
Abstract
Emerging research suggests an uptick in mental health challenges during the COVID-19 pandemic among university students. Using a sequential explanatory mixed methods design, this study examined first-year university students’ mental health and help-seeking behaviors during the COVID-19 pandemic. Findings reveal approximately one third of students had mental health needs, but few sought out mental health services. Participants described a range of barriers across external, interpersonal, and intrapersonal domains that influenced whether or not they sought out mental health services. Findings indicate the need for structural changes among universities that increase access to services and facilitate narrative change about mental health help-seeking.
Introduction
First-year university students often experience significant distress and are highly susceptible to mental health conditions. According to Pedrelli et al. (2014), students struggle to navigate the numerous identity, academic, and social challenges characteristic of the first year of university. Many students experience isolation from key sources of childhood support, comfort, and security as they begin living independently for the first time and may be unable to travel home or visit their families frequently (Pedrelli et al., 2014). Students also face various social challenges during this time as they aim to find a sense of connectedness and belonging amongst a new peer group (Lederer et al., 2021). Additionally, Lederer et al. (2021) propose that financial struggles and vast social media usage further contribute to stress levels experienced by this population (Lederer et al., 2021).
The COVID-19 pandemic has exacerbated these typical emerging adulthood and university stressors (Lederer et al., 2021). Copeland et al. (2021) found that a majority of first-year university students in their sample experienced a substantial decline in daily wellness and mood after the start of the pandemic. Another nationwide survey of university students found that 85% of undergraduates reported increased stress levels since the onset of COVID-19 (Lee et al., 2021). These heightened stress levels can be attributed to instability and social isolation caused by pandemic-induced disruptions in on-campus activity, shifts to online/remote learning, and virtual social clubs/organizations. To cope with these stressors, university students often rely on relaxation techniques, media use, exercise, and avoidance strategies, such as refraining from watching or reading the news (Sutherland et al., 2023).
Though emergency measures have been lifted and regular activities have resumed, COVID-19 has had long-term consequences on individuals’ mental health. Several scholars have documented a deterioration in mental health (i.e., increases in anxiety, depression, PTSD, and loneliness; decreased life satisfaction) among the general population during the pandemic (Benke et al., 2022; Li et al., 2023). Similar findings hold true for university students. Allen et al. (2023) tracked the mental well-being of n = 554 British university students over a year during the pandemic and found that students continued to struggle with prolonged and high levels of anxiety and psychological distress. Other scholars have reported similar findings (Al-Kumaim et al., 2021; Wathelet et al., 2022).
With the additional stressors imposed by the pandemic, it can be reasonably hypothesized that rates of support-seeking would increase among university students. However, help-seeking among students remains relatively low: of the more than 1.3 million U.S. adults surveyed during the first eight months of the pandemic, 18% of young adults reported an unmet need for mental health counseling – 8% higher than the study’s average (Coley & Baum, 2022). Some commonly reported barriers to help-seeking that have contributed to poor service utilization rates amongst undergraduates over the past decade include stigma, lack of perceived need, and lack of knowledge about services (Cadigan et al., 2019; Eisenberg et al., 2012).
Further, many barriers to mental health service utilization prevalent before the onset of the pandemic have persisted, along with additional obstacles specific to COVID-19. During the pandemic, face-to-face peer counseling sessions and professional consultations were limited due to in-person restrictions. According to Lee et al. (2021), 60% of American university students found it more difficult to access mental health services during COVID-19 (Lee et al., 2021). The combination of these obstacles with the pre-existing barriers led to the persistence of poor help-seeking behaviors and lowered service utilization rates throughout the pandemic. For instance, a recent survey of 195 undergraduates at a public university in Texas revealed that 71% of students reported heightened stress and anxiety levels during COVID-19, but only 5% of them utilized counseling (Lee et al., 2021). The mental health treatment gap is particularly concerning among racial/ethnic minority students. Lipson et al. (2022) report that despite increases in mental health problems, students of color have the lowest rates of mental health help-seeking and service utilization, highlighting considerable inequalities in access to treatment and widening inequities. More research is needed to further understand the impact of pandemic-related factors on the help-seeking behaviors of first-year university students and how they compare across diverse groups.
In a longitudinal survey of n = 430 university students (Cohen et al., 2023), found that though the majority of students reported above average levels of stress and loneliness and increases in mental health symptoms (e.g., anxiety, mood disturbances) at each study time point, only a third received some type of mental health service during the study period. Building on this work, the present study utilized a sequential explanatory mixed methods design to understand first-year students’ experiences related to how the COVID-19 pandemic both contributed to their distress and impacted their mental health help-seeking behaviors. Specifically, this study asked: 1) How aware were first-year students of their own distress during the COVID-19 pandemic, and how did this differ among gender and racial/ethnic groups? 2) How did first-year students cope with their distress during the COVID-19 pandemic? 3) Did first-year students seek out mental health services? and 4) What barriers did first-year students experience when they sought out mental health services?
Materials and Methods
Research Design
This study is a secondary analysis of a longitudinal project that aimed to understand university students’ distress and willingness to seek mental health services. This study specifically examines data from first-year students, as findings from the parent study are not disaggregated by student class standing. Results of the parent study are published elsewhere (Cohen et al., 2023). This study used a sequential explanatory mixed methods design (quan → QUAL) to understand how the pandemic impacted the mental health of first-year university students in two phases. In Phase 1, the authors administered an online longitudinal quantitative survey (August 2020 - February 2021) to students at a university in Texas to understand the mental health status and service utilization during the COVID-19 pandemic. Informed by quantitative results, Phase 2 consisted of one-hour virtual in-depth interviews with a subset of survey respondents to understand how the pandemic impacted student mental health help-seeking. The mixed methods approach of this study offers a comprehensive understanding of first-year university students' mental health during the COVID-19 pandemic. While Phase 1 provides a snapshot of first-year students’ mental health status and service utilization that allows for comparison to similar populations, Phase 2 offers insights into how and why first-year students sought mental health support and what barriers they experienced. Both studies were approved by the university’s Institutional Review Board.
