t healthy, because you feel like you always have to be on guard.” Teshell echoed this, describing Blackness as linked to the expectation of trauma—a “never-ending feeling that makes me feel like anything could happen at any moment.” Chronic exposure to racialized trauma during this formative life stage may undermine one’s sense of control, agency, safety, and belonging—while contributing to cumulative mental and physical health consequences across the life course. While prior scholarship has documented the quantitative relationship between racism and trauma-related symptoms, this study offers a qualitative depth that captures both how Black emerging adults make sense of race-based experiences they perceive as traumatic, and how they connect those experiences to their mental well-being. Additionally, our findings pose important questions surrounding the direction of future research investigating manifestations of RBTS. For example, many participant recollections of their experience linked to RBTS explicitly mention or involved an overt threat to their safety and livelihood. As currently theorized, the racist or racially discriminatory event that operates as a conduit for RBTS does not have to be life-threatening. Given that the model does not necessitate the event to be life-threatening, it is imperative public health and mental health professionals alike interrogate the role an individual’s environment may play in how they make meaning of RBTS and its connection to their health. Future research could utilize mixed methods to explore what makes an event life-threatening and if the categorization of life-threatening has implications on the severity of the accompanying RBTS symptom(s). The narrative experiences shared by participants serve as both data and declaration—asserting that Black emerging adults possess critical knowledge about their own suffering and the injurious nature of RBTS. Importantly, participants did not merely describe pain—they offered insight into how racial trauma is internalized, negotiated, and resisted. Their stories call for a broader public reckoning with the ways racism operates not only as a form of racialized state-sanctioned violence that regulates space and behavior but also as a traumatic interpersonal injury that harms one’s mental and physical health.
These findings also carry critical clinical implications. Black emerging adults, in comparison to other emerging adult populations, consistently report the highest rates of unmet mental health need and the lowest rates of professional mental health service utilization (Williams, 2018). This underutilization not only compromises their quality of life but also increases the risk of prolonged illness following a mental health diagnosis (NeMoyer et al., 2022). When Black emerging adults do seek care, clinicians often lack the formal diagnostic language, guidance, or culturally relevant models—such as recognition of RBTS in major diagnostic frameworks like the DSM—to adequately assess or treat the symptoms they present (Carter et al., 2020). A national survey of counselors, for example, found that although 71% had encountered race-based trauma in their clinical work, the majority had not received training in how to assess or treat it (Hemmings & Evans, 2018).
This widespread gap in clinical preparation compounds existing disparities and underscores the urgency of integrating race-based traumatic stress into diagnostic frameworks, assessment tools, and therapeutic practices. In response, scholars have advocated for the inclusion of a distinct DSM diagnosis for RBTS (Bryant-Davis & Ocampo, 2007; Carter et al., 2020; Roberson & Carter, 2021). While these scholars acknowledge parallels between the symptom profiles of RBTS and PTSD, they consistently caution against simply expanding DSM-based PTSD criteria to encompass race-based traumatic stress, noting that such an approach risks misdiagnosis and obscures the unique sociocultural nature of racialized harm. In particular, they argue that PTSD does not fully capture the symptom clusters commonly associated with RBTS—where emotions such as anger, shame, and diminished self-esteem; physiological symptoms such as headaches, elevated heart rate, blood pressure, or blood sugar; and behavioral responses such as racial hypervigilance may be more central (Carter & Muchow, 2017; Dieujuste et al., 2024; Roberson & Carter, 2021). Although depression emerges as a core feature of both RBTS and PTSD for example, researchers note that hallmark PTSD features such as Criterion B intrusion symptoms (e.g., flashbacks, nightmares) or Criterion E arousal symptoms (e.g., exaggerated startle response, concentration problems, sleep disturbance) may be less prominent or absent in many RBTS cases (Pieterse et al., 2024). As Pieterse et al. (2023) explain, individuals meeting RBTS criteria may feel “afraid and scared, nervous and jittery, irritable or hostile, guilty and shamed,” while also experiencing “depression, physical pains and aches, a sense of worthlessness, and withdrawal,” a presentation that “does not…look like traditional PTSD…because a person may not meet the criteria for the core reaction of intrusion” (pp. 213–214). Together, these findings underscore that RBTS represents a distinct, clinically significant trauma response as evident within Table 2 that warrants targeted assessment and intervention strategies beyond the traditional PTSD framework.