Setting
Data were collected from students at a large public university in Texas during the 2020-2021 academic year. The university maintained a primarily online educational format in which 77% of course registrations were online-only, 18% hybrid, and 5% in-person. The university offers enrolled students counseling and mental health services, including assessment and referral, group and individual counseling, psychiatry, and well-being services (e.g., wellness centers). These services include a 24/7 crisis hotline and a 24/7 virtual mental health platform. The university operates a website where all information about students’ physical and mental health services can be found, and the counseling center has a physical location on campus where students can go for information. When asked, “With whom do you currently live?” in the Phase 1 survey, the majority of students reported living with their friends/roommates (43.4%) or their family (42.5%).
Sampling Strategy and Study Participants
The Phase 1 survey invitations were emailed to a stratified random sample of 2,000 students from a large public university with an approximate enrollment of 50,000 undergraduate and graduate students in Fall 2020. Four hundred and twenty-four (n = 424) students consented to participate and completed the survey; a sub-sample of first-year students who completed the longitudinal survey (n = 111) was utilized for this study. Phase 2 interviews were conducted with a stratified random sample of students who completed the survey. Forty-eight students were invited to participate in an interview. Twenty students did not respond. The final interview sample size was n = 28 first-year students. Both samples were constructed to match the racial/ethnic and gender makeup of the university student population.
Measures
Phase 1 Survey
The Phase 1 survey included demographics, current mental health symptoms, and access to mental health services. The demographic section consisted of questions related to participant age, race/ethnicity, gender, sexual orientation, class standing, and education delivery mode.
The current mental health symptoms section included three measures that have been validated for use with university students: 1) the Perceived Stress Scale (PSS), a 14-item measure of perceived stress on a five-point Likert scale (Dias et al., 2015); 2) the Patient Health Questionnaire-2 (PHQ-2), a two-item depression screener on a four-point Likert scale (Zhang et al., 2013); and 3) the Three-Item UCLA Loneliness Scale (ULS), a brief measure of perceived loneliness on a three-point Likert scale (Matthews-Ewald & Zullig, 2013). This survey section also consisted of three locally developed questions measuring the impact of COVID-19 and current events on a five-point Likert scale (Cohen et al., 2023).
The final section of the survey consisted of questions about participants’ perceived need for mental health services, history of mental health service utilization, recent mental health service utilization, and interest in mental health app utilization. In follow-up surveys, participants were asked if they utilized mental health services and whether those services met their needs.
Phase 2 Interviews
The interview protocol was collaboratively developed by a team of researchers that included undergraduate and graduate students. The interview protocol was informed by survey responses and explored the perceived impact of the COVID-19 pandemic on participants’ mental health and experiences participating in mental health services (if applicable). For example, the protocol asked, “Have you talked with friends, family, or a professional about your distress around the COVID-19 pandemic? If so, who did you talk to, and what was it like? If not, why not?” and “Have you considered connecting to a mental health service provider in 2020? If so, why didn’t you? What got in the way?” Each researcher subjectively utilized probes informed by Rickwood’s Model of Mental Health Help-Seeking (2005) to better understand each participant’s perceived mental health and unique experience seeking mental health help.
Procedures
Phase 1 Survey
The survey was designed and administered online using university-licensed survey software. The initial survey was administered to participants during the first full week of classes (August 2020), and follow-up surveys were distributed the following five months. The first survey asked participants to reflect on the beginning of the pandemic (March 2020), while the follow-up surveys asked participants to reflect on the past 30 days. Participants received a $10 electronic gift card for each survey and a $15 bonus electronic gift card for completing all six surveys.
Phase 2 Interviews
Interviews were conducted virtually using university-licensed video conferencing software. A subset of survey participants were invited to participate in an interview via email. Interested participants were prompted to complete a consent form before scheduling an interview. Interviews were conducted in the Spring of 2021. The majority of interviews were co-facilitated by two members of the research team. Interviews were audio-recorded with the interviewee’s consent. Participants received a $50 electronic gift card upon completion of the interview and a mental health resource list.
Data Analysis Plan
Phase 1 Survey
Descriptive statistics were employed to describe participant characteristics. Due to the small number of self-reported gender-diverse participants, genders were grouped as women/gender-diverse (0) and men (1) to allow statistical comparisons. To allow for comparisons by race/ethnicity, participants identifying as Black, Hispanic, multi-racial, or another race were grouped and compared to participants who identified as White and Asian/Pacific Islander. Students were not consulted regarding gender and race/ethnicity terminology; instead, terms used mirrored the parent study and were informed by evidence of disproportionate negative impacts of the pandemic on historically marginalized racial/ethnic groups and increased rates of discrimination during the pandemic (Hooper et al., 2020; Hahm et al., 2021). Mental health measures (i.e., PSS, PHQ-2, TILS) were assessed at six time points using repeated measures analysis of variance (ANOVA). Fisher’s Least Significant Difference (LSD) test was used for post hoc comparisons. SPSS version 27 was used for all statistical analyses, and a probability level of .05 was used for statistical significance.
Phase 2 Interviews
Interviews were audio-recorded, transcribed verbatim, and scrubbed of identifying information. Authors assigned participants pseudonyms to protect confidentiality. The authors employed thematic analysis (Boyatzis, 1998; Braun & Clarke, 2006) to understand how the pandemic impacted participants’ mental health and help-seeking experiences. The authors reviewed the quantitative results and then created an a priori coding structure to focus the analysis of the qualitative interviews on how participants perceived mental health services and what barriers influenced their mental health help-seeking behaviors.
Results
Sample Characteristics
Demographic Characteristics of Institutional Population Versus Study Sample, n(%).
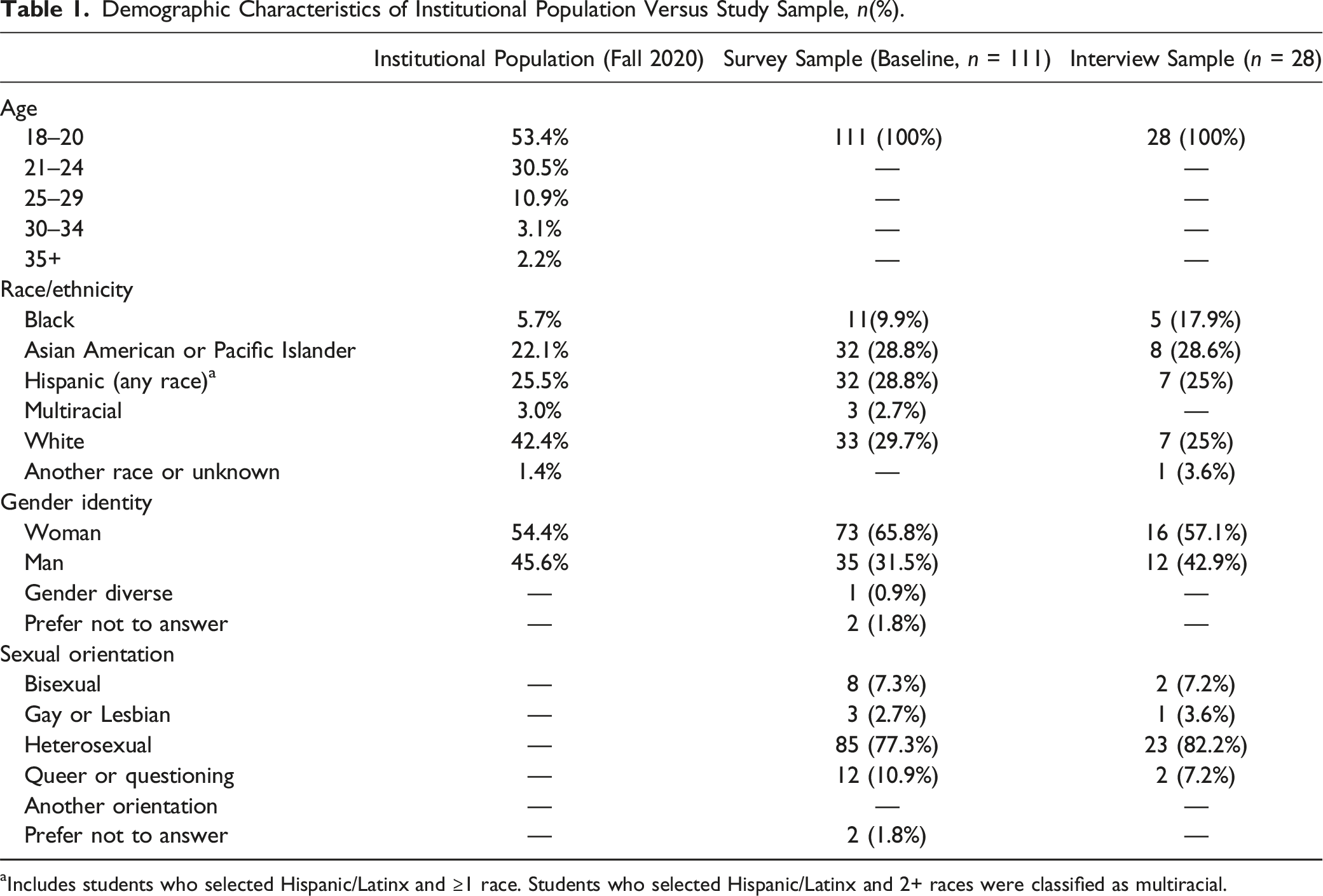
aIncludes students who selected Hispanic/Latinx and ≥1 race. Students who selected Hispanic/Latinx and 2+ races were classified as multiracial.
Quantitative Results
Descriptive Statistics for Mental Health Symptoms Over Time.
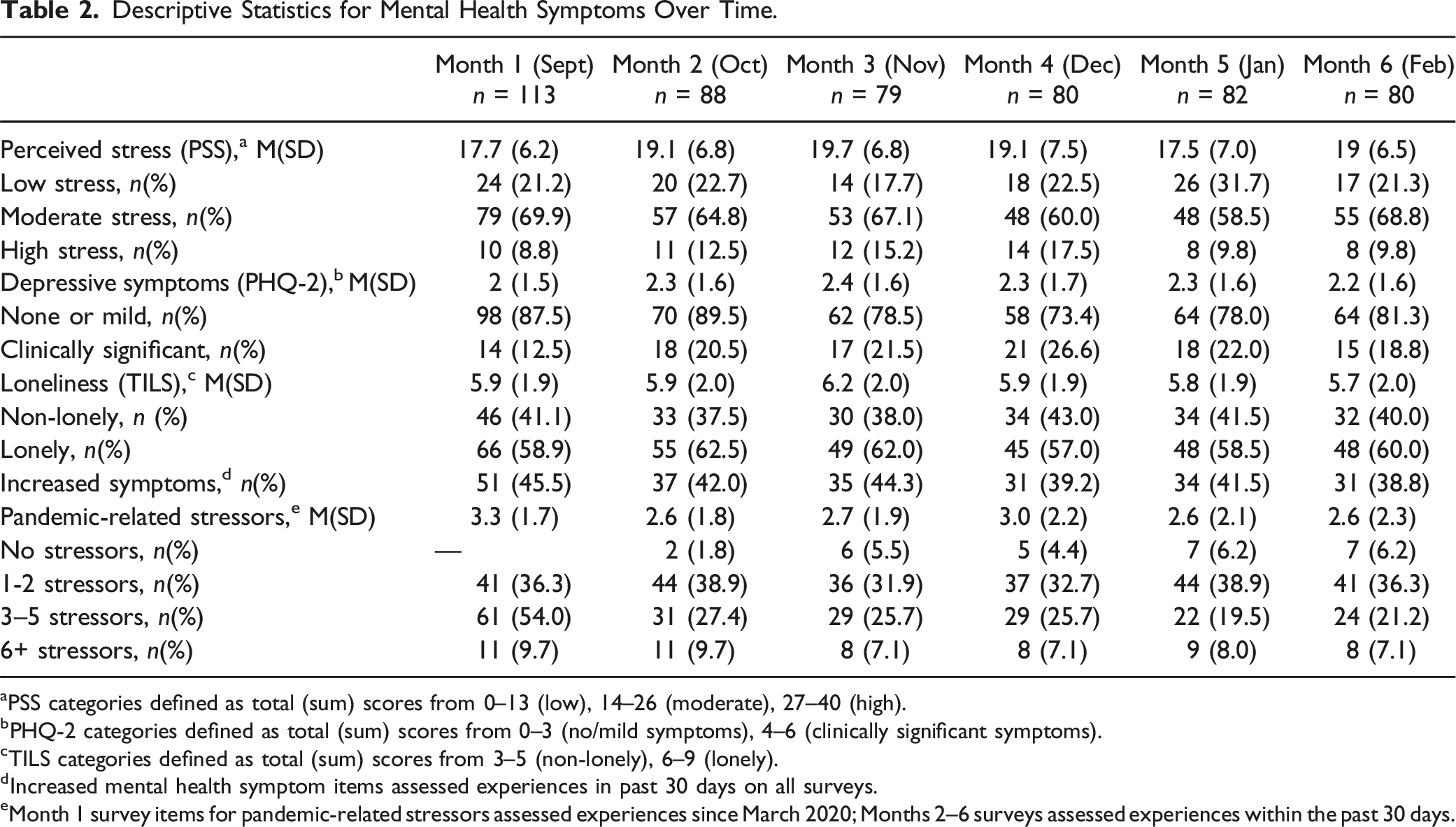
aPSS categories defined as total (sum) scores from 0–13 (low), 14–26 (moderate), 27–40 (high).
bPHQ-2 categories defined as total (sum) scores from 0–3 (no/mild symptoms), 4–6 (clinically significant symptoms).