Reimagining clinical interventions requires moving beyond narrowly prescribing medications to victims impacted by RBTS. Kira (2010), for example, emphasizes the importance of race-based interventions specific to RBTS that focus on empowering victims of oppression and increasing their perceived control. These interventions—including those that support individuals in seeking retributive justice—align with other trauma-informed, race-conscious approaches that center empowerment, agency, racial/ethnic pride, and other culturally relevant forms of healing (Carlson et al., 2018). Likewise, Holmes et al., 2024 developed a treatment protocol that spans three stages (stabilization, healing, and empowerment) and is designed to reduce distress, address internalized harm, and foster resilience in the face of ongoing racism. Their three staged approach staged moves beyond symptom reduction by targeting structural and identity-based mechanisms of harm, supporting both individual healing and empowerment in the context of enduring racial oppression (Williams et al., 2023). Without such targeted and culturally attuned interventions, RBTS will remain under-acknowledged, undertreated, and invisible in mainstream clinical practice— contributing to ongoing cycles of racialized suffering and reinforcing the psychiatric community’s longstanding failure to adequately address race-based trauma.
Ultimately, this study calls for mental health professionals, educators, and policymakers to recognize RBTS as a legitimate and urgent mental health concern. This includes developing culturally responsive therapeutic practices, expanding access to trauma-informed care, and addressing the structural determinants that render Black communities vulnerable to ongoing racial harm. Qualitative inquiry plays a vital role in this process by illuminating the material injuries of racism in the lives of Black emerging adults—harms that statistics alone cannot fully capture. Only by listening to and learning from the lived experiences of those most impacted can we begin to counter/dismantle cultures of anti-black racism while imagining and enacting forms of care that affirm Black humanity and foster healing.
Supplemental Material
Supplemental Material - “These Experiences Kill You Emotionally”: Examining How Black Emerging Adults Construct Meaning of Race-Based Traumatic Stress
Supplemental Material for “These Experiences Kill You Emotionally”: Examining How Black Emerging Adults Construct Meaning of Race-Based Traumatic Stress by Kaleea R. Lewis, Kymbriona Taylor, Tiara Watson and Jason L. Cummings in Emerging Adulthood.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by University of Missouri System - Research Council Grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Transparency and Openness Statement
This qualitative study employed purposive and criterion sampling techniques to recruit a community sample of Black emerging adults living in St. Louis County and city, Missouri. Information power was used to determine an appropriate: (1) study aim, (2) sample specificity, (3) use of established theory, (4) analysis strategy, and (5) quality of dialogue. Collaborations with the University of Missouri (MU) Extension aided in recruiting participants located across the state of Missouri. We collaborated with MU Extension sites located in St. Louis County. Participating MU Extension staff were equipped with IRB-approved research flyers and a brief informational paragraph that employees used to recruit potential participants. Extension employees will be asked to collect demographic data (e.g., name, phone number, and email address) of individuals interested in the study. Afterward, the first three authors contacted individuals to assess eligibility criteria and schedule interviews. Snowball sampling was also utilized to recruit additional participants. Data were collected through in-depth, individual interviews as guided by a semi-structured interview guide. Verbal consent and demographic data were collected before the commencement of each interview. NVivo qualitative data analysis software was used to analyze the professionally transcribed interview data. The first three authors analyzed the interview data using a reflexive thematic analysis approach. The first three authors identify as Black cisgender women. The final co-author identifies as a Black cisgender man. The second and third co-authors are Counseling Psychology doctoral students. The fourth co-author initially served as a member of the first authors dissertation committee and later as a collaborator. He made significant contributions to writing and revising the manuscript as he engaged in multiple sessions of peer debriefing. Each coauthor contributed to the manuscript’s development by helping shape and strengthen its theoretical framework, central findings, and study implications.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.