cTILS categories defined as total (sum) scores from 3–5 (non-lonely), 6–9 (lonely).
dIncreased mental health symptom items assessed experiences in past 30 days on all surveys.
eMonth 1 survey items for pandemic-related stressors assessed experiences since March 2020; Months 2–6 surveys assessed experiences within the past 30 days.
Prevalence of COVID-19-Related Stressors Over Time, n(%).
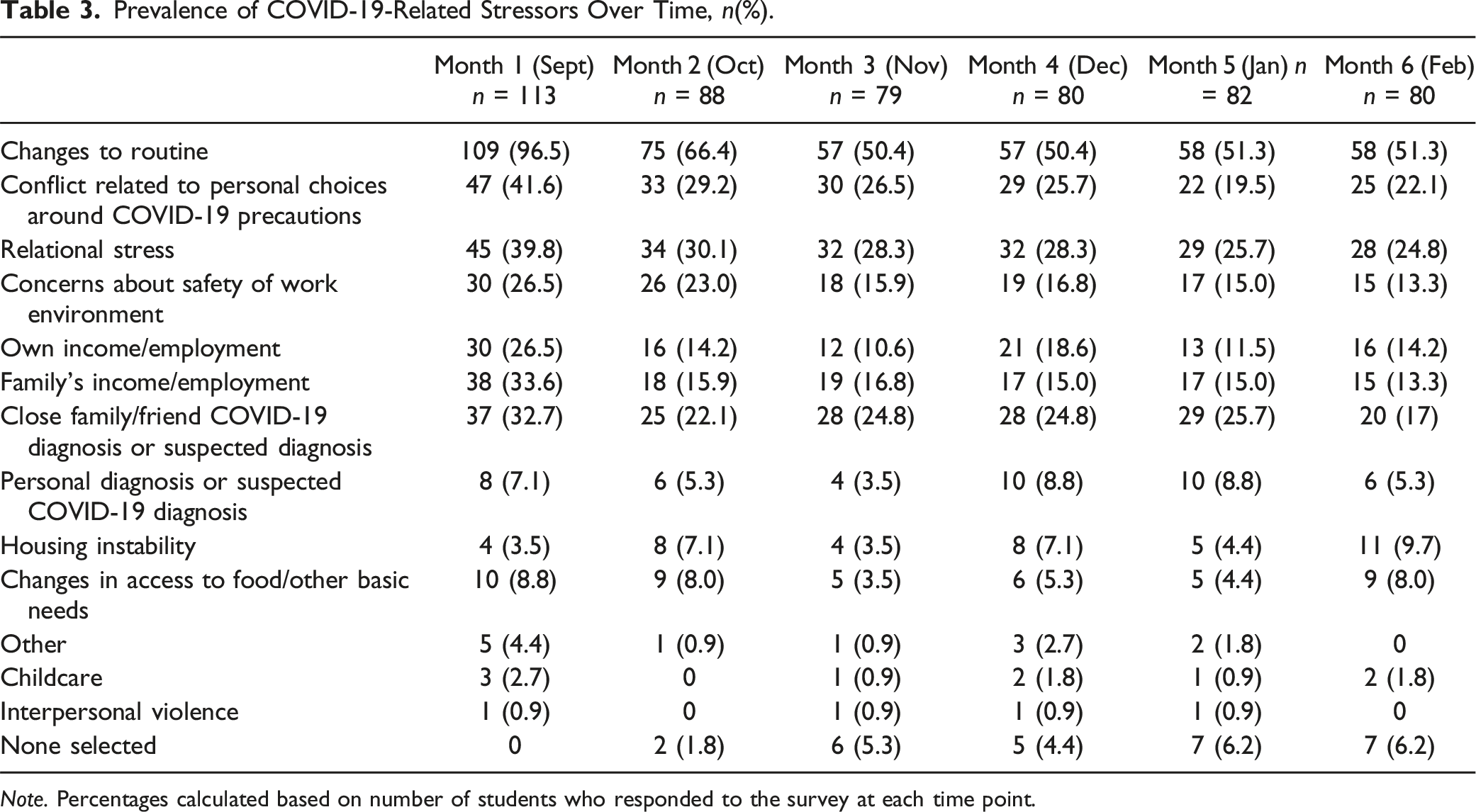
Note. Percentages calculated based on number of students who responded to the survey at each time point.
Descriptive Statistics for Mental Health Service Utilization and Support-Seeking Over Time, n(%).
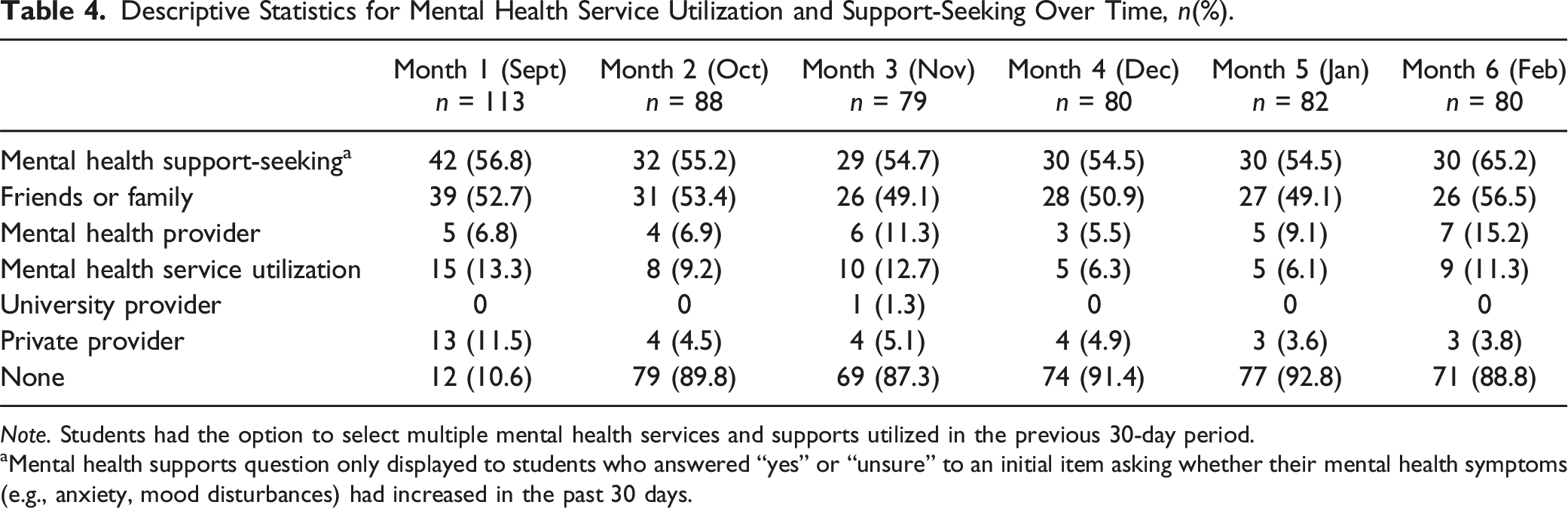
Note. Students had the option to select multiple mental health services and supports utilized in the previous 30-day period.
aMental health supports question only displayed to students who answered “yes” or “unsure” to an initial item asking whether their mental health symptoms (e.g., anxiety, mood disturbances) had increased in the past 30 days.
Results of One-Way Repeated Measures ANOVA of Mental Health Measures Over Time.
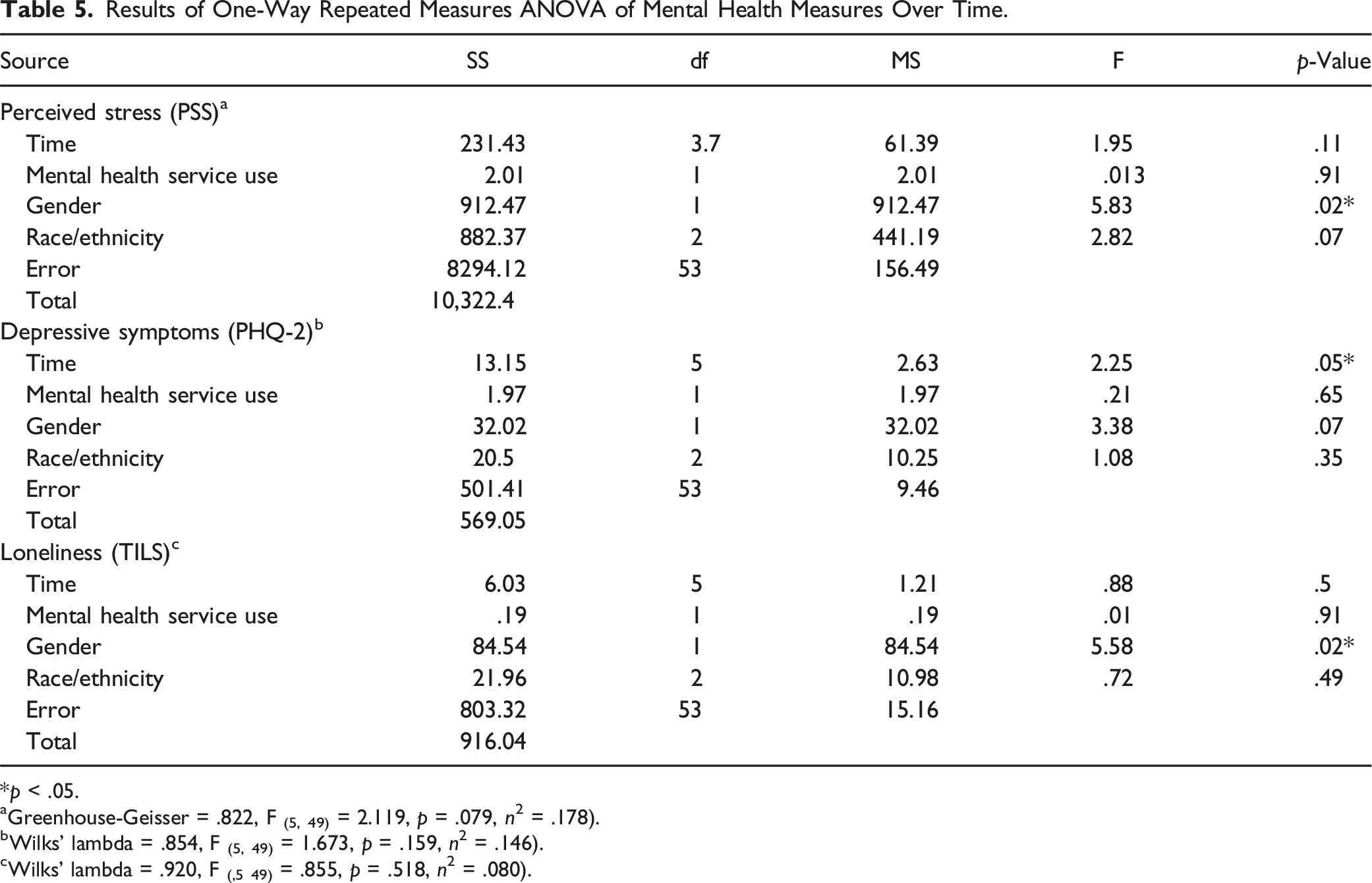
*p < .05.
aGreenhouse-Geisser = .822, F (5, 49) = 2.119, p = .079, n2 = .178).
bWilks’ lambda = .854, F (5, 49) = 1.673, p = .159, n2 = .146).
cWilks’ lambda = .920, F (,5 49) = .855, p = .518, n2 = .080).
Qualitative Results
Qualitative results provided insight into participants’ decisions to seek out mental health services, including the barriers that shaped their experiences.
Willingness to Seek Out Mental Health Services
When participants were asked about their engagement in mental health services, four pathways emerged: 1) participants did not consider seeking help (n = 12, 44%), 2) participants only considered seeking help (n = 8, 30%), 3) participants attempted to seek help but experienced barriers (n = 3, 11%), or 4) participants sought and received help (n = 4, 15%). Most participants who did not consider services were men (n = 7, 58%), and the majority of participants who considered services were women (n = 7, 88%). All participants who attempted to access services but experienced barriers were racial/ethnic minorities (n = 3, 100%). No demographic patterns were apparent among participants who accessed and utilized services.
Perceived Barriers to Mental Health Help-Seeking
While many participants (n = 12, 44%) felt like they did not need mental health services, those who did described three types of barriers that influenced whether or not they sought out mental health help: external (i.e., systems, structures, events, or circumstances outside of their control), interpersonal (i.e., relationships with family, friends, or peers), and intrapersonal (i.e., personality, preferences, knowledge).
External Barriers
Participants described various external barriers that influenced their decision to seek out mental health services. Common barriers included not knowing where to start, confusion navigating the university website, difficulty scheduling appointments (e.g., lack of timely availability, inflexible hours), session limits (e.g., three one-hour sessions), and being too busy with school pressures. For example, Halima (#6) sought out university mental health services due to relational stress with her family but struggled to understand how to access those services: “I went to the website, and it was so confusing to me that I gave up… I was like, ‘How do I schedule an appointment?’… I definitely went to the website… and then I gave up on it.”
For some participants who were utilizing mental health care services before attending university, moving to campus for the school year disrupted their care. This was true for Andrew (#24), who began engaging in mental health services after the pandemic due to social isolation but discontinued services when he moved to the university only to find out he still needed support: I think that was right when the pandemic kind of started… and then I stopped talking to him [mental health provider] right when I came to [university] last semester… I kind of stopped talking to him [mental health provider] because I had this idea that, you know, coming to [university], and living in the dorms, and just being at [university] would fix a lot of my problems, especially related to like social things, like wanting to be with new friends, that kind of stuff… And I came to find out that the issues didn’t really go away.
While some participants, like Eduardo (#15), viewed virtual mental health services as less stigmatizing – “I know there’s like telehealth kind of going around right now, like seeing a therapist virtually. I think that can be like a bit less scary maybe. Like instead of like going in person and walking into like their office” – most participants expressed a preference for in-person services, as they felt it was more personal and made it easier to talk about deeper things. Danita (#44) shared, “I feel like I [would] be able to open up more and I [would] be able to form a legitimate connection with the person [mental health provider] or they [would] be able to understand me more.”
Interpersonal Barriers
Participants also described interpersonal barriers that influenced their decision to seek out mental health help. Several participants explained that their culture played a role. For example, Chimamanda (#37) reflected, “There’s like stigma… like in the Black community, the African community, with like mental health, it’s kind of just brushed over or talked around or like spiritualized or whatever.” Similarly, Taj (#8) shared, Like I live in a family that- I guess in my culture, mental health is not really talked about. So, I never really connected things that are going on in my life with mental health. So, I wouldn’t really- I guess I wouldn’t know what to talk about if I was to talk to some professional in the industry.
Relatedly, another interpersonal barrier for participants was their families. Several participants described their families as unsupportive of mental health services. For some, this was a passive resistance in which parents “don’t think too greatly of it,” as was the case for Shivani (#45). For others, this was an explicit lack of support, as described by Catherine (#27), who shared: My mother does not believe in mental health… She thinks that I can talk to her about what I’m feeling, and I explained to her that she’s not qualified to help me like that, even though she thinks that she can do that.
Privacy concerns were another interpersonal barrier that played a role in participants’ mental health help-seeking. While virtual mental health services created flexibility, participants expressed concerns about family members overhearing conversations, which prevented them from fully engaging. This is exemplified by Jessica (#29), who explained: And it’s definitely hard, obviously, with technical issues or, of course, like privacy. I mean, I am in my own room but of course I’m not the only person in my house and because it’s such like a sensitive topic, it’s definitely hard sometimes I feel like to get what I want like across.
Intrapersonal Barriers
Intrapersonal factors emerged as the most common barrier to participants’ seeking out mental health help. Many participants lacked knowledge about services regarding cost, who services are for, and how services can help.
Some participants mentioned cost as a barrier to seeking and utilizing mental health services. For some, like Jiya (#34), their concerns were rooted in previous experiences of managing the expense of multiple providers and medications while uninsured. For others, this concern was rooted in a lack of knowledge about the actual cost of services. For example, Eduardo (#15) shared, “I think it’s also like pretty expensive and like for me like I’m a pretty-like pretty frugal person, like I find it hard to like justify the price.”
Several participants felt like their problems were “not big enough” for them to seek out mental health services. This was aptly described by Shantell (#11), who shared, I just always assumed that if you need to reach out [for] mental health services or professionals, like it had to be something very serious, and I wasn’t really sure if like this was serious enough, so I didn’t want to waste anybody’s time.
Halima (#6) shared a similar sentiment, stating, …Like the services they offer, […] I feel […] like my problem didn’t matter that much because it’s not – like it’s a very stupid thing, like ‘Oh, your sister fought with you, oh hurray.’ You know what I mean? […] It wasn’t like [as] serious as the other mental services probably talked about, I guess.
Other participants shared that tending to mental health needs felt like “self-improvement” or a luxury as opposed to a necessity. For example, Claudia (#42) stated, “But it’s hard, I think, with school and everything. It’s hard to focus on like myself and stuff.” Similarly, Latasha (#39) stated, I’m still kind of at that point where like I feel like [if] I’m not doing schoolwork that I’m wasting my time. So, if it- if it doesn’t like benefit me in any way school-wise, then I’m probably not doing it.
A few participants felt afraid to engage in mental health services. When asked what got in the way of seeking out mental health services, Catherine (#27) shared, “Maybe just being afraid. I don’t know what of, but [it is] just kind of intimidating being vulnerable like that.” Chimimanda (#37) described her ambivalence: Another reason is I’m kind of afraid of like the unknown. Like what if you’re diagnosed with something or like- I just don’t know if it’d be opening a can of worms, and I don’t know if I’m ready to like ambush it right now.
Mixed Methods Results
Though quantitative and qualitative findings are meaningful in their own right, the sequential explanatory mixed methods design of this study facilitates the utilization of both data sources to gain a richer understanding of first-year students’ help-seeking behaviors and mental health service utilization. Quantitative findings provided a snapshot of students' mental health status and help-seeking behaviors, revealing that students have high mental health needs but low levels of mental health support-seeking and mental health service utilization. Informed by these results, we sought to understand how and why students sought mental health support. Qualitative findings revealed pathways to help-seeking and provided descriptive insight into students’ decisions to seek mental health services and the multi-level barriers that shaped their experiences.
Discussion
First-year university students experience numerous stressors that contribute to significant distress and increase their susceptibility to mental health problems. The COVID-19 pandemic exacerbated these pre-existing stressors and added new ones. This study aimed to understand how the pandemic contributed to first-year students’ psychological distress and impacted their mental health help-seeking behaviors.
The first research question explored students’ awareness of their own psychological distress during the COVID-19 pandemic. Participants reported low levels of depression but high levels of stress and loneliness. This is comparable to findings from Son et al. (2020), who found that 71% of students in their sample (n = 195) reported increases in stress and anxiety due to the pandemic. However, these findings also differ from those of Fruehwirth et al. (2021), who found that depression increased between 22%–32% among first-year students during the pandemic. Differing results regarding depression could be a function of different measures used. Our findings suggest that first-year students have high levels of stress and loneliness, which the pandemic may have exacerbated.
The second research question explored how students coped with their psychological distress during the pandemic. Although participants indicated high levels of stress and loneliness, only 25% sought professional mental health services during the study period. These findings extend the large body of literature showing that university students seldom utilize mental health services, even amid the COVID-19 pandemic when their mental health concerns increased and indicated a need for professional support (Healthy Minds, 2019; Lee et al., 2021; Son et al., 2020). Despite low rates of mental health service utilization, first-year students often turned to informal sources of support, such as family or friends, aligning with existing evidence (Brown et al., 2014; Healthy Minds, 2019; Son et al., 2020).
The last two research questions asked if first-year university students sought mental health services and what barriers they experienced when seeking them. Data revealed four help-seeking pathways: not considering, only considering, attempting but experiencing barriers, and utilizing. Researchers observed that, in general, fewer men than women sought out mental health services. This finding echoes research on gender differences in mental health help-seeking and service use (Rafal et al., 2018; Seehuus et al., 2021). All participants who attempted to access mental health services but experienced barriers were racial/ethnic minorities, with common barriers being primarily related to structural issues, such as the limited availability of in-person services, a confusing website, unhelpful receptionists, and long waitlists, adding to existing literature about barriers to university mental health services for students with minoritized identities (Busby et al., 2021; Eisenberg et al., 2011; Roulston et al., 2022). Although many of the barriers participants expressed experiencing are reflected in existing literature, it is notable that all participants in the attempting group were racial/ethnic minorities. It is unclear if racial/ethnic minority participants in this study were more likely to experience barriers that wholly prevented them from receiving services than were White participants or if they were more likely to end the search for services upon experiencing barriers than were White participants. Additional research is needed to answer this question. Further research is also warranted to better understand the nuance of how structural barriers to help-seeking may contribute to intrapersonal barriers around help-seeking (e.g., does experiencing limited availability of services increase one’s belief that they should self-manage their symptoms?), especially for racial/ethnic minorities.
Participants elucidated three types of barriers that influenced whether or not they sought mental health support. Of note, participants were concerned about the expense of utilizing mental health services, a concern not uncommon among university students (Busby et al., 2021; Cadigan et al., 2019). Results indicate that participant hesitancy due to cost may result from 1) lack of knowledge about the actual cost of services, or 2) conflicting information and difficulty navigating university websites, corroborating existing research (Marsh & Wilcoxon, 2015). For example, upon examining the mental health services webpage of the university at which this study took place, though service fees are listed on the university counseling center’s website, they are embedded within layered menus and contradictory language (i.e., service fees listed first, followed by “students are never turned away for their inability to pay” two-thirds of the way down the page). This is an intervenable factor that requires little more than universities simplifying their websites and more clearly stating the cost of services.
Perhaps more salient, though, were intrapersonal barriers. Many participants lacked knowledge about mental health services, expressing that mental health services felt like a “luxury” when they should be focused on schoolwork and fear of what engaging with mental health services might mean (e.g., diagnosis). Interestingly, several students reflected a sentiment that they did not feel their problems were severe enough to warrant mental health support and a sense that they might be wasting their or someone else’s time if their concerns were not more severe. Given that roughly two-thirds of the participants in this sample reported high levels of stress and loneliness and were experiencing several pandemic-related stressors, it is surprising that they did not find their needs warranted support. This finding may indicate poor mental health literacy, a lack of understanding of the breadth of support and skill building that mental health services can offer, and a need for interventions that address problem-recognition skills (Cadigan et al., 2018).
On the other hand, some participants simply expressed they “just didn’t need it” (i.e., formal mental health support), referencing how they felt healthy, well, and able to manage stress through various coping mechanisms (e.g., social support, exercise, prayer/religious practices, hobbies). Indeed, most participants relied on friends and family for support rather than formal support. This may reveal a preference for self-management of mental health concerns (Son et al., 2020) or may be a further reflection of a lack of understanding of what mental health services can offer (e.g., an enhancement of coping skills). Future research would benefit from exploring whether students do not engage with mental health services due to a perceived lack of severity and need or due to an actual ability to self-manage and preference for and efficacy of informal supports.
Overall, study findings have several implications. First, universities should strengthen their efforts to promote a culture of emotional wellness and mental health help-seeking, increase mental health service literacy, and reduce barriers, particularly among first-year students. Importantly, all of these should consider the unique barriers experienced by this population as identified in this study. Suggestions include making cost information transparent, easy to understand, and easy to find; better explanations of the many reasons someone might benefit from mental health supports (e.g., to learn ways to enhance skills to self-manage mental health concerns); and an explanation that mental health services are not only for individuals in crisis or with “serious” needs and that those who perceive their needs to be minor may also benefit. Further, outreach efforts should particularly target demographics and populations who are less likely to seek services, such as men, as well as those likely to experience barriers when attempting to access services (i.e., racial/ethnic minorities). Notably, as this study was conducted in the context of the COVID-19 pandemic, should a similar event occur in the future, universities would benefit from taking a public health approach to mental health comparable to that of physical health. Examples of this approach might include increased psychoeducation about the effects of isolation and loneliness, signs and symptoms of mental health distress, and information about how to access services both through the university and more broadly (e.g., virtual options).
Universities also need to offer a wide array of mental health services to support the range of student needs and preferences (e.g., individual, group, in-person, phone, videoconference). This diversity of options is essential in the context of the pandemic, given that many students were off campus, out of the city, or bound by quarantine restrictions and, therefore unable to access in-person mental health services. Notably, students in this study who received formal support went to private providers rather than university providers. This contradicts previous studies indicating student preferences for university mental health services (Flaherty, 2023; Lipson et al., 2019). Further research is needed to better understand this trend, but universities should provide students with information about accessing mental health resources outside of the campus community given this finding.
This study found that most students relied on friends and family for support over formal mental health support. This calls for a multiplicity of supports beyond therapy type and mode. Indeed, offering options such as peer support, affinity groups, or mentoring opportunities that allow students to connect with peers with similar experiences and challenges may provide an opportunity for the more informal type of support that students in this study appeared to prefer. Additionally, universities should provide outreach and education to parents and families about supporting their students/children through mental health challenges and needs, as families were a common source of support for students in this study.
Limitations
Study findings should be considered in light of several limitations. The sample was drawn from a large public university in the southwestern United States, thus limited generalizability to other campuses and regions. Additionally, while the longitudinal design of the quantitative component of the study allowed us to examine changes in mental health symptoms over time, this data was not collected before the start of the pandemic; thus, we are unable to determine if and how pre-existing mental health challenges contributed to participants’ mental health status during the study. Despite these limitations, a notable strength of this study is that undergraduate and graduate students (the first two authors of this paper) were meaningfully engaged throughout the research process. Specifically, these students contributed to study conceptualization and research question formulation, executed data collection and analysis activities, and led several dissemination efforts at local and national conferences.
Conclusion
Study findings extend the growing body of research related to the impact of the COVID-19 pandemic on the mental health of first-year university students, highlighting the multitude of factors that influence students’ willingness and ability to seek out and engage in mental health services. Findings indicate the need for structural changes among universities that increase access to services and robust efforts to facilitate broader narrative change about mental health and help-seeking behaviors among first-year university students.
Supplemental Material
Supplemental Material - Mental Health Needs and Help-Seeking Behaviors Among First-Year University Students Amidst COVID-19: A Mixed Methods Inquiry
Supplemental Material for Mental Health Needs and Help-Seeking Behaviors Among First-Year University Students Amidst COVID-19: A Mixed Methods Inquiry by Katie A. McCormick, Ishaan Manohar, Laura E. Merola, and Deborah A. Cohen in Emerging Adulthood
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Michael and Susan Dell Foundation.
Transparency and Openness Statement
The raw data, analysis syntax and coding manuals, and materials used in this study are not openly available due to privacy restrictions set forth by the institutional ethics board but are available upon request to the corresponding author. No aspects of the study were pre-registered.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